A Prospective Study of Serum Trace Elements in Healthy Korean Pregnant Women

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Data Collection
2.3. Pregnancy and Neonatal Outcomes
2.4. Laboratory Analyses
2.5. Statistical Analysis
3. Results
3.1. General Characteristics of the Study Population
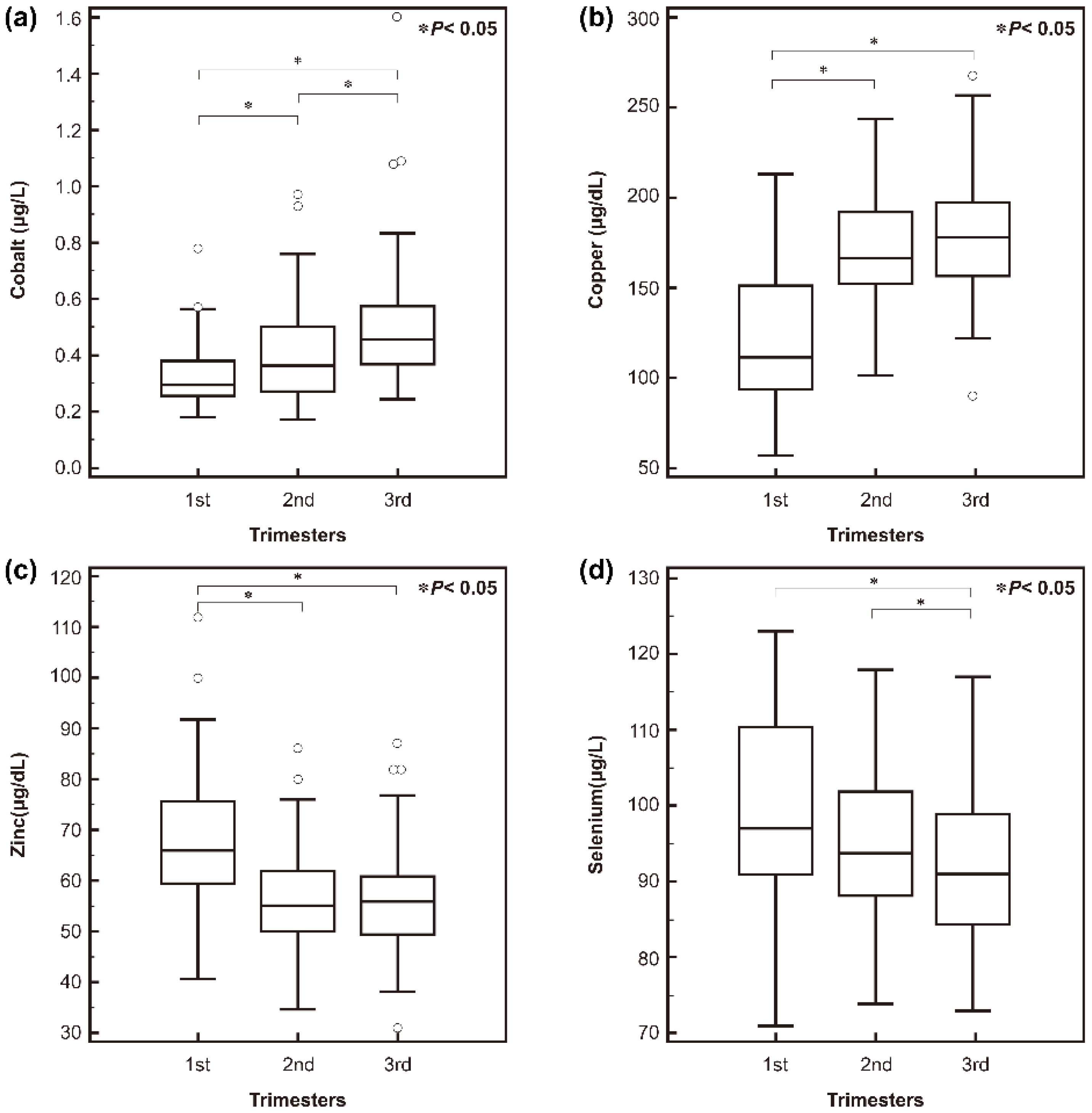
3.2. Serum Trace Element Levels in Korean Pregnant Women
3.3. Prevalence of High or Low Trace Elements Status in Korean Pregnant Women
3.4. Association between High or Low Trace Element Status and Pregnancy and Neonatal Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
References
- Burtis, C.A.; Ashwood, E.R.; Bruns, D.E. Tietz Textbook of Clinical Chemistry and Molecular Diagnostics, 5th ed.; Elsevier: St. Louis, MO, USA, 2012. [Google Scholar]
- Bettmer, J.; Bayon, M.M.; Encinar, J.R.; Sanchez, M.L.F.; de la Campa, M.D.R.F.; Medel, A.S. The emerging role of icp-ms in proteomic analysis. J. Proteom. 2009, 72, 989–1005. [Google Scholar] [CrossRef] [PubMed]
- Bolann, B.J.; Rahil-Khazen, R.; Henriksen, H.; Isrenn, R.; Ulvik, R.J. Evaluation of methods for trace-element determination with emphasis on their usability in the clinical routine laboratory. Scand. J. Clin. Lab. Investig. 2007, 67, 353–366. [Google Scholar] [CrossRef] [PubMed]
- Evans, D.M.; Zhu, G.; Dy, V.; Heath, A.C.; Madden, P.A.; Kemp, J.P.; McMahon, G.; St Pourcain, B.; Timpson, N.J.; Golding, J.; et al. Genome-wide association study identifies loci affecting blood copper, selenium and zinc. Hum. Mol. Genet. 2013, 22, 3998–4006. [Google Scholar] [CrossRef] [PubMed]
- Gibson, R.S. The role of diet- and host-related factors in nutrient bioavailability and thus in nutrient-based dietary requirement estimates. Food Nutr. Bull. 2007, 28, S77–S100. [Google Scholar] [CrossRef] [PubMed]
- Mocchegiani, E.; Giacconi, R.; Costarelli, L.; Muti, E.; Cipriano, C.; Tesei, S.; Pierpaoli, S.; Giuli, C.; Papa, R.; Marcellini, F.; et al. Zinc deficiency and IL-6 -174G/C polymorphism in old people from different European countries: Effect of zinc supplementation. Zincage study. Exp. Gerontol. 2008, 43, 433–444. [Google Scholar] [CrossRef] [PubMed]
- Freeland-Graves, J.H.; Sanjeevi, N.; Lee, J.J. Global perspectives on trace element requirements. J. Trace Elem. Med. Biol. 2015, 31, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Kilinc, M.; Coskun, A.; Bilge, F.; Imrek, S.S.; Atli, Y. Serum reference levels of selenium, zinc and copper in healthy pregnant women at a prenatal screening program in southeastern mediterranean region of turkey. J. Trace Elem. Med. Biol. 2010, 24, 152–156. [Google Scholar] [CrossRef] [PubMed]
- Otten, J.J.; Hellwig, J.P.; Meyers, L.D. Dri, Dietary Reference Intakes: The Essential Guide to Nutrient Requirements; National Academies Press: Washington, DC, USA, 2006. [Google Scholar]
