Changes in Antioxidant Defense System Using Different Lipid Emulsions in Parenteral Nutrition in Children after Hematopoietic Stem Cell Transplantation


 ,
,
Abstract
:1. Introduction
2. Experimental Section
2.1. Subjects
2.2. Clinical Evaluation
2.3. Parenteral Nutrition
2.4. Sampling and Biochemical Analysis
2.5. Antioxidant Biomarker Analysis
2.6. Antioxidant Defense Enzymes
2.7. Non-Enzymatic Antioxidant Exogenous Compounds
2.8. Statistical Analysis
3. Results

{kind=link}
| Clinical Parameters | Soybean | FO | p |
|---|---|---|---|
| Mean Age (months) | 79 ± 56 (28–131) | 94 ± 40 (56–131) | 0.67 |
| Sex (male/female) | 4/3 | 3/4 | 1.00 |
| Diagnostic: | 0.08 | ||
| Acute Leukemia | 6 | 2 | |
| Bone marrow aplasia | 0 | 1 | |
| Wiskot Aldrich | 0 | 1 | |
| Solid tumors | 1 | 3 | |
| Type of HSCT | |||
| Autologous | 1 | 3 | 0.39 |
| Allogenic | 6 | 4 | 0.56 |
| Complications: | |||
| Mucositis | 7 | 7 | 0.39 |
| GVHD | 4 | 2 | 0.43 |
| VOD | 1 | 1 | 1 |
| Mortality | 1 | 1 | 1 |
| Total days of PN | 16.7 ± 7.36 (10.1–23.8) | 16.85 ± 5.52(11.7–22.2) | 0.97 |
| Days of PN alone | 12.71 ± 8.42 (6.9–20.5) | 15.28 ± 6.01(9.7–20.8) | 0.52 |
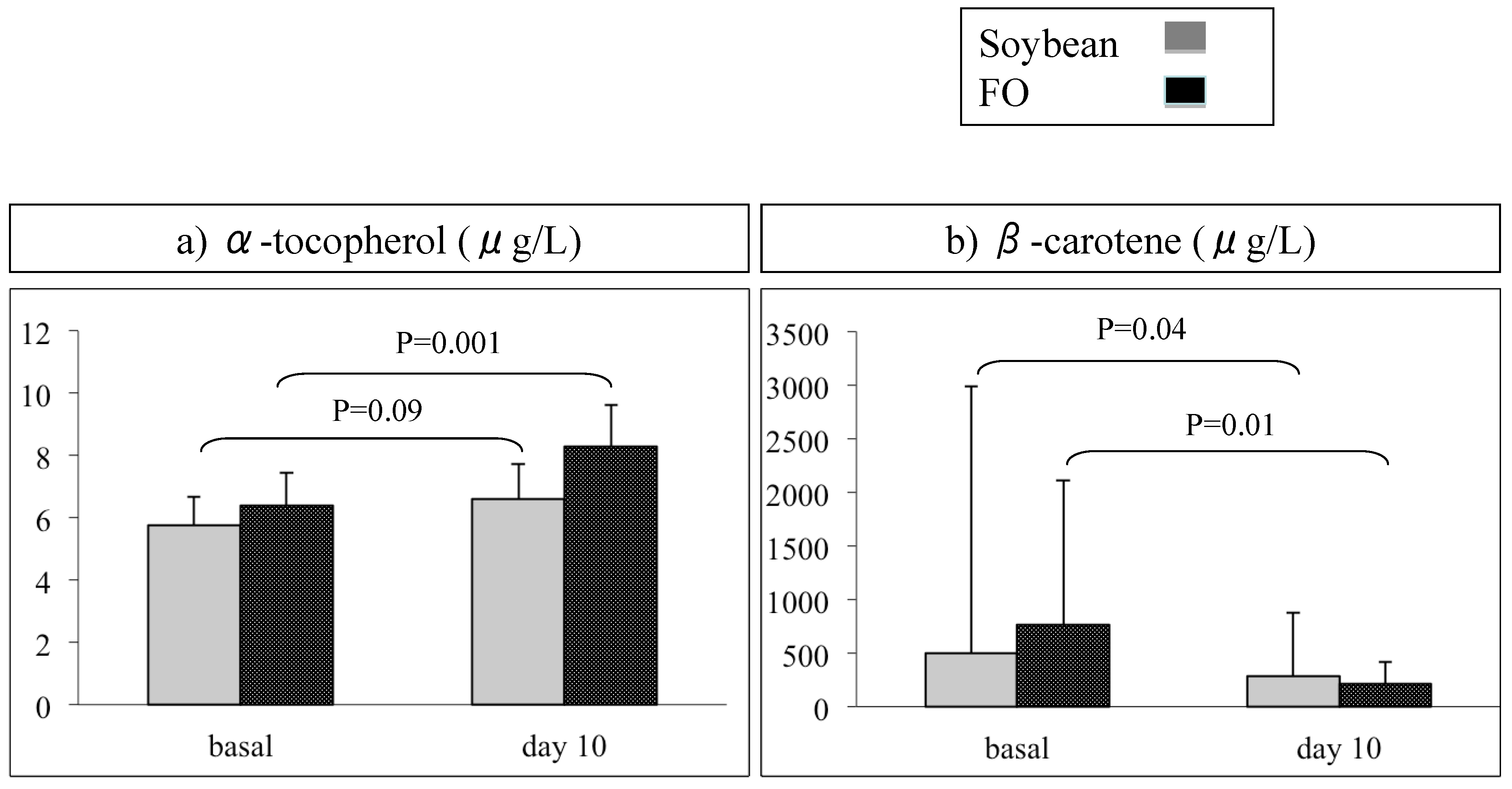
Antioxidant Status
| Antioxidants | Lipid Emulsions | Baseline | p | Day 10 | p |
|---|---|---|---|---|---|
| Vitamin A (mg/L) | Soybean | 0.25 ± 0.11 | 0.25 | 0.24 ± 0.05 | 0.89 |
| FO | 0.19 ± 0.06 | 0.25 ± 0.12 | |||
| α-tocopherol (mg/L) | Soybean | 5.75 ± 1.04 | 0.27 | 6.62 ± 1.34 | 0.03 * |
| FO | 6.39 ± 0.94 | 8.29 ± 1.10 | |||
| β-carotene (μg/L) | Soybean a | 503.15(2482.12) | 0.39 | 282.86(596.13) | 0.75 |
| FO a | 767.94(1344.77) | 212.17(206.61) | |||
| Q9 (μg/L) | Soybean | 10.99 ± 2.56 | 0.39 | 12.55 ± 3.57 | 0.64 |
| FO | 9.89 ± 1.91 | 13.96 ± 6.47 | |||
| Q10 (μg/L) | Soybean | 146.23 ± 92.70 | 0.51 | 142.25 ± 64.23 | 0.64 |
| FO | 120.20 ± 33.82 | 170.14 ± 141.92 | |||
| SOD (U/mg Hb) | Soybean | 1.86 ± 0.93 | 0.69 | 1.60 ± 0.91 | 0.34 |
| FO | 2.03 ± 0.56 | 2.03 ± 0.64 | |||
| GR (μmol/min·g−1 Hb) | Soybean | 2.36 ± 0.80 | 0.07 | 2.68 ±0.91 | 0.49 |
| FO | 3.11 ± 0.52 | 2.41 ± 0.39 | |||
| CAT (nmol/seg·g−1 Hb) | Soybean | 5.71 ± 1.10 | 0.67 | 7.45 ± 1.60 | 0.09 |
| FO | 5.98 ± 1.17 | 5.95 ± 1.30 | |||
| GPOX (μmol/g Hb) | Soybean | 11.94 ± 6.13 | 0.74 | 10.13 ± 4.61 | 0.23 |
| FO | 12.90 ± 4.38 | 13.26 ± 4.27 | |||
| GPOX (μU/g Hb) | Soybean | 10.36 ± 5.32 | 0.74 | 8.79 ± 4.00 | 0.23 |
| FO | 11.20 ± 3.80 | 11.51 ± 3.71 |

4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of interest
References
- Chaudhry, M.; Ali, N. Reduced-intensity conditioning hematopoietic stem cell transplantation: Looking forward to an international consensus. Blood Res. 2015, 50, 69–70. [Google Scholar] [CrossRef] [PubMed]
