The Association of Ankle Brachial Index, Protein-Energy Wasting, and Inflammation Status with Cardiovascular Mortality in Patients on Chronic Hemodialysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Enrolled Subjects
2.2. Endpoints
2.3. Statistics
3. Results
3.1. Baseline Characteristics
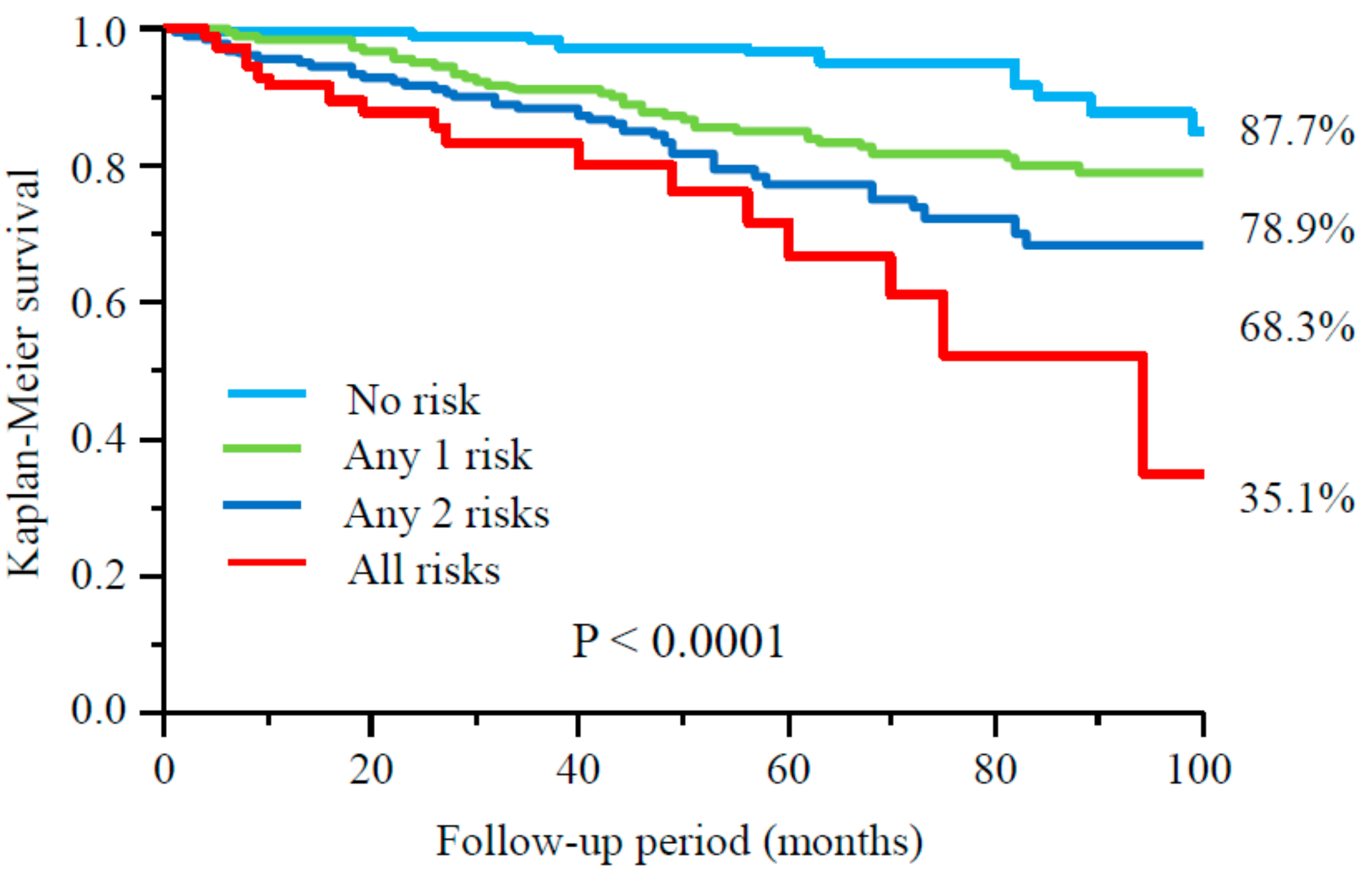
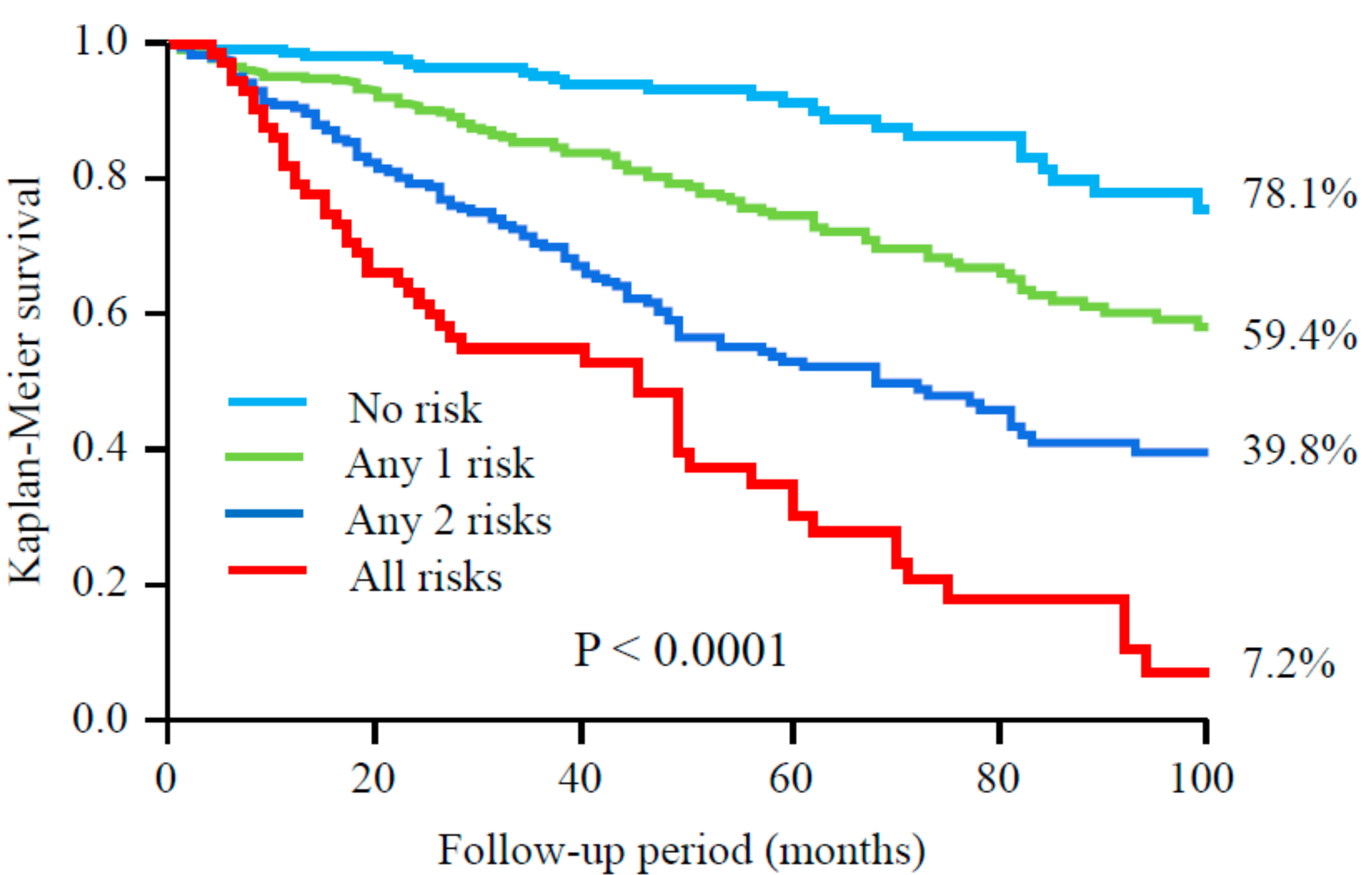
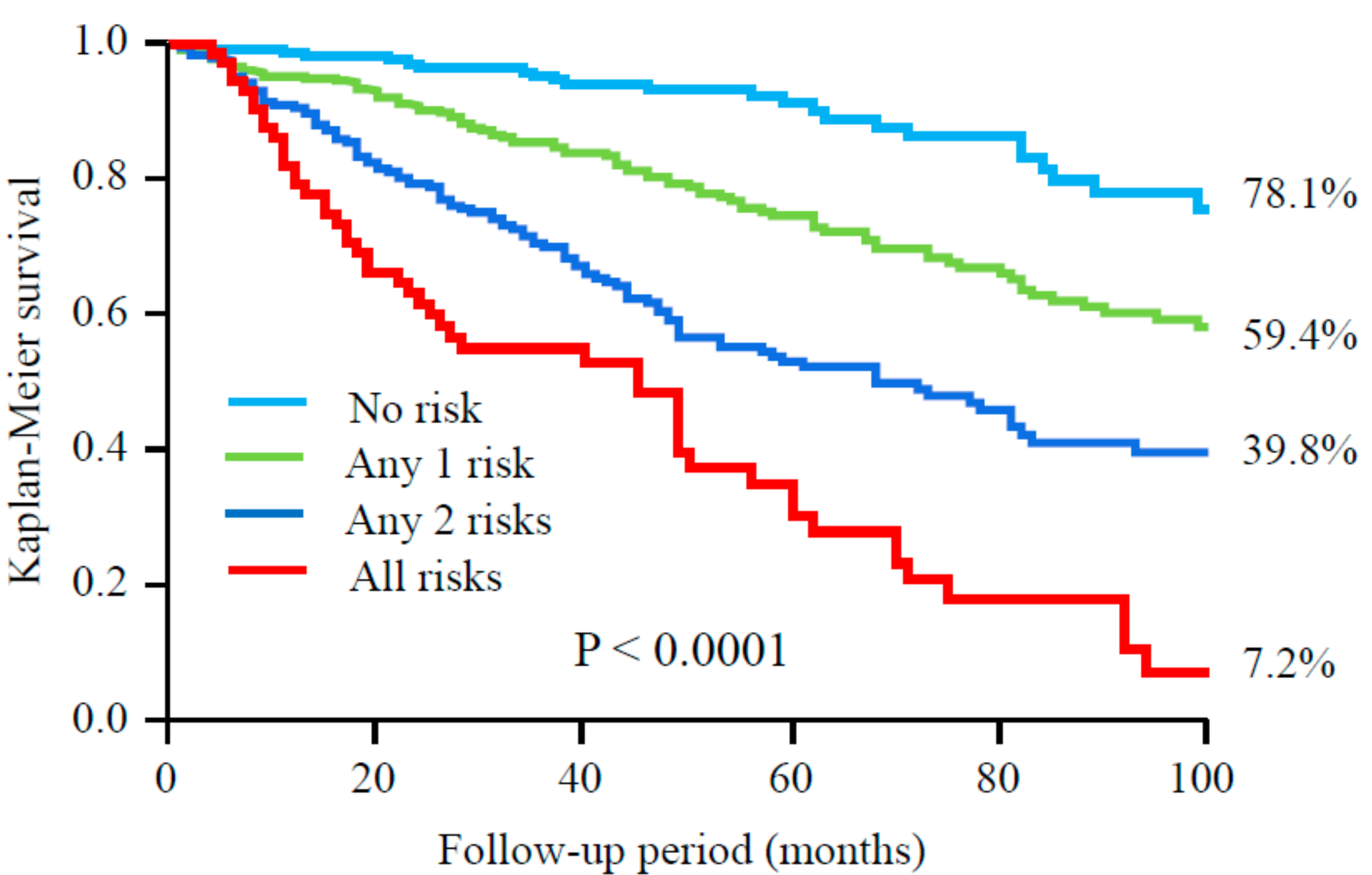
3.2. Follow-Up
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Sarnak, M.J.; Levey, A.S.; Schoolwerth, A.C.; Coresh, J.; Culleton, B.; Hamm, L.L.; McCullough, P.A.; Kasiske, B.L.; Kelepouris, E.; Klag, M.J.; et al. American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Kidney disease as a risk factor for development of cardiovascular disease: A statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation 2003, 108, 2154–2169. [Google Scholar] [PubMed]
- Go, A.S.; Chertow, G.M.; Fan, D.; McCulloch, C.E.; Hsu, C.Y. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N. Engl. J. Med. 2004, 23, 1296–1305. [Google Scholar] [CrossRef] [PubMed]
- Foley, R.N.; Parfrey, P.S.; Sarnak, M.J. Clinical epidemiology of cardiovascular disease in chronic renal disease. Am. J. Kidney Dis. 1998, 32 (Suppl. S3), S112–S119. [Google Scholar] [CrossRef] [PubMed]
- O’Hare, A.M.; Johansen, K.L. Lower-extremity peripheral arterial disease among patients with end-stage renal disease. J. Am. Soc. Nephrol. 2001, 12, 2838–2847. [Google Scholar] [PubMed]
