Exploring Diet Quality between Urban and Rural Dwelling Women of Reproductive Age


 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
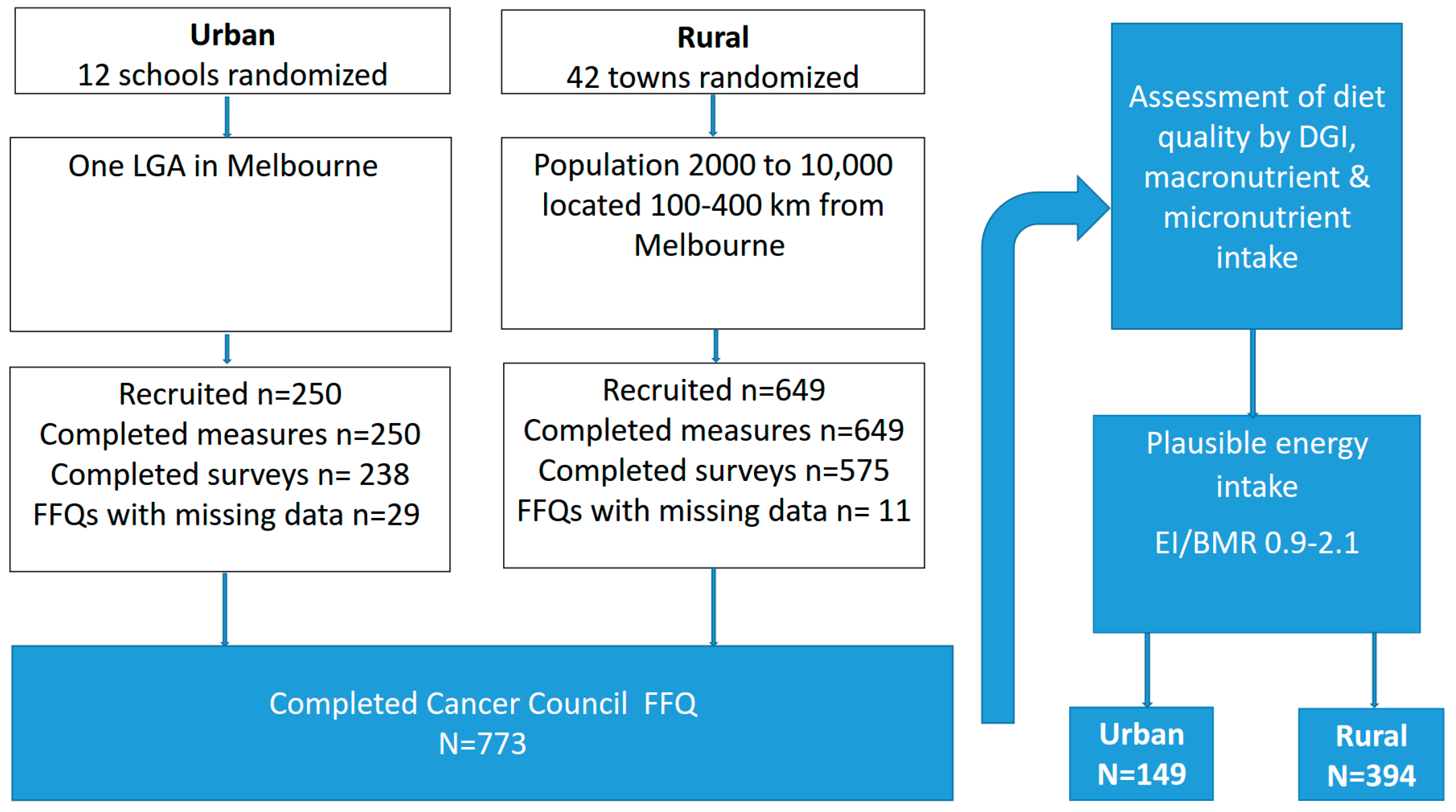
2.2. Participants
2.3. Baseline Measures
2.4. Anthropometrics
2.5. Dietary Intake
2.6. Dietary Quality
2.7. Data Analysis
3. Results
3.1. Participants
3.2. Participant Characteristics
3.3. Macronutrient and Micronutrient Intake
3.4. Diet Quality
3.5. Predictors of Diet Quality in All Women
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| $AUD | Australian dollar |
| DGI | Dietary Guideline Index |
| BMI | Body Mass Index |
| HeLP-her | The Healthy Lifestyle Program |
| FFQ | Food Frequency Questionnaire |
| EI/BMR | Energy Intake: Basal Metabolic Rate |
| AGHE | Australian Guide to Healthy Eating |
| SD | Standard Deviation |
| N | Number |
| ARFS | Australian Recommended Food Score |
| CHO | Carbohydrate |
| SFA | Saturated fatty acid |
| MUFA | Monounsaturated fatty acid |
| PUFA | Polyunsaturated fatty acid |
| GI | Glycemic Index |
| GL | Glycemic load |
References
- Brown, W. Australian women and their weight: A growing problem. In Proceedings of the Meeting of Commonwealth Department of Health and Ageing, Canberra, Australia, 11 October 2005. [Google Scholar]
- World Health Organization. Obesity and Overweight. Available online: http://www.who.int/mediacentre/factsheets/fs311/en/ (accessed on 9 September 2016).