- Cetin, I.; Berti, C.; Calabrese, S. Role of micronutrients in the periconceptional period. Hum. Reprod. Update 2010, 16, 80–95. [Google Scholar] [CrossRef] [PubMed]
- Mariath, A.B.; Bergamaschi, D.P.; Rondo, P.H.; Tanaka, A.C.; Hinnig Pde, F.; Abbade, J.F.; Diniz, S.G. The possible role of selenium status in adverse pregnancy outcomes. Br. J. Nutr. 2011, 105, 1418–1428. [Google Scholar] [CrossRef] [PubMed]
- Nassi, N.; Ponziani, V.; Becatti, M.; Galvan, P.; Donzelli, G. Anti-oxidant enzymes and related elements in term and preterm newborns. Pediatr. Int. 2009, 51, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Sievers, E.; Arpe, T.; Schleyerbach, U.; Garbe-Schonberg, D.; Schaub, J. Plasma selenium in preterm and term infants during the first 12 months of life. J. Trace Elem. Med. Biol. 2001, 14, 218–222. [Google Scholar] [CrossRef]
- Dobrzynski, W.; Trafikowska, U.; Trafikowska, A.; Pilecki, A.; Szymanski, W.; Zachara, B.A. Decreased selenium concentration in maternal and cord blood in preterm compared with term delivery. Analyst 1998, 123, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Mistry, H.D.; Wilson, V.; Ramsay, M.M.; Symonds, M.E.; Broughton Pipkin, F. Reduced selenium concentrations and glutathione peroxidase activity in preeclamptic pregnancies. Hypertension 2008, 52, 881–888. [Google Scholar] [CrossRef] [PubMed]
- Mistry, H.D.; Gill, C.A.; Kurlak, L.O.; Seed, P.T.; Hesketh, J.E.; Meplan, C.; Schomburg, L.; Chappell, L.C.; Morgan, L.; Poston, L. Association between maternal micronutrient status, oxidative stress, and common genetic variants in antioxidant enzymes at 15 weeks gestation in nulliparous women who subsequently develop preeclampsia. Free Radic. Biol. Med. 2015, 78, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Fritzsche, J.; Borisch, C.; Schaefer, C. Case report: High chromium and cobalt levels in a pregnant patient with bilateral metal-on-metal hip arthroplasties. Clin. Orthop. Relat. Res. 2012, 470, 2325–2331. [Google Scholar] [CrossRef] [PubMed]
- Al-Jameil, N.; Tabassum, H.; Al-Mayouf, H.; Aljohar, H.I.; Alenzi, N.D.; Hijazy, S.M.; Khan, F.A. Analysis of serum trace elements-copper, manganese and zinc in preeclamptic pregnant women by inductively coupled plasma optical emission spectrometry: A prospective case controlled study in Riyadh, Saudi Arabia. Int. J. Clin. Exp. Pathol. 2014, 7, 1900–1910. [Google Scholar] [PubMed]
- Keen, C.L.; Clegg, M.S.; Hanna, L.A.; Lanoue, L.; Rogers, J.M.; Daston, G.P.; Oteiza, P.; Uriu-Adams, J.Y. The plausibility of micronutrient deficiencies being a significant contributing factor to the occurrence of pregnancy complications. J. Nutr. 2003, 133, 1597S–1605S. [Google Scholar] [PubMed]
- Mori, R.; Ota, E.; Middleton, P.; Tobe-Gai, R.; Mahomed, K.; Miyazaki, C.; Bhutta, Z.A. Zinc supplementation for improving pregnancy and infant outcome. Cochrane Database Syst. Rev. 2012, 7, CD000230. [Google Scholar]
