1. Introduction
Vitamin D status is a well-known determinant of skeletal health and influences the risk of fracture, rickets, osteomalacia, and osteoporosis [
1]. Humans obtain vitamin D from exposure to sunlight and diet, which are the two main determinants of vitamin D status in a population. Vitamin D3 is formed by exposure of the skin to sunlight and can also be obtained from the diet via animal products, whereas vitamin D2 is obtained from the diet via plant sources [
1]. Vitamin D (hereafter used to refer to both D2 and D3) from the skin and diet is converted into the circulating metabolite 25-hydroxyvitamin D—25(OH)D, including both 25(OH)D2 and 25(OH)D3—in the liver. This metabolite is often used as a biomarker to determine a patient’s vitamin D status [
2]. The 25(OH)D is metabolized in the kidneys into its active form, 1,25-dihydroxyvitamin D—1,25(OH)2D. The active form circulates in the blood at a significantly lower concentration (approximately 1/1000) compared with the concentration of 25(OH)D [
1]. Circulating vitamin D, 25(OH)D, and 1,25(OH)2D are all bound to vitamin D-binding protein, a specific transporter protein. In target tissues, 1,25(OH)2D exerts its actions by associating with the VDR nuclear receptor (vitamin D receptor). Since the VDR is ubiquitously expressed in most cell types, including brain, prostate, breast, placenta, and immune, vitamin D has been hypothesized to have a number of functions outside the skeletal system [
1].
Due to the importance of vitamin D, many concerns have been raised regarding the functional impacts of maternal vitamin D deficiency on multiple adverse health outcomes in mothers and their offspring. Moreover, low maternal levels of 25-hydroxyvitamin D have been suggested to be associated with a number of adverse obstetrical and neonatal outcomes [
3,
4]. Vitamin deficiency is a modifiable factor; therefore, it is important to determine the optimal vitamin D status during pregnancy. In the context of increasing clinical concern regarding the high prevalence of vitamin D deficiency worldwide, different prevalences of vitamin D deficiency have been reported in different geographic regions and latitudes. These prevalences have been determined by different diagnostic methods [
5,
6].
Multiple studies have shown that immunoassays may be limited by the cross-reactivity of antibodies and by non-equimolar recognition of the D2 and D3 forms of 25(OH)D, thereby overestimating the serum 25(OH)D concentration and the influence of vitamin D binding protein, which is known to circulate at higher concentrations in pregnant women [
7,
8]. Therefore, liquid chromatography-tandem mass spectrometry (LC-MS/MS) has been used as a reference method to accurately estimate patient vitamin D status [
9,
10].
However, a large population-based estimate of the vitamin D status of pregnant Korean women has not yet been performed. Therefore, this study aimed to investigate the vitamin D status of pregnant Korean women. This study also set out to investigate the determinants of vitamin D status during pregnancy and to assess the impact of vitamin D deficiency on pregnancy outcomes.
4. Discussion
The strengths of this study include its prospective study design, the fairly ethnically homogenous sample of adult Koreans, and the use of the gold standard LC-MS/MS method to measure 25(OH)D concentrations. Also, to the best of our knowledge, this is the first report of vitamin D status in Korean pregnant women, the first risk assessment for vitamin D deficiency during pregnancy, and the first investigation of the effect of vitamin D deficiency on pregnancy outcomes.
