Iron Supplementation during Pregnancy and Infancy: Uncertainties and Implications for Research and Policy

Abstract
:1. Introduction
2. Iron Needs: Considerations during Pregnancy and Infancy
3. Iron Homeostasis: Physiologic and Developmental Adaptations during Pregnancy and Infancy
4. Iron Status: Uncertainties in Assessment of Pregnant Women and Infants
4.1. Commonly Used Indicators
4.2. Analytic Challenges
4.3. Confounding
4.4. Linking Measures to Health Outcomes
5. U-Shaped Risk for Iron Status: Concerns for Pregnant Women and Young Infants
5.1. Left-Side of U-Shapes Risk Curve: Low Iron Status
5.2. Right-Side of U-Shaped Risk Curve: High Iron Status
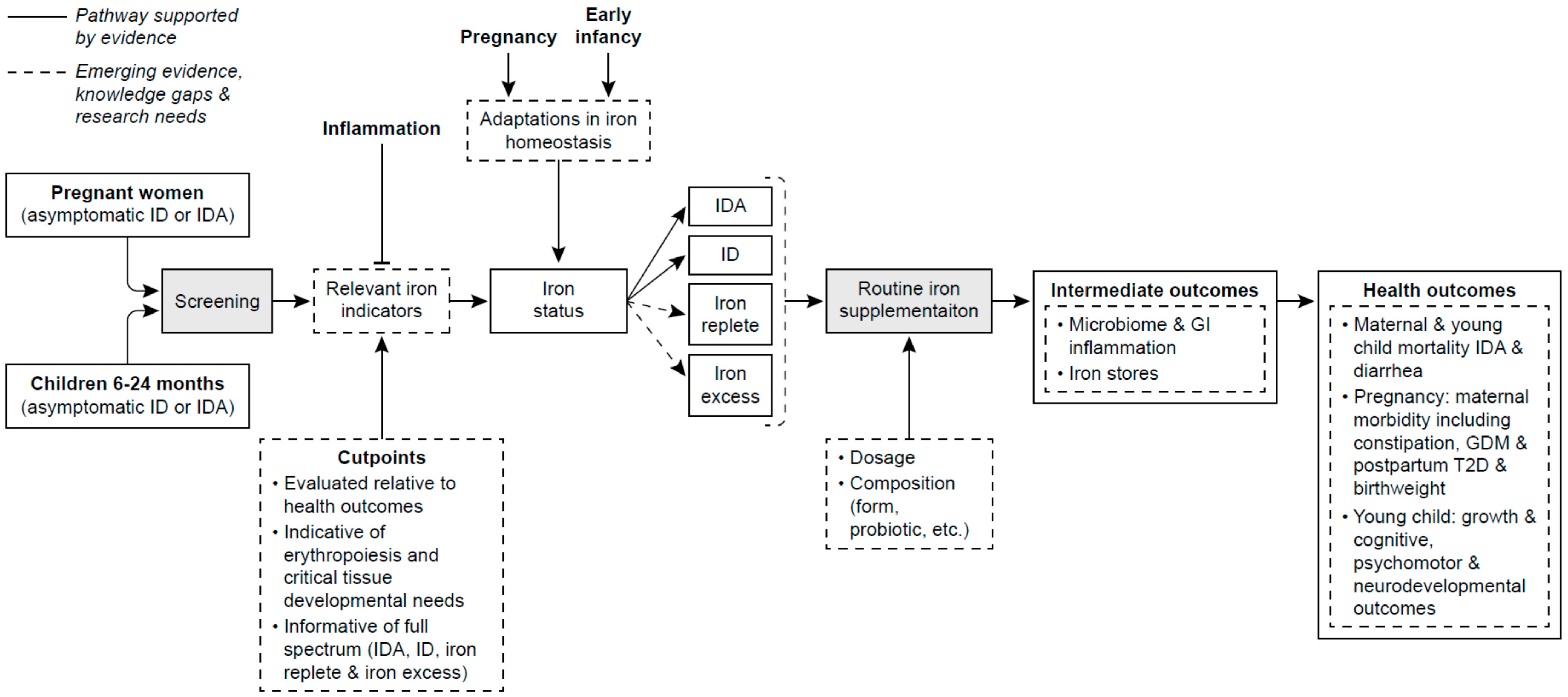
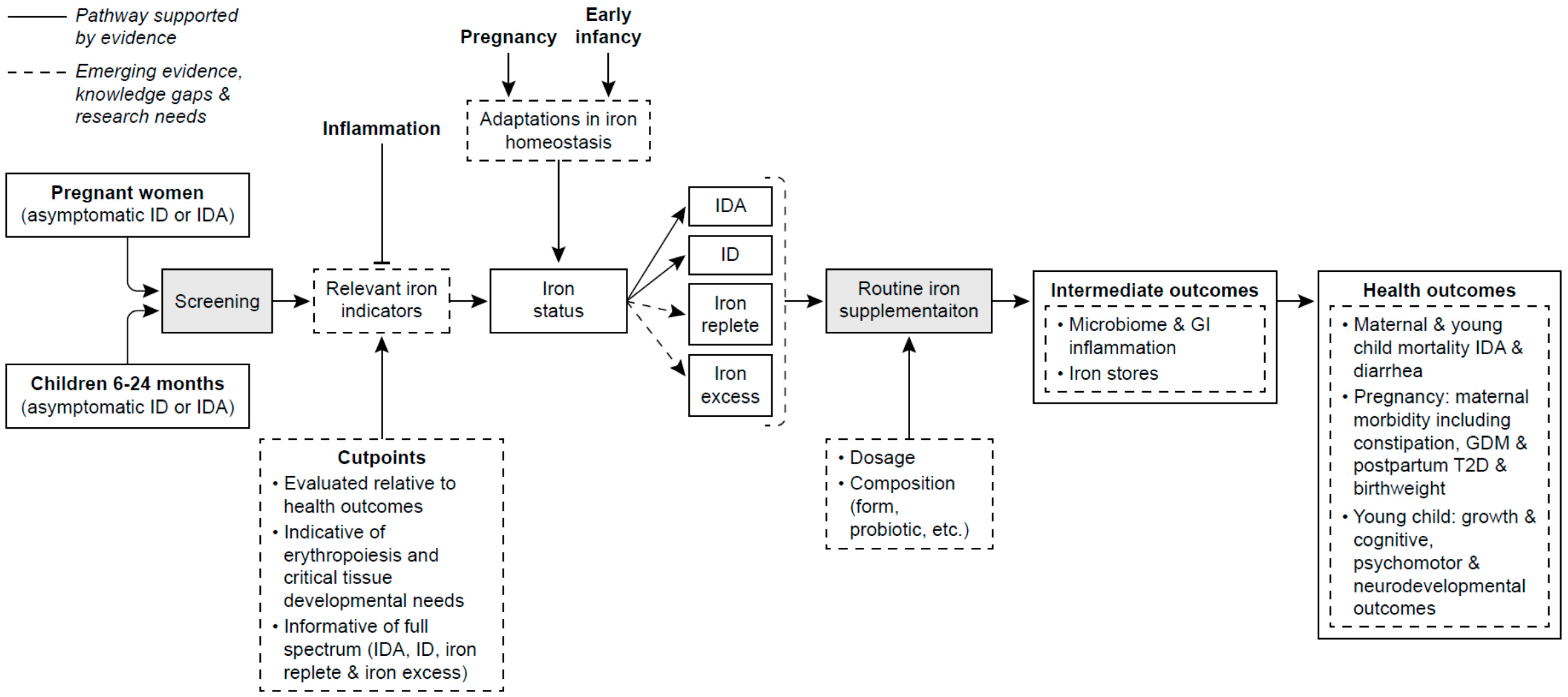
6. Implications for Research and Policy
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Aisen, P.; Enns, C.; Wessling-Resnick, M. Chemistry and biology of eukaryotic iron metabolism. Int. J. Biochem. Cell Biol. 2001, 33, 940–959. [Google Scholar] [CrossRef]
- Wessling-Resnick, M. Excess iron: Considerations related to development and early growth. Am. J. Clin. Nutr. 2017. [Google Scholar] [CrossRef]
- World Health Organization. World-Wide Prevalence of Anaemia 1993–2005: Who Global Database on Anaemia; WHO Press: Geneva, Switzerland, 2005. [Google Scholar]
- Petry, N.; Olofin, I.; Hurrell, R.F.; Boy, E.; Wirth, J.P.; Moursi, M.; Donahue, A.M.; Rohner, F. The proportion of anemia associated with iron deficiency in low, medium, and high human development index countries: A systematic analysis of national surveys. Nutrients 2016, 8, 693. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Daily Iron Supplementation in Children 6–23 Months of Age. Available online: http://www.who.int/elena/titles/guidance_summaries/iron_children/en/ (accessed on 11 July 2017).
