Disordered Eating Behaviors and Food Addiction among Nutrition Major College Students

Abstract
:1. Introduction
2. Materials and Methods
2.1. Samples
2.2. Measures
2.3. Statistical Analysis
3. Results
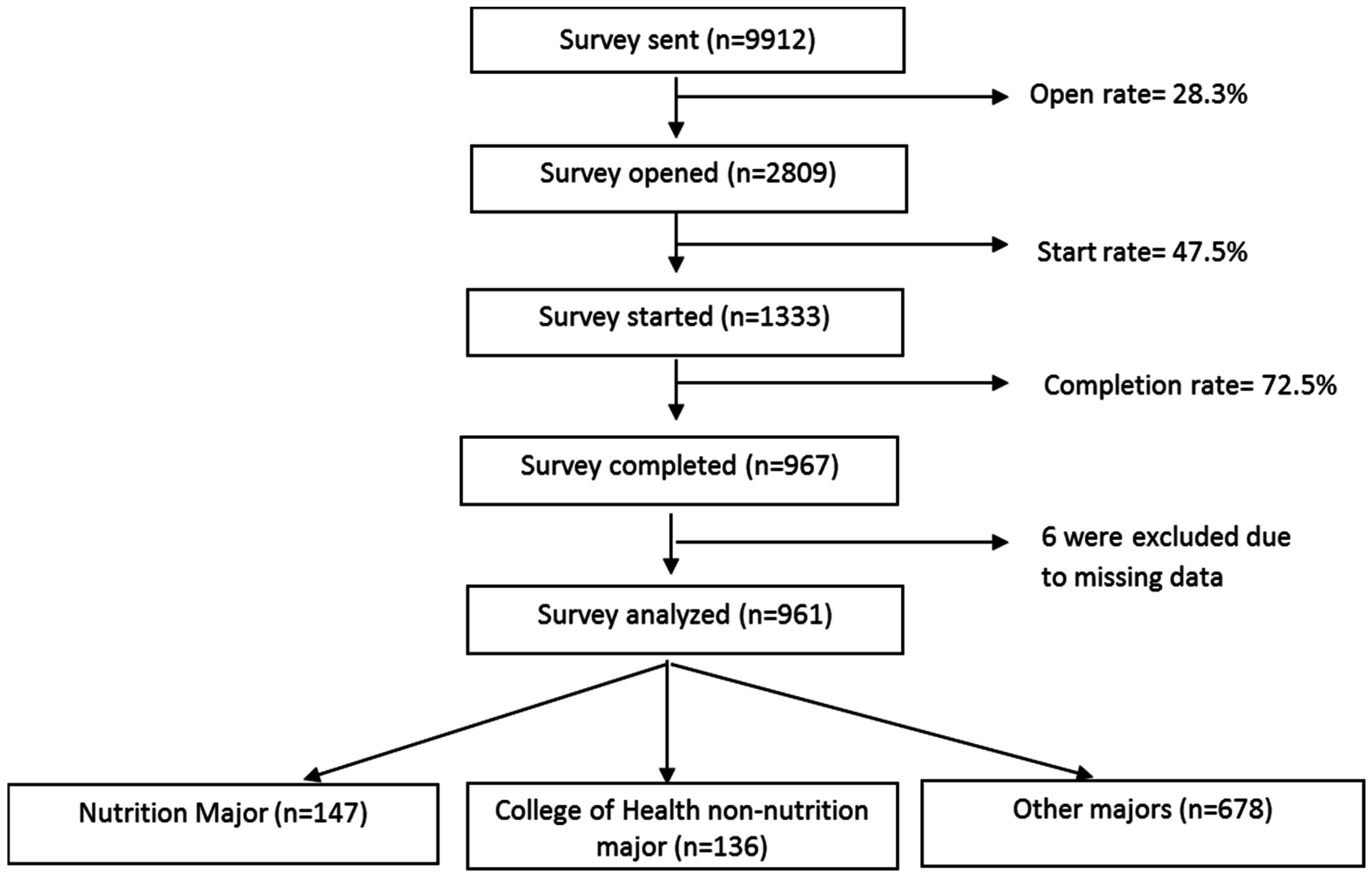
3.1. Respondent Characteristics
3.2. Disordered Eating Behaviors and Food Addiction among Groups
3.3. High Risk Subgroup Analysis by Weight Status
3.4. High Risk Subgroup Analysis by Academic Year
3.5. Co-Occurrence of EAT Score ≥ 20 and Food Addiction Diagnosis by Weight Status
3.6. Co-Occurrence of EAT Score ≥ 20 and Food Addiction Diagnosis by Academic Year
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-V; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Kinzl, J.F.; Traweger, C.; Trefalt, E.; Mangweth, B.; Biebl, W. Binge eating disorder in females: A population-based investigation. Int. J. Eat. Disord. 1999, 25, 287–292. [Google Scholar] [CrossRef]
- Quick, V.M.; Byrd-Bredbenner, C. Disturbed eating behaviours and associated psychographic characteristics of college students. J. Hum. Nutr. Diet. 2013, 26, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Hudson, J.I.; Hiripi, E.; Pope, H.G., Jr.; Kessler, R.C. The prevalence and correlates of eating disorders in the national comorbidity survey replication. Biol. Psychiatry 2007, 61, 348–358. [Google Scholar] [CrossRef] [PubMed]
- Hoek, H.W. Incidence, prevalence and mortality of anorexia nervosa and other eating disorders. Curr. Opin. Psychiatry 2006, 19, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Hoerr, S.L.; Bokram, R.; Lugo, B.; Bivins, T.; Keast, D.R. Risk for disordered eating relates to both gender and ethnicity for college students. J. Am. Coll. Nutr. 2002, 21, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Eisenberg, D.; Nicklett, E.J.; Roeder, K.; Kirz, N.E. Eating disorder symptoms among college students: Prevalence, persistence, correlates, and treatment-seeking. J. Am. Coll. Health 2011, 59, 700–707. [Google Scholar] [CrossRef] [PubMed]
- Tavolacci, M.P.; Grigioni, S.; Richard, L.; Meyrignac, G.; Dechelotte, P.; Ladner, J. Eating disorders and associated health risks among university students. J. Nutr. Educ. Behav. 2015, 47, 412–420. [Google Scholar] [CrossRef] [PubMed]
- Striegel-Moore, R.H. Risk factors for eating disorders. Ann. N. Y. Acad. Sci. 1997, 817, 98–109. [Google Scholar] [CrossRef] [PubMed]
- Ozier, A.D.; Henry, B.W.; American Dietetic, A. Position of the American dietetic association: Nutrition intervention in the treatment of eating disorders. J. Am. Diet. Assoc. 2011, 111, 1236–1241. [Google Scholar] [CrossRef] [PubMed]
- Reiter, C.S.; Graves, L. Nutrition therapy for eating disorders. Nutr. Clin. Pract. 2010, 25, 122–136. [Google Scholar] [CrossRef] [PubMed]
