Recognising and Managing Refractory Coeliac Disease: A Tertiary Centre Experience

 ,
,
Abstract
:1. Introduction

{kind=link}
{kind=link}
{kind=link}
| Investigations | RCD Type 1 | RCD Type 2 | Ulcerative Jejunitis | EATL |
|---|---|---|---|---|
| Histopathology | Identical to any Marsh classification of coeliac disease | Marsh ≥ II | Mucosal ulceration with villous atrophy and IEL in adjacent mucosa. | Infiltration of medium-sized or large pleomorphic lymphoid cells |
| Intraepithelial lymphocyte (IEL) phenotype | >70% IEL are surface CD3+ and CD8+ | Majority have an aberrant IEL CD3+/CD8− phenotype Rarely have normal CD3+ and CD8+ | Mucosal ulceration with villous atrophy and IEL in adjacent mucosa. | Neoplastic cells are CD3+ and large cell variant are CD30+ Background IELs are mostly phenotypically abnormal (CD3+/CD8−) |
| T-cell receptor gamma gene rearrangement PCR | Polyclonal | Monoclonal | Monoclonal | Monoclonal |
2. Methods
3. Results


| Gender | Age | PRE-TREATMENT | TREATMENT | POST TREATMETN | Clinical Outcome | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Histology Marsh Grade | IEL Phenotype | T-Cell Receptor Status | Hb (g/dL) | Albumin (g/L) | B12 (ng/L) | Folate (µg/L) | Treatment | Time from Treatment (Months) | Histology Marsh Grade | IEL Phenotype | T-Cell Receptor Status | Hb (g/dL) | Albumin (g/L) | B12 (ng/L) | Folate (µg/L) | |||
| Female | 69 | 3a | CD8 + ve | Clonal | 12.9 | 48 | 319 | 20 | Azathioprine + Prednisolone | 0 | 1 | CD8 + ve | Polyclonal | 13.9 | 52 | 407 | 3 | Asymptomatic Good quality of life (QOL) |
| Female | 83 | 3b | CD8 − ve | Clonal | 11.7 | 35 | 294 | 17.3 | Azathioprine + Prednisolone | 6 | 3a | CD8 − ve | No amplification | 11.6 | 40 | 495 | 4 | Asymptomatic QOL affected by comorbidities. |
| Female | 80 | 3b | CD8 − ve | Clonal | 11 | 45 | 379 | 3.5 | Azathioprine + Prednisolone | 12 | 3a | CD8 − ve | Clonal | 11.9 | 43 | >128 | 4.5 | Asymptomatic QOL affected by comorbidities. |
| Male | 49 | 3b | CD8 + ve | Clonal | 14 | 47 | 319 | 14.3 | Azathioprine + Prednisolone | 14 | 3a | CD8 − ve | Polyclonal | 14.5 | 46 | >128 | 17.2 | Asymptomatic Good QOL |
| Female | 79 | 3b | CD8 + ve | Clonal | 14.8 | 47 | 279 | 4.7 | Azathioprine + Prednisolone | 18 | 3a | CD8 + ve | Polyclonal | 14.9 | 49 | >1000 | 7.2 | Asymptomatic QOL affected by comorbidities. |
| Female | 74 | 3c | CD8 − ve | Clonal | 11.4 | 41 | 1500 | 6.9 | Azathioprine + Prednisolone | 20 | 3b | CD8 + ve | Polyclonal | NA | NA | NA | NA | Asymptomatic Good QOL |
| Male | 50 | 3a | CD8 + ve | Clonal | 14.2 | 49 | 177 | 15.4 | Azathioprine + Prednisolone | 21 | 1 | CD8 + ve | Polyclonal | 13.9 | 50 | 70 | 17.6 | Asymptomatic Good QOL |