- World Health Organization. Who Recommendations on Antenatal Care for a Positive Pregnancy Experience. Available online: http://www.who.int/reproductivehealth/publications/maternal_perinatal_health/anc-positive-pregnancy-experience/en/ (accessed on 14 September 2017).
- Gupta, P.M.; Hamner, H.C.; Suchdev, P.S.; Flores-Ayala, R.; Mei, Z. Iron deficiency and adequacy in young children, non-pregnant, and pregnant women in the United States. Am. J. Clin. Nutr. 2017, 106, 1640S–1646S. [Google Scholar] [CrossRef] [PubMed]
- Milman, N.; Taylor, C.; Merkel, J.; Brannon, P. Iron status in pregnant women and women of reproductive age in Europe. Am. J. Clin. Nutr. 2017, 106, 1655S–1662S. [Google Scholar] [CrossRef] [PubMed]
- Van der Merwe, L.F.; Eussen, S.R. Iron status of young children in Europe. Am. J. Clin. Nutr. 2017, 106, 1663S–1671S. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.L.; Brannon, P.M. Introduction to workshop on iron screening and supplementation in iron-replete pregnant women and young children. Am. J. Clin. Nutr. 2017, 106, 1547S–1554S. [Google Scholar] [CrossRef] [PubMed]
- Fisher, A.L.; Nemeth, E. Iron homeostasis during pregnancy. Am. J. Clin. Nutr. 2017, 106, 1567S–1574S. [Google Scholar] [CrossRef] [PubMed]
- Lönnerdal, B. Development of iron homeostasis in infants and young children. Am. J. Clin. Nutr. 2017, 106, 1575S–1580S. [Google Scholar] [CrossRef] [PubMed]
- Bothwell, T.H. Iron requirements in pregnancy and strategies to meet them. Am. J. Clin. Nutr. 2000, 72, 257S–264S. [Google Scholar] [PubMed]
- Zhang, C.; Rawal, S. Dietary iron intake, iron status and gestational diabetes. Am. J. Clin. Nutr. 2017, 106, 1672S–1680S. [Google Scholar] [CrossRef] [PubMed]
- Paganini, D.; Zimmermann, M.B. The effects of iron fortification and supplementation on the gut microbiome and diarrhea in infants and children: A review. Am. J. Clin. Nutr. 2017, 106, 1688S–1693S. [Google Scholar] [CrossRef] [PubMed]
- Vricella, L.K. Emerging understanding and measurement of plasma volume expansion in pregnancy. Am. J. Clin. Nutr. 2017, 106, 1620S–1625S. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US) Panel on Micronutrients. Dietary Reference Intakes for Vitamin A, Vitamin k, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc; National Academies Press: Washington, DC, USA, 2001. [Google Scholar]
- EFSA Panel on Dietetic Products Nutrition and Allergies (NDA). Scientific opinion on dietary reference values for iron. EFSA J. 2015, 13, 115. [Google Scholar]
- Scientific Advisory Committee on Nutrition (SACN). Iron and Health; The Stationery Office: London, UK, 2010.
