The Two-Component Model for Calculating Total Body Fat from Body Density: An Evaluation in Healthy Women before, during and after Pregnancy


Abstract
:
1. Introduction
2. Experimental Section
2.1. Subjects, Design, Body Composition Methodology and Calculations
2.2. Statistics
3. Results
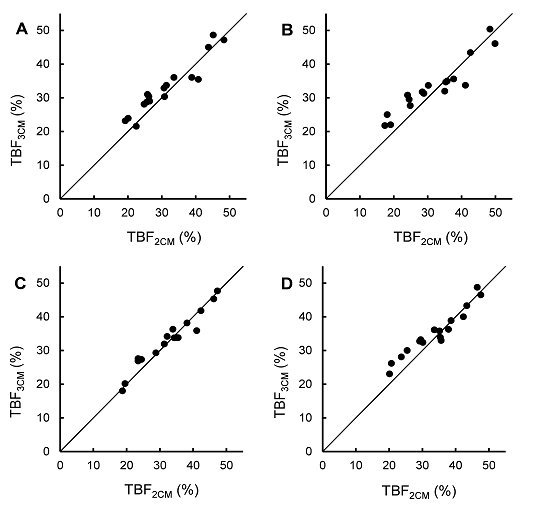
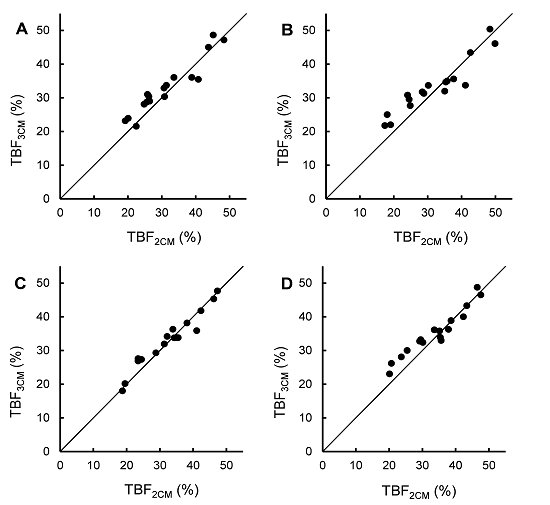
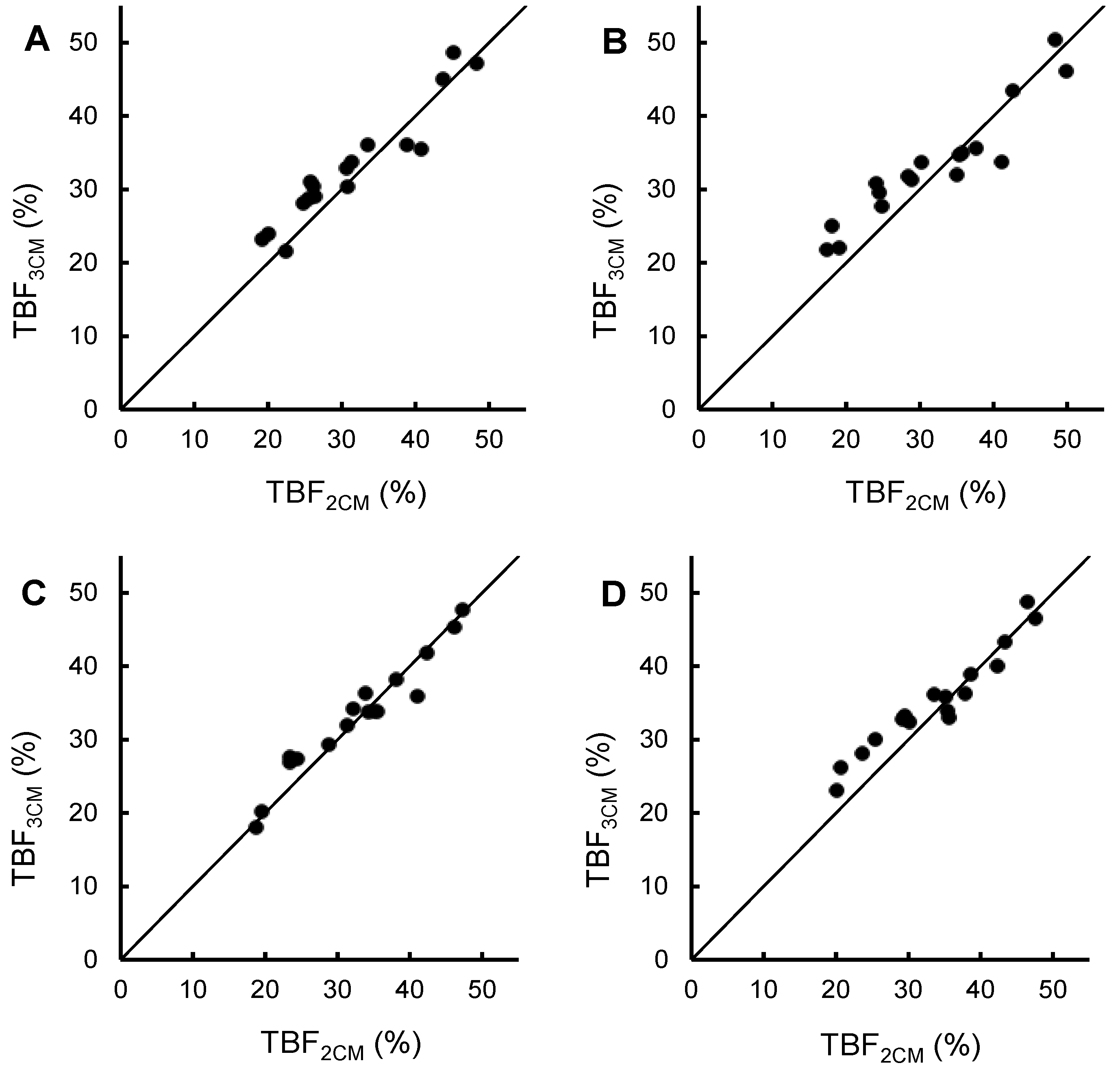
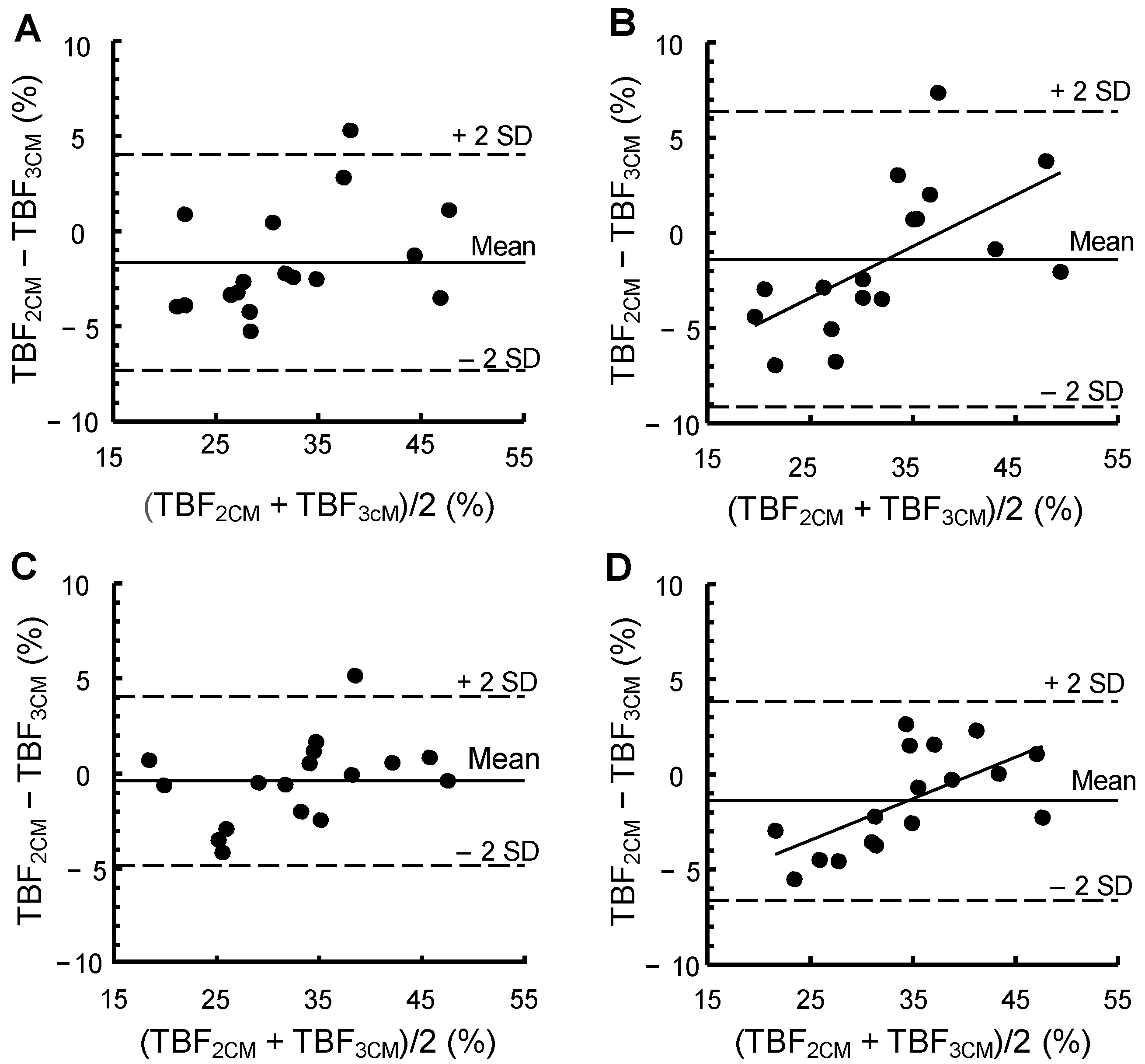
3.1. Total Body Fat Calculated by Means of the 2CM versus the 3CM

{kind=link}
{kind=link}
{kind=link}
| Before Pregnancy | Gestational Week 14 | Gestational Week 32 | 2 Weeks Postpartum | |
|---|---|---|---|---|
| Body weight (kg) | 66.6 ± 12.8 | 68.4 ± 13.2 | 77.3 ± 13.0 | 71.5 ± 12.8 |
| Total body water (kg) | 31.5 ± 4.0 | 32.5 ± 4.3 | 38.1 ± 4.4 | 33.6 ± 4.2 |
| Body density (g/mL) | 1.029 ± 0.019 | 1.027 ± 0.021 | 1.021 ± 0.018 | 1.020 ± 0.017 |
| Total body fat (%) | ||||
| Two-component model | 31.4 ± 9.0 2 | 31.8 ± 10.1 3 | 32.7 ± 8.8 4 | 33.8 ± 8.5 5,6 |
| Three-component model 7 | 33.0 ± 7.9 | 33.2 ± 7.7 | 33.1 ± 7.9 | 35.2 ± 6.8 |
| p for difference 8 | 0.031 | 0.16 | 0.49 | 0.043 |


3.2. FFM Density and Its Variability
4. Discussion
| Average FFM density 1g/mL | Total variability of FFM density | Propagation of error analysis 1 2 | Propagation of error analysis 2 3 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Methodological error | Biological variability | Methodological error | Biological variability | |||||||
| SD | SD | % 4 | SD | % 4 | SD | % 4 | SD | % 4 | ||
| Before pregnancy | 1.106 | 0.010 | 0.007 | 49 | 0.007 | 51 | 0.006 | 33 | 0.009 | 67 |
| Gestational week 14 | 1.104 | 0.014 | 0.007 | 28 | 0.012 | 72 | 0.006 | 18 | 0.013 | 82 |
| Gestational week 32 | 1.093 | 0.008 | 0.007 | 96 | 0.002 | 4 | 0.005 | 47 | 0.006 | 53 |
| 2 weeks postpartum | 1.099 | 0.009 | 0.007 | 70 | 0.005 | 30 | 0.006 | 41 | 0.007 | 59 |