- TePoel, M.R.; Saftlas, A.F.; Wallis, A.B. Association of seasonality with hypertension in pregnancy: A systematic review. J. Reprod. Immunol. 2011, 89, 140–152. [Google Scholar] [CrossRef] [PubMed]
- Jiang, T.; Christian, P.; Khatry, S.K.; Wu, L.; West, K.P., Jr. Micronutrient deficiencies in early pregnancy are common, concurrent, and vary by season among rural Nepali pregnant women. J. Nutr. 2005, 135, 1106–1112. [Google Scholar] [PubMed]
- Reyes, H.; Baez, M.E.; Gonzalez, M.C.; Hernandez, I.; Palma, J.; Ribalta, J.; Sandoval, L.; Zapata, R. Selenium, zinc and copper plasma levels in intrahepatic cholestasis of pregnancy, in normal pregnancies and in healthy individuals, in Chile. J. Hepatol. 2000, 32, 542–549. [Google Scholar] [CrossRef]
- Bath, S.C.; Furmidge-Owen, V.L.; Redman, C.W.; Rayman, M.P. Gestational changes in iodine status in a cohort study of pregnant women from the United Kingdom: Season as an effect modifier. Am. J. Clin. Nutr. 2015, 101, 1180–1187. [Google Scholar] [CrossRef] [PubMed]
- Coustan, D.R.; Carpenter, M.W. The diagnosis of gestational diabetes. Diabetes Care 1998, 21 (Suppl. 2), B5–B8. [Google Scholar] [CrossRef] [PubMed]
- Vest, A.R.; Cho, L.S. Hypertension in pregnancy. Curr. Atheroscler. Rep. 2014, 16, 395. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Oh, H.J.; Choi, Y.H.; Kim, J.W.; Kim, S.H. Trace metal analysis using inductively coupled plasma-mass spectrometry (ICP-MS). Korean J. Lab. Med. 2004, 24, 362–370. [Google Scholar]
- Tabrizi, F.M.; Pakdel, F.G. Serum level of some minerals during three trimesters of pregnancy in Iranian women and their newborns: A longitudinal study. Indian J. Clin. Biochem. 2014, 29, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Tande, D.L.; Ralph, J.L.; Johnson, L.K.; Scheett, A.J.; Hoverson, B.S.; Anderson, C.M. First trimester dietary intake, biochemical measures, and subsequent gestational hypertension among nulliparous women. J. Midwifery Women’s Health 2013, 58, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Awadallah, S.; Abu-Elteen, K.; Elkarmi, A.; Qaraein, S.; Salem, N.; Mubarak, M. Maternal and cord blood serum levels of zinc, copper, and iron in healthy pregnant Jordanian women. J. Trace Elem. Exp. Med. 2004, 17, 1–8. [Google Scholar] [CrossRef]
- Louro, M.O.; Cocho, J.A.; Tutor, J.C. Assessment of copper status in pregnancy by means of determining the specific oxidase activity of ceruloplasmin. Clin. Chim. Acta Int. J. Clin. Chem. 2001, 312, 123–127. [Google Scholar] [CrossRef]
- Izquierdo Alvarez, S.; Castanon, S.G.; Ruata, M.L.; Aragues, E.F.; Terraz, P.B.; Irazabal, Y.G.; Gonzalez, E.G.; Rodriguez, B.G. Updating of normal levels of copper, zinc and selenium in serum of pregnant women. J. Trace Elem. Exp. Med. 2007, 21 (Suppl. 1), 49–52. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Yuan, E.; Liu, J.; Lou, X.; Jia, L.; Li, X.; Zhang, L. Gestational age-specific reference intervals for blood copper, zinc, calcium, magnesium, iron, lead, and cadmium during normal pregnancy. Clin. Biochem. 2013, 46, 777–780. [Google Scholar] [CrossRef] [PubMed]