This study showed a high prevalence (77.3%) of vitamin D deficiency during pregnancy. Although many reports have reported high prevalences of vitamin D deficiency among pregnant women, most of these studies have focused on white and black pregnant women. Only a few studies have assessed vitamin D status in pregnant women living in Asia [
15,
16,
17,
18,
19]. Sunlight exposure at different latitudes is likely to be an important factor that influences vitamin D status. The results of previous studies of vitamin D status among pregnant women in Asia at variable latitudes and in other regions near 36°N [
3,
4,
20,
21,
22,
23,
24], which is similar to the latitude of the present study, are summarized in
Table 6. The high prevalence of vitamin D deficiency observed in the present study is comparable with the findings of previous studies of Asian populations [
15,
16,
17,
18,
19]. These studies tested vitamin D status at different gestational periods and used different cutoffs to define vitamin D deficiency. Moreover, most studies measured vitamin D levels by immunoassays rather than LC-MS/MS, thereby hindering direct comparisons of reported values of 25(OH)D concentrations. A recent study of 311 pregnant Chinese women in Guiyang, China reported a slightly higher prevalence of vitamin D deficiency (83.6%) with a slightly higher mean 25(OH)D concentration (14.69 ng/mL) [
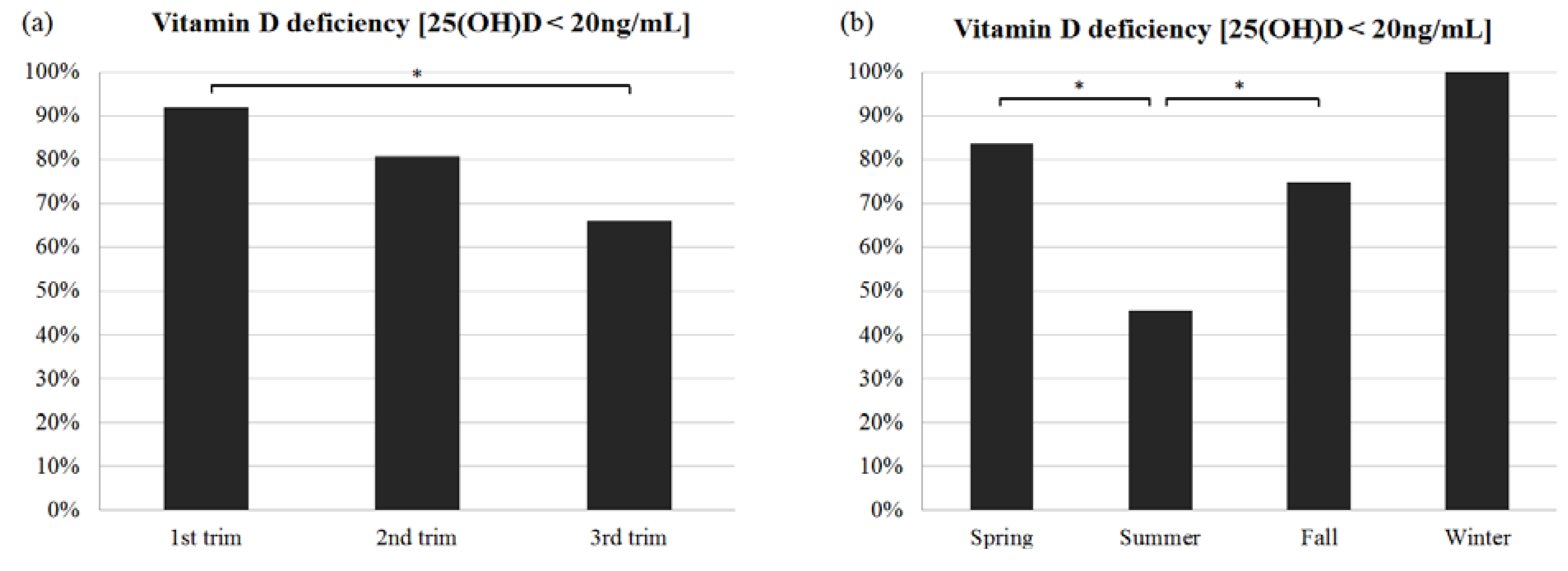
19]. This study used LC-MS/MS for measurement and sampled during the second and third trimesters. Additional studies using accurate measurement methods are needed to obtain more robust estimates of vitamin D status among Asian populations. In the present study, we found that the median 25(OH)D level among pregnant Korean women was significantly lower in the winter (9.4 ng/mL) than in the summer (20.5 ng/mL) or the fall (13.9 ng/mL) (
p < 0.05). Consistent with this finding, the prevalence of vitamin D deficiency was much higher in the winter (100%) than in the summer (45.5%) (
p < 0.05). Even in the summer, a vitamin D deficiency was still found in 45.5% of all women in our cohort. These results are comparable with those of previous studies in China, Greece, Iran, the Spanish Mediterranean seacoast, and California (USA) [
15,
19,
22,
23]. One previous study in Japan found no significant seasonal variation of vitamin D levels in pregnant women [
16], although the highest concentration occurred in the fall. Moreover, a high prevalence of vitamin D deficiency was seen in all four seasons. Thus, it appears to be a general trend that the vitamin D levels in Asian populations are higher in the summer than in the winter.
Table 6.
Serum 25(OH)D concentrations in pregnant women in Asian populations and in regions at latitudes near 36°N.
Table 6.