- Korinth, A.; Schiess, S.; Westenhoefer, J. Eating behaviour and eating disorders in students of nutrition sciences. Public Health Nutr. 2010, 13, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Drummond, D.; Hare, M.S. Dietitians and eating disorders: An international issue. Can. J. Diet. Pract. Res. 2012, 73, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Poinhos, R.; Alves, D.; Vieira, E.; Pinhao, S.; Oliveira, B.M.; Correia, F. Eating behaviour among undergraduate students. Comparing nutrition students with other courses. Appetite 2015, 84, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Gonidakis, F.; Sigala, A.; Varsou, E.; Papadimitriou, G. A study of eating attitudes and related factors in a sample of first-year female nutrition and dietetics students of Harokopion University in Athens, Greece. Eat. Weight Disord. 2009, 14, e121–e127. [Google Scholar] [CrossRef] [PubMed]
- Kolka, M.; Abayomi, J. Body image dissatisfaction among food-related degree students. Nutr. Food Sci. 2012, 42, 139–147. [Google Scholar] [CrossRef]
- Kassier, S.; Veldman, F. Eating behavior, eating attitude and body mass index of dietetic students versus non-dietetic majors: A South African perspective. S. Afr. J. Clin. Nutr. 2014, 27, 109–113. [Google Scholar] [CrossRef]
- Mealha, V.; Ferreira, C.; Guerra, I.; Ravasco, P. Students of dietetics & nutrition; a high risk group for eating disorders? Nutr. Hosp. 2013, 28, 1558–1566. [Google Scholar] [PubMed]
- Nergiz-Unal, R.; Bilgic, P.; Yabanci, N. High tendency to the substantial concern on body shape and eating disorders risk of the students majoring nutrition or sport sciences. Nutr. Res. Pract. 2014, 8, 713–718. [Google Scholar] [CrossRef] [PubMed]
- Racette, S.B.; Deusinger, S.S.; Strube, M.J.; Highstein, G.R.; Deusinger, R.H. Weight changes, exercise, and dietary patterns during freshman and sophomore years of college. J. Am. Coll. Health 2005, 53, 245–251. [Google Scholar] [CrossRef] [PubMed]
- De Macedo, I.C.; de Freitas, J.S.; da Silva Torres, I.L. The Influence of Palatable Diets in Reward System Activation: A Mini Review. Adv. Pharmacol. Sci. 2016, 2016, 7238679. [Google Scholar] [CrossRef] [PubMed]
- Randolph, T.G. The descriptive features of food addiction; addictive eating and drinking. Q. J. Stud. Alcohol 1956, 17, 198–224. [Google Scholar] [PubMed]
- Gearhardt, A.N.; Corbin, W.R.; Brownell, K.D. Preliminary validation of the yale food addiction scale. Appetite 2009, 52, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Gearhardt, A.N.; Davis, C.; Kuschner, R.; Brownell, K.D. The addiction potential of hyperpalatable foods. Curr. Drug Abuse Rev. 2011, 4, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Gearhardt, A.N.; Corbin, W.R.; Brownell, K.D. Food addiction: An examination of the diagnostic criteria for dependence. J. Addict. Med. 2009, 3, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Corwin, R.L.; Grigson, P.S. Symposium overview—Food addiction: Fact or fiction? J. Nutr. 2009, 139, 617–619. [Google Scholar] [CrossRef] [PubMed]