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic; World Health Organization: Geneva, Switzerland, 2000; pp. 154–162. [Google Scholar]
- Zugravu, C.A. Eating habits and influential factors for mothers and children in Romania. Int. J. Collab. Res. Intern. Med. Public Health 2012, 4, 362–374. [Google Scholar]
- Smith, K.J.; McNaughton, S.A.; Gall, S.L.; Blizzard, L.; Dwyer, T.; Venn, A.J. Involvement of young Australian adults in meal preparation: Cross-sectional associations with sociodemographic factors and diet quality. J. Am. Diet. Assoc. 2010, 110, 1363–1367. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.B.; Humphreys, J.S.; Wilson, M.G. Addressing the health disadvantage of rural populations: How does epidemiological evidence inform rural health policies and research. Aust. J. Rural Health 2008, 16, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Eberhardt, M.S.; Pamuk, E.R. The importance of place of residence: Examining health in rural and nonrural areas. Am. J. Public Health 2004, 94, 1682–1686. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Rural Poverty and Health Systems in the WHO European Region; WHO Regional Office for Europe: Copenhagen, Denmark, 2010. [Google Scholar]
- Palermo, C.; McCartan, J.; Kleve, S.; Sinha, K.; Shiell, A. A longitudinal study of the cost of food in Victoria influenced by geography and nutritional quality. Aust. N. Z. J. Public Health 2016, 40, 270–273. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Women’s Health Fact Sheet Number 334. Available online: http://www.who.int/mediacentre/factsheets/fs334/en/ (accessed on 6 December 2016).
- Wirt, A.; Collins, C.E. Diet quality-what is it and does it matter. Public Health Nutr. 2009, 12, 2473–2492. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Hoffmann, G. Diet quality as assessed by the healthy eating index, the alternate healthy eating index, the dietary approaches to stop hypertension score, and health outcomes: A systematic review and meta-analysis of cohort studies. J. Acad. Nutr. Diet. 2015, 115, 780–800. [Google Scholar] [CrossRef] [PubMed]
- Alhazmi, A.; Stojanovski, E.; McEvoy, M.; Brown, W.; Garg, M.L. Diet quality score is a predictor of type 2 diabetes risk in women: The Australian longitudinal study on women’s health. Br. J. Nutr. 2014, 112, 945–951. [Google Scholar] [CrossRef] [PubMed]
- Huot, I.; Paradis, G.; Receveur, O.; Ledoux, M. Correlates of diet quality in the Quebec population. Public Health Nutr. 2004, 7, 1009–1016. [Google Scholar] [CrossRef] [PubMed]
- Pedroza-Tobías, A.; Hernández-Barrera, L.; López-Olmedo, N.; García-Guerra, A.; Rodríguez-Ramírez, S.; Ramírez-Silva, I.; Villalpando, S.; Carriquiry, A.; Rivera, J.A. Usual vitamin intakes by Mexican populations. J. Nutr. 2016, 146, 1866–1873. [Google Scholar] [CrossRef] [PubMed]
- Bojar, I.; Owoc, A.; Humeniuk, E.; Fronczak, A.; Walecka, I. Quality of pregnant women’s diet in Poland-macro-elements. Arch. Med. Sci. 2014, 10, 361–365. [Google Scholar] [CrossRef] [PubMed]
- Ntandou, G.; Delisle, H.; Agueh, V.; Fayomi, B. Abdominal obesity explains the positive rural-urban gradient in the prevalence of the metabolic syndrome in Benin, West Africa. Nutr. Res. 2009, 29, 180–189. [Google Scholar] [CrossRef] [PubMed]
- Tsigga, M.; Filis, V.; Hatzopoulou, K.; Kotzamanidis, C.; Grammatikopoulou, M.G. Healthy eating index during pregnancy according to pre-gravid and gravid weight status. Public Health Nutr. 2011, 14, 290–296. [Google Scholar] [CrossRef] [PubMed]