- Australian Ministry of Health. Nutrient Reference Intakes for Australia and New Zealand: Iron. Available online: https://www.nrv.gov.au/nutrients/iron (accessed on 15 September 2017).
- FAO/WHO. Human Vitamin and Mineral Requirements; Iron; FAO: Geneva, Switzerland, 2002; Chapter 13. [Google Scholar]
- Rios, E.; Lipschitz, D.A.; Cook, J.D.; Smith, N.J. Relationship of maternal and infant iron stores as assessed by determination of plasma ferritin. Pediatrics 1975, 55, 694–699. [Google Scholar] [PubMed]
- Proytcheva, M.A. Issues in neonatal cellular analysis. Am. J. Clin. Pathol. 2009, 131, 560–573. [Google Scholar] [CrossRef] [PubMed]
- Dewey, K.G. The challenge of meeting nutrient needs of infants and young children during the period of complementary feeding: An evolutionary perspective. J. Nutr. 2013, 143, 2050–2054. [Google Scholar] [CrossRef] [PubMed]
- Baker, R.D.; Greer, F.R. Diagnosis and prevention of iron deficiency and iron-deficiency anemia in infants and young children (0–3 years of age). Pediatrics 2010, 126, 1040–1050. [Google Scholar] [CrossRef] [PubMed]
- Finn, K.; Callen, C.; Bhatia, J.; Reidy, K.; Bechard, L.J.; Carvalho, R. Importance of dietary sources of iron in infants and toddlers: Lessons from the fits study. Nutrients 2017, 9, 733. [Google Scholar] [CrossRef] [PubMed]
- Siu, A.L.; U.S. Preventive Services Task Force. Screening for iron deficiency anemia and iron supplementation in pregnant women to improve maternal health and birth outcomes: U.S. Preventive services task force recommendation statement. Ann. Intern. Med. 2015, 163, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Siu, A.L.; U.S. Preventive Services Task Force. Screening for iron deficiency anemia in young children: Uspstf recommendation statement. Pediatrics 2015, 136, 746–752. [Google Scholar] [CrossRef] [PubMed]
- Garner, C.D. Nutrition in pregnancy. In Uptodate; Post, T.W., Ed.; UpToDate: Waltham, MA, USA, 2017. [Google Scholar]
- American College of Obstetrics and Gynecology. Acog practice bulletin No. 95: Anemia in pregnancy. Obstet. Gynecol. 2008, 112, 201–207. [Google Scholar]
- Yip, R.; Parvanta, I.; Cogswell, M.E.; McDonnell, S.M.; Bowman, B.A.; Grummer-Strawn, L.M.; Trowbridge, F. Recommendations to prevent and control iron deficiency in the United States. Morb. Mortal. Wkly. Rep. 1998, 47, 1–29. [Google Scholar]
- Infant Feeding Working Group. Nutrition for Healthy Term Infants: Recommendations from Birth to Six Months. Available online: http://www.hc-sc.gc.ca/fn-an/nutrition/infant-nourisson/recom/index-eng.php (accessed on 18 September 2017).
- Domellöf, M.; Braegger, C.; Campoy, C.; Colomb, V.; Decsi, T.; Fewtrell, M.; Hojsak, I.; Mihatsch, W.; Molgaard, C.; Shamir, R.; et al. Iron requirements of infants and toddlers. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 119–129. [Google Scholar] [CrossRef] [PubMed]
- Pavord, S.; Myers, B.; Robinson, S.; Allard, S.; Strong, J.; Oppenheimer, C.; British Committee for Standards in Haematology. UK guidelines on the management of iron deficiency in pregnancy. Br. J. Haematol. 2012, 156, 588–600. [Google Scholar] [CrossRef] [PubMed]
- Australian Department of Health. Nutritional Supplements, 10.4.4 Iron Supplementation. Available online: http://www.health.gov.au/internet/publications/publishing.nsf/Content/clinical-practice-guidelines-ac-mod1~part-b~lifestyle-considerations~nutritional-supplements (accessed on 18 September 2017).