| Male | 64 | 3a | CD8 − ve | Clonal | 14.7 | 48 | 333 | 3.6 | Azathioprine + Prednisolone | 26 | 2 | CD8 – ve | Polyclonal | 14.9 | 50 | 500 | 3.4 | Asymptomatic Good quality of life |
| Male | 45 | 3a | CD8 − ve | Clonal | 13.8 | 43 | 177 | 15.4 | Azathioprine + Prednisolone | 28 | 3a | CD8 + ve | Polyclonal | 12.1 | 46 | 203 | 13.8 | Asymptomatic Good QOL |
| Female | 55 | 3a | CD8 + ve | Clonal | 11.9 | 41 | 247 | 5.1 | Azathioprine + Prednisolone | 36 | 3a | CD8 + ve | Equivocal | 127 | 44 | 198 | 5.8 | Asymptomatic Good QOL |
| Female | 66 | 3b | CD8 − ve 50% | Clonal | 13.7 | 43 | 200 | 9.5 | Azathioprine + Prednisolone | 36 | 3a | CD8 + ve 75% | Equivocal | 14.1 | 54 | 231 | 12 | Asymptomatic Good QOL |
| Male | 63 | 3a | CD8 − ve | Clonal | 16.1 | 47 | 140 | 2 | Azathioprine + Prednisolone | 36 | 3a | CD8 – ve | Clonal | 15.9 | 47 | 195 | 3.1 | Asymptomatic Good QOL |
| Female | 57 | 3b | CD8 + ve | Clonal | 13.5 | 47 | 559 | 4.2 | Azathioprine + Prednisolone | 36 | 1 | CD8 + ve | Polyclonal | 14 | 46 | 470 | 18 | Asymptomatic Good QOL |
| Female | 67 | 3a | CD8 + ve | Clonal | 13 | 46 | 696 | 16.8 | Mycophenolate mofetil | 36 | 3a | CD8 + ve | Polyclonal | 12.9 | 46 | 128 (active B12) | 5.2 | Asymptomatic Good QOL |
| Male | 71 | 3a | CD8 + ve 50% | Clonal | 14.9 | 36 | 155 | 9.5 | Azathioprine + Prednisolone | 36 | 1 | CD8 + ve 100% | Clonal | 12.6 | 47 | 339 | 7.8 | Asymptomatic. QOL affected by comorbidities. |
| Male | 70 | 3a | CD8 − ve | Clonal | 13.7 | 48 | 64 (active B12) | 5.2 | Azathioprine + Prednisolone | 53 | 1 | CD8 − ve 50% | Polyclonal | 15 | 45 | 68 (active B12) | 20 | Asymptomatic Good QOL |
| Female | 84 | 3b | CD8 − ve | Clonal | 12.4 | 38 | 81 | 12.3 | Azathioprine + Budesnonide | 54 | 3b | CD8 + ve | Polyclonal | 14.1 | 40 | 210 | >20 | Asymptomatic. QOL affected by comorbidities. |
| Female | 74 | 3b | CD8 − ve | Clonal | 13.7 | 43 | 287 | 1.9 | Azathioprine + Prednisolone | 60 | 3b | CD8 − ve 50% | Polyclonal | 11.7 | 42 | 86 | 2.7 | Asymptomatic Good QOL |
| Treatment Outcome | Number of Patients with Identical Clones at the Start of Treatment | Number of Cases with Identical Closes at the End of Treatment or at Latest Follow up |
|---|---|---|
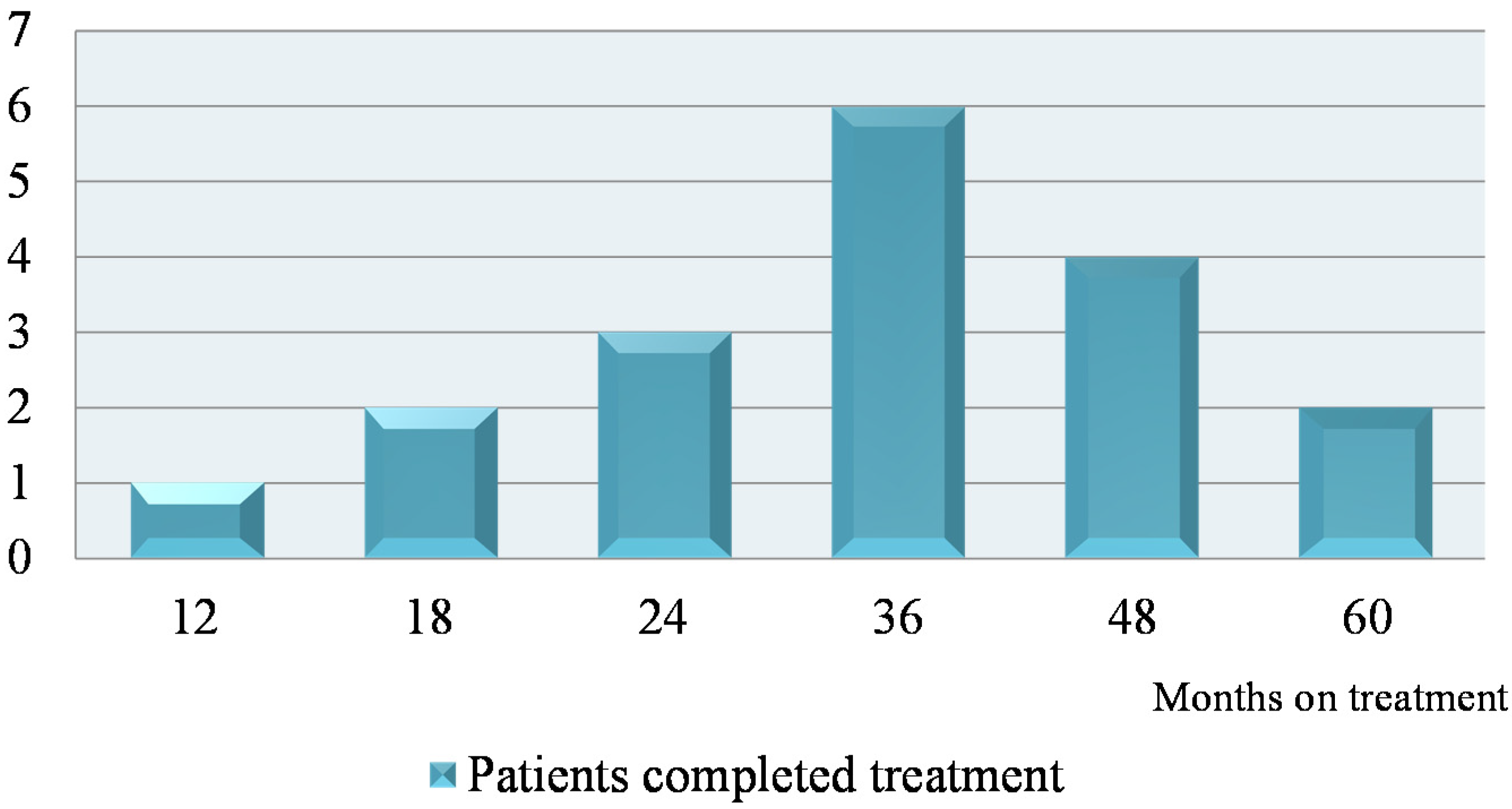
| RCD type 2 patient responded to treatment (n = 18) | 7 patients with identical clones | 0 persistent clones |
| RCD type 2 who remain on treatment (n = 12) | 9 patient identical clones | 9 persistent identical clones |