- Foster, W.G.; Cheung, A.P.; Davis, K.; Graves, G.; Jarrell, J.; Leblanc, A.; Liang, C.L.; Leech, T.; Walker, M.; Weber, J.P.; et al. Circulating metals and persistent organic pollutant concentrations in Canadian and non-Canadian born primiparous women from five Canadian centres: Results of a pilot biomonitoring study. Sci. Total Environ. 2012, 435–436, 326–336. [Google Scholar] [CrossRef] [PubMed]
- Callan, A.C.; Hinwood, A.L.; Ramalingam, M.; Boyce, M.; Heyworth, J.; McCafferty, P.; Odland, J.O. Maternal exposure to metals-concentrations and predictors of exposure. Environ. Res. 2013, 126, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Silberstein, T.; Saphier, M.; Mashiach, Y.; Paz-Tal, O.; Saphier, O. Elements in maternal blood and amniotic fluid determined by ICP-MS. J. Mater. Fetal Neonatal Med. 2015, 28, 88–92. [Google Scholar] [CrossRef] [PubMed]
- Vigeh, M.; Yokoyama, K.; Ramezanzadeh, F.; Dahaghin, M.; Sakai, T.; Morita, Y.; Kitamura, F.; Sato, H.; Kobayashi, Y. Lead and other trace metals in preeclampsia: A case-control study in Tehran, Iran. Environ. Res. 2006, 100, 268–275. [Google Scholar] [CrossRef] [PubMed]
- Blumfield, M.L.; Hure, A.J.; Macdonald-Wicks, L.; Smith, R.; Collins, C.E. A systematic review and meta-analysis of micronutrient intakes during pregnancy in developed countries. Nutr. Rev. 2013, 71, 118–132. [Google Scholar] [CrossRef] [PubMed]
- Hansen, S.; Nieboer, E.; Sandanger, T.M.; Wilsgaard, T.; Thomassen, Y.; Veyhe, A.S.; Odland, J.O. Changes in maternal blood concentrations of selected essential and toxic elements during and after pregnancy. J. Environ. Monit. 2011, 13, 2143–2152. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Yang, H.; Shi, H.; Shen, C.; Zhou, W.; Dai, Q.; Jiang, Y. Blood copper, zinc, calcium, and magnesium levels during different duration of pregnancy in Chinese. Biol. Trace Elem. Res. 2010, 135, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Donangelo, C.M.; King, J.C. Maternal zinc intakes and homeostatic adjustments during pregnancy and lactation. Nutrients 2012, 4, 782–798. [Google Scholar] [CrossRef] [PubMed]
- Horton, D.K.; Adetona, O.; Aguilar-Villalobos, M.; Cassidy, B.E.; Pfeiffer, C.M.; Schleicher, R.L.; Caldwell, K.L.; Needham, L.L.; Rathbun, S.L.; Vena, J.E.; et al. Changes in the concentrations of biochemical indicators of diet and nutritional status of pregnant women across pregnancy trimesters in Trujillo, Peru, 2004–2005. Nutr. J. 2013, 12, 80. [Google Scholar] [CrossRef] [PubMed]
- Mihailovic, M.; Cvetkovic, M.; Ljubic, A.; Kosanovic, M.; Nedeljkovic, S.; Jovanovic, I.; Pesut, O. Selenium and malondialdehyde content and glutathione peroxidase activity in maternal and umbilical cord blood and amniotic fluid. Biol. Trace Elem. Res. 2000, 73, 47–54. [Google Scholar] [CrossRef]