Serum 25(OH)D concentrations in pregnant women in Asian populations and in regions at latitudes near 36°N.
| Ref. | Region | Lat. (°N) * | N of Preg | GA at Blood Sampling | 25(OH)D Concentration | % <20 ng/mL § (% <50 nmol/L) | Pregnancy and Birth Outcome | Significant Association (p < 0.05) | Method | |
|---|
| Presented as | Reported Value | Units † | Converted to ng/mL ‡ |
|---|
| Asia |
| This study | South Korea | 36 | 220 | First, Second, Third trimesters | median (IQR) | 12.6 (9.65–17.30) | ng/mL | 12.6 | 77.3% | PROM, preterm delivery, SGA | No | LC-MS/MS |
| [16] | Tokai, Japan | 35.3 | 93 ¶ | 30 weeks | mean ± SD | 14.5 ± 5.0 | ng/mL | 14.5 | 89.5% | premature delivery | premature delivery | RIA |
| [17] | Beijing, China ** | 39.9 | 125 | 15–20 weeks | mean ± SD | 28.4 ± 9.5 | nmol/L | 11.42 | 96.8% | NA | | ELISA |
| [19] | Guiyang, China | NA * | 311 | Second and third trimesters | mean ± SD | 14.69 ± 6.81 | ng/mL | 14.69 | 83.6% | NA | | LC-MS/MS |
| [17] | Beijing, China | 39.9 | 70 | Prior to labor | mean ± SE | 28.64 ± 1.41 | nmol/L | 11.47 | 90.2% | birth weight, birth length, HC | birth weight, birth length | ELISA |
| [15]. | Nanjing, China | 31 | 152 | 24–28 weeks | mean ± SD | 10.9 ± 4.78 | ng/mL | 10.9 | in winter 96.1% in summer 94.7% | NA | | ELISA |
| [18] | Chengdu, China | 30.7 | 77 | Before labor | mean ± SD | 35.95 ± 19.7 | nmol/L | 14.40 | NA | NA | | EIA |
| Studies at regions near 36°N |
| [21] | Tehran, Iran ** | NA * | 552 | Delivery | mean ± 2 SD | 27.8 ± 21.71 | nmol/L | 11.1 | NA | birth height, weight, HC, post. & ant. fontanel diameter, Apgar score | No | RIA |
| [20] | USA | NA * | 928 | First, second, third trimesters | mean (95% CI) | 65 (61–68) | nmol/L | 26.0 | 33.8% | NA | | RIA |
| [23] | Almeria, Spain | 36 | 502 | 11–14 weeks | median (IQR) | 27.4 (20.9–32.8) | ng/mL | 27.4 | 22.7% | NA | | ECLIA |
| [3] | Almeria, Spain ‡‡ | 36 | 466 | First, third trimesters | NA | NA | ng/mL | NA | 23.4% | §§ PROM, preterm delivery, SGA, etc. | No | ECLIA |
| [22] | Athens, Greece | NA * | 123 | Delivery | median (IQR) | 16.4 (11–21.1) | ng/mL | 16.4 | NA | NA | | CLIA |
| [4] | Izmir, Turkey | 38.25 | 300 | ≥37 weeks | mean ± SD | 11.5 ± 5.4 | ng/mL | 11.5 | 90.3% | NA | | CLIA |
| [24] | Ankara, Turkey ** | 40 | 79 | Third trimester | mean ± SD | 11.95 + 7.20 | ng/mL | 11.95 | NA | birth height, weight, HC, post. & ant. fontanel diameter, MUAC, Apgar score | No | HPLC |
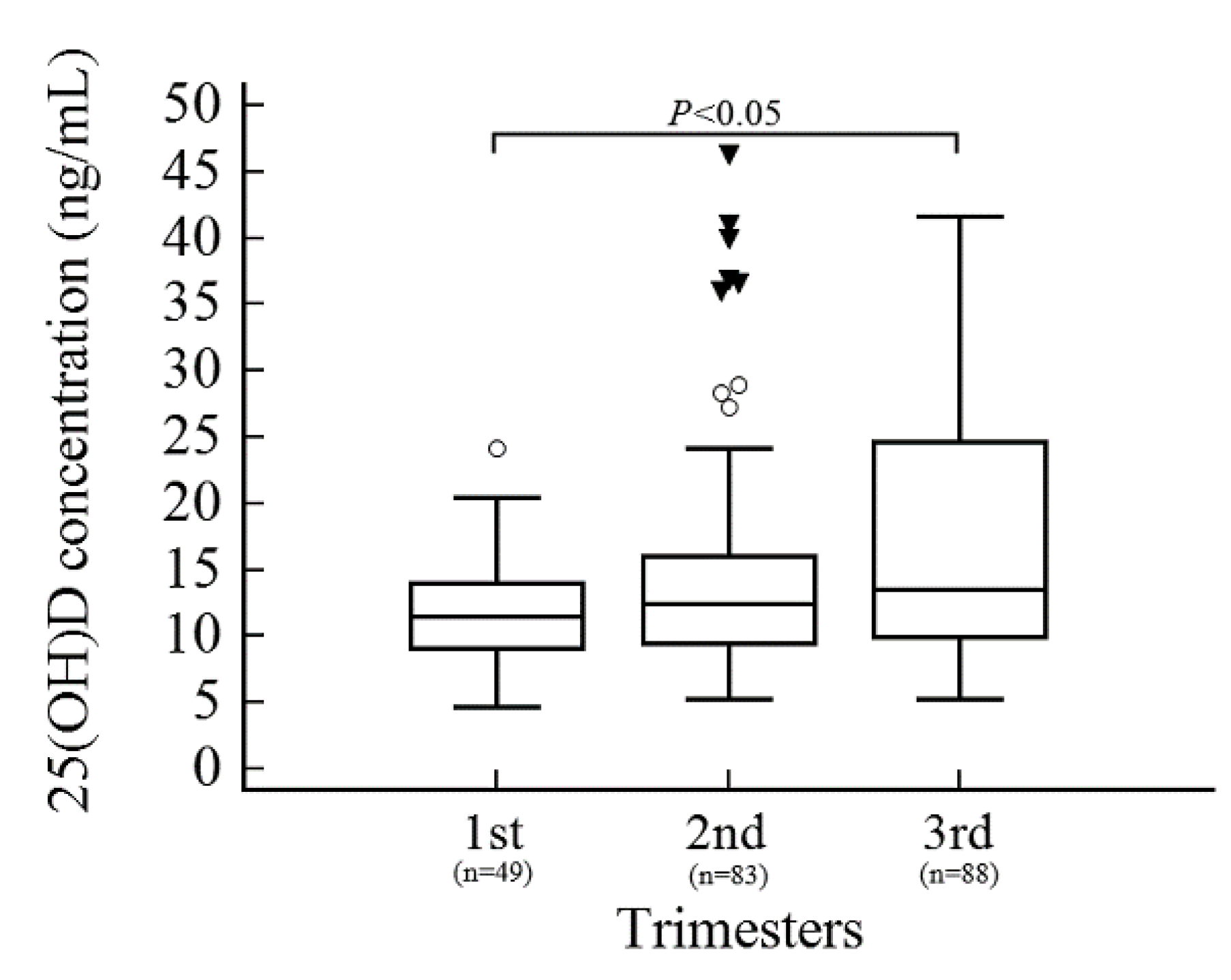