- Australian Government National Health and Medical Research Council. Infant Feeding Guidelines: Summary. Available online: https://www.eatforhealth.gov.au/sites/default/files/files/the_guidelines/n56b_infant_feeding_summary_130808.pdf (accessed on 18 September 2017).
- Auckland District Health Board—National Women’s Health. Iron in Pregnancy. Available online: http://nationalwomenshealth.adhb.govt.nz/Portals/0/Documents/Policies/Iron%20in%20Pregnancy_.pdf (accessed on 18 September 2017).
- Anderson, G.W.; Frazer, D.M. Current understanding of iron homeostasis. Am. J. Clin. Nutr. 2017, 106, 1547S–1554S. [Google Scholar] [CrossRef] [PubMed]
- Ross, A.C. Impact of chronic and acute inflammation on extra- and intracellular iron homeostasis. Am. J. Clin. Nutr. 2017, 106, 1581S–1587S. [Google Scholar] [CrossRef] [PubMed]
- Gordeuk, V.R.; Brannon, P.M. Ethnic and genetic factors of iron status in women of reproductive age. Am. J. Clin. Nutr. 2017, 106, 1594S–1599S. [Google Scholar] [CrossRef] [PubMed]
- Rehu, M.; Punnonen, K.; Ostland, V.; Heinonen, S.; Westerman, M.; Pulkki, K.; Sankilampi, U. Maternal serum hepcidin is low at term and independent of cord blood iron status. Eur. J. Haematol. 2010, 85, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Domellöf, M.; Lönnerdal, B.; Abrams, S.A.; Hernell, O. Iron absorption in breast-fed infants: Effects of age, iron status, iron supplements, and complementary foods. Am. J. Clin. Nutr. 2002, 76, 198–204. [Google Scholar] [PubMed]
- Leong, W.I.; Bowlus, C.L.; Tallkvist, J.; Lönnerdal, B. Iron supplementation during infancy—Effects on expression of iron transporters, iron absorption, and iron utilization in rat pups. Am. J. Clin. Nutr. 2003, 78, 1203–1211. [Google Scholar] [PubMed]
- Leong, W.I.; Bowlus, C.L.; Tallkvist, J.; Lönnerdal, B. DMT1 and FPN1 expression during infancy: Developmental regulation of iron absorption. Am. J. Physiol. Gastrointest. Liver Physiol. 2003, 285, G1153–G1161. [Google Scholar] [CrossRef] [PubMed]
- Georgieff, M.K. Iron assessment to protect the developing brain. Am. J. Clin. Nutr. 2017, 106, 1588S–1593S. [Google Scholar] [CrossRef] [PubMed]
- Hoofnagle, A.N. Bioindicator harmonization in clinical research: Making the hard work matter. Am. J. Clin. Nutr. 2017, 106, 1615S–1619S. [Google Scholar] [CrossRef] [PubMed]
- Pfeiffer, C.M.; Looker, A.C. Laboratory methodologies for indicators of iron status: Strengths, limitations and analytical challenges. Am. J. Clin. Nutr. 2017, 106, 1606S–1614S. [Google Scholar] [CrossRef] [PubMed]
- Brannon, P.M.; Stover, P.J.; Taylor, C.L. Integrating themes, evidence gaps and research needs identified by workshop on iron screening and supplementation in iron-replete pregnant women and young children. Am. J. Clin. Nutr. 2017, 106, 1703S–1712S. [Google Scholar] [CrossRef] [PubMed]
- Namaste, S.M.; Rohner, F.; Huang, J.; Bhushan, N.L.; Flores-Ayala, R.; Kupka, R.; Mei, Z.; Rawat, R.; Williams, A.M.; Raiten, D.J.; et al. Adjusting ferritin concentrations for inflammation: Biomarkers reflecting inflammation and nutritional determinants of anemia (brinda) project. Am. J. Clin. Nutr. 2017, 106, 359S–371S. [Google Scholar] [PubMed]