- Rajagopalan, S.; Dellegrottaglie, S.; Furniss, A.L.; Gillespie, B.W.; Satayathum, S.; Lameire, N.; Saito, A.; Akiba, T.; Jadoul, M.; Ginsberg, N.; et al. Peripheral arterial disease in patients with end-stage renal disease: Observations from the Dialysis Outcomes and Practice Patterns Study (DOPPS). Circulation 2006, 114, 1914–1922. [Google Scholar] [CrossRef] [PubMed]
- Norgren, L.; Hiatt, W.R.; Dormandy, J.A.; Nehler, M.R.; Harris, K.A.; Fowkes, F.G.; TASC II Working Group. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). Eur. J. Vasc. Endovasc. Surg. 2007, 33 (Suppl. S1), S1–S75. [Google Scholar] [CrossRef] [PubMed]
- Fouque, D.; Kalantar-Zadeh, K.; Kopple, J.; Cano, N.; Chauveau, P.; Cuppari, L.; Franch, H.; Guarnieri, G.; Ikizler, T.A.; Kaysen, G.; et al. A proposed nomenclature and diagnostic criteria for protein-energy wasting in acute and chronic kidney disease. Kidney Int. 2008, 73, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, H.; Ito, Y.; Ishii, H.; Aoyama, T.; Kamoi, D.; Kasuga, H.; Yasuda, K.; Maruyama, S.; Matsuo, S.; Murohara, T.; et al. Geriatric nutritional risk index accurately predicts cardiovascular mortality in incident hemodialysis patients. J. Cardiol. 2014, 64, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, H.; Ishii, H.; Aoyama, T.; Kamoi, D.; Kasuga, H.; Ito, Y.; Yasuda, K.; Tanaka, M.; Yoshikawa, D.; Maruyama, S.; et al. Association of cardiac valvular calcifications and C-reactive protein with cardiovascular mortality in incident hemodialysis patients: A Japanese cohort study. Am. J. Kidney Dis. 2013, 61, 254–261. [Google Scholar] [CrossRef] [PubMed]
- Yamada, K.; Furuya, R.; Takita, T.; Maruyama, Y.; Yamaguchi, Y.; Ohkawa, S.; Kumagai, H. Simplified nutritional screening tools for patients on maintenance hemodialysis. Am. J. Clin. Nutr. 2008, 87, 106–113. [Google Scholar] [PubMed]