- Jonas, C.R.; Puckett, A.B.; Jones, D.P.; Griffith, D.P.; Szeszycki, E.E.; Bergman, G.F.; Furr, C.E.; Tyre, C.; Carlson, J.L.; Galloway, J.R.; et al. Plasma antioxidant status after high-dose chemotherapy: A randomized trial of parenteral nutrition in bone marrow transplantation patients. Am. J. Clin. Nutr. 2000, 72, 181–189. [Google Scholar] [PubMed]
- Murray, S.M.; Pindoria, S. Nutrition support for bone marrow transplant patients. Cochrane Database Syst. Rev. 2009, 21, CD002920. [Google Scholar] [CrossRef]
- Jain, A.; Jadhav, A.A.; Varma, M. Relation of oxidative stress, zinc and alkaline phosphatase in protein energy malnutrition. Arch. Physiol. Biochem. 2013, 119, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Owens, J.L.; Hanson, S.J.; McArthur, J.A.; Mikhailov, T.A. The need for evidence based nutritional guidelines for pediatric acute lymphoblastic leukaemia patients: Acute and long-term following treatment. Nutrients 2013, 5, 4333–4346. [Google Scholar] [CrossRef] [PubMed]
- Sari, I.; Cetin, A.; Kaynar, L.; Saraymen, R.; Hacioglu, S.K.; Ozturk, A.; Kocyigit, I.; Altuntas, F.; Eser, B. Disturbance of pro-oxidative/antioxidative balance in allogeneic peripheral blood stem cell transplantation. Ann. Clin. Lab. Sci. 2008, 38, 120–125. [Google Scholar] [PubMed]
- Sabuncuoğlu, S.; Kuşkonmaz, B.; UckunÇetinkaya, D.; Ozgüneş, H. Evaluation of oxidative and antioxidative parameters in pediatric hematopoietic SCT patients. Bone Marrow Transplant. 2012, 47, 651–656. [Google Scholar] [CrossRef] [PubMed]
- Mayor-Oxilia, R. Estrés Oxidativo y Sistema de Defensa Antioxidante. Rev. Inst. Med. Trop. 2010, 5, 23–29. [Google Scholar]
- Ren, T.; Cong, L.; Wang, Y.; Tang, Y.; Tian, B.; Lin, X.; Zhang, Y.; Tang, X. Lipid emulsions in parenteral nutrition: Current applications and future developments. Expert. Opin. Drug. Deliv. 2013, 10, 1533–1549. [Google Scholar] [CrossRef] [PubMed]
- Manzanares, W.; Langlois, P.L.; Dhaliwal, R.; Lemieux, M.; Heyland, D.K. Intravenous fish oil lipid emulsions in critically ill patients: An updated systematic review and meta-analysis. Crit. Care 2015, 19, 167. [Google Scholar] [CrossRef] [PubMed]
- Tian, H.; Yao, X.; Zeng, R.; Sun, R.; Tian, H.; Shi, C.; Li, L.; Tian, J.; Yang, K. Safety and efficacy of a new parenteral lipid emulsion (SMOF) for surgical patients: A systematic review and meta-analysis of randomized controlled trials. Nutr. Rev. 2013, 71, 815–821. [Google Scholar] [CrossRef] [PubMed]
- Li, N.N.; Zhou, Y.; Qin, X.P.; Chen, Y.; He, D.; Feng, J.Y.; Wu, X.T. Does intravenous fish oil benefit patients post-surgery? A meta-analysis of randomised controlled trials. Clin. Nutr. 2014, 33, 226–239. [Google Scholar] [CrossRef] [PubMed]
- Pradelli, L.; Mayer, K.; Muscaritoli, M.; Heller, A.R. N-3 fatty acid-enriched parenteral nutrition regimens in elective surgical and ICU patients: A meta-analysis. Crit. Care 2012, 16, R184. [Google Scholar] [CrossRef] [PubMed]