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Hytten, F.E. Nutrition. In Clinical Physiology in Obstetrics; Hytten, F.E., Chamberlain, G., Eds.; Blackwell Scientific Publications: Oxford, UK, 1980; pp. 163–192. [Google Scholar]
- Van Raaij, J.M.A.; Peek, M.E.M.; Vermaat-Miedema, S.H.; Schonk, C.M.; Hautvast, J.G.A.J. New equations for estimating body fat mass in pregnancy from body density or total body water. Am. J. Clin. Nutr. 1988, 48, 24–29. [Google Scholar]
- Food and Agricultural Organization of the United Nations. Energy requirements of pregnancy. In Human Energy Requirements; Report of a Joint FAO/WHO/UNU Expert Consultation, Food and Nutrition Technical Report Series 1; Food and Agricultural Organization of the United Nations: Rome, Italy, 2004; pp. 53–62. [Google Scholar]
- Institute of Medicine and National Research Council. Weight Gain during Pregnancy—Reexaming the Guidelines; Rasmussen, K.M., Yaktine, A.L., Eds.; The National Academies Press: Washington, DC, USA, 2009; p. 80. [Google Scholar]
- Hopkinson, J.M.; Butte, N.F.; Ellis, K.J.; Wong, W.W.; Puyan, M.R.; O’Brian Smith, E. Body fat estimation in late pregnancy and early postpartum: Comparison of two-, three-, and four-component models. Am. J. Clin. Nutr. 1997, 65, 432–438. [Google Scholar] [PubMed]
- Going, S.B. Densitometry. In Human Body Composition; Roche, A.F., Heymsfield, S.B., Lohman, T.G., Eds.; Human Kinetics: Champaign, IL, USA, 1996; pp. 3–23. [Google Scholar]
- Fields, D.A.; Goran, M.I.; McCrory, M.A. Body-composition assessment via air-displacement plethysmography in adults and children: A review. Am. J. Clin. Nutr. 2002, 75, 453–467. [Google Scholar] [PubMed]
- Ginde, S.R.; Geliebter, A.; Rubiano, F.; Silva, A.M.; Wang, J.; Heshka, S.; Heymsfield, S.B. Air displacement plethysmography: Validation in overweight and obese subjects. Obes. Res. 2005, 13, 1232–1237. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B. Measurements of adiposity and body composition. In Obesity Epidemiology; Oxford University Press: New York, NY, USA, 2008; pp. 53–83. [Google Scholar]