- Zachara, B.A.; Wardak, C.; Didkowski, W.; Maciag, A.; Marchaluk, E. Changes in blood selenium and glutathione concentrations and glutathione peroxidase activity in human pregnancy. Gynecol. Obstet. Investig. 1993, 35, 12–17. [Google Scholar] [CrossRef]
- Okubo, H.; Miyake, Y.; Sasaki, S.; Tanaka, K.; Murakami, K.; Hirota, Y. Nutritional adequacy of three dietary patterns defined by cluster analysis in 997 pregnant Japanese women: The Osaka maternal and child health study. Public Health Nutr. 2011, 14, 611–621. [Google Scholar] [CrossRef] [PubMed]
- Sarwar, M.S.; Ahmed, S.; Ullah, M.S.; Kabir, H.; Rahman, G.K.; Hasnat, A.; Islam, M.S. Comparative study of serum zinc, copper, manganese, and iron in preeclamptic pregnant women. Biol. Trace Elem. Res. 2013, 154, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Kang, Y.; Zhang, M. A meta-analysis of copper level and risk of preeclampsia: Evidence from 12 publications. Biosci. Rep. 2016, 36. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.J.; Park, S.K.; Lim, H.S.; Ko, K.P.; Ahn, Y.; Ahn, Y.O. Seasonal variation of food intake in food frequency questionnaire among workers in a nuclear power plant. J. Prev. Med. Public Health 2007, 40, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Ko, Y.S.; Ahn, H.S. Seasonal difference of nutrient intake, serum lipid and antioxidative index in female college students. Korean J. Community Nutr. 2007, 12, 142–149. [Google Scholar]
- Mistry, H.D.; Kurlak, L.O.; Young, S.D.; Briley, A.L.; Pipkin, F.B.; Baker, P.N.; Poston, L. Maternal selenium, copper and zinc concentrations in pregnancy associated with small-for-gestational-age infants. Matern. Child Nutr. 2014, 10, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Ramakrishnan, U.; Grant, F.; Goldenberg, T.; Zongrone, A.; Martorell, R. Effect of women’s nutrition before and during early pregnancy on maternal and infant outcomes: A systematic review. Paediatr. Perinat. Epidemiol. 2012, 26 (Suppl. 1), 285–301. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Hu, Y.F.; Hao, J.H.; Chen, Y.H.; Su, P.Y.; Wang, Y.; Yu, Z.; Fu, L.; Xu, Y.Y.; Zhang, C.; et al. Maternal zinc deficiency during pregnancy elevates the risks of fetal growth restriction: A population-based birth cohort study. Sci. Rep. 2015, 5, 11262. [Google Scholar] [CrossRef] [PubMed]
- Uriu-Adams, J.Y.; Keen, C.L. Zinc and reproduction: Effects of zinc deficiency on prenatal and early postnatal development. Birth Defects Res. B Dev. Reprod. Toxicol. 2010, 89, 313–325. [Google Scholar] [CrossRef] [PubMed]
- Schulpis, K.H.; Karakonstantakis, T.; Vlachos, G.D.; Mentis, A.F.; Karikas, G.A.; Afordakou, D.; Papastamataki, M.; Antsaklis, A.; Papassotiriou, I. Maternal-neonatal magnesium and zinc serum concentrations after vaginal delivery. Scand. J. Clin. Lab. Investig. 2010, 70, 465–469. [Google Scholar] [CrossRef] [PubMed]