- Potter, J.L.; Collins, C.E.; Brown, L.J.; Hure, A.J. Diet quality of Australian breast cancer survivors: A cross-sectional analysis from the Australian longitudinal study on women’s health. J. Hum. Nutr. Diet. 2014, 27, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Aljadani, H.M.; Patterson, A.; Sibbritt, D.; Hutchesson, M.J.; Jensen, M.E.; Collins, C.E. Diet quality, measured by fruit and vegetable intake, predicts weight change in young women. J. Obes. 2013, 2013, 525161. [Google Scholar] [CrossRef] [PubMed]
- Tobias, D.; Zhang, C.; Chavarro, J.; Olsen, S.; Bao, W.; Bjerregaard, A.; Fung, T.; Manson, J.; Hu, F. Healthful dietary patterns and long-term weight change among women with a history of gestational diabetes mellitus. Int. J. Obes. 2016. [Google Scholar] [CrossRef] [PubMed]
- Zamora, D.; Gordon-Larsen, P.; He, K.; Jacobs, D.R.; Shikany, J.M.; Popkin, B.M. Are the 2005 dietary guidelines for Americans associated with reduced risk of type 2 diabetes and cardiometabolic risk factors? Twenty-year findings from the cardia study. Diabetes Care 2011, 34, 1183–1185. [Google Scholar] [CrossRef] [PubMed]
- Lombard, C.; Deeks, A.; Jolley, D.; Teede, H.J. Preventing weight gain: The baseline weight related behaviors and delivery of a randomized controlled intervention in community based women. BMC Public Health 2009, 9, 2. [Google Scholar] [CrossRef] [PubMed]
- Lombard, C.B.; Harrison, C.L.; Kozica, S.L.; Zoungas, S.; Keating, C.; Teede, H.J. Effectiveness and implementation of an obesity prevention intervention: The HeLP-her rural cluster randomised controlled trial. BMC Public Health 2014, 14, 1471–2458. [Google Scholar] [CrossRef] [PubMed]
- Harrison, C.; Teede, H.; Kozica, S.; Zoungas, S.; Lombard, C. Individual, social and environmental factors and their association with weight in rural dwelling women of reproductive age. Aust. N. Z. J. Public Health 2016. [Google Scholar]
- Lombard, C.; Deeks, A.; Jolley, D.; Ball, K.; Teede, H. A low intensity, community based lifestyle programme to prevent weight gain in women with young children: Cluster randomized controlled trial. BMJ 2010, 341, c3215. [Google Scholar] [CrossRef] [PubMed]
- Lombard, C.; Harrison, C.; Kozica, S.; Zoungas, S.; Ranasinha, S.; Teede, H. Preventing weight gain in women in rural communities: A cluster randomised controlled trial. PLoS Med. 2016, 13, e1001941. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. Rural, Regional and Remote Health: A Guide to Remoteness Classifications; Australian Institute of Health and Welfare: Canberra, Australia, 2004. [Google Scholar]
- Australian Bureau of Statistics. 2033.0.55.001-Census of Population and Housing: Socio-Economic Indexes for Areas (SEIFA), Australia. 2011. Available online: http://www.abs.gov.au/websitedbs/censushome.nsf/home/seifa2011?opendocument&navpos=260 (accessed on 12 November 2016).
- Lombard, C.B.; Deeks, A.A.; Ball, K.; Jolley, D.; Teede, H.J. Weight, physical activity and dietary behavior change in young mothers: Short term results of the help-her cluster randomized controlled trial. Nutr. J. 2009, 8, 17. [Google Scholar] [CrossRef] [PubMed]
- Cancer Council Victoria. Dietary Questionnaire for Epidemiological Studies Version 2. Available online: http://www.cancervic.org.au/research/epidemiology/nutritional_assessment_services (accessed on 12 November 2016).