- Hebebrand, J.; Albayrak, O.; Adan, R.; Antel, J.; Dieguez, C.; de Jong, J.; Leng, G.; Menzies, J.; Mercer, J.G.; Murphy, M.; et al. “Eating addiction”, rather than “food addiction”, better captures addictive-like eating behavior. Neurosci. Biobehav. Rev. 2014, 47, 295–306. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-IV; American Psychiatric Association: Washington, DC, USA, 2010. [Google Scholar]
- Pursey, K.M.; Stanwell, P.; Gearhardt, A.N.; Collins, C.E.; Burrows, T.L. The Prevalence of Food Addiction as Assessed by the Yale Food Addiction Scale: A Systematic Review. Nutrients 2014, 6, 4552–4590. [Google Scholar] [CrossRef] [PubMed]
- Obregón, A.; Fuentes, J.; Pettinelli, P. Association between food addiction and nutritional status in Chilean college students. Rev. Med. Chil. 2015, 143, 589–597. [Google Scholar] [CrossRef] [PubMed]
- Pedram, P.; Wadden, D.; Amini, P.; Gulliver, W.; Randell, E.; Cahill, F.; Vasdev, S.; Goodridge, A.; Carter, J.C.; Zhai, G.; et al. Food addiction: Its prevalence and significant association with obesity in the general population. PLoS ONE 2013, 8, e74832. [Google Scholar] [CrossRef] [PubMed]
- Gearhardt, A.N.; White, M.A.; Masheb, R.M.; Morgan, P.T.; Crosby, R.D.; Grilo, C.M. An examination of the food addiction construct in obese patients with binge eating disorder. Int. J. Eat. Disord. 2012, 45, 657–663. [Google Scholar] [CrossRef] [PubMed]
- Gearhardt, A.N.; White, M.A.; Masheb, R.M.; Grilo, C.M. An examination of food addiction in a racially diverse sample of obese patients with binge eating disorder in primary care settings. Compr. Psychiatry 2013, 54, 500–505. [Google Scholar] [CrossRef] [PubMed]
- Meule, A.; von Rezori, V.; Blechert, J. Food addiction and bulimia nervosa. Eur Eat. Disord. Rev. 2014, 22, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Gearhardt, A.N.; Boswell, R.G.; White, M.A. The Association of “Food Addiction” with Disordered Eating and Body Mass Index. Eat. Behav. 2014, 15, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Imperatori, C.; Innamorati, M.; Lamis, D.A.; Farina, B.; Pompili, M.; Contardi, A.; Fabbricatore, M. Childhood trauma in obese and overweight women with food addiction and clinical-level of binge eating. Child. Abuse Negl. 2016, 58, 180–190. [Google Scholar] [CrossRef] [PubMed]
- Kass, A.E.; Wang, A.Z.; Kolko, R.P.; Holland, J.C.; Altman, M.; Trockel, M.; Taylor, C.B.; Wilfley, D.E. Identification as overweight by medical professionals: Relation to eating disorder diagnosis and risk. Eat. Behav. 2015, 17, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Napolitano, M.A.; Himes, S. Race, weight, and correlates of binge eating in female college students. Eat. Behav. 2011, 12, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Harris, N.; Gee, D.; d’Acquisto, D.; Ogan, D.; Pritchett, K. Eating disorder risk, exercise dependence, and body weight dissatisfaction among female nutrition and exercise science university majors. J. Behav. Addict. 2015, 4, 206–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mintz, L.B.; O’Halloran, M.S. The Eating Attitudes Test: Validation with DSM-IV eating disorder criteria. J. Personal. Assess. 2000, 74, 489–503. [Google Scholar] [CrossRef] [PubMed]