| Gender | Age | PRE-TREATMENT | TREATMENT | POST TREATMETN | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Histology Marsh Grade | IEL Phenotype | T-Cell Receptor Status | Hb (g/dL) | Albumin (g/L) | B12 (ng/L) | Folate (µg/L) | Treatment | Time from Treatment (Months) | Histology Marsh Grade | IEL Phenotype | T-Cell Receptor Status | Hb (g/dL) | Albumin (g/L) | B12 (ng/L) | Folate (µg/L) | ||
| Male | 61 | 5.2 | CD8 − ve | Clonal | 12.9 | 28 | 42 (active B12) | 5.2 | Azathioprine + Prednisolone | 12 | NA | NA | Equivocal | NA | NA | NA | NA |
| Male | 71 | 7.5 | CD8 + ve 50% | Clonal | 13.2 | 28 | 18 | 7.5 | Azathioprine + Prednisolone | 13 | 3a | CD8 − ve | Polyclonal | 15.1 | 41 | 40 | >20 |
| Female | 68 | 3c | CD8 + ve | Clonal | 14.7 | 47 | 120 | 13.4 | Thioguanine | 21 | 3b | CD8 + ve | Polyclonal | 14.9 | 49 | 78 | 7.7 |
| Female | 79 | 3a | CD8 + ve | Clonal | 14.8 | 47 | 279 | 4.7 | Azathioprine + Prednisolone | 42 | 1 | CD8 + ve | Clonal | NA | NA | NA | NA |
| Male | 48 | 3b | CD8 − ve | Clonal | 11.7 | 33 | 207 | 3.5 | Methotrexate | 57 | 3a | CD8 − ve | Clonal | 14.8 | 38 | 54 | 12.6 |
| Male | 68 | 3c | CD8 − ve | Clonal | 9.7 | 47 | 1500 | 3.6 | Azathioprine + Prednisolone | 60 | 0 | CD8 + ve | Clonal | 11.3 | 47 | 1500 | 8.5 |
| Female | 80 | 3a | CD8 + ve | Clonal | 12.4 | 38 | 81 | 12.3 | Azathioprine + Prednisolone | 72 | 0 | CD8 + ve | Clonal | 14.1 | 40 | 210 | >20 |
| Female | 64 | 3a | CD8 + ve | Clonal | 12.4 | 46 | 210 | 2.6 | Azathioprine + Prednisolone | 72 | 1 | CD8 − ve 50% | Clonal | 13 | 49 | 127 | 13.6 |
| Male | 54 | 3a | CD8 + ve | Clonal | 14.1 | 46 | 171 | 4.1 | Azathioprine + Prednisolone | 72 | 3a | CD8 + ve | Polyclonal | 14.8 | 46 | 70 (active B12) | 7.3 |
| Male | 77 | 3a | CD8 + ve | Clonal | 14.6 | 41 | 286 | 3.1 | Azathioprine + Prednisolone | 74 | 3a | CD8 + ve | Clonal | 14.3 | 45 | 123 | 8.6 |
| Female | 67 | 3a | CD8 + ve | Clonal | 13.7 | 46 | 157 | >20 | Azathioprine + Prednisolone | 78 | 3a | CD8 − ve | Clonal | 142 | 45 | na | 4.5 |
| Female | 85 | 3b | CD8 − ve | Clonal | 13.2 | 46 | 208 | 8.9 | Azathioprine + Prednisolone | 78 | 2 | CD8 − ve | Clonal | 134 | 41 | 37 | 18.1 |
4. Discussion
4.1. Non-Responsive Coeliac Disease (NRCD)

4.2. Refractory Coeliac Disease (RCD)
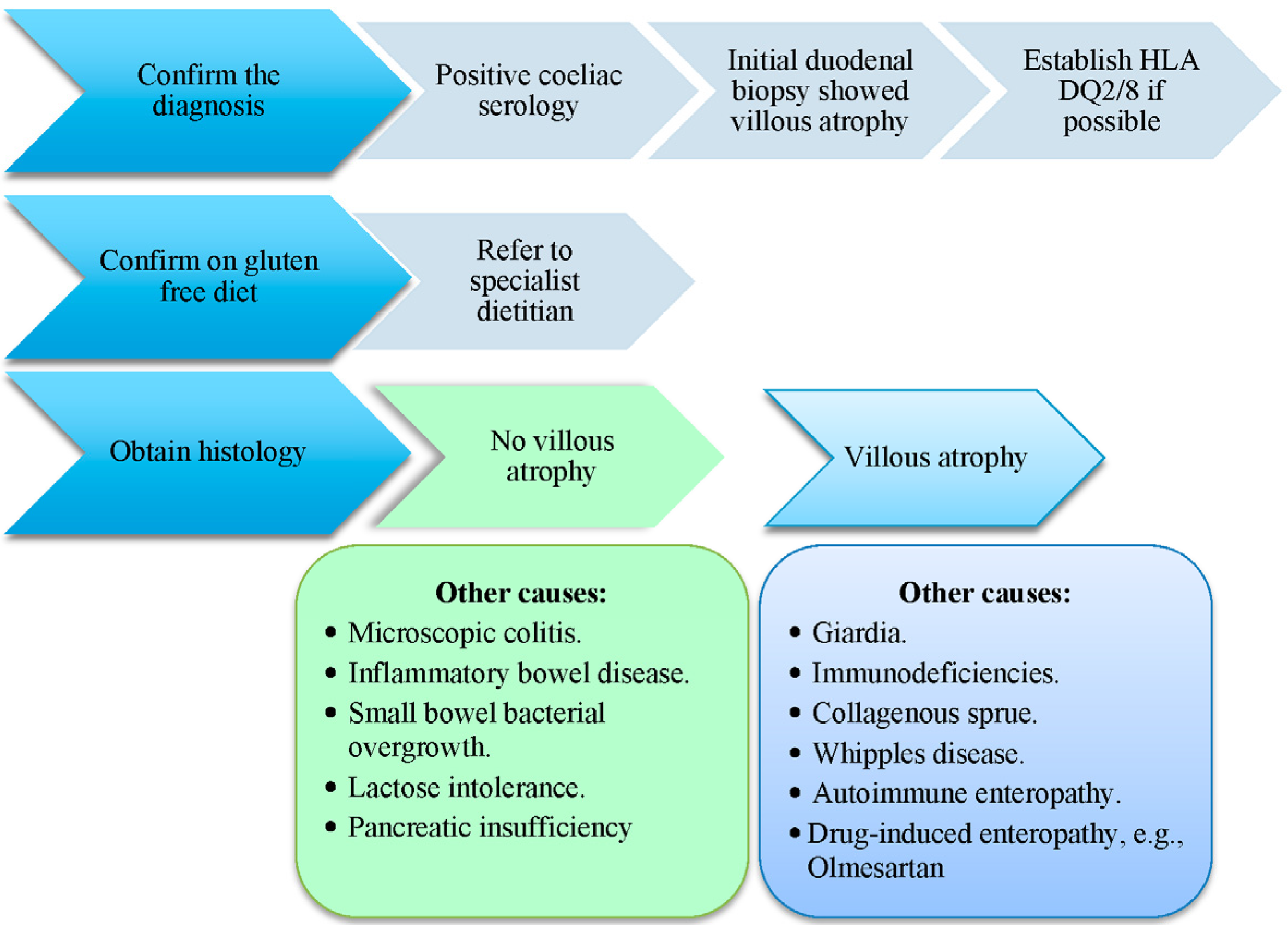
4.3. Diagnosis
- When making the diagnosis, the patient needs to be on a strict GFD with a negative anti-enterocyte antibody result. Dietary assessment of compliance to GFD is key and instruction and education by a specialized dietitian is advised.
- Upper gastrointestinal endoscopy to obtain small bowel biopsies for tissue analysis. The samples are used for Marsh scoring.