- Lewis, J.; Milligan, G.C.; Hunt, A. Nuttab 95: Nutrient Data Table for Use in Australia; Food Standards Australia New Zealand: Canberra, Australia, 1995. [Google Scholar]
- McNaughton, S.A.; Ball, K.; Crawford, D.; Mishra, G.D. An index of diet and eating patterns is a valid measure of diet quality in an Australian population. J. Nutr. 2008, 138, 86–93. [Google Scholar] [PubMed]
- National Health and Medical Research Council. Australian Dietary Guidelines; National Health and Medical Research Council: Canberra, Australia, 2013. [Google Scholar]
- National Health and Medical Research Council. Australian Guide to Healthy Eating. Available online: https://www.eatforhealth.gov.au/guidelines/australian-guide-healthy-eating (accessed on 20 October 2016).
- Jessri, M.; Lou, W.Y.; L’Abbé, M.R. Evaluation of different methods to handle misreporting in obesity research: Evidence from the Canadian national nutrition survey. Br. J. Nutr. 2016, 115, 147–159. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. 4363.0.55.001—Australian Health Survey: Users’ Guide, 2011–13 Under-Reporting in Nutrition Surveys. Available online: http://www.abs.gov.au/ausstats/abs@.nsf/Lookup/4363.0.55.001Chapter651512011-13 (accessed on 8 September 2016).
- Schofield, W. Predicting basal metabolic rate, new standards and review of previous work. Hum. Nutr. Clin. Nutr. 1984, 39, 5–41. [Google Scholar]
- Black, A.E. Critical evaluation of energy intake using the Goldberg cut-off for energy intake: Basal metabolic rate. A practical guide to its calculation, use and limitations. Int. J. Obes. 2000, 24, 1119. [Google Scholar] [CrossRef]
- Stata Statistical Software: Release 12, StataCorp: College Station, TX, USA, 2011.
- Lutfiyya, M.N.; Chang, L.F.; Lipsky, M.S. A cross-sectional study of US rural adults’ consumption of fruits and vegetables: Do they consume at least five servings daily. BMC Public Health 2012, 12, 1. [Google Scholar] [CrossRef] [PubMed]
- Suliga, E. Nutritional behaviours of pregnant women in rural and urban environments. Ann. Agric. Environ. Med. 2015, 22. [Google Scholar] [CrossRef] [PubMed]
- Trivedi, T.; Liu, J.; Probst, J.; Merchant, A.; Jhones, S.; Martin, A. Obesity and obesity-related behaviors among rural and urban adults in the USA. Rural. Remote. Health 2015, 15, 3267. [Google Scholar] [PubMed]
- Collins, C.E.; Young, A.F.; Hodge, A. Diet quality is associated with higher nutrient intake and self-rated health in mid-aged women. J. Am. Coll. Nutr. 2008, 27, 146–157. [Google Scholar] [CrossRef] [PubMed]
- Kant, A.K. Dietary patterns and health outcomes. J. Am. Diet. Assoc. 2004, 104, 615–635. [Google Scholar] [CrossRef] [PubMed]
- Miller, J.; Chan, L.; Mehta, K.; Roberts, R.; Dickinson, K.M.; Yaxley, A.; Matwiejczyk, L.; Thomas, J.; Wray, A.; Jackson, K. Dietary intake of working women with children does not appear to be influenced by hours of employment: A secondary analysis of the Australian health survey (2011–2013). Appetite 2016, 105, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Ralston, R.A.; Truby, H. Influence of food cost on diet quality and risk factors for chronic disease: A systematic review. Nutr. Diet. 2011, 68, 248–261. [Google Scholar] [CrossRef]