- Cereda, E.; Zagami, A.; Vanotti, A.; Piffer, S.; Pedrolli, C. Geriatric Nutritional Risk Index and overall-cause mortality prediction in institutionalised elderly: A 3-year survival analysis. Clin. Nutr. 2008, 27, 717–723. [Google Scholar] [CrossRef] [PubMed]
- Narumi, T.; Arimoto, T.; Funayama, A.; Kadowaki, S.; Otaki, Y.; Nishiyama, S.; Takahashi, H.; Shishido, T.; Miyashita, T.; Miyamoto, T.; et al. Prognostic importance of objective nutritional indexes in patients with chronic heart failure. J. Cardiol. 2013, 62, 307–313. [Google Scholar] [CrossRef] [PubMed]
- Stenvinkel, P.; Heimbürger, O.; Paultre, F.; Diczfalusy, U.; Wang, T.; Berglund, L.; Jogestrand, T. Strong association between malnutrition, inflammation, and atherosclerosis in chronic renal failure. Kidney Int. 1999, 55, 1899–1911. [Google Scholar] [CrossRef] [PubMed]
- Bergström, J.; Lindholm, B. Malnutrition, cardiac disease, and mortality: An integrated point of view. Am. J. Kidney Dis. 1998, 32, 834–841. [Google Scholar] [CrossRef]
- Kaysen, G.A. Malnutrition and the acute-phase reaction in dialysis patients-how to measure and how to distinguish. Nephrol. Dial. Transplant. 2000, 15, 1521–1524. [Google Scholar] [CrossRef] [PubMed]
- Bouillanne, O.; Morineau, G.; Dupont, C.; Coulombel, I.; Vincent, J.P.; Nicolis, I.; Benazeth, S.; Cynober, L.; Aussel, C. Geriatric Nutritional Risk Index: A new index for evaluating at-risk elderly medical patients. Am. J. Clin. Nutr. 2005, 82, 777–783. [Google Scholar] [PubMed]