- Linseisen, J.; Hoffmann, J.; Lienhard, S.; Jauch, K.W.; Wolfram, G. Antioxidant status of surgical patients receiving TPN with an omega-3-fatty acid-containing lipid emulsion supplemented with alpha-tocopherol. Clin. Nutr. 2000, 19, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Wu, Y.; Pei, J.; Chen, Z.; Wang, Q.; Xiang, B. Safety and efficacy of parenteral fish oil-containing lipid emulsions in premature neonates. J. Pediatr. Gastroenterol. Nutr. 2015, 60, 708–716. [Google Scholar] [CrossRef] [PubMed]
- Lansky, S.B.; List, M.A.; Lansky, L.L.; Ritter-Sterr, C.; Miller, D.R. The measurement of performance in childhood cancer patients. Cancer 1987, 60, 1651–1656. [Google Scholar] [CrossRef]
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Sobradillo, B.; Aguirre, A.; Aresti, U.; Bilbao, A.; Fernández-Ramos, C.; Lizárraga, A.; Lorenzo, H.; Madariaga, L.; Rica, I.; Ruiz, I.; et al. Curvasy Tablas de Crecimiento (Estudios Longitudinaly Transversal); Fundación Faustino Orbegozo Eizaguirre: Bilbao, Spain, 2004; pp. 1–31. [Google Scholar]
- Aebi, H. Catalase in vitro. Methods Enzymol. 1984, 105, 121–126. [Google Scholar] [PubMed]
- Carlberg, I.; Mannervik, B. Glutathione reductase. Methods Enzymol. 1985, 113, 484–490. [Google Scholar] [PubMed]
- Flohé, L.; Günzler, W.A. Assays of glutathione peroxidase. Methods Enzymol. 1984, 105, 114–121. [Google Scholar] [PubMed]
- McCord, J.M.; Fridovich, I. The utility of superoxide dismutase in studying free radical reactions. I. Radicals generated by the interaction of sulfite, dimethylsulfoxide, and oxygen. J. Biol. Chem. 1969, 25, 6056–6063. [Google Scholar]
- Battino, M.; Leone, L.; Bompadre, S. High-performance liquid chromatography-EC assay of mitochondrial coenzyme Q9, coenzyme Q9H2, coenzyme Q10, coenzyme Q10H2, and vitamin E with a simplified on-line solid-phase extraction. Methods Enzymol. 2004, 378, 156–162. [Google Scholar] [PubMed]
- Hartman, C.; Ben-Artzi, E.; Berkowitz, D.; Elhasid, R.; Lajterer, N.; Postovski, S.; Hadad, S.; Shamir, R. Olive oil-based intravenous lipid emulsion in pediatric patients undergoing bone marrow transplantation: A short-term prospective controlled trial. Clin. Nutr. 2009, 28, 631–635. [Google Scholar] [CrossRef] [PubMed]
- D’Ascenzo, R.; D’Egidio, S.; Angelini, L.; Bellagamba, M.P.; Manna, M.; Pompilio, A.; Cogo, P.E.; Carnielli, V.P. Parenteral nutrition of preterm infants with a lipid emulsion containing 10% fish oil: Effect on plasma lipids and long-chain polyunsaturated fatty acids. J. Pediatr. 2011, 159, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Rayyan, M.; Devlieger, H.; Jochum, F.; Allegaert, K. Short-term use of parenteral nutrition with a lipid emulsion containing a mixture of soybean oil, olive oil, medium-chain triglycerides, and fish oil: A randomized double-blind study in preterm infants. J. Parenter. Enter. Nutr. 2012, 36, 81–94. [Google Scholar] [CrossRef] [PubMed]