- Assessment of IEL phenotyping and polymerase chain reaction (PCR) for TCR (T-cell receptor) monoclonality at the β and/or γ loci.
- 4.
- All cases of RCD type 2 should have a capsule endoscopy to exclude EATL (enteropathy associated T cell lymphoma). It is our practice if there is any suggestion of possible EATL to undertake a small bowel magnetic resonance imaging (MRI) in the first instance to exclude an obstructing lesion, which would be a contra-indication to capsule endoscopy. The capsule endoscopy should be repeated after a year to exclude the development of EATL in view of the high risk. It has been proposed that RCD type 2 should be renamed pre-EATL [17]. Double balloon enteroscopy may be required depending on the findings on capsule endoscopy in order to make a better assessment of an abnormality and obtain samples if required.
- 5.
- Cross sectional imaging including small bowel MRI, computed tomography (CT) scan and positron emission tomography (PET) scan are recommended when suspecting EATL. This can identify abnormal areas within the bowel, abnormal lymph nodes and other organ involvement.
4.4. Management of RCD Type 2
| Treatment Option | Recommended Dose | Outcome | References |
|---|---|---|---|
| Budesonide | 9 mg (range 6–12 mg) | Good Clinical response. Also used in maintenance of clinical remission in collagenous colitis | Brar et al. [19] Daum et al. [20] Miehlke et al. [21] Bonderup et al. [22] |
| Combination thiopurine, including azathioprine, mercaptopurine or thioguanine, combined with prednisolone | 52% progression to EATL within 4–6 years | Al-Toma et al. [12]. | |
| Alemtuzumab (anti CD-52 monoclonal antibody) | 30 mg twice a week per 12 weeks | Not effective | Verbeek et al. [8]. |
| Effective | Vivas et al. [7]. | ||
| Cladribine | 0.1 mg/kg/day for 5 days | Thirty-two patients treated with cladribine, of whom 18 had a good response | Tack et al. [25]. |
| Six of 17 patients had clinical and histologic improvement Clinical improvement (36%), histological improvement (59%), and significant decrease in the number of clonal intraepithelial lymphocytes (35%). However, up to 41% developed EATL and died despite cladribine therapy. | Al-Toma et al. [33] | ||
| Cyclosporin A | 5 mg/kg/day | Case report of histological and clinical improvement in a 45 year old lady with RCD type 2 | Longstreth et al. [26]. |
| Single cases reported to show improvement of clinical parameters and mucosal abnormalities during treatment with cyclosporine | Bernstein et al. [27]. Eijsbouts et al. [28]. | ||
| 61% histological improvement with this treatment in a group of 13 patients with RCD type 2 | Wahab et al. [29]. | ||