- Rao, M.; Afshin, A.; Singh, G.; Mozaffarian, D. Do healthier foods and diet patterns cost more than less healthy options? A systematic review and meta-analysis. BMJ Open 2013, 3, e004277. [Google Scholar] [CrossRef] [PubMed]
- Grant, D.K.; Maxwell, S. Food coping strategies: A century on from rowntree. Nutr. Health 1999, 13, 45–60. [Google Scholar] [CrossRef] [PubMed]
- Black, A.P.; Brimblecombe, J.; Eyles, H.; Morris, P.; Vally, H.; O’Dea, K. Food subsidy programs and the health and nutritional status of disadvantaged families in high income countries: A systematic review. BMC Public Health 2012, 12, 1099. [Google Scholar] [CrossRef] [PubMed]
- McFadden, A.; Green, J.M.; Williams, V.; McLeish, J.; McCormick, F.; Fox-Rushby, J.; Renfrew, M.J. Can food vouchers improve nutrition and reduce health inequalities in low-income mothers and young children: A multi-method evaluation of the experiences of beneficiaries and practitioners of the healthy start programme in England. BMC Public Health 2014, 14, 148. [Google Scholar] [CrossRef] [PubMed]
- Odoms-Young, A.M.; Kong, A.; Schiffer, L.A.; Porter, S.J.; Blumstein, L.; Bess, S.; Berbaum, M.L.; Fitzgibbon, M.L. Evaluating the initial impact of the revised special supplemental nutrition program for women, infants, and children (WIC) food packages on dietary intake and home food availability in African-American and hispanic families. Public Health Nutr. 2014, 17, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Dennis, B.; Pajak, A.; Pardo, B.; Davis, C.; Williams, O.; Piotrowski, W. Weight gain and its correlates in Poland between 1983 and 1993. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 1507. [Google Scholar] [CrossRef] [PubMed]
- Hruby, A.; Manson, J.E.; Qi, L.; Malik, V.S.; Rimm, E.B.; Sun, Q.; Willett, W.C.; Hu, F.B. Determinants and consequences of obesity. Am. J. Public Health 2016, 106, 1656–1662. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. Rural, Regional and Remote Health: Indicators of Health Status and Determinants of Health Rural Health Series, 9th ed.; Australian Institute of Health and Welfare: Canberra, Australia, 2008; p. 9. [Google Scholar]
- Mishra, G.; Ball, K.; Patterson, A.; Brown, W.; Hodge, A.; Dobson, A. Socio-demographic inequalities in the diets of mid-aged Australian women. Eur. J. Clin. Nutr. 2005, 59, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Kubberød, E.; Ueland, Ø.; Tronstad, Å.; Risvik, E. Attitudes towards meat and meat-eating among adolescents in Norway: A qualitative study. Appetite 2002, 38, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Dietary Assessment Primer. Food Frequency Questionnaire at a Glance. Available online: http://dietassessmentprimer.cancer.gov/profiles/questionnaire/ (accessed on 27 January 2016).
- Hodge, A.; Patterson, A.J.; Brown, W.J.; Ireland, P.; Giles, G. The anti cancer council of Victoria FFQ: Relative validity of nutrient intakes compared with weighed food records in young to middle-aged women in a study of iron supplementation. Aust. N. Z. J. Public Health 2000, 24, 576–583. [Google Scholar] [CrossRef] [PubMed]