- Garner, D.M.; Olmsted, M.P.; Bohr, Y.; Garfinkel, P.E. The eating attitudes test: Psychometric features and clinical correlates. Psychol. Med. 1982, 12, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Mocanu, V. Overweight, obesity and dieting attitudes among college students in Romania. Endocr. Care 2013, 9, 241–248. [Google Scholar] [CrossRef]
- Eat-26 Self-Test Interpretation. Available online: http://www.eat-26.com/interpretation.php (accessed on 3 March 2016).
- Karlsson, J.; Persson, L.O.; Sjostrom, L.; Sullivan, M. Psychometric properties and factor structure of the three-factor eating questionnaire (TFEQ) in obese men and women. Results from the Swedish obese subjects (SOS) study. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 1715–1725. [Google Scholar] [CrossRef] [PubMed]
- De Lauzon, B.; Romon, M.; Charles, M.; Lafay, L.; Borys, J.M.; Karlsson, J.; Ducimetière, P.; Charles, M.A. The Three-Factor Eating Questionnaire-R18 is Able to Distinguish among Different Eating Patterns is a General Population. J. Nutr. 2004, 134, 2372–2380. [Google Scholar] [PubMed]
- Lowe, M.; Caputo, G. Binge eating in obesity: Toward the specification of predictors. Int. J. Eat. Disord. 1991, 10, 49–55. [Google Scholar] [CrossRef]
- Burmeister, J.M.; Hinman, N.; Koball, A.; Hoffmann, D.A.; Carels, R.A. Food addiction in adults seeking weight loss treatment. Implications for psychosocial health and weight loss. Appetite 2013, 60, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Desai, M.N.; Miller, W.C.; Staples, B.; Bravender, T. Risk factors associated with overweight and obesity in college students. J. Am. Coll. Health 2008, 57, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Sira, N.; Pawlak, R. Prevalence of overweight and obesity, and dieting attitudes among Caucasian and African American college students in eastern north Carolina: A cross-sectional survey. Nutr. Res. Pract. 2010, 4, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Memon, A.A.; Adil, S.E.; Siddiqui, E.U.; Naeem, S.S.; Ali, S.A.; Mehmood, K. Eating disorders in medical students of Karachi, Pakistan-a cross-sectional study. BMC Res. Notes 2012, 5, 84. [Google Scholar] [CrossRef] [PubMed]
- Gan, W.Y.; Mohd, N.M.; Zalilah, M.S.; Hazizi, A.S. Differences in eating behaviours, dietary intake and body weight status between male and female Malaysian university students. Malays. J. Nutr. 2011, 17, 213–228. [Google Scholar] [PubMed]
- Sepulveda, A.R.; Carrobles, J.A.; Gandarillas, A.M. Gender, school and academic year differences among Spanish university students at high-risk for developing an eating disorder: An epidemiologic study. BMC Public Health 2008, 8, 102. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Lu, M.; Tian, L.; Lu, W.; Meng, F.; Chen, C.; Tang, T.; He, L.; Yao, Y. Prevalence of disordered eating attitudes among university students in Wuhu, China. Nutr. Hosp. 2015, 32, 1752–1757. [Google Scholar] [PubMed]