- Rohner, F.; Namaste, S.; Larson, L.; Addo, Y.; Mei, Z.; Suchdev, P.S.; Ashour, F.; Rawat, R.; Raiten, D.J.; Northrop-Clewes, C. Adjusting soluble transferrin receptor concentrations for inflammation: Brinda project. Am. J. Clin. Nutr. 2017, 106, 372S–382S. [Google Scholar] [PubMed]
- Mei, Z.; Namaste, S.M.; Serdula, M.; Suchdev, P.S.; Rohner, F.; Flores-Ayala, R.; Addo, O.Y.; Raiten, D.J. Adjusting total body iron for inflammation: Biomarkers reflecting inflammation and nutrition determinants of anemia (BRINDA) project. Am. J. Clin. Nutr. 2017, 106, 383S–389S. [Google Scholar] [PubMed]
- O’Brien, K.O. Iron status of north american pregnant women: Other evidence from the united states and canada. Am. J. Clin. Nutr. 2017, 106, 1647S–1654S. [Google Scholar] [CrossRef] [PubMed]
- Daru, J.; Colman, K.; Stanworth, S.J.; De La Salle, B.; Wood, E.M.; Pasricha, S.R. Serum ferritin as an indicator of iron status: What do we need to know? Am. J. Clin. Nutr. 2017, 106, 1634S–1639S. [Google Scholar] [CrossRef] [PubMed]
- Kemper, A.R.; Fan, T.; Grossman, D.C.; Phipps, M.G. Gaps in evidence regarding iron deficiency anemia in pregnant women and young children: Summary of united states preventive services task force recommendations. Am. J. Clin. Nutr. 2017, 106, 1555S–1558S. [Google Scholar] [CrossRef] [PubMed]
- Breymann, C. Iron deficiency anemia in pregnancy. Semin. Hematol. 2015, 52, 339–347. [Google Scholar] [CrossRef] [PubMed]
- Dewey, K.G.; Oaks, B.M. U-shaped curve for risk associated with maternal iron status or supplementation. Am. J. Clin. Nutr. 2017, 106, 1694S–1702S. [Google Scholar] [CrossRef] [PubMed]
- Kozuki, N.; Lee, A.C.; Katz, J. Moderate to severe, but not mild, maternal anemia is associated with increased risk of small-for-gestational-age outcomes. J. Nutr. 2012, 142, 358–362. [Google Scholar] [CrossRef] [PubMed]
- Lozoff, B.; Beard, J.; Connor, J.; Barbara, F.; Georgieff, M.; Schallert, T. Long-lasting neural and behavioral effects of iron deficiency in infancy. Nutr. Rev. 2006, 64, S34–S43. [Google Scholar] [CrossRef] [PubMed]
- Lozoff, B.; Goerogieff, M. Iron deficiency and brain development. Semin. Pediatr. Neonatol. 2006, 13, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Georgieff, M.K. Long-term brain and behavioral consequences of early iron deficiency. Nutr. Rev. 2011, 69, S43–S48. [Google Scholar] [CrossRef] [PubMed]
- Cai, C.; Granger, M.; Eck, P.; Friel, J. Effect of daily iron supplementation in healthy exclusively breastfed infants: A systematic review with meta-analysis. Breastfeed. Med. 2017. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, M.S.; Blazina, I.; Dana, T.; Cantor, A.; Bougatsos, C. Screening and routine supplementation for iron deficiency anemia: A systematic review. Pediatrics 2015, 135, 723–733. [Google Scholar] [CrossRef] [PubMed]
- Reveiz, L.; Gyte, G.M.; Cuervo, L.G.; Casasbuenas, A. Treatments for iron-deficiency anaemia in pregnancy. Cochrane Database Syst. Rev. 2011, 10, CD003094. [Google Scholar]
- Haider, B.A.; Olofin, I.; Wang, M.; Spiegelman, D.; Ezzati, M.; Fawzi, W.W.; Nutrition Impact Model Study Group. Anaemia, prenatal iron use, and risk of adverse pregnancy outcomes: Systematic review and meta-analysis. BMJ 2013, 346, f3443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDonagh, M.; Blazina, I.; Dana, T.; Cantor, A.; Bougatsos, C. Routine Iron Supplementation and Screening for Iron Deficiency Anemia in Children Ages 6 to 24 Months: A Systematic Review to Update the U.S. Preventive Services Task Force Recommendation; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2015. [Google Scholar]