- Harada, K.; Suzuki, S.; Ishii, H.; Hirayama, K.; Aoki, T.; Shibata, Y.; Negishi, Y.; Sumi, T.; Kawashima, K.; Kunimura, A.; et al. Nutrition Status Predicts Severity of Vascular Calcification in Non-Dialyzed Chronic Kidney Disease. Circ. J. 2017, 81, 316–321. [Google Scholar] [CrossRef] [PubMed]
- Izawa, K.P.; Watanabe, S.; Hirano, Y.; Yamamoto, S.; Oka, K.; Suzuki, N.; Kida, K.; Suzuki, K.; Osada, N.; Omiya, K.; et al. The relation between Geriatric Nutritional Risk Index and muscle mass, muscle strength, and exercise capacity in chronic heart failure patients. Int. J. Cardiol. 2014, 177, 1140–1141. [Google Scholar] [CrossRef] [PubMed]
- Saitoh, M.; Dos Santos, M.R.; Ebner, N.; Emami, A.; Konishi, M.; Ishida, J.; Valentova, M.; Sandek, A.; Doehner, W.; Anker, S.D.; et al. Nutritional status and its effects on muscle wasting in patients with chronic heart failure: Insights from Studies Investigating Co-morbidities Aggravating Heart Failure. Wien. Klin. Wochenschr. 2016, 128, 497–504. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, H.; Inoue, K.; Shimizu, K.; Hiraga, K.; Takahashi, E.; Otaki, K.; Yoshikawa, T.; Furuta, K.; Tokunaga, C.; Sakakibara, T.; et al. Tokai Renal Nutrition Study Group. Comparison of Nutritional Risk Scores for Predicting Mortality in Japanese Chronic Hemodialysis Patients. J. Ren. Nutr. 2017. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Variables | All Patients (n = 973) | No Risk Factor (n = 259) | 1 Risk Factors (n = 380) | 2 Risk Factors (n = 257) | All Risk Factors (n = 77) | p Value |
|---|---|---|---|---|---|---|
| Male (%) | 62.6 | 61.0 | 60.5 | 66.2 | 66.2 | 0.42 |
| Age (years) | 64 ± 12 | 62 ± 12 | 63 ± 11 | 66 ± 12 | 69 ± 11 | <0.0001 |