- Ireland, P.; Jolley, D.; Giles, G.; O’Dea, K.; Powles, J.; Rutishauser, I.; Wahlqvist, M.L.; Williams, J. Development of the Melbourne FFQ: A food frequency questionnaire for use in an Australian prospective study involving an ethnically diverse cohort. Asia Pacific J. Clin. Nutr. 1994, 3, 19–31. [Google Scholar]
- Bodnar, L.M.; Siega-Riz, A.M. A diet quality index for pregnancy detects variation in diet and differences by sociodemographic factors. Public Health Nutr. 2002, 5, 801–809. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| 2013 Australian Dietary Guidelines | DGI Component and Description | Maximum Score (10) | Intermediate Score (5) | No (0) |
|---|---|---|---|---|
| Enjoy a wide variety of nutritious foods | Dietary variety: proportion of foods for each core food group that were consumed at least once per week | 100% | 50% | 0% |
| Eat plenty of vegetables, legumes and fruits | Vegetables: servings of vegetables and legumes per day | ≥5 | 2.5 | 0 |
| Fruit: servings of fruit per day | ≥2 | 1 | 0 | |
| Eat plenty of cereals (including breads, rice, pasta and noodles), preferably wholegrain | Breads and cereals: frequency of consumption of breads and cereals per day | ≥6 | 3 | 0 |
| Wholegrain cereals: proportion of whole meal/wholegrain bread consumed relative to total bread | 100% | 50% | 0% | |
| Include lean meat, fish, poultry or alternatives | Meat and meat alternatives: frequency of consumption of lean meats and alternatives per day | ≥2.5 | 1.25 | 0 |
| Lean protein sources: proportion of lean meats & alternatives relative to total meats and alternatives | 100% | 50% | 0% | |
| Include milks, yoghurts, cheeses and/or alternatives Reduced fat varieties should be chosen, where possible | Dairy: frequency of consumption of dairy products per day | ≥2.5 | 1.25 | 0 |
| Saturated fat intake: type of milk usually consumed | Low fat milk | Whole milk | ||
| Limit saturated fat intake and moderate total fat intake | Saturated fat intake: type of milk usually consumed | Low fat milk | Whole milk | |
| Limit your alcohol intake if you choose to drink | Alcohol: frequency of consumption of all alcoholic beverages per day | ≤1 | 1.5 | ≥2 |
| Consume only moderate amounts of sugars and foods containing added sugars | Added sugars: frequency of consumption of soft drink, cordial, fruit juice, jam, chocolate, confectionary per day | <1.25 | 1.25 | >1.25 |
| Prevent weight gain: by being physically active and eating according to your energy needs | Extra foods: frequency of consumption of extra foods per day | <2.5 | 2.5 | >2.5 |
| TOTAL DGI SCORE | 0–130 |
| Variables | Urban (n = 149) | Rural (n = 394) | p-Value |
|---|---|---|---|
| Age (years) | 40.4 ± 4.4 | 39.7 ± 6.4 | 0.227 |
| BMI (kg/m2) | 27.6 ± 5.6 | 27.7 ± 6.0 | 0.860 |
| Employment | |||
| Working | 96 (64.9%) | 291 (74.8%) | 0.093 |
| Not working | 52 (35.1%) | 98 (25.2%) | |
| Marital status | |||
| Never married | 4 (2.7%) | 24 (6.1%) | 0.306 |
| Married | 131 (87.9%) | 338 (86.2%) | |
| No longer married | 14 (9.4%) | 30 (7.7%) | |
| Education | |||
