Abdominal Obesity and Lung Cancer Risk: Systematic Review and Meta-Analysis of Prospective Studies

Abstract
:1. Introduction
2. Materials and Methods
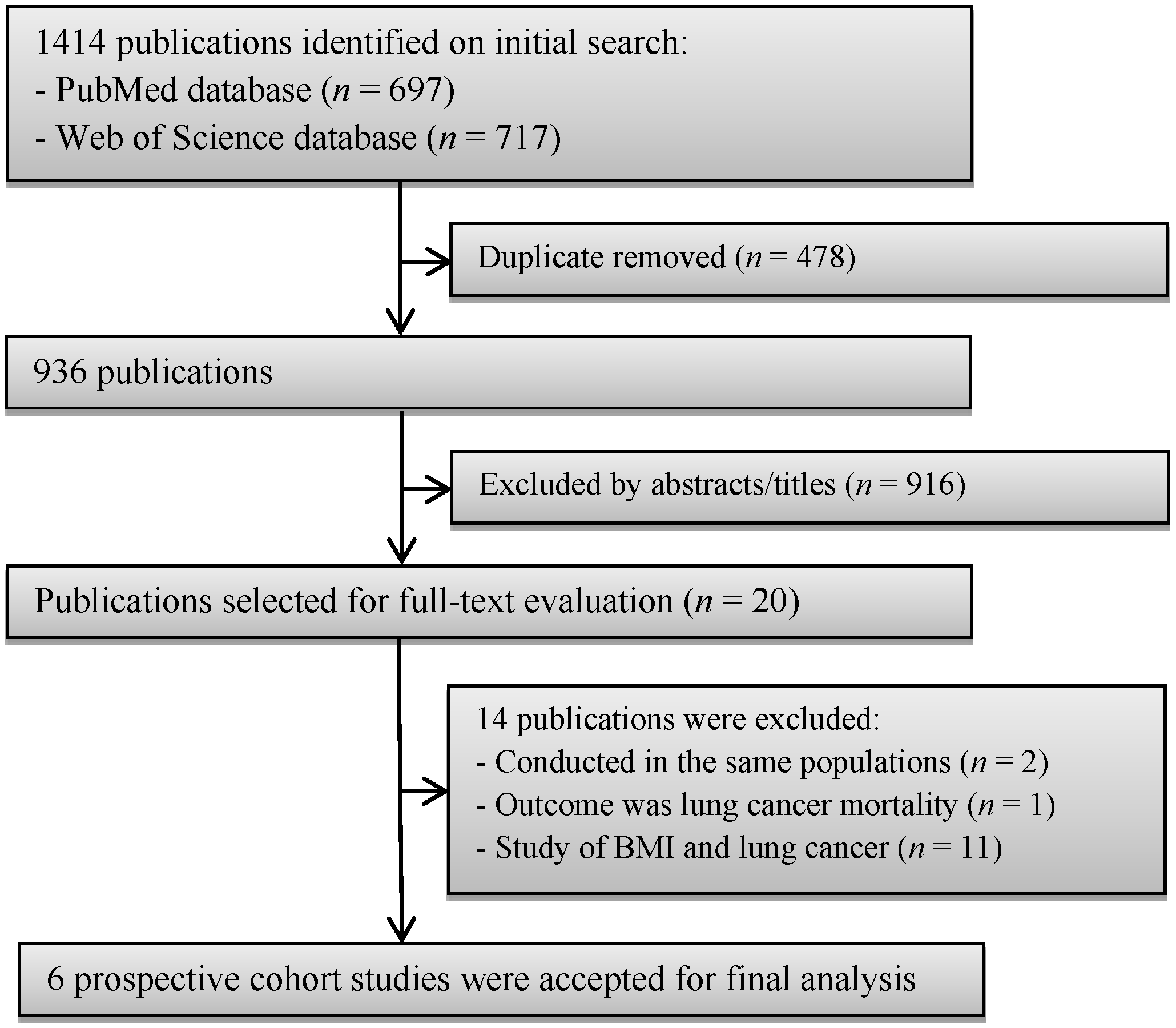
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction and Quality Assessment
2.4. Statistical Analysis
3. Results
3.1. Study Characteristics
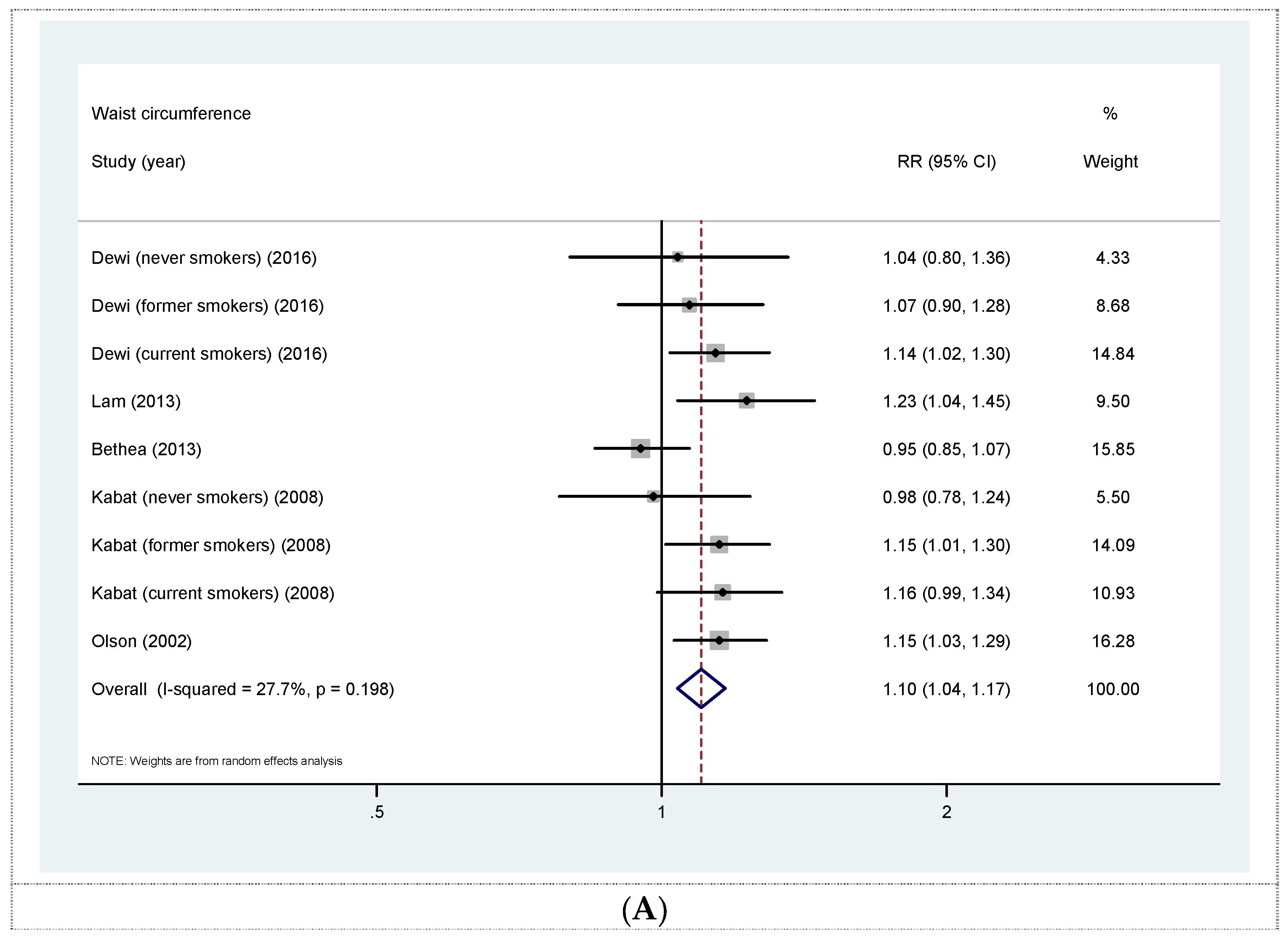
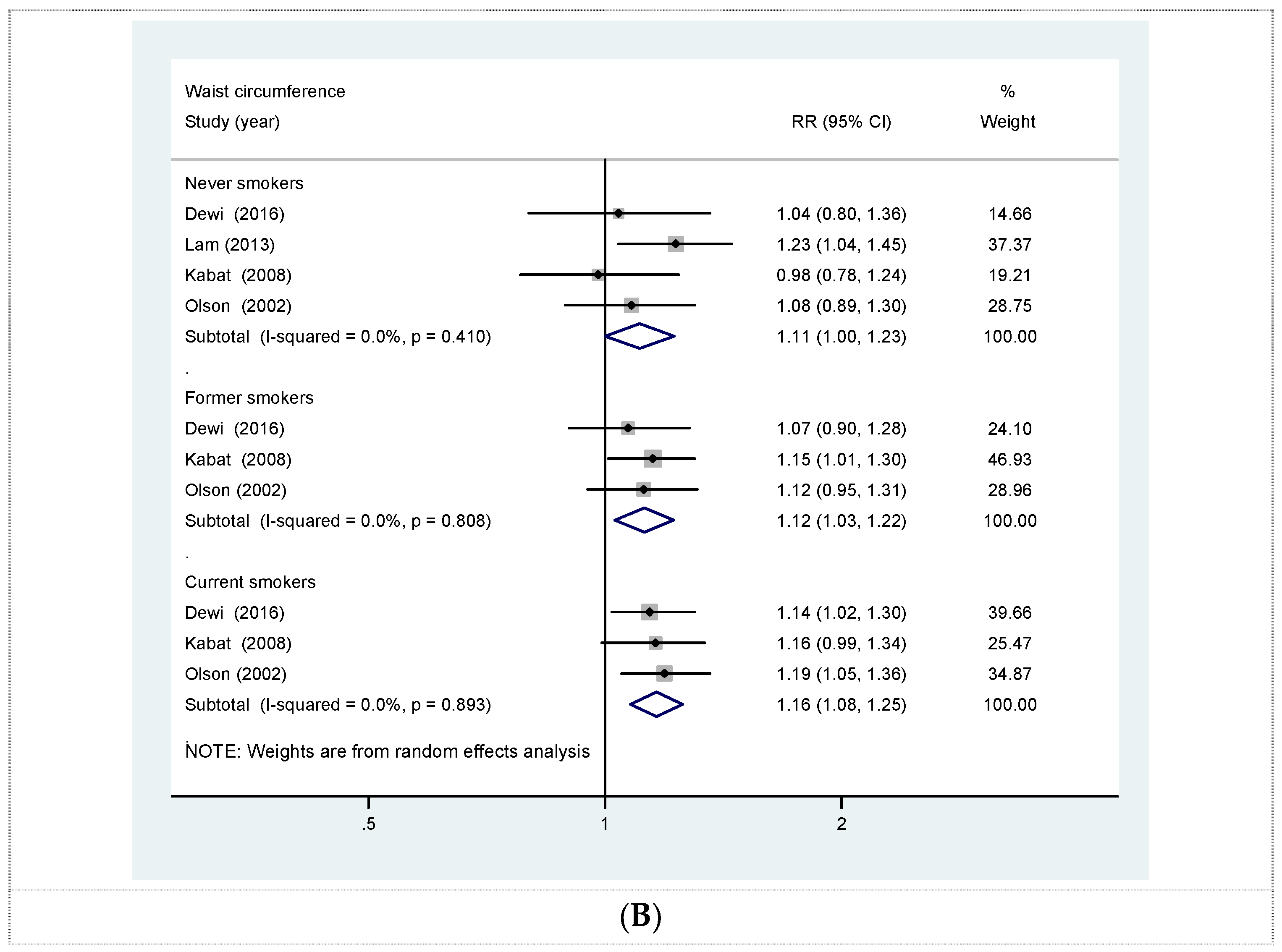
3.2. WC and Lung Cancer
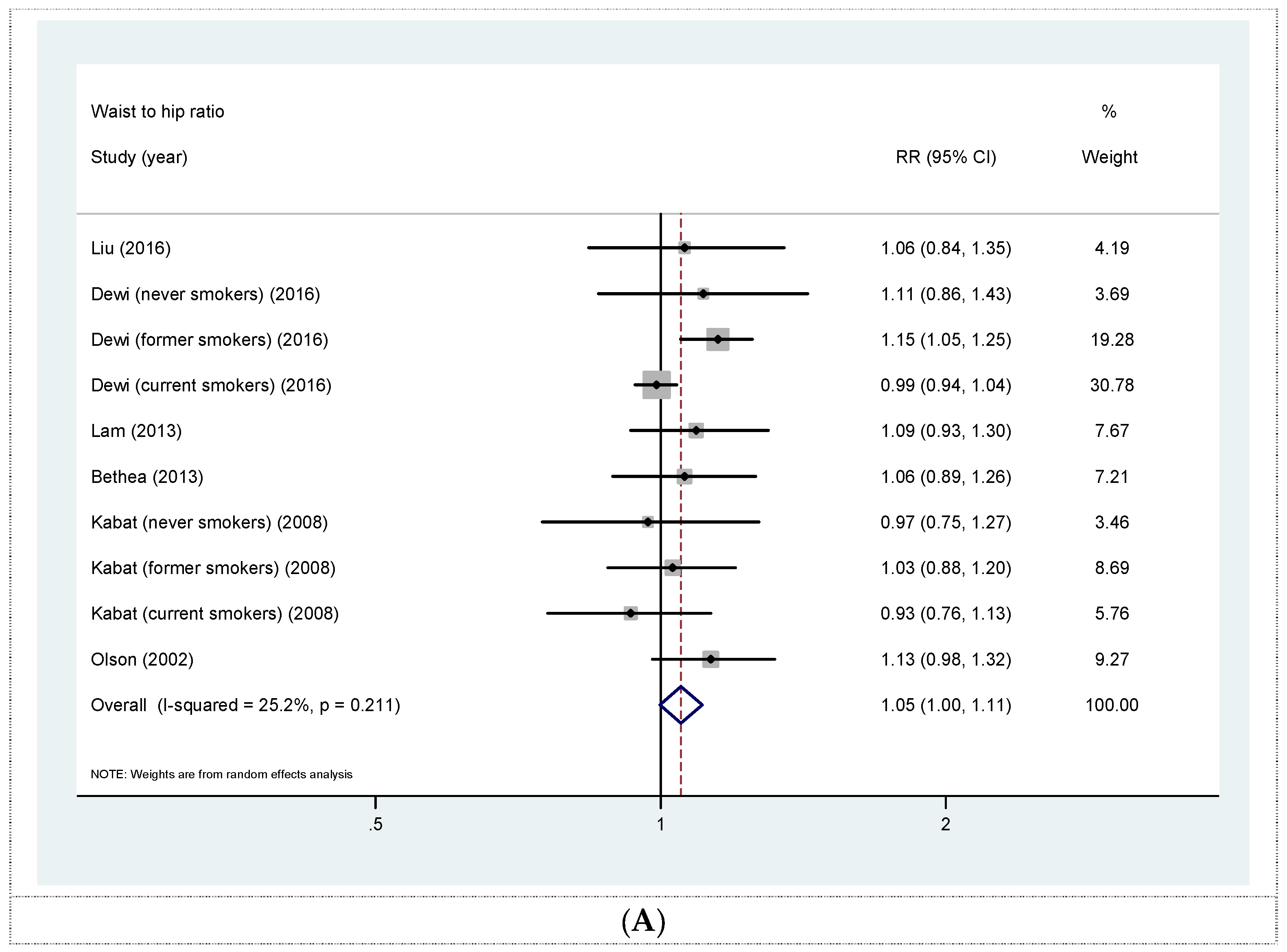
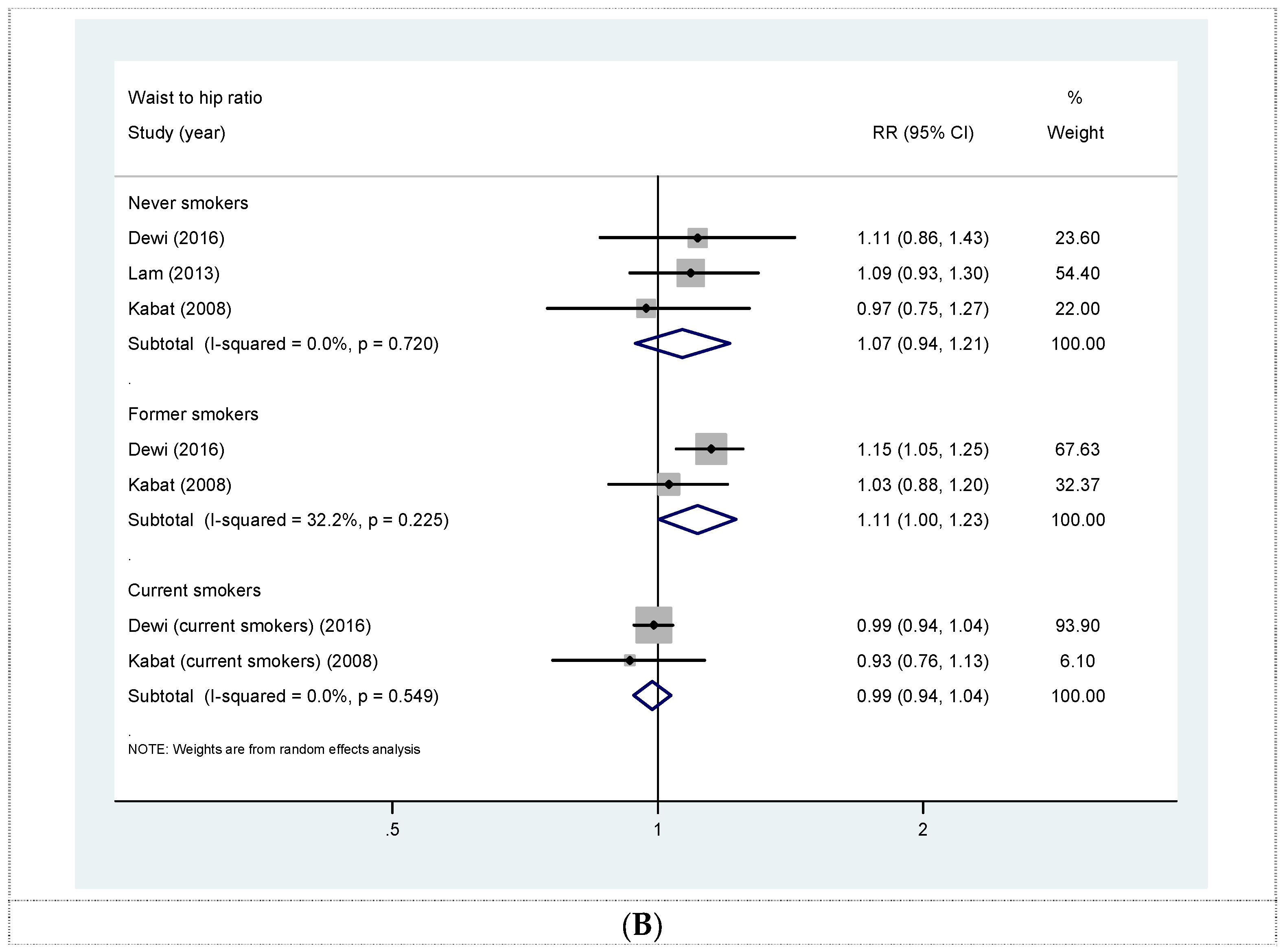
3.3. WHR and Lung Cancer
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.C.; Chen, S.J.; Zhang, R.; Hidayat, K.; Qin, J.B.; Zhang, Y.S.; Qin, L.Q. Central obesity and risks of pre- and postmenopausal breast cancer: A dose-response meta-analysis of prospective studies. Obes. Rev. 2016, 17, 1167–1177. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Yang, Y.; Wang, F.; Zhang, P.; Shi, C.; Zou, Y.; Qin, H. Obesity and risk of colorectal cancer: A systematic review of prospective studies. PLoS ONE 2013, 8, e53916. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Navarro Rosenblatt, D.A.; Chan, D.S.; Vingeliene, S.; Abar, L.; Vieira, A.R.; Greenwood, D.C.; Bandera, E.V.; Norat, T. Anthropometric factors and endometrial cancer risk: A systematic review and dose-response meta-analysis of prospective studies. Ann. Oncol. 2015, 26, 1635–1648. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Xu, Y. Body mass index and risk of renal cell cancer: A dose-response meta-analysis of published cohort studies. Int. J. Cancer 2014, 135, 1673–1686. [Google Scholar] [CrossRef] [PubMed]
- Xia, X.; Chen, W.; Li, J.; Chen, X.; Rui, R.; Liu, C.; Sun, Y.; Liu, L.; Gong, J.; Yuan, P. Body mass index and risk of breast cancer: A nonlinear dose-response meta-analysis of prospective studies. Sci. Rep. 2014, 4, 7480. [Google Scholar] [CrossRef] [PubMed]