- Widen, E.M.; Gallagher, D. Body composition changes in pregnancy: Measurements, predictors and outcomes. Eur. J. Clin. Nutr. 2014, 68, 643–652. [Google Scholar] [CrossRef] [PubMed]
- Elia, M. Body composition analysis: An evaluation of 2 component models, multicomponent models and bedside techniques. Clin. Nutr. 1992, 11, 114–127. [Google Scholar] [CrossRef] [PubMed]
- Lof, M.; Forsum, E. Hydration of fat-free mass in healthy women with special reference to the effect of pregnancy. Am. J. Clin. Nutr. 2004, 80, 960–965. [Google Scholar] [PubMed]
- Siri, W.E. Body composition from fluid spaces and density: Analysis of methods. In Techniques for Measuring Body Composition; Brozek, J., Henschel, A., Eds.; National Academy of Sciences/National Research Council: Washington, DC, USA, 1961; pp. 223–244. [Google Scholar]
- Swedish Maternity Care Registry—2012 Annual Report. Available online: http://www.ucr.uu.se/mhv/index.php/arsrapporter (accessed on 13 September 2014).
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef] [PubMed]
- Kendall, M.; Stewart, A. The Advanced Theory of Statistics, 4th ed.; Griffin & Co Ltd.: London, UK, 1977; pp. 246–247. [Google Scholar]
- Wells, J.; Fuller, N.; Dewit, O.; Fewtrell, M.; Elia, M.; Cole, T. Four-component model of body composition in children: Density and hydration of fat-free mass and comparison with simpler models. Am. J. Clin. Nutr. 1999, 69, 904–912. [Google Scholar] [PubMed]
- Murgatroyd, P.; Coward, W. An improved method for estimating changes in whole-body fat and protein mass in man. Br. J. Nutr. 1989, 62, 311–314. [Google Scholar] [CrossRef] [PubMed]