- Madanat, H.N.; Hawks, S.R.; Novilla, M.L. A comparison of disordered eating attitudes and behaviors among Filipino and American college students. Eat. Weight Disord. 2006, 11, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Siervo, M.; Boschi, V.; Papa, A.; Bellini, O.; Falconi, C. Application of the scoff, eating attitude test 26 (eat 26) and eating inventory (TFEQ) questionnaires in young women seeking diet-therapy. Eat. Weight Disord. 2005, 10, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Pastore, D.R.; Fisher, M.; Friedman, S.B. Abnormalities in weight status, eating attitudes, and eating behaviors among urban high school students: Correlations with self-esteem and anxiety. J. Adolesc. Health 1996, 18, 312–319. [Google Scholar] [CrossRef]
- Orbitello, B.; Ciano, R.; Corsaro, M.; Rocco, P.L.; Taboga, C.; Tonutti, L.; Armellini, M.; Balestrieri, M. The eat-26 as screening instrument for clinical nutrition unit attenders. Int. J. Obes. 2006, 30, 977–981. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.; Curtis, C.; Levitan, R.D.; Carter, J.C.; Kaplan, A.S.; Kennedy, J.L. Evidence that ‘food addiction’ is a valid phenotype of obesity. Appetite 2011, 57, 711–717. [Google Scholar] [CrossRef] [PubMed]
- Houston, C.A.; Bassler, E.; Anderson, J. Eating disorders among dietetics students: An educator’s dilemma. J. Am. Diet. Assoc. 2008, 108, 722–724. [Google Scholar] [CrossRef] [PubMed]
- Sanlier, N.; Turkozu, D.; Toka, O. Body image, food addiction, depression, and body mass index in university students. Ecol. Food Nutr. 2016, 55, 491–507. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| All (n = 961) | Nutrition (n = 147) | COH # Non-Nutrition (n = 136) | Other Majors (n = 678) | p-Value | |
|---|---|---|---|---|---|
| Sex | |||||
| Male | 262 (27.2%) | 23 (15.6%) | 29 (21.5%) | 209 (30.8%) | <0.0001 |
| Female | 699 (72.7%) | 124 (84.4%) | 106 (78.5%) | 469 (69.2%) | |
| Height (inches) ** | 66.32 ± 3.71 | 65.44 ± 3.16 a | 66.23 ± 3.51 a,b | 66.53 ± 3.83 b | <0.01 |
| Weight (lbs) ** | 150.10 ± 37.08 | 140.38 ± 27.78 a | 147.16 ± 35.37 a,b | 152.79 ± 38.77 b | 0.001 |
| BMI ** | 23.89 ± 5.16 | 22.99 ± 4.03 a | 23.43 ± 4.40 a,b | 24.17 ± 5.49 b | <0.05 |
| BMI category | |||||
| Underweight < 18.5 | 51 (5.3%) | 6 (4.1%) | 7 (5.2%) | 38 (5.6%) | NS |
| Normal 18.5–25 | 630 (65.6%) | 105 (71.9%) | 100 (74.1%) | 422 (62.4%) | |
| Overweight 25–30 | 186 (19.4%) | 28 (19.2%) | 17 (12.6%) | 140 (20.7%) | |
| Obese I 30–35 | 77 (8.0%) | 6 (4.1%) | 10 (7.4%) | 61 (9.0%) | |
| Obese II > 35 | 17 (1.8%) | 1 (0.7%) | 1 (0.7%) | 15 (2.2%) | |
| Ethnicity | |||||
| White | 717 (74.8%) | 107 (74.1%) | 100 (73.5%) | 510 (75.4%) | NS |
| African American | 60 (6.3%) | 9 (6.1%) | 12 (8.8%) | 39 (5.8%) | |