| Combination of pentostatin (4 mg/m2 every two weeks per 24 weeks) and budesonide | Pentostatin (4 mg/m2 every two weeks per 24 weeks) | Clinical and histological response as well as a decrease but not disappearance of clonal intraepithelial lymphocytes in 1 case | Dray et al. [34] |
| High-dose chemotherapy followed by ASCT has been explored for RCD type 2 in a pilot study from a single center | All 7 patients: Significant reduction in the aberrant T cells in duodenal biopsies associated with improvement 1 out of the 7 died of progressive neurosypillis | Al-Toma et al. [35] | |
| Out of the 4 patients with EATL, 1 patient sustained remission 32 months after ASCT. Three patients died from relapse within few months after ASCT. | Al-Toma et al. [36] |
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Nasr, I.; Nasr, I.H.; Ciclitira, P.J. Patient management: Coeliac disease. Found. Years J. 2015, 9, 26–29. [Google Scholar]
- Nasr, I.; Leffler, D.A.; Ciclitira, P.J. Management of celiac disease. Gastrointest. Endosc. Clin. N. Am. 2012, 22, 695–704. [Google Scholar] [CrossRef] [PubMed]
- Woodward, J. The management of refractory coeliac disease. Ther. Adv. Chronic Dis. 2013, 4, 77–90. [Google Scholar] [CrossRef] [PubMed]
- Cellier, C.; Delabesse, E.; Helmer, C.; Patey, N.; Matuchansky, C.; Jabri, B.; Macintyre, E.; Cerf-Bensussan, N.; Brousse, N.; the French Coeliac Disease Study Group. Refractory sprue, coeliac disease, and enteropathy-associated T-cell lymphoma. Lancet 2000, 356, 203–208. [Google Scholar] [CrossRef]
- Rubio-Tapia, A.; Murray, J.A. Classification and management of refractory celiac disease. Gut 2010, 59, 547–557. [Google Scholar] [CrossRef] [PubMed]
- Malamut, G.; Afchain, P.; Verkarre, V.; Lecomte, T.; Amiot, A.; Damotte, D. Presentation and long term follow up of refractory coeliac disease: Comparison of type I with type II. Gastroenterology 2009, 136, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Vivas, S.; de Morales, J.; Ramos, R.; Suárez-Vilela, D. Alemtuzumab for refractory celiac disease in a patient at risk for enteropathy-associated T-cell lymphoma. N. Engl. J. Med. 2006, 354, 2514–2515. [Google Scholar] [CrossRef] [PubMed]
- Verbeek, W.H.M.; Mulder, C.J.J.; Zweegman, S. Alemtuzumab for refractory celiac disease. N. Engl. J. Med. 2006, 355, 1396–1397. [Google Scholar] [PubMed]
- Di Sabatino, A.; Biagi, F.; Gobbi, P.G.; Corazza, G.R. How I treat enteropathy-associated T-cell lymphoma. Blood 2012, 119, 2458–2468. [Google Scholar] [CrossRef] [PubMed]