- Genkinger, J.M.; Spiegelman, D.; Anderson, K.E.; Bernstein, L.; Van Den Brandt, P.A.; Calle, E.E.; English, D.R.; Folsom, A.R.; Freudenheim, J.L.; Fuchs, C.S.; et al. A pooled analysis of 14 cohort studies of anthropometric factors and pancreatic cancer risk. Int. J. Cancer 2011, 129, 1708–1717. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.; Cai, Q.; Chen, D.; Zhu, W.; Huang, W.; Li, Z. Abdominal obesity and the risk of colorectal adenoma: A meta-analysis of observational studies. Eur. J. Cancer Prev. 2012, 21, 523–531. [Google Scholar] [CrossRef] [PubMed]
- Turati, F.; Tramacere, I.; La Vecchia, C.; Negri, E. A meta-analysis of body mass index and esophageal and gastric cardia adenocarcinoma. Ann. Oncol. 2013, 24, 609–617. [Google Scholar] [CrossRef] [PubMed]
- Schmid, D.; Ricci, C.; Behrens, G.; Leitzmann, M.F. Adiposity and risk of thyroid cancer: A systematic review and meta-analysis. Obes. Rev. 2015, 16, 1042–1054. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.M.; Wu, Z.X.; Han, B.; Mao, Y.Q.; Chen, H.L.; Han, S.F.; Xia, J.L.; Wang, L.S. The association between BMI and gallbladder cancer risk: A meta-analysis. Oncotarget 2016, 7, 43669–43679. [Google Scholar] [CrossRef] [PubMed]
- Renehan, A.G.; Tyson, M.; Egger, M.; Heller, R.F.; Zwahlen, M. Body-mass index and incidence of cancer: A systematic review and meta-analysis of prospective observational studies. Lancet 2008, 371, 569–578. [Google Scholar] [CrossRef]
- Yang, Y.; Dong, J.; Sun, K.; Zhao, L.; Zhao, F.; Wang, L.; Jiao, Y. Obesity and incidence of lung cancer: A meta-analysis. Int. J. Cancer 2013, 132, 1162–1169. [Google Scholar] [CrossRef] [PubMed]
- Duan, P.; Hu, C.; Quan, C.; Yi, X.; Zhou, W.; Yuan, M.; Yu, T.; Kourouma, A.; Yang, K. Body mass index and risk of lung cancer: Systematic review and dose-response meta-analysis. Sci. Rep. 2015, 19, 16938. [Google Scholar] [CrossRef] [PubMed]
- Drinkard, C.R.; Sellers, T.A.; Potter, J.D.; Zheng, W.; Bostick, R.M.; Nelson, C.L.; Folsom, A.R. Association of body mass index and body fat distribution with risk of lung cancer in older women. Am. J. Epidemiol. 1995, 142, 600–607. [Google Scholar] [PubMed]