In the present study, analysis of vitamin D status according to trimester revealed that being in the first trimester was a risk factor for vitamin D deficiency in pregnant Korean women. During pregnancy, the serum levels of 1,25(OH)D increase up to 2-fold starting at 10–12 weeks of gestation and reaching a maximum in the third trimester [
25]. However, it is unclear whether 25(OH)D levels steadily increase throughout pregnancy [
20]. The lower vitamin D concentration in the first trimester observed in the present study is comparable with previous studies in Thailand [
26] and the United States [
20], but conflicts with a study in Delhi, India, which found no significant difference among trimesters [
27]. However, the latitude of Delhi is 28.6°N, and this region enjoys abundant sunlight during most of the year, in contrast to the region of the present study (36°N). This study is the first to assess vitamin D status across pregnancy trimesters in Asia at latitudes near 36°N. Although the National Health and Nutrition Examination Survey was conducted in the United States at a latitude similar to this study (36°N) [
20] and reported that later trimester was independently associated with a higher 25(OH)D level—Asian pregnant women were only a small percentage of the participants and were categorized with other ethnic minorities. It is of particular note that, although the latitudes of the studied regions were similar to the latitude in this study, the vitamin D levels were higher in Western countries (the United States and the Spanish Mediterranean seacoast) than in Asian countries, including Korea. This difference could be due to other covariates such as demographics, genetic backgrounds of different ethnic groups, vitamin D supplement use, and outdoor activities [
1,
14]. Our results are most relevant to vitamin D studies of Asian populations in temperate climate areas.
In the present study, we compared the prevalence of vitamin D deficiency between pregnant women and healthy nonpregnant women. A high prevalence was observed in both groups (79.2% in healthy nonpregnant women and 77.3% in pregnant women). The finding that severe vitamin D deficiency was more prevalent in pregnant women (28.6%) than in nonpregnant women (7.2%) suggests that pregnancy itself could be a risk factor for vitamin D deficiency. This finding could be due to physiological changes resulting from nutrient demand and loss during pregnancy [
14].