| No formal | 67 (45.0%) | 60 (15.4%) | <0.001 |
| Trade/apprentice a | 39 (26.2%) | 185 (47.3%) | |
| University degree or higher | 43(28.9%) | 146 (37.3%) | |
| Income | |||
| ≤$AUD40,000 | 28 (21.7%) | 77 (20.6%) | 0.792 |
| $AUD41–80,000 | 60 (46.5%) | 164 (43.9%) | |
| $AUD80,000 and above | 41 (31.8%) | 133 (35.6%) |
| Nutrients | Urban (n = 149) | Rural (n = 394) | Unadjusted β (95% Confidence Interval) (CI) | p-Value | Adjusted a β (95% CI) | p-Value |
|---|---|---|---|---|---|---|
| Energy (kJ/day) | 7644.3 ± 1905.9 | 7965.4 ± 1930.5 | 321.1 (−38.7, 680.9) | 0.079 | 360.8 (−42.4, 764.1) | 0.078 |
| Protein (g/day) | 87.2 ± 26.2 | 93.7 ± 28.6 | 6.5 (2.2, 10.8) | 0.004 | 7.0 (1.7, 12.3) | 0.010 |
| % Protein | 19.3 | 20 | 0.007 (0.0002, 0.01) | 0.044 | 0.007 (−0.0006, 0.01) | 0.073 |
| CHO (g/day) | 188.1 ± 52.0 | 189.1 ± 51.1 | 1.0 (−10.1, 12.1) | 0.857 | 2.5 (−9.2, 14.2) | 0.668 |
| % CHO | 39.4 | 38 | −0.01(−0.03, −0.001) | 0.031 | −0.01 (−0.03, 0.0005) | 0.059 |
| Fat (g/day) | 73.5 ± 23.7 | 79.3 ± 23.3 | 5.8 (0.79, 10.7) | 0.024 | 6.7 (1.6, 11.8) | 0.011 |
| % Fat | 35.3 | 36.6 | 0.01 (0.002, 0.02) | 0.026 | 0.02 (0.006, 0.03) | 0.004 |
| SFA (g/day) | 29.3 ± 11.0 | 32.9 ± 11.3 | 3.6 (1.0, 6.1) | 0.007 | 3.9 (1.4, 6.3) | 0.003 |
| % SFA | 14 | 15.1 | 0.01 (0.004, 0.02) | 0.003 | 0.01 (0.006, 0.02) | <0.001 |
| MUFA (g/day) | 26.3 ± 9.1 | 28.5 ± 8.6 | 2.2 (0.49, 3.9) | 0.012 | 2.6 (0.81, 4.3) | 0.005 |
| % MUFA | 12.6 | 13.1 | 0.005 (0.0008, 0.01) | 0.022 | 0.007 (0.002, 0.01) | 0.005 |
| PUFA (g/day) | 11.4 ± 4.6 | 11.0 ± 4.1 | −0.40 (−1.1, 0.34) | 0.282 | −0.17 (−0.96, 0.62) | 0.670 |
| % PUFA | 5.5 | 5.1 | −0.004 (−0.006, −0.001) | 0.003 | −0.003 (−0.005, −0.0004) | 0.023 |
| Fibre (g/day) | 21.3 ± 7.0 | 21.6 ± 6.1 | 0.34 (−0.95, 1.6) | 0.600 | 0.46 (−0.77, 1.7) | 0.459 |
| Cholesterol (mg/day) | 267.0 ± 106.7 | 314.6 ± 112.4 | 47.6 (24.7, 70.6) | <0.001 | 49.4 (25.4, 73.4) | <0.001 |
| GI | 52.2 ± 3.6 | 50.9 ± 4.0 | −1.3 (−2.0, −0.64) | <0.001 | −0.76 (−1.6, 0.04) | 0.062 |
| GL | 97.8 ± 29.5 | 96.1 ± 29.9 | −1.7 (−8.4, 4.9) | 0.601 | 0.11 (−6.9, 7.1) | 0.974 |
| Calcium (mg/day) | 897.7 ± 272.5 | 925.4 ± 273.0 | 27.7 (−15.7, 71.0) | 0.207 | 4.0 (−38.6, 46.6) | 0.850 |
| Iron (mg/day) | 12.6 ± 4.0 | 13.6 ± 4.0 | 0.97 (0.43, 1.5) | 0.001 | 1.1 (0.48, 1.6) | 0.001 |
| Folate (µg/day) | 257.1 ± 80.4 | 267.1 ± 79.8 | 10.0 (−1.8, 21.8) | 0.094 | 9.6 (−2.3, 21.5) | 0.113 |
| Sodium (mg/day) | 2517.5 ± 779.5 | 2525.0 ± 756.9 | 7.5 (−138.6, 153.6) | 0.918 | 30.5 (−142.5, 203.5) | 0.725 |
| DGI and Components | Urban (n = 149) DGI Score | Rural (n = 394) DGI Score | Unadjusted β (95% Confidence Interval) (CI) | p-Value | Adjusted a β (95% Confidence Interval) (CI) | p-Value |
|---|---|---|---|---|---|---|
| Dietary variety | 0.66 ± 0.08 | 0.65 ± 0.10 | −0.01 (−0.03, 0.007) | 0.206 | −0.02 (−0.04, 0.001) | 0.066 |
| Vegetables | 2.2 ± 0.96 | 2.4 ± 1.0 | 0.15 (−0.01, 0.32) | 0.073 | 0.15 (−0.07, 0.36) | 0.174 |
| Fruit | 1.6 ± 0.97 | 1.6 ± 1.0 | −0.03 (−0.20, 0.15) | 0.770 | 0.0004 (−0.17, 0.18) | 0.996 |
| Wholegrain cereals | 0.68 ± 0.46 | 0.69 ± 0.46 | 0.04 (−0.36, 0.44) | 0.832 | −0.11 (−0.58, 0.36) | 0.636 |