- Audrain-McGovern, J.; Benowitz, N. Cigarette smoking, nicotine, and body weight. Clin. Pharmacol. Ther. 2011, 90, 164–168. [Google Scholar] [CrossRef] [PubMed]
- Chiolero, A.; Faeh, D.; Paccaud, F.; Cornuz, J. Consequences of smoking for body weight, body fat distribution, and insulin resistance. Am. J. Clin. Nutr. 2008, 87, 801–809. [Google Scholar] [PubMed]
- Olson, J.E.; Yang, P.; Schmitz, K.; Vierkant, R.A.; Cerhan, J.R.; Sellers, T.A. Differential association of body mass index and fat distribution with three major histologic types of lung cancer: Evidence from a cohort of older women. Am. J. Epidemiol. 2002, 156, 606–615. [Google Scholar] [CrossRef] [PubMed]
- Kabat, G.C.; Kim, M.; Hunt, J.R.; Chlebowski, R.T.; Rohan, T.E. Body mass index and waist circumference in relation to lung cancer risk in the Women’s Health Initiative. Am. J. Epidemiol. 2008, 168, 158–169. [Google Scholar] [CrossRef] [PubMed]
- Lam, T.K.; Moore, S.C.; Brinton, L.A.; Smith, L.; Hollenbeck, A.R.; Gierach, G.L.; Freedman, N.D. Anthropometric measures and physical activity and the risk of lung cancer in never-smokers: A prospective cohort study. PLoS ONE 2013, 8, e70672. [Google Scholar] [CrossRef] [PubMed]
- Dewi, N.U.; Boshuizen, H.C.; Johansson, M.; Vineis, P.; Kampman, E.; Steffen, A.; Tjønneland, A.; Halkjær, J.; Overvad, K.; Severi, G.; et al. Anthropometry and the Risk of Lung Cancer in EPIC. Am. J. Epidemiol. 2016, 184, 129–139. [Google Scholar] [CrossRef] [PubMed]
- Leitzmann, M.F.; Moore, S.C.; Koster, A.; Harris, T.B.; Park, Y.; Hollenbeck, A.; Schatzkin, A. Waist circumference as compared with body-mass index in predicting mortality from specific causes. PLoS ONE 2011, 6, e18582. [Google Scholar] [CrossRef] [PubMed]
- Bethea, T.N.; Rosenberg, L.; Charlot, M.; O’Connor, G.T.; Adams-Campbell, L.L.; Palmer, J.R. Obesity in relation to lung cancer incidence in African American women. Cancer Causes Control 2013, 24, 1695–1703. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Warren Andersen, S.; Wen, W.; Gao, Y.T.; Lan, Q.; Rothman, N.; Ji, B.T.; Yang, G.; Xiang, Y.B.; Shu, X.O.; Zheng, W. Prospective cohort study of general and central obesity, weight change trajectory and risk of major cancers among Chinese women. Int. J. Cancer 2016, 139, 1461–1470. [Google Scholar] [CrossRef] [PubMed]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-Analysis of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 10 March 2016).
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Greenland, S.; Longnecker, M.P. Methods for trend estimation from summarized dose-response data, with applications to meta-analysis. Am. J. Epidemiol. 1992, 135, 1301–1309. [Google Scholar] [PubMed]
- Orsini, N.; Bellocco, R.; Greenland, S. Generalized least squares for trend estimation of summarized dose-response data. Stata J. 2006, 6, 40–57. [Google Scholar]
- Folsom, A.R.; Kushi, L.H.; Anderson, K.E.; Mink, P.J.; Olson, J.E.; Hong, C.P.; Sellers, T.A.; Lazovich, D.; Prineas, R.J. Associations of general and abdominal obesity with multiple health outcomes in older women: The Iowa Women’s Health Study. Arch. Intern. Med. 2000, 160, 2117–2128. [Google Scholar] [CrossRef] [PubMed]
- Kaye, S.A.; Folsom, A.R.; Prineas, R.J.; Potter, J.D.; Gapstur, S.M. The association of body fat distribution with lifestyle and reproductive factors in a population study of postmenopausal women. Int. J. Obes. 1990, 14, 583–591. [Google Scholar] [CrossRef]
- Shimokata, H.; Muller, D.C.; Andres, R. Studies in the distribution of body fat. III. Effects of cigarette smoking. JAMA 1989, 261, 1169–1173. [Google Scholar] [CrossRef] [PubMed]
- Barrett-Connor, E.; Khaw, K.T. Cigarette smoking and increased central adiposity. Ann. Intern. Med. 1989, 111, 783–787. [Google Scholar] [CrossRef] [PubMed]
- Soler, J.T.; Folsom, A.R.; Kaye, S.A.; Prineas, R.J. Associations of abdominal adiposity, fasting insulin, sex hormone binding globulin, and estrone with lipids and lipoproteins in post-menopausal women. Atherosclerosis 1989, 79, 21–27. [Google Scholar] [CrossRef]