- Dewar, D.H.; Donnelly, S.C.; McLaughlin, S.D.; Johnson, M.W.; Ellis, H.J.; Ciclitira, P.J. Coeliac disease: Management of persistent symptoms in patients on a gluten-free diet. World J. Gastroenterol. 2012, 18, 1348–1356. [Google Scholar] [CrossRef] [PubMed]
- Ludvigsson, J.F.; Leffler, D.A.; Bai, J.; Biagi, F.; Fasano, A.; Green, P.H.; Hadjivassiliou, M.; Kaukinen, K.; Kelly, C.P.; Leonard, J.N.; et al. The Oslo definitions for coeliac disease and related terms. Gut 2013, 62, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Al-Toma, A.; Verbeek, M.; Hadithi, M.; von Blomberg, B.; Mulder, C. Survival in refractory coeliac disease and enteropathy-associated T-cell lymphoma: Retrospective evaluation of single centre experience. Gut 2007, 56, 1373–1378. [Google Scholar] [CrossRef] [PubMed]
- Rubio-Tapia, A.; Kelly, D.; Lahr, B.; Dogan, A.; Wu, T.; Murray, J. Clinical staging and survival in refractory coeliac disease: A single center experience. Gastroenterology 2009, 136, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Al-Toma, A.; Goerres, M.S.; Meijer, J.W.; Peña, A.S.; Crusius, J.B.; Mulder, C.J. Human leukocyte antigen-DQ2 homozygosity and the development of refractory celiac disease and enteropathy-associated T-cell lymphoma. Clin. Gastroenterol. Hepatol. 2006, 4, 315–319. [Google Scholar] [CrossRef] [PubMed]
- Prisco, A.; Troncone, R.; Mazzarella, G.; Gianfrani, C.; Auricchio, S.; Even, J. Identical T-cell receptor beta chain rearrangements are present in T cells infiltrating the jejunal mucosa of untreated coeliac patients. Hum. Immunol. 1997, 55, 22–33. [Google Scholar] [CrossRef]
- Ubiali, A.; Villanacci, V.; Facchetti, F.; Lanzini, A.; Lanzarotto, F.; Rindi, G. Is TCRgamma clonality assay useful to detect early coeliac disease? J. Clin. Gastroenterol. 2007, 41, 275–279. [Google Scholar] [CrossRef] [PubMed]
- Nijeboer, P.; Malamut, G.; Bouma, G.; Cerf-Bensussan, N.; Koning, F.; van Bergen, J.; Cellier, C.; Mulder, C.J.J. Therapy in RCDII: Rationale for combination strategies? Dig. Dis. 2015, 33, 227–230. [Google Scholar] [CrossRef] [PubMed]
- Van Weyenberg, S.; Meijerink, M.; Jacobs, M.; van Kuijk, C.; Mulder, C.; van Waesberghe, J. MR enteroclysis in refractory coeliac disease: Proposal and validation of a severity scoring system. Radiology 2011, 259, 151–161. [Google Scholar] [CrossRef] [PubMed]
- Brar, P.; Lee, S.; Lewis, S.; Egbuna, I.; Bhagat, G.; Green, P. Budesonide in the treatment of refractory celiac disease. Am. J. Gastroenterol. 2007, 97, 2016–2021. [Google Scholar] [CrossRef] [PubMed]