- Lazebnik, N.; Kuhnert, B.R.; Kuhnert, P.M.; Thompson, K.L. Zinc status, pregnancy complications, and labor abnormalities. Am. J. Obstet. Gynecol. 1988, 158, 161–166. [Google Scholar] [CrossRef]
- Ota, E.; Mori, R.; Middleton, P.; Tobe-Gai, R.; Mahomed, K.; Miyazaki, C.; Bhutta, Z.A. Zinc supplementation for improving pregnancy and infant outcome. Cochrane Database Syst. Rev. 2015, 2, CD000230. [Google Scholar]
- Lee, Y.A.; Hwang, J.Y.; Kim, H.; Ha, E.H.; Park, H.; Ha, M.; Kim, Y.; Hong, Y.C.; Chang, N. Relationships of maternal zinc intake from animal foods with fetal growth. Br. J. Nutr. 2011, 106, 237–242. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Total (n = 245) | 1st Trimester (n = 52) | 2nd Trimester (n = 97) | 3rd Trimester (n = 96) | p | ||||
|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | ||
| Season | 0.10 | ||||||||
| Spring | 110 | 44.9% | 22 | 20.0% | 39 | 35.5% | 49 | 44.5% | |
| Summer | 25 | 10.2% | 6 | 24.0% | 10 | 40.0% | 9 | 36.0% | |
| Fall | 94 | 38.4% | 18 | 19.1% | 39 | 41.5% | 37 | 39.4% | |
| Winter | 16 | 6.5% | 6 | 37.5% | 9 | 56.3% | 1 | 6.3% | |
| Education level | 1.0 | ||||||||
| ≤12 years | 11 | 4.5% | 2 | 18.2% | 5 | 45.5% | 4 | 36.4% | |
| >12 years | 234 | 95.5% | 50 | 21.4% | 92 | 39.3% | 92 | 39.3% | |
| Jobs | 0.94 | ||||||||
| Any job | 167 | 68.2% | 36 | 21.6% | 67 | 40.1% | 64 | 38.3% | |
| Homemaker | 78 | 31.8% | 16 | 20.5% | 30 | 38.5% | 32 | 41.0% | |
| Type of current pregnancy | 0.15 | ||||||||
| Spontaneous pregnancy | 239 | 97.6% | 52 | 21.8% | 92 | 38.5% | 95 | 39.7% | |
| Artificial pregnancy | 6 | 2.4% | 0 | 0.0% | 5 | 83.3% | 1 | 16.7% | |
| Parity | 0.53 | ||||||||
| 0 (nullipara) | 151 | 61.6% | 32 | 21.2% | 56 | 37.1% | 63 | 41.7% | |
| ≥1 | 94 | 38.4% | 20 | 21.3% | 41 | 43.6% | 33 | 35.1% | |
| Pregnant Women (n = 245) | Healthy Non-Pregnant Women (n = 227) | Healthy Men (n = 300) | p a | ||||
|---|---|---|---|---|---|---|---|
| Median | Interquartile Range | Median | Interquartile Range | Median | Interquartile Range | ||
| Cobalt (μg/L) bcd | 0.39 | (0.29–0.53) | 0.36 | (0.25–0.51) | 0.30 | (0.18–0.45) | <0.0001 |
| Copper (μg/dL) bcd | 165.0 | (144.0–187.0) | 100.0 | (86.3–120.0) | 91.5 | (81.0–105.5) | <0.0001 |
| Zinc (μg/dL) bc | 57.0 | (50.0–64.0) | 92.0 | (84.0–104.8) | 92.0 | (82.0–103.0) | <0.0001 |
| Selenium (μg/L) bcd | 94.0 | (89.0–101.0) | 140.0 | (120.0–171.8) | 150.0 | (127.5–179.0) | <0.0001 |
| Pregnancy and Neonatal Outcomes | Cobalt (μg/L) | Copper (μg/dL) | Zinc (μg/dL) | Selenium (μg/L) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| High (n = 9) | Not High (n = 236) | p a | p b | High (n = 172) | Not High (n = 73) | p a | p b | Low (n = 187) | Not Low (n = 58) | p a | p b | Low (n = 5) | Not Low (n = 240) | p a | p b | |