- Mohamed-Ali, V.; Pinkney, J.H.; Coppack, S.W. Adipose tissue as an endocrine and paracrine organ. Int. J. Obes. Relat. Metab. Disord. 1998, 22, 1145–1158. [Google Scholar] [CrossRef] [PubMed]
- Wajchenberg, B.L. Subcutaneous and visceral adipose tissue: Their relation to the metabolic syndrome. Endocr. Rev. 2000, 21, 697–738. [Google Scholar] [CrossRef] [PubMed]
- Macauley, V.M.; Teale, J.D.; Everard, M.J.; Joshi, G.P.; Smith, I.E.; Millar, J.L. Somatomedin-C/insulin-like growth factor I is a potent mitogen for human small cell lung cancer. Br. J. Cancer 1988, 57, 91–93. [Google Scholar] [CrossRef]
- Ankrapp, D.P.; Bevan, D.R. Insulin-like growth factor I and human fibroblast-derived insulin-like growth factor-I stimulate the proliferation of human lung carcinoma cells in vitro. Cancer Res. 1993, 53, 3399–3404. [Google Scholar] [PubMed]
- Beattie, C.W.; Hansen, N.W.; Thomas, P.A. Steroid receptors in human lung cancer. Cancer Res. 1985, 45, 4206–4414. [Google Scholar] [PubMed]
- Cagle, P.T.; Mody, D.R.; Schwartz, M.R. Estrogen and progesterone receptors in bronchiogenic carcinoma. Cancer Res. 1990, 50, 6632–6635. [Google Scholar] [PubMed]
- Marquez-Garban, D.C.; Mah, V.; Alavi, M.; Maresh, E.L.; Chen, H.W.; Bagryanova, L.; Horvath, S.; Chia, D.; Garon, E.; Goodglick, L.; et al. Progesterone and estrogen receptor expression and activity in human non-small cell lung cancer. Steroids 2011, 76, 910–920. [Google Scholar] [CrossRef] [PubMed]
- Alberg, A.J.; Brock, M.V.; Samet, J.M. Epidemiology of lung cancer: Looking to the future. J. Clin. Oncol. 2005, 23, 3175–3185. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, D.R., Jr.; Gottenborg, S. Smoking and weight: The Minnesota Lipid Research Clinic. Am. J. Public Health 1981, 71, 391–396. [Google Scholar] [CrossRef] [PubMed]