| Hispanic | 78 (8.2%) | 9 (6.1%) | 13 (9.6%) | 56 (8.3%) | |
| Asian/Pacific Islander | 57 (6.0%) | 14 (9.5%) | 6 (4.4%) | 37 (5.5%) | |
| Others | 45 (4.7%) | 6 (4.1%) | 5 (3.7%) | 34 (5.0%) | |
| Academic Year | |||||
| Freshman | 179 (18.6%) | 12 (8.2%) | 36 (26.7%) | 131 (19.4%) | <0.0001 |
| Sophomore | 185 (19.3%) | 17 (11.6%) | 36 (26.7%) | 132 (19.5%) | |
| Junior | 353 (36.9%) | 69 (46.9%) | 41 (30.4%) | 243 (35.9%) | |
| Senior | 242 (25.2%) | 49 (33.3%) | 22 (16.3%) | 171 (25.3%) |
| All (n = 961) | Nutrition (n = 147) | COH # Non-Nutrition (n = 136) | Other Majors (n = 678) | p-Value | |||
| Theoretical Range | Min–Max | Value | |||||
| EAT-26 | |||||||
| Dieting scale | 6.21 ± 6.56 | 6.33 ± 6.14 | 5.81 ± 6.28 | 6.26 ± 6.70 | NS | ||
| Bulimia/Food preoccupation | 1.31 ± 2.61 | 1.49 ± 2.44 | 1.12 ± 2.33 | 1.31 ± 2.70 | NS | ||
| Oral control scale | 1.81 ± 2.28 | 1.49 ± 1.47 | 1.57 ± 1.89 | 1.92 ± 2.47 | NS | ||
| Total score | 9.32 ± 9.34 | 9.31 ± 7.83 | 8.49 ± 8.72 | 9.49 ± 9.76 | NS | ||
| EAT score ≥ 20 (%) | 96 (10.0%) | 14 (9.5%) | 14 (10.3%) | 68 (10.0%) | NS | ||
| TFEQ-R18 | |||||||
| Cognitive restraint | 6–24 | 6–24 | 12.9 ± 3.8 | 12.9 ± 3.6 | 12.8 ± 3.1 | 12.9 ± 4.0 | NS |
| Uncontrolled eating | 9–36 | 9–36 | 18.7 ± 5.6 | 18.8 ± 5.5 | 18.5 ± 5.1 | 18.7 ± 5.6 | NS |
| Emotional eating | 3–12 | 3–12 | 6.4 ± 2.6 | 6.5 ± 2.5 | 6.5 ± 2.6 | 6.4 ± 2.7 | NS |
| All (n = 942) | Nutrition (n = 145) | COH Non-Nutrition (n = 134) | Other Majors (n = 663) | p-Value | |||
| Theoretical Range | Min–Max | Value | |||||
| YFAS | |||||||
| Symptom count | 0–7 | 0–7 | 1.91 ± 1.55 | 1.85 ± 1.35 | 1.96 ± 1.72 | 1.92 ± 1.55 | NS |
| “Food dependence” diagnosis | 11.6% | 99 (10.3%) | 14 (9.5%) | 19 (14%) | 66 (9.7%) | NS | |
| Loss of control | 21.7% | 81 (8.6%) | 12 (8.3%) | 11 (8.2%) | 58 (8.7%) | NS | |
| Have tried unsuccessfully | 71.3% | 845 (89.7%) | 130 (89.7%) | 122 (91.0%) | 593 (89.4%) | NS | |
| Large amount of time spent | 24.0% | 177 (18.8%) | 29 (20.0%) | 29 (21.6%) | 119 (17.9%) | NS | |
| Important activities given up | 10.3% | 128 (13.6%) | 16 (11.0%) | 20 (14.9%) | 92 (13.9%) | NS | |
| Continued despite problems | 28.3% | 251 (26.6%) | 36 (24.8%) | 26 (19.4%) | 189 (28.5%) | NS | |
| Tolerance | 13.5% | 239 (25.4%) | 35 (24.1%) | 32 (23.9%) | 172 (25.9%) | NS | |
| Withdrawal ** | 16.3% | 118 (12.5%) | 14 (9.7%) a | 27 (20.1%) b | 77 (11.6%) a | <0.05 | |
| Clinical significance | 14% | 129 (13.7%) | 17 (11.7%) | 24 (17.9%) | 88 (13.3%) | NS |
| All (n = 957) | Nutrition (n = 145) | COH # Non-Nutrition (n = 134) | Other Majors (n = 678) | p-Value 1 | |
| Total | |||||
| Underweight/Normal | 678 | 111 | 107 | 460 | |
| Overweight/Obese | 279 | 34 | 27 | 218 | |
| EAT ≥ 20 | |||||
| Underweight/Normal | 60 (8.8%) | 11 (9.9%) | 6 (5.6%) | 43 (9.3%) | NS |
| Overweight/Obese | 36 (12.9%) | 2 (5.9%) | 7 (25.9%) | 27 (12.4%) | NS |
| p-value 2 | NS | NS | <0.005 | NS | |