| Duration of HD (years) | 2.0 (0.4–7.2) | 1.8 (0.5–6.4) | 2.2 (0.5–7.9) | 2.0 (0.3–7.4) | 2.1 (0.8–10.1) | 0.41 |
| Diabetes (%) | 47.9 | 45.0 | 46.7 | 49.2 | 58.7 | 0.19 |
| Hypertension (%) | 74.9 | 77.4 | 72.8 | 76.4 | 72.2 | 0.54 |
| Dyslipidemia (%) | 14.4 | 13.9 | 12.9 | 17.3 | 13.9 | 0.54 |
| Smoking (%) | 25.4 | 21.4 | 26.9 | 27.8 | 23.9 | 0.38 |
| Body mass index | 21.6 ± 3.4 | 22.8 ± 3.6 | 22.0 ± 3.4 | 20.5 ± 2.9 | 19.2 ± 2.2 | <0.0001 |
| Previous CAD (%) | 31.0 | 25.5 | 34.5 | 29.6 | 37.7 | 0.053 |
| Previous stroke (%) | 18.8 | 18.5 | 21.3 | 16.7 | 14.3 | 0.34 |
| Hemoglobin (mg/dL) | 10.5 ± 1.3 | 10.9 ± 1.0 | 10.6 ± 1.3 | 10.1 ± 1.2 | 9.6 ± 1.4 | <0.0001 |
| Albumin (g/dL) | 3.6 ± 0.3 | 3.8 ± 0.2 | 3.6 ± 0.3 | 3.4 ± 0.4 | 3.3 ± 0.3 | <0.0001 |
| Creatinine (mg/dL) | 9.6 ± 3.1 | 10.5 ± 3.6 | 9.9 ± 2.7 | 8.7 ± 2.8 | 7.8 ± 2.4 | <0.0001 |
| Calcium (mg/dL) | 8.8 ± 0.8 | 8.7 ± 0.8 | 8.9 ± 0.9 | 8.6 ± 0.9 | 8.6 ± 0.9 | 0.37 |
| Phosphate (mg/dL) | 5.2 ± 1.3 | 5.4 ± 1.3 | 5.3 ± 1.3 | 5.1 ± 1.4 | 5.0 ± 1.3 | 0.012 |
| Calcium x phosphate | 46.1 ± 20.5 | 47.1 ± 12.0 | 47.9 ± 28.6 | 43.7 ± 13.3 | 43.2 ± 13.5 | 0.035 |
| Total cholesterol (mg/dL) | 161 ± 35 | 161 ± 34 | 163 ± 36 | 159 ± 35 | 159 ± 38 | 0.56 |
| LDL cholesterol (mg/dL) | 90 ± 30 | 87 ± 28 | 91 ± 30 | 89 ± 28 | 90 ± 30 | 0.59 |
| HDL cholesterol (mg/dL) | 44 ± 14 | 46 ± 14 | 43 ± 13 | 43 ± 14 | 43 ± 13 | 0.061 |
| Triglyceride (mg/dL) | 120 ± 85 | 118 ± 61 | 124 ± 77 | 117 ± 94 | 117 ± 86 | 0.78 |
| CRP (mg/L) | 1.6 (0.8–5.0) | 0.8 (0.5–1.2) | 1.6 (0.7–4.6) | 3.8 (2.0–10.5) | 5.0 (3.1–16.7) | <0.0001 |
| Abnormal ABI (%) | 34.1 | 0.0 | 27.9 | 58.0 | 100.0 | <0.0001 |