| Gestational diabetes, n (%) | 0 (0) | 18 (7.6) | 0.76 | 0.80 | 15 (8.7) | 3 (4.1) | 0.22 | 0.45 | 15 (8.0) | 3 (5.2) | 0.47 | 0.58 | 0 (0) | 18 (7.5) | 0.96 | 0.79 |
| Preeclampsia, n (%) | 0 (0) | 5 (2.1) | 0.62 | 0.43 | 2 (1.2) | 3 (4.1) | 0.16 | 0.03 | 5 (2.7) | 0 (0) | 0.40 | 0.54 | 0 (0) | 5 (2.1) | 0.42 | 0.44 |
| Gestational age at delivery, weeks, median | 39.6 | 39.5 | 0.43 | 0.27 | 39.4 | 39.6 | 0.37 | 0.99 | 39.6 | 39.5 | 0.88 | 0.44 | 39.6 | 39.4 | 0.39 | 0.64 |
| Baby weight, g, median | 3540 | 3180 | 0.08 | 0.03 | 3180 | 3190 | 0.76 | 0.47 | 3180 | 3175 | 0.59 | 0.30 | 3440 | 3180 | 0.04 | 0.03 |
| Preterm, n (%) | 0 (0) | 11 (4.7) | 0.98 | 0.65 | 10 (5.8) | 1 (1.4) | 0.16 | 0.18 | 7 (3.7) | 4 (6.9) | 0.32 | 0.66 | 0 (0) | 11 (4.6) | 0.72 | 0.64 |
| Low birth weight, n (%) | 0 (0) | 9 (3.8) | 0.88 | 0.94 | 6 (3.5) | 3 (4.1) | 0.81 | 0.72 | 8 (4.3) | 1 (1.7) | 0.38 | 0.56 | 0 (0) | 9 (3.8) | 0.63 | 0.97 |
| Small for gestational age, n (%) | 1 (11.1) | 35 (14.8) | 0.76 | 0.40 | 27 (15.7) | 9 (12.3) | 0.50 | 0.80 | 31 (16.6) | 5 (8.6) | 0.14 | 0.19 | 0 (0) | 36 (15.0) | 0.68 | 0.50 |
| Congenital abnormality, n (%) | 0 (0) | 14 (5.9) | 0.89 | 0.83 | 10 (5.8) | 4 (5.5) | 0.92 | 0.84 | 11 (5.9) | 3 (5.2) | 0.84 | 0.94 | 0 (0) | 14 (5.8) | 0.83 | 0.95 |
| Ethnicity | Method | Specimen | Preg All | 1st Trimester | 2nd Trimester | 3rd Trimester | Healthy Non-Pregnant Women | Healthy Men | Reference | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | n | conc. | n | conc. | n | conc. | n | conc. | n | conc. | |||||
| Cobalt (μg/L) | Korean | ICP-MS | Serum | 245 | 52 | 0.30 a | 97 | 0.36 a | 96 | 0.46 a | 227 | 0.36 a | 300 | 0.30 a | This study |
| Copper (μg/dL) | Korean | ICP-MS | Serum | 245 | 52 | 112.0 a | 97 | 167.0 a | 96 | 178.0 a | 227 | 100.0 a | 300 | 91.5 a | This study |
| Iranian | ICP-MS | Serum | 162 | 162 | 130.9 ± 43.5 | 162 | 172 ± 38.94 | 162 | 193.2 ± 28.5 | - | - | - | - | [28] | |
| USA d | ICP-OES | Serum | 44 | 44 | 168.5 ± 5.18 b | - | - | - | - | - | - | - | - | [29] | |
| Jordanian | AAS | Serum | 186 | 52 | 175 ± 42 | 42 | 226 ± 51 | 92 | 236 ± 36 | - | - | - | - | [30] | |
| Turkish | AAS | Serum | 351 | 177 | 132.33 ± 38.24 | 174 | 164.86 ± 39.69 | - | - | 30 | 104.75 ± 39.14 | 30 | 78.29 ± 20.90 | [8] | |
| Spanish | AAS | Serum | 52 | 52 | 217.1 ± 4.9 b | - | - | - | - | 50 | 106.9 ± 2.8 b | - | - | [31] | |
| Spanish | AAS | Serum | 159 | 73 | 147.5 ± 34.6 | 30 | 197.1 ± 24.0 | GA 25–35 wk: 18 GA >35 wk: 38 | 195.1 ± 35.0 204.2 ± 41.8 | - | - | - | - | [32] | |
| Chinese | AAS | Blood | 2380 | 550 | 102.6 a | GA 13–20 wk: 552 GA 21–27 wk: 600 | 130.2 a 135.6 a | GA 28–35 wk: 553 GA 36–42 wk: 125 | 136.6 a 145.2 a | 552 | 83.5 a | - | - | [33] c | |
| Chilean | AAS | Plasma | 98 | - | - | - | - | GA 27–32 wk: 34 GA 33–35 wk: 47 GA >36 wk: 45 | 203.0 ± 39.9 217.7 ± 37.2 218.2 ± 45.2 | 29 | 131.0 ± 21.2 | - | - | [23] c | |