- Daum, S.; Ipczynski, R.; Heine, B.; Schulzke, J.D.; Zeitz, M.; Ullrich, R. Therapy with budesonide in patients with refractory sprue. Digestion 2006, 73, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Miehlke, S.; Maddish, A.; Karimi, D.; Wonschik, S.; Kuhlisch, E.; Beckmann, R.; Morgner, A.; Mueller, R.; Greenwald, R.; Seitz, G.; et al. Budesonide is effective in treating lymphocytic colitis: A randomized double-blind placebo-controlled study. Gastroenterology 2009, 136, 2092–2100. [Google Scholar] [CrossRef] [PubMed]
- Bonderup, O.K.; Hansen, J.B.; Birket-Smith, L.; Vestergaard, V.; Teglbjærg, P.S.; Fallingborg, J. Long-term budesonide treatment of collagenous colitis: A randomised, double-blind, placebo-controlled trial. Gut 2003, 52, 248–251. [Google Scholar] [CrossRef] [PubMed]
- Malamut, G.; Meresse, B.; Verkarre, V.; Kaltenbach, S.; Montcuquet, N.; van Huyen, J.P.D.; Callens, C.; Lenglet, J.; Rahmi, G.; Samaha, E.; et al. Large granular lymphocytic leukemia: A treatable form of refractory coeliac disease. Gastroenterology 2012, 143, 1470–1472. [Google Scholar] [CrossRef] [PubMed]
- Tack, G.J.; Wondergem, M.J.; al-Toma, A.; Verbeek, W.H.M.; Schmittel, A.; Machado, M.V.; Perri, F.; Ossenkoppele, G.J.; Huijgens, P.C.; Schreurs, M.W.J.; et al. Auto-SCT in refractory celiac disease type II patients unresponsive to cladribine therapy. Bone Marrow Transpl. 2011, 46, 840–846. [Google Scholar] [CrossRef] [PubMed]
- Tack, G.J.; Verbeek, W.H.; al-Toma, A.; Kuik, D.J.; Schreurs, M.W.; Visser, O.; Mulder, C. Evaluation of Cladribine treatment in refractory coeliac disease type II. World J. Gastroenterol. 2011, 17, 506–513. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, E.F.; Whitington, P.F. Successful treatment of atypical sprue in an infant with cyclosporin. Gastroenterology 1988, 95, 199–204. [Google Scholar] [PubMed]
- Eijsbouts, A.M.M.; Witteman, B.J.M.; de Sevaux, R.G.L. Undefined malabsorption syndrome with villous atrophy successfully reversed by treatment with cyclosporin. Eur. J. Gastroenterol. Hepatol. 1995, 7, 803–806. [Google Scholar] [PubMed]
- Wahab, P.J.; Crusius, J.B.; Meijer, J.W.; Uil, J.J.; Mulder, C. Cyclosporin in the treatment of adults with refractory coeliac disease—An open pilot study. Aliment. Pharmacol. Ther. 2000, 14, 767–774. [Google Scholar] [CrossRef] [PubMed]
- Dray, X.; Joly, F.; Lavergne-Slove, A.; Treton, X.; Bouhnik, Y.; Messing, B. A severe but reversible refractory sprue. Gut 2006, 55, 1210–1211. [Google Scholar] [CrossRef] [PubMed]
- Turner, S.M.; Moorghen, M.; Probert, C.S. Refractory coeliac disease: Remission with infliximab and immunomodulators. Eur. J. Gastroenterol. Hepatol. 2005, 17, 667–669. [Google Scholar] [CrossRef] [PubMed]