| GNRI | 94.1 ± 8.8 | 99.7 ± 7.0 | 95.4 ± 0.4 | 89.3 ± 0.5 | 85.3 ± 0.9 | <0.0001 |
| Variables | Univariate | Multivariate | ||
|---|---|---|---|---|
| OR (95% CI) | p value | OR (95% CI) | p value | |
| Age | 1.02 (1.01–1.03) | <0.0001 | 1.01 (1.00–1.03) | 0.047 |
| Diabetes | 1.68 (1.2–2.209 | 0.0001 | 1.72 (1.30–2.26) | 0.0001 |
| Previous CAD | 1.82 (1.38–2.41) | <0.0001 | 1.82 (1.36–2.43) | <0.0001 |
| GNRI | 0.97 (0.96–0.99) | 0.0004 | 0.97 (0.96–0.99) | 0.0009 |
| CRP | 1.16 (1.04–1.33) | 0.011 | 1.13 (1.01–1.29) | 0.043 |
| Variables | Β | p Value |
|---|---|---|
| Age | −0.217 | <0.0001 |
| Hemoglobin | 0.196 | <0.0001 |
| Creatinine | 0.197 | <0.0001 |
| Phosphate | 0.117 | 0.0020 |
| CRP | −0.138 | <0.0001 |
| Abnormal ABI | −0.072 | 0.017 |
| Variables | Univariate | Multivariate * | ||
|---|---|---|---|---|
| HR (95% CI) | p value | HR (95% CI) | p value | |
| Mortality Due to CVD | ||||
| Abnormal ABI | 1.96 (1.37–2.80) | 0.0002 | 1.62 (1.13–2.32) | 0.0096 |
| GNRI < 91.2 | 1.83 (1.27–2.61) | 0.0011 | 1.57 (1.06–2.33) | 0.023 |
| CRP > 1.9 mg/L | 2.13 (1.48–3.08) | <0.0001 | 1.89 (1.31–2.77) | 0.0007 |
| All-Cause Mortality | ||||
| Abnormal ABI | 2.07 (1.64–2.62) | <0.0001 | 1.68 (1.33–2.14) | <0.0001 |
| GNRI < 91.2 | 2.47 (1.96–3.13) | <0.0001 | 2.12 (1.64–2.74) | <0.0001 |
| CRP > 1.9 mg/L | 2.34 (1.85–2.99) | <0.0001 | 2.02 (1.58–2.60) | <0.0001 |
| Variables | Univariate | Multivariate * | ||
|---|---|---|---|---|
| HR (95% CI) | p value | HR (95% CI) | p value | |
| Mortality Due to CVD (vs. no risk factor) | ||||
| Any single risk factor | 2.43 (1.35–4.67) | 0.0023 | 2.28 (1.26–4.42) | 0.0054 |