| Zinc (μg/dL) | Korean | ICP-MS | Serum | 245 | 52 | 66.0 a | 97 | 55.0 a | 96 | 94.0 a | 227 | 92.0 a | 300 | 92.0 a | This study |
| Iranian | ICP-MS | Serum | 162 | 162 | 79.5 ± 15 | 162 | 74.5 ± 16.1 | 162 | 65.3 ± 14.9 | - | - | - | - | [28] | |
| USA d | ICP-OES | Serum | 44 | 44 | 78.9 ± 2.15 b | - | - | - | - | - | - | - | - | [29] | |
| Jordanian | AAS | Serum | 186 | 52 | 77.0 ± 16.0 | 42 | 73.0 ± 14.0 | 92 | 68.0 ± 10.0 | - | - | - | - | [30] | |
| Turkish | AAS | Serum | 351 | 177 | 81.30 ± 31.94 | 174 | 74.25 ± 22.47 | - | - | 30 | 121.41 ± 29.22 | 30 | 134.85 ± 15.95 | [8] | |
| Spanish | AAS | Serum | 159 | 73 | 71.3 ± 12.9 | 30 | 61.1 ± 8.6 | GA 25–35 wk: 18 GA >35 wk: 38 | 59.8 ± 10.0 58.5 ± 11.5 | - | - | - | - | [32] | |
| Chinese | AAS | Blood | 2380 | 550 | 83.3 a | GA 13–20 wk: 552 GA 21–27 wk: 600 | 81.75 a 78.95 a | GA 28–35 wk: 553 GA 36–42 wk: 125 | 79.95 a 81.2 a | 552 | 83.1 a | - | 83.1 a | [33] | |
| Chilean | AAS | Plasma | 98 | - | - | - | - | GA 27–32 wk: 34 GA 33–35 wk: 47 GA >36 wk: 45 | 105.9 ± 33.3 110.1 ± 34.1 117.0 ± 23.6 | 29 | 128.8 ± 21.0 | - | - | [23] c | |
| Selenium (μg/L) | Korean | ICP-MS | Serum | 245 | 52 | 97.0 a | 97 | 94.0 a | 96 | 91.0 a | 227 | 140.0 a | 300 | 150.0 a | This study |
| Turkish | AAS | Serum | 351 | 177 | 44.85 ± 9.23 | 174 | 47.18 ± 10.92 | - | - | 30 | 55.38 ± 8.81 | 30 | 72.24 ± 9.28 | [8] | |
| Spanish | AAS | Serum | 159 | 73 | 108.6 ± 20.1 | 30 | 99.0 ± 24.4 | GA 25–35 wk: 18 GA >35 wk: 38 | 87.1 ± 16.1 85.5 ± 12.8 | - | - | - | - | [32] | |
| UK Whites | AAS | Serum | 27 | - | - | - | - | Before delivery: 27 | 58.4 ± 14.9 | 22 | 69.8 ± 11.7 | - | - | [15] | |
| Chilean | AAS | Plasma | 98 | - | - | - | - | GA 27–32 wk: 34 GA 33–35 wk: 47 GA >36 wk: 45 | 100.0 ± 16.5 90.6 ± 15.7 85.1 ± 19.7 | 29 | 112.6 ± 26.8 | - | - | [23] c | |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, R.; Sun, J.; Yoo, H.; Kim, S.; Cho, Y.Y.; Kim, H.J.; Kim, S.W.; Chung, J.H.; Oh, S.-y.; Lee, S.-Y. A Prospective Study of Serum Trace Elements in Healthy Korean Pregnant Women. Nutrients 2016, 8, 749. https://doi.org/10.3390/nu8110749
Choi R, Sun J, Yoo H, Kim S, Cho YY, Kim HJ, Kim SW, Chung JH, Oh S-y, Lee S-Y. A Prospective Study of Serum Trace Elements in Healthy Korean Pregnant Women. Nutrients. 2016; 8(11):749. https://doi.org/10.3390/nu8110749
Chicago/Turabian StyleChoi, Rihwa, Jiyu Sun, Heejin Yoo, Seonwoo Kim, Yoon Young Cho, Hye Jeong Kim, Sun Wook Kim, Jae Hoon Chung, Soo-young Oh, and Soo-Youn Lee. 2016. "A Prospective Study of Serum Trace Elements in Healthy Korean Pregnant Women" Nutrients 8, no. 11: 749. https://doi.org/10.3390/nu8110749
APA StyleChoi, R., Sun, J., Yoo, H., Kim, S., Cho, Y. Y., Kim, H. J., Kim, S. W., Chung, J. H., Oh, S. -y., & Lee, S. -Y. (2016). A Prospective Study of Serum Trace Elements in Healthy Korean Pregnant Women. Nutrients, 8(11), 749. https://doi.org/10.3390/nu8110749