- Baena-Gómez, M.A.; de la Torre Aguilar, M.J.; Mesa, M.D.; Llorente-Cantarero, F.J.; Pérez Navero, J.L.; Gil-Campos, M. Effects of parenteral nutrition formulas on plasma lipid profile in children with bone marrow transplantation. Ann. Nutr. Metab. 2013, 63, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, J.; Smiley, D.; Newton, C.; Le, N.A.; Gosmanov, A.R.; Spiegelman, R.; Peng, L.; Osteen, S.J.; Jones, D.P.; Quyyumi, A.A.; et al. Substitution of standard soybean oil with olive oil-based lipid emulsion in parenteral nutrition: Comparison of vascular, metabolic, and inflammatory effects. J. Clin. Endocrinol. Metab. 2011, 96, 3207–3216. [Google Scholar] [CrossRef] [PubMed]
- Krohn, K.; Koletzko, B. Parenteral lipid emulsions in paediatrics. Curr. Opin. Clin. Nutr. Metab. Care 2006, 9, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Kalish, B.T.; Le, H.D.; Gura, K.M.; Bistrian, B.R.; Puder, M. A metabolomic analysis of two intravenous lipid emulsions in a murine model. PLoS ONE 2013, 8, e59653. [Google Scholar] [CrossRef] [PubMed]
- Hasanoğlu, A.; Dalgiç, N.; Tümer, L.; Atalay, Y.; Cinasal, G.; Biberoğlu, G.; Bukan, N.; Aybar, C. Free oxygen radical-induced lipid peroxidation and antioxidant in infants receiving total parenteral nutrition. Prostaglandins Leukot. Essent. Fat. Acids 2005, 73, 99–102. [Google Scholar] [CrossRef] [PubMed]
- Lespine, A.; Fernandez, Y.; Periquet, B.; Galinier, A.; Garcia, J.; Anglade, F.; Ghisolfi, J.; Thouvenot, J.P. Total parenteral nutrition decreases liver oxidative metabolism and antioxidant defenses in healthy rats: Comparative effect of dietary olive and soybean oil. J. Parenter. Enter. Nutr. 2001, 25, 52–59. [Google Scholar] [CrossRef]
- Versleijen, M.W.; Roelofs, H.M.; Rombouts, C.; Hermans, P.W.; Noakes, P.S.; Calder, P.C.; Wanten, G.J. Short-term infusion of a fish oil-based lipid emulsion modulates fatty acid status, but not immune function or (anti)oxidant balance: A randomized cross-over study. Eur. J. Clin. Invest. 2012, 42, 290–302. [Google Scholar] [CrossRef] [PubMed]
- Choi, I.C.; Fung, P.C.; Leung, A.Y.; Lie, A.K.; Liang, R. Plasma nitric oxide is associated with the occurrence of moderate to severe acute graft-versus-host disease in haemopoietic stem cell transplant recipients. Haematologica 2001, 86, 972–976. [Google Scholar] [PubMed]
- Kelley, N.S.; Yoshida, Y.; Erickson, K.L. Do n-3 polyunsaturated fatty acids increase or decrease lipid peroxidation in humans? Metab. Syndr. Relat. Disord. 2014, 12, 403–415. [Google Scholar] [CrossRef] [PubMed]
- Wichmann, M.W.; Thul, P.; Czarnetzki, H.D.; Morlion, B.J.; Kemen, M.; Jauch, K.W. Evaluation of clinical safety and beneficial effects of a fish oil containing lipid emulsion (Lipoplus, MLF541): Data from a prospective, randomized, multicenter trial. Crit. Care Med. 2007, 35, 700–706. [Google Scholar] [CrossRef] [PubMed]