| Any two risk factors | 4.05 (2.25–7.82) | <0.0001 | 3.61 (1.97–7.05) | <0.0001 |
| All risk factors | 7.38 (3.63–15.4) | <0.0001 | 5.26 (2.51–11.3) | <0.0001 |
| All-Cause Mortality (vs. no risk factor) | ||||
| Any single risk factor | 2.46 (1.62–3.88) | <0.0001 | 2.55 (1.66–4.06) | <0.0001 |
| Any two risk factors | 5.04 (3.34–7.88) | <0.0001 | 4.59 (3.00–7.29) | <0.0001 |
| All risk factors | 10.6 (6.64–17.2) | <0.0001 | 7.97 (4.88–13.2) | <0.0001 |
| Variables | C-Index | p Value | NRI | p Value | IDI | p Value |
|---|---|---|---|---|---|---|
| Mortality Due to CVD | ||||||
| Established risk factors | 0.654 | Reference | Reference | Reference | ||
| +abnormal ABI | 0.710 | 0.012 | 0.534 | <0.0001 | 0.018 | <0.0001 |
| +GNRI | 0.711 | 0.0027 | 0.415 | <0.0001 | 0.017 | <0.0001 |
| +CRP | 0.692 | 0.0083 | 0.388 | <0.0001 | 0.015 | 0.0049 |
| +All factors | 0.765 | <0.0001 | 0.518 | <0.0001 | 0.036 | <0.0001 |
| +all factors vs. +abnormal ABI | 0.055 * | 0.0027 | 0.470 | <0.0001 | 0.028 | <0.0001 |
| +all factors vs. +GNRI | 0.054 * | 0.0051 | 0.348 | 0.0002 | 0.019 | <0.0001 |
| +all factors vs. +CRP | 0.073 * | 0.0004 | 0.459 | <0.0001 | 0.031 | <0.0001 |
| All-Cause Mortality | ||||||
| Established risk factors | 0.669 | Reference | Reference | Reference | ||
| +abnormal ABI | 0.718 | 0.0008 | 0.511 | <0.0001 | 0.040 | <0.0001 |
| +GNRI | 0.737 | <0.0001 | 0.412 | <0.0001 | 0.065 | <0.0001 |
| +CRP | 0.710 | <0.0001 | 0.462 | <0.0001 | 0.036 | <0.0001 |
| +All factors | 0.794 | <0.0001 | 0.587 | <0.0001 | 0.132 | <0.0001 |
| +all factors vs. +abnormal ABI | 0.076 * | <0.0001 | 0.685 | <0.0001 | 0.092 | <0.0001 |