- Wannamethee, S.G.; Shaper, A.G.; Walker, M. Weight change, body weight and mortality: The impact of smoking and ill health. Int. J. Epidemiol. 2001, 30, 777–786. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.W.; Keil, D.; Gold, E.J.; Williams, S.M.; Goulding, A. Body mass index, waist girth, and waist-to-hip ratio as indexes of total and regional adiposity in women: Evaluation using receiver operating characteristic curves. Am. J. Clin. Nutr. 1998, 67, 44–49. [Google Scholar] [PubMed]
- Hill, J.O.; Sidney, S.; Lewis, C.E.; Tolan, K.; Scherzinger, A.L.; Stamm, E.R. Racial differences in amounts of visceral adipose tissue in young adults: The CARDIA (Coronary Artery Risk Development in Young Adults) study. Am. J. Clin. Nutr. 1999, 69, 381–387. [Google Scholar] [PubMed]
- Janssen, I.; Heymsfield, S.B.; Allison, D.B.; Kotler, D.P.; Ross, R. Body mass index and waist circumference independently contribute to the prediction of nonabdominal, abdominal subcutaneous, and visceral fat. Am. J. Clin. Nutr. 2002, 75, 683–688. [Google Scholar] [PubMed]
- Neamat-Allah, J.; Wald, D.; Hüsing, A.; Teucher, B.; Wendt, A.; Delorme, S.; Dinkel, J.; Vigl, M.; Bergmann, M.M.; Feller, S. Validation of anthropometric indices of adiposity against whole-body magnetic resonance imaging—A study within the German European Prospective Investigation into Cancer and Nutrition (EPIC) cohorts. PLoS ONE 2014, 9, e91586. [Google Scholar] [CrossRef] [PubMed]
- Després, J.P.; Lemieux, I.; Bergeron, J.; Pibarot, P.; Mathieu, P.; Larose, E.; Rodés-Cabau, J.; Bertrand, O.F.; Poirier, P. Abdominal obesity and the metabolic syndrome: Contribution to global cardiometabolic risk. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 1039–1049. [Google Scholar] [CrossRef] [PubMed]
- Eyre, H.; Kahn, R.; Robertson, R.M.; Clark, N.G.; Doyle, C.; Hong, Y.; Gansler, T.; Glynn, T.; Smith, R.A.; Taubert, K.; et al. Preventing cancer, cardiovascular disease, and diabetes: A common agenda for the American Cancer Society, the American Diabetes Association, and the American Heart Association. Circulation 2004, 109, 3244–3255. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| References (Country) | Study Population (Age) | Duration of Follow-Up (Years) | Sample Size (Lung Cancer Cases) | Ascertainment of Adiposity | Measure of Adiposity | Categories, Highest vs. Lowest (Measurement Unit) | Adjusted RR (95% CI) | Adjustment for Anthropometric Variables | Adjustment for Confounders |