Interestingly, in addition to trimester and season as risk factors for vitamin D deficiency, we also identified a history of gynecological disease (
i.e., leiomyomas of the uterus or benign ovarian cysts) as a risk factor for vitamin D deficiency through multivariable logistic regression analysis (adjusted OR 3.4662; 95% CI 1.1550–10.3999;
p < 0.05). Previous studies have suggested an association between vitamin D status and uterine diseases such as uterine myoma and endometriosis in both black and white women, although the mechanisms underlying this association remain to be clarified [
28,
29]. However, the present study is the first study of an Asian population to reveal an association between vitamin D deficiency and gynecological disease. Although bacterial vaginosis, which has been reported to be associated with vitamin D deficiency among pregnant women in western populations [
30], was not evaluated in the present study, future research should investigate the relationship between bacterial vaginosis and vitamin D deficiency in Asian populations.
The Endocrine Society recently recommended that pregnant women consume at least 1500–2000 IU of vitamin D per day [
31]. A recent randomized controlled trial showed that vitamin D supplementation for pregnant women of 4000 IU/day was both safe and the most effective level [
32]. However, vitamin D supplementation is not part of most routine antenatal care programs in Korea. Although obstetricians in Korea usually recommend that pregnant women take a vitamin supplement during pregnancy, no consensus has yet been reached among physicians regarding whether the consumption of vitamin D-fortified food or specific vitamin D supplementation should be recommended. This lack of consensus is due at least in part to the lack of sufficient data on vitamin D status, vitamin D supplementation, and their associations with pregnancy-related outcomes to establish guidelines for the Korean population. The present study provides a foundation on which future research on vitamin D status and its associations with pregnancy-related outcomes in Korea can build. Vitamin D supplementation should only be recommended when many factors are taken into consideration. First, the designs and settings of the studies that inform these recommendations should be carefully considered. For instance, the current study included low-risk pregnant women and only looked at a few outcomes; moreover, the current study only enrolled participants with low vitamin D concentrations. Vitamin D expenditure should also be considered in the context of the plasma half-life of vitamin D. The details of supplementation regimens could also be important factors since different doses, boluses, and forms of supplementation could lead to varying biological effects. Moreover, geographical characteristics should also be considered because vitamin D needs can vary significantly within a country, particularly in countries that span large latitudes. During pregnancy, alterations in metabolism such as changes in vitamin D and calcium equilibrium compared with the non-pregnant state support the need for assessing vitamin D status and supplementation in the context of pregnancy. Improved assay methodologies that can detect vitamin D metabolites would also be useful for informing vitamin D supplementation needs, since most studies only report a minority of vitamin D metabolites. All these parameters should be taken into consideration in the design of future vitamin D supplementation trials.
The potential impact of vitamin D deficiency during pregnancy on maternal and neonatal health has attracted much interest in recent years. However, a causal link between vitamin D deficiency during pregnancy and adverse pregnancy-related outcomes remains to be determined using Hill’s criteria [
33], which may be due in part to our limited knowledge. Although one report supported a possible link between a low 25(OH)D status and poor neonatal outcomes [
5], the precise mechanisms underlying this association are yet to be determined. A recent systematic review and meta-analysis found that spontaneous preterm birth and childbirth with SGA were significantly associated with 25(OH)D levels <20 ng/mL [
34]. In the present study, two pregnancy outcomes (preterm delivery and childbirth with SGA) were examined, and no significant association was found between vitamin D deficiency and either pregnancy outcome. These results are comparable with those of a study of pregnant Spanish women [
3]. This agreement may be due to the small numbers of adverse pregnancy outcomes in both studies and the high prevalences of vitamin D deficiency among pregnant Korean women in the groups with and without adverse pregnancy-related outcomes. However, this finding limits the comparisons that can be made, thus warranting further research in this area. Another limitation of the current study is its lack of data about UVB levels and vitamin D intake. However, the current study is also valuable because it is the first to assess potential associations between vitamin D deficiency, preterm delivery, and SGA in a temperate climate region in an ethnically homogeneous Korean population.
In conclusion, our data indicate a high prevalence of vitamin D deficiency among pregnant women in Korea. Even during the summer months, a majority of pregnant women suffered from vitamin D deficiency. Being in the first trimester of pregnancy and the winter season were both associated with an increased risk of vitamin D deficiency in pregnant Korean women. Although no significant associations between vitamin D deficiency and preterm delivery or delivery of SGA babies were observed in the present study, this work will serve as a foundation for future research on vitamin D status and/or supplementation associated with pregnancy-related outcomes among pregnant Korean women.

 ,
, 
{kind=link}
{kind=link}