- Klek, S.; Chambrier, C.; Singer, P.; Rubin, M.; Bowling, T.; Staun, M.; Joly, F.; Rasmussen, H.; Strauss, B.J.; Wanten, G.; et al. Four-week parenteral nutrition using a third generation lipid emulsion (SMOF lipid)—A double-blind, randomised, multicentre study in adults. Clin. Nutr. 2013, 32, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Tomsits, E.; Pataki, M.; Tölgyesi, A.; Fekete, G.; Rischak, K.; Szollár, L. Safety and efficacy of a lipid emulsion containing a mixture of soybean oil, medium-chain triglycerides, olive oil, and fish oil: A randomised, double-blind clinical trial in premature infants requiring parenteral nutrition. J. Pediatr. Gastroenterol. Nutr. 2010, 51, 514–521. [Google Scholar] [CrossRef] [PubMed]
- Pham-Huy, L.A.; He, H.; Pham-Huy, C. Free radicals, antioxidants in disease and health. Int. J. Biomed. Sci. 2008, 4, 89–96. [Google Scholar] [PubMed]
- Skouroliakou, M.; Konstantinou, D.; Koutri, K.; Kakavelaki, C.; Stathopoulou, M.; Antoniadi, M.; Xemelidis, N.; Kona, V.; Markantonis, S. A double-blind, randomized clinical trial of the effect of omega-3 fatty acids on the oxidative stress of preterm neonates fed through parenteral nutrition. Eur. J. Clin. Nutr. 2010, 64, 940–947. [Google Scholar] [CrossRef] [PubMed]
- Goulet, O.; Antébi, H.; Wolf, C.; Talbotec, C.; Alcindor, L.G.; Corriol, O.; Lamor, M.; Colomb-Jung, V. A new intravenous fat emulsion containing soybean oil, medium-chain triglycerides, olive oil, and fish oil: A single-center, double-blind randomized study on efficacy and safety in pediatric patients receiving home parenteral nutrition. J. Parenter. Enter. Nut. 2010, 34, 485–495. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, G.; Simmer, K.; Deshmukh, M.; Mori, T.A.; Croft, K.D.; Kristensen, J. Fish Oil (SMOFlipid) and Olive Oil Lipid (Clinoleic) in Very Preterm Neonates. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 179–184. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baena-Gómez, M.A.; Aguilar, M.J.D.L.T.; Mesa, M.D.; Navero, J.L.P.; Gil-Campos, M. Changes in Antioxidant Defense System Using Different Lipid Emulsions in Parenteral Nutrition in Children after Hematopoietic Stem Cell Transplantation. Nutrients 2015, 7, 7242-7255. https://doi.org/10.3390/nu7095335
Baena-Gómez MA, Aguilar MJDLT, Mesa MD, Navero JLP, Gil-Campos M. Changes in Antioxidant Defense System Using Different Lipid Emulsions in Parenteral Nutrition in Children after Hematopoietic Stem Cell Transplantation. Nutrients. 2015; 7(9):7242-7255. https://doi.org/10.3390/nu7095335
Chicago/Turabian StyleBaena-Gómez, María Auxiliadora, María José De La Torre Aguilar, María Dolores Mesa, Juan Luis Pérez Navero, and Mercedes Gil-Campos. 2015. "Changes in Antioxidant Defense System Using Different Lipid Emulsions in Parenteral Nutrition in Children after Hematopoietic Stem Cell Transplantation" Nutrients 7, no. 9: 7242-7255. https://doi.org/10.3390/nu7095335