- Rawal, N.; Twaddell, W.; Fasano, A.; Blanchard, S.; Safta, A. Remission of refractory coeliac disease with infliximab in a pediatric patient. ACG Case Rep. J. 2015, 2, 121–123. [Google Scholar] [PubMed]
- Al-Toma, A.; Goerres, M.S.; Meijer, J.W.; von Blomberg, B.M.; Wahab, P.J.; Kerckhaert, J.A.; Mulder, C.J. Cladribine therapy in refractory celiac disease with aberrant T cells. Clin. Gastroenterol. Hepatol. 2006, 4, 1322–1327. [Google Scholar] [CrossRef] [PubMed]
- Longstreth, G.F. Successful treatment of refractory sprue with cyclosporine. Ann. Intern. Med. 1993, 119, 1014–1016. [Google Scholar] [CrossRef] [PubMed]
- Al-Toma, A.; Visser, O.J.; van Roessel, H.M.; von Blomberg, B.M.; Verbeek, W.H.; Scholten, P.E.; Ossenkoppele, G.J.; Huijgens, P.C.; Mulder, C.J. Autologous hematopoietic stem cell transplantation in refractory coeliac disease with aberrant T cells. Blood 2007, 109, 2243–2249. [Google Scholar] [CrossRef] [PubMed]
- Al-Toma, A.; Verbeek, W.H.; Visser, O.J.; Kuijpers, K.C.; Oudejans, J.J.; Kluin-Nelemans, H.C.; Mulder, C.J.; Huijgens, P.C. Disappointing outcome of autologous stem cell transplantation for enteropathy-associated T-cell lymphoma. Dig Liver Dis. 2007, 39, 634–641. [Google Scholar] [CrossRef] [PubMed]
- Gillett, H.R.; Arnott, I.D.; McIntyre, M.; Campbell, S.; Dahele, A.; Priest, M.; Jackson, R.; Ghosh, S. Successful infliximab treatment for steroid-refractory coeliac disease: A case report. Gastroenterology 2002, 22, 800–805. [Google Scholar] [CrossRef]
- Patey-Mariaud de Serre, N.; Cellier, C.; Jabri, B. Distinction between coeliac disease and refractory sprue: A simple immunohistochemical method. Histopathology 2000, 37, 70–77. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nasr, I.; Nasr, I.; Beyers, C.; Chang, F.; Donnelly, S.; Ciclitira, P.J. Recognising and Managing Refractory Coeliac Disease: A Tertiary Centre Experience. Nutrients 2015, 7, 9896-9907. https://doi.org/10.3390/nu7125506
Nasr I, Nasr I, Beyers C, Chang F, Donnelly S, Ciclitira PJ. Recognising and Managing Refractory Coeliac Disease: A Tertiary Centre Experience. Nutrients. 2015; 7(12):9896-9907. https://doi.org/10.3390/nu7125506
Chicago/Turabian StyleNasr, Ikram, Iman Nasr, Carl Beyers, Fuju Chang, Suzanne Donnelly, and Paul J. Ciclitira. 2015. "Recognising and Managing Refractory Coeliac Disease: A Tertiary Centre Experience" Nutrients 7, no. 12: 9896-9907. https://doi.org/10.3390/nu7125506
APA StyleNasr, I., Nasr, I., Beyers, C., Chang, F., Donnelly, S., & Ciclitira, P. J. (2015). Recognising and Managing Refractory Coeliac Disease: A Tertiary Centre Experience. Nutrients, 7(12), 9896-9907. https://doi.org/10.3390/nu7125506