- Fields, D.A.; Wilson, G.D.; Gladden, L.B.; Hunter, G.R.; Pascoe, D.D.; Goran, M.I. Comparison of the BOD POD with the four-compartment model in adult females. Med. Sci. Sports. Exerc. 2001, 33, 1605–1610. [Google Scholar] [CrossRef] [PubMed]
- Widdowson, E.M. Changes in body proportions and composition during growth. In Scientific Foundations of Pediatrics, 2nd ed.; Davis, J.A., Dobbing, J., Eds.; Heinemann Medical Books Ltd.: London, UK, 1981; pp. 330–342. [Google Scholar]
- Fomon, S.J.; Haschke, F.; Ziegler, E.E.; Nelson, S.E. Body composition of reference children from birth to age 10 years. Am. J. Clin. Nutr. 1982, 35, 1169–1175. [Google Scholar] [PubMed]
- Fuller, N.J.; Jebb, S.A.; Laskey, M.A.; Coward, W.A.; Elia, M. Four-component model for the assessment of body composition in humans: Comparison with alternative methods, and evaluation of the density and hydration of fat-free mass. Clin. Sci. 1992, 82, 687–693. [Google Scholar] [PubMed]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Forsum, E.; Henriksson, P.; Löf, M. The Two-Component Model for Calculating Total Body Fat from Body Density: An Evaluation in Healthy Women before, during and after Pregnancy. Nutrients 2014, 6, 5888-5899. https://doi.org/10.3390/nu6125888
Forsum E, Henriksson P, Löf M. The Two-Component Model for Calculating Total Body Fat from Body Density: An Evaluation in Healthy Women before, during and after Pregnancy. Nutrients. 2014; 6(12):5888-5899. https://doi.org/10.3390/nu6125888
Chicago/Turabian StyleForsum, Elisabet, Pontus Henriksson, and Marie Löf. 2014. "The Two-Component Model for Calculating Total Body Fat from Body Density: An Evaluation in Healthy Women before, during and after Pregnancy" Nutrients 6, no. 12: 5888-5899. https://doi.org/10.3390/nu6125888
APA StyleForsum, E., Henriksson, P., & Löf, M. (2014). The Two-Component Model for Calculating Total Body Fat from Body Density: An Evaluation in Healthy Women before, during and after Pregnancy. Nutrients, 6(12), 5888-5899. https://doi.org/10.3390/nu6125888