- Scholl, T.O. Iron status during pregnancy: Setting the stage for mother and infant. Am. J. Cliln. Nutr. 2005, 81, 741–748. [Google Scholar]
- Pasricha, S.R.; Hayes, E.; Kalumba, K.; Biggs, B.A. Effect of daily iron supplementation on health in children aged 4–23 months: A systematic review and meta-analysis of randomised controlled trials. Lancet Glob. Health 2013, 1, e77–e86. [Google Scholar] [CrossRef]
- Lönnerdal, B. Excess iron intake as a factor in growth, infections and development of infants and young children. Am. J. Clin. Nutr. 2017, 106, 1681S–1687S. [Google Scholar] [CrossRef] [PubMed]
- Singhal, A.; Morley, R.; Abbott, R.; Fairweather-Tait, S.; Stephenson, T.; Lucas, A. Clinical safety of iron-fortified formulas. Pediatrics 2000, 105, E38. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, S.; Berggren, K.L.; Marks, E.; Fox, J.H. Impact of high iron intake on cognition and neurodegeneration in humans and in animal models: A systematic review. Nutr. Rev. 2017, 75, 456–470. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Women of Reproductive Age | Pregnant Women | Infants | Young Children | |||
|---|---|---|---|---|---|---|
| 0 to 6 Months | 6 to 12 Months | 12 to 23 Months | ||||
| 0 to 3 | 4 to 6 | |||||
| United States & Canada (IOM 1) | 8.1/18 2 | 22/27 2 | 0.26 3 | 6.9/11 2 | 3/7 2 | |
| Europe | ||||||
| EFSA 4 | 7/16 2 | 7/16 2 | Not specified | 8/11 2 | 5/7 2 | |
| UK (SACN 5) | 11.4/14.8 2 | 11.4/14.8 2 | 1.3/1.7 2 | 2.3/3.3 2 | 6/7.9 2 | 5.3/6.9 2 |
| Australia & New Zealand 6 | 8/18 2 | 22/27 2 | 0.2 3 | 7/11 2 | 4/9 2 | |
| WHO/FAO 7 | 19.5/24.5/29.4/58.8 8 | Not specified | Not specified | 6.2/7.7/9.3/18.6 8 | 3.9/4.8/5.8/11.6 8 | |
| Source | Recommendations | |
|---|---|---|
| Supplement | Supplement and Iron-Rich Complementary Feeding | |
| Pregnant Women | Infants (0–12 Months) | |
| United States | ||
| UpToDate 1 | 15–30 mg/day increase | Supplement 1 mg/kg/day (max. 15 mg/day) breastfed ≥4 months. until consuming sufficient quantities of iron-rich complementary foods |
| American College of Gynecology 2 | If iron deficiency anemia (IDA) identified | -- |
| Centers for Disease Control 3 | Universal (30 mg/day) | Suggest supplement (1 mg/kg/day) breast-fed infants ≥6 months. consuming insufficient iron from supplementary foods (<1 mg/kg/day) |
| American Academy of Pediatrics 4 | - | Screen for ID/IDA at 12 months. Supplement (1 mg/kg/day) infants ≥4 months. exclusively breast-fed or consuming >1/2 intake from breast milk until receiving appropriate iron-containing complementary foods |
| Canada | ||
| Infant Feeding Working Group for Health Canada, Canadian Paeditric Society, Dietitians of Canada & Breastfeeding Committee for Canada 5 | Recommend meat, meat-alternatives & iron-fortified cereals for firs complementary foods at 6 months. | |
| Europe | ||
| European Food Safety Authority 6 | If at risk | - |