| All (n = 939) | Nutrition (n = 144) | COH Non-Nutrition (n = 133) | Other Majors (n = 662) | p-Value 1 | |
| Total | |||||
| Underweight/Normal | 666 | 110 | 105 | 451 | |
| Overweight/Obese | 273 | 34 | 28 | 211 | |
| Food addiction (YFAS) | |||||
| Underweight/Normal | 59 (8.9%) | 10 (9.1%) | 11 (10.5%) | 38 (8.4%) | NS |
| Overweight/Obese | 40 (14.7%) | 4 (11.8%) | 8 (28.6%) | 28 (13.3%) | NS |
| p-value 2 | <0.01 | NS | <0.05 | NS |
| All (n = 959) | Nutrition (n = 147) | COH # Non-Nutrition (n = 135) | Other Majors (n = 677) | p-Value 1 | |
| Total | |||||
| Freshman/Sophomore | 364 | 29 | 72 | 263 | |
| Junior/Senior | 595 | 118 | 63 | 414 | |
| EAT ≥ 20 | |||||
| Freshman/Sophomore | 32 (8.8%) | 4 (13.8%) | 6 (8.3%) | 22 (8.4%) | NS |
| Junior/Senior | 63 (10.6%) | 10 (8.5%) | 7 (11.1%) | 46 (11.1%) | NS |
| p-value 2 | NS | NS | NS | NS | |
| All (n = 940) | Nutrition (n = 145) | COH Non-Nutrition (n = 133) | Other Majors (n = 662) | p-Value 1 | |
| Total | |||||
| Freshman/Sophomore | 357 | 28 | 71 | 258 | |
| Junior/Senior | 583 | 117 | 62 | 404 | |
| Food addiction (YFAS) | |||||
| Freshman/Sophomore | 34 (9.5%) | 5 (17.9%) | 9 (12.7%) | 20 (7.8%) | NS |
| Junior/Senior | 64 (11.0%) | 9 (7.7%) | 9 (14.5%) | 46 (11.4%) | NS |
| p-value 2 | NS | NS | NS | NS |
| Total | Underweight/Normal | Overweight/Obese | p-Value 1 | |
|---|---|---|---|---|
| EAT ≥ 20 and FA | 43 | 27 | 16 | |
| Total | 957 | 678 | 279 | |
| EAT ≥ 20 | 96 | 60 | 36 | |
| % of total | 4.5% | 4.0% | 5.7% | NS |
| % of all EAT ≥ 20 | 44.8% | 45% | 44.4% | NS |
| EAT ≥ 20 and FA | 43 | 27 | 16 | |
| Total | 939 | 666 | 273 | |
| FA | 99 | 59 | 40 | |
| % of total | 4.6% | 4.1% | 5.9% | NS |
| % of all FA | 43.4% | 45.8% | 40% | NS |
| Total | Freshman/Sophomore | Junior/Senior | p-Value 1 | |
|---|---|---|---|---|
| EAT ≥ 20 and FA | 42 | 13 | 29 | |
| Total | 959 | 364 | 595 | |
| EAT ≥ 20 | 95 | 32 | 63 | |
| % of total | 4.4% | 3.6% | 4.9% | NS |
| % of all EAT ≥ 20 | 44.2% | 40.6% | 46% | NS |
| EAT ≥ 20 and FA | 42 | 13 | 29 | |
| Total | 940 | 357 | 583 | |
| FA | 98 | 34 | 64 | |
| % of total | 4.5% | 3.6% | 5.0% | NS |
| % of all FA | 42.9% | 38.2% | 45.3% | NS |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, Z.; Tan, M. Disordered Eating Behaviors and Food Addiction among Nutrition Major College Students. Nutrients 2016, 8, 673. https://doi.org/10.3390/nu8110673
Yu Z, Tan M. Disordered Eating Behaviors and Food Addiction among Nutrition Major College Students. Nutrients. 2016; 8(11):673. https://doi.org/10.3390/nu8110673
Chicago/Turabian StyleYu, Zhiping, and Michael Tan. 2016. "Disordered Eating Behaviors and Food Addiction among Nutrition Major College Students" Nutrients 8, no. 11: 673. https://doi.org/10.3390/nu8110673
APA StyleYu, Z., & Tan, M. (2016). Disordered Eating Behaviors and Food Addiction among Nutrition Major College Students. Nutrients, 8(11), 673. https://doi.org/10.3390/nu8110673