|---|---|---|---|---|---|---|---|---|---|
| Olson et al. 2002 (USA) [18] | Older women (55–69 years) | 13 | 38,006 (596) | Self-measured | WC | >99.0 cm vs. ≤75.56 cm | All: 1.76 (1.14, 2.73); never smokers: 1.43 (0.69, 2.97); former smokers: 1.62 (0.85, 3.09); current smokers: 1.83 (1.11, 3.01) | BMI, BMI at age 18 years, and height | Age, pack-years of smoking, smoking status, physical activity score, educational level, and beer consumption |
| WHR | >0.90 vs. ≤0.76 | 1.29 (0.96, 1.75) | |||||||
| Kabat et al. 2008 (USA) [19] | Postmenopausal women (50–79 years) | 8 | 161,809 (1365) | Trained | WC | ≥97.6 cm vs. <74.6 cm | Never smokers: 1.01 (0.45, 2.28); former smokers a: 1.50 (0.98, 2.31); current smokers b: 1.56 (0.91, 2.69) | Height and BMI 1 | Age, education, ethnicity, use of HRT, intakes of total fat, fruits, vegetables, alcohol, and total calories, physical activity, and study |
| WHR | ≥0.87 vs. <0.75 | Never smokers: 1.01 (0.64, 1.66); former smokers a: 1.02 (0.77, 1.35); current smokers b: 0.89 (0.62, 1.27) | |||||||
| Bethea et al. 2013 (USA) [23] | African American women (21–69 years) | 7 | 56,944 (323) | Self-measured | WC | >93.9 cm vs. <71.1 cm | 0.85 (0.54, 1.35) | BMI | Age, education, physical activity, alcohol consumption, parity, age at first birth, family history of lung cancer, geographic region, and pack-years of smoking |
| WHR | >0.87 vs. <0.71 | 1.27 (0.86, 1.87) | |||||||
| Lam et al. 2013 (USA) [20] | Never-smokers (50–71 years) | 11 | 158,415 (532) | Self-measured | WC | Men: 110.5 cm vs. 86.4 cm; women: 99.1 cm vs. 70.6 cm | 1.75 (1.09, 2.79) | BMI and hip circumference 1 | Age, education, ethnicity, alcohol consumption, vigorous physical activity, physical activity at work, and total caloric intake |
| WHR | Men: 1.02 vs. 0.88; women: 0.90 vs. 0.73 | 1.22 (0.83, 1.81) | |||||||