| European Society Pediatric Gastroenterology, Hepatoloy & Nutrition 7 | No evidence iron supplementation of European women improves iron status of their infants. | No convincing evidence for iron supplements of exclusively breast-fed term infant <6 months. except on individual basis in high risk groups. Recommend iron rich complementary foods (meat, iron-fortified follow-on formulas & iron-fortified foods) |
| UK – British | ||
| Committee for Standards in Haematology 8 | Supplement if serum ferritin (SF) <30 µg/L | - |
| Australia | ||
| Department of Health 9 | Do not routinely supplement | - |
| National Health and Medical Research Council 10 | - | Introduce first iron-containing nutritious foods (iron-fortified cereals, pureed meat and poultry dishes; care with plant sources such as cooked plain tofu and legumes/beans) |
| New Zealand | ||
| National Women’s Health 11 | Screen SF & Hb mid 26–28 weeks; supplement low dose (65 mg) if iron deficient and high dose (130 mg) if IDA | - |
| World | ||
| WHO 12,13 | Supplement (30–60 mg/day) | Iron supplementation (10–12.5 mg/day) in young children (6–23 months) for 3 consecutive months/year. in settings ≥40% anemia prevalence |
| Indicator | Assesses | Advantages | Limitations |
|---|---|---|---|
| Hemoglobin (Hb) | Anemia | Is commonly available Has low complexity of analytic procedures | Has low specificity and sensitivity Affected by hemodilution in pregnancy and postnatal red blood cell turnover in early infancy May be complicated by certain factors (elevation? age? ethnicity?) Affected by inflammation and obesity |
| Ferritin (primarily serum, SF) | Size of iron stores | Is commonly available Has World Health Organization (WHO) International Standard Material | Confounded by inflammation |
| Soluble transferrin receptor (sTfR) | Inadequate tissue availability Iron deficient erythropoiesis | Less affected by inflammation | Has limited availability Exhibits assay differences Lacks a standard reference material (although one is in development) |
| Ratio of sTfR-to-ferritin (derived using various calculations) | Total body iron stores | Reflects full range of status | Requires two measurements Less affected by inflammation |
| Transferrin saturation | Iron deficient erythropoiesis | Is commonly available | Varies diurnally and prandially |
| Erythrocyte protoporphyrin | Iron deficient erythropoiesis | Is reliability infield instrumentation | |
| Hepcidin | Determinant of iron needs and utilization | Is relatively sensitive | Is experimental and under development May possibly be less affected by inflammation |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brannon, P.M.; Taylor, C.L. Iron Supplementation during Pregnancy and Infancy: Uncertainties and Implications for Research and Policy. Nutrients 2017, 9, 1327. https://doi.org/10.3390/nu9121327
Brannon PM, Taylor CL. Iron Supplementation during Pregnancy and Infancy: Uncertainties and Implications for Research and Policy. Nutrients. 2017; 9(12):1327. https://doi.org/10.3390/nu9121327
Chicago/Turabian StyleBrannon, Patsy M., and Christine L. Taylor. 2017. "Iron Supplementation during Pregnancy and Infancy: Uncertainties and Implications for Research and Policy" Nutrients 9, no. 12: 1327. https://doi.org/10.3390/nu9121327
APA StyleBrannon, P. M., & Taylor, C. L. (2017). Iron Supplementation during Pregnancy and Infancy: Uncertainties and Implications for Research and Policy. Nutrients, 9(12), 1327. https://doi.org/10.3390/nu9121327