| +all factors vs. +GNRI | 0.057 * | 0.0002 | 0.343 | <0.0001 | 0.066 | <0.0001 |
| +all factors vs. +CRP | 0.084 * | <0.0001 | 0.553 | <0.0001 | 0.095 | <0.0001 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ishii, H.; Takahashi, H.; Ito, Y.; Aoyama, T.; Kamoi, D.; Sakakibara, T.; Umemoto, N.; Kumada, Y.; Suzuki, S.; Murohara, T. The Association of Ankle Brachial Index, Protein-Energy Wasting, and Inflammation Status with Cardiovascular Mortality in Patients on Chronic Hemodialysis. Nutrients 2017, 9, 416. https://doi.org/10.3390/nu9040416
Ishii H, Takahashi H, Ito Y, Aoyama T, Kamoi D, Sakakibara T, Umemoto N, Kumada Y, Suzuki S, Murohara T. The Association of Ankle Brachial Index, Protein-Energy Wasting, and Inflammation Status with Cardiovascular Mortality in Patients on Chronic Hemodialysis. Nutrients. 2017; 9(4):416. https://doi.org/10.3390/nu9040416
Chicago/Turabian StyleIshii, Hideki, Hiroshi Takahashi, Yasuhiko Ito, Toru Aoyama, Daisuke Kamoi, Takashi Sakakibara, Norio Umemoto, Yoshitaka Kumada, Susumu Suzuki, and Toyoaki Murohara. 2017. "The Association of Ankle Brachial Index, Protein-Energy Wasting, and Inflammation Status with Cardiovascular Mortality in Patients on Chronic Hemodialysis" Nutrients 9, no. 4: 416. https://doi.org/10.3390/nu9040416
APA StyleIshii, H., Takahashi, H., Ito, Y., Aoyama, T., Kamoi, D., Sakakibara, T., Umemoto, N., Kumada, Y., Suzuki, S., & Murohara, T. (2017). The Association of Ankle Brachial Index, Protein-Energy Wasting, and Inflammation Status with Cardiovascular Mortality in Patients on Chronic Hemodialysis. Nutrients, 9(4), 416. https://doi.org/10.3390/nu9040416