| Dewi et al. 2016 (European countries) [21] | Men and women (30–70 years) | 11 | 348,108 (2400) | Trained | WC | Men: ≥102 cm vs. <94 cm; women: ≥88 cm vs. <80 cm | Never smokers: 0.95 (0.54, 1.65); former smokers: 1.15 (0.80, 1.63); current smokers: 1.38 (1.10, 1.72) | Height and BMI 1 | The duration of smoking, the lifetime number of cigarettes smoked, the number of cigarettes smoked at baseline, educational level, physical activity level, fruit consumption, vegetable consumption, meat consumption, fat intake, and energy intake |
| WHR | Men: >1.00 vs. <0.95; women: >0.85 vs. <0.80 | Never smokers: 0.76 (0.1, 1.15); former smokers: 1.44 (1.14, 1.82); current smokers: 0.98 (0.85, 1.12) | |||||||
| Liu et al. 2016 (China) [24] | Shanghai women (40–70 years) | 15.1 | 68,253 (611) | Trained | WHR | >0.85 vs. ≤0.77 | 1.03 (0.77, 1.37) | BMI | Education, total energy intake, total vegetable and fruit intake, total meat intake, leisure-time physical activity, alcohol consumption, menopausal status, spouse smoking exposure, parity, and family history of cancer |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hidayat, K.; Du, X.; Chen, G.; Shi, M.; Shi, B. Abdominal Obesity and Lung Cancer Risk: Systematic Review and Meta-Analysis of Prospective Studies. Nutrients 2016, 8, 810. https://doi.org/10.3390/nu8120810
Hidayat K, Du X, Chen G, Shi M, Shi B. Abdominal Obesity and Lung Cancer Risk: Systematic Review and Meta-Analysis of Prospective Studies. Nutrients. 2016; 8(12):810. https://doi.org/10.3390/nu8120810
Chicago/Turabian StyleHidayat, Khemayanto, Xuan Du, Guochong Chen, Minhua Shi, and Bimin Shi. 2016. "Abdominal Obesity and Lung Cancer Risk: Systematic Review and Meta-Analysis of Prospective Studies" Nutrients 8, no. 12: 810. https://doi.org/10.3390/nu8120810
APA StyleHidayat, K., Du, X., Chen, G., Shi, M., & Shi, B. (2016). Abdominal Obesity and Lung Cancer Risk: Systematic Review and Meta-Analysis of Prospective Studies. Nutrients, 8(12), 810. https://doi.org/10.3390/nu8120810