| Breads and cereals | 4.4 ± 1.6 | 4.2 ± 1.6 | −0.25 (−0.54, 0.04) | 0.086 | −0.18 (−0.55, 0.19) | 0.336 |
| Meat and meat alternatives | 2.1 ± 1.2 | 2.4 ± 1.3 | 0.33 (0.12, 0.53) | 0.002 | 0.37 (0.14, 0.61) | 0.003 |
| Lean protein sources | 0.83 ± 0.12 | 0.82 ± 0.10 | −0.03 (−0.17, 0.11) | 0.668 | 0.004 (−0.14, 0.14) | 0.952 |
| Dairy | 1.7 ± 0.72 | 1.8 ± 0.72 | 0.10 (−0.03, 0.23) | 0.128 | 0.04 (−0.08, 0.16) | 0.546 |
| Low fat/skim milk whole milk (frequency & percentage) (%) | ||||||
| Whole milk | 54 (36.2%) | 170 (43.2%) | ||||
| Low fat/skim milk | 95 (63.8%) | 224 (56.9%) | 0.75 (0.48, 1.2) | 0.193 | 0.63 (0.38, 1.1) | 0.081 |
| Saturated fat Low fat/skim milk whole milk (frequency & percentage) (%) | ||||||
| Whole milk | 54 (36.2%) | 170 (43.2%) | ||||
| Low fat/skim milk | 95 (63.8%) | 224 (56.9%) | 0.75 (0.48, 1.2) | 0.193 | 0.63 (0.38, 1.1) | 0.081 |
| Extra foods b | 4.4 ± 1.9 | 4.6 ± 2.2 | 0.12 (−0.34, 0.57) | 0.612 | 0.08 (−0.38, 0.54) | 0.727 |
| DGI total | 84.8 ± 15.9 | 83.9 ± 16.5 | −0.90 (−4.4, 2.6) | 0.606 | −1.8 (−5.1, 1.4) | 0.264 |
| Variables | Unadjusted β (95% CI) | p-Value | Adjusted b β (95% CI) | p-Value |
|---|---|---|---|---|
| Rural status | −0.90 (−4.4, 2.6) | 0.606 | −1.8 (−5.1, 1.4) | 0.264 |
| Age (years) | 0.26 (0.06, 0.46) | 0.012 | 0.25 (−0.02, 0.52) | 0.068 |
| BMI (kg/m2) | 0.03 (−0.21, 0.26) | 0.805 | 0.12 (−0.12, 0.36) | 0.324 |
| Employment | ||||
| Working | Ref (1) | |||
| Not working | −5.6 (−9.1, −2.0) | 0.003 | −4.1 (−8.1, −0.14) | 0.043 |
| Marital status | ||||
| Married | Ref (1) | |||
| Never married | 3.0 (−3.6, 9.7) | 0.367 | 1.8 (−5.8, 9.3) | 0.639 |
| No longer married | −0.71 (−8.9, 7.5) | 0.862 | −3.0 (−7.9, 1.9) | 0.225 |
| Education | ||||
| No formal | Ref (1) | |||
| Trade/apprentice a | 0.61 (−2.6, 3.8) | 0.703 | 0.82 (−3.7, 5.4) | 0.720 |
| University degree and higher | 4.1 (0.90, 7.3) | 0.013 | 3.3 (−0.94, 7.6) | 0.124 |
| Income | ||||
| $≤AUD40,000 | Ref (1) | |||
| $AUD41–80,000 | 3.8 (0.46, 7.1) | 0.026 | 2.6 (−1.2, 6.5) | 0.176 |
| $AUD80,000 and above | 7.6 (3.6, 11.6) | <0.001 | 5.5 (1.2, 9.8) | 0.013 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martin, J.C.; Moran, L.J.; Teede, H.J.; Ranasinha, S.; Lombard, C.B.; Harrison, C.L. Exploring Diet Quality between Urban and Rural Dwelling Women of Reproductive Age. Nutrients 2017, 9, 586. https://doi.org/10.3390/nu9060586
Martin JC, Moran LJ, Teede HJ, Ranasinha S, Lombard CB, Harrison CL. Exploring Diet Quality between Urban and Rural Dwelling Women of Reproductive Age. Nutrients. 2017; 9(6):586. https://doi.org/10.3390/nu9060586
Chicago/Turabian StyleMartin, Julie C., Lisa J. Moran, Helena J. Teede, Sanjeeva Ranasinha, Catherine B. Lombard, and Cheryce L. Harrison. 2017. "Exploring Diet Quality between Urban and Rural Dwelling Women of Reproductive Age" Nutrients 9, no. 6: 586. https://doi.org/10.3390/nu9060586
APA StyleMartin, J. C., Moran, L. J., Teede, H. J., Ranasinha, S., Lombard, C. B., & Harrison, C. L. (2017). Exploring Diet Quality between Urban and Rural Dwelling Women of Reproductive Age. Nutrients, 9(6), 586. https://doi.org/10.3390/nu9060586