A Systematic Review of Fatalities Related to Acute Ingestion of Salt. A Need for Warning Labels?

Abstract
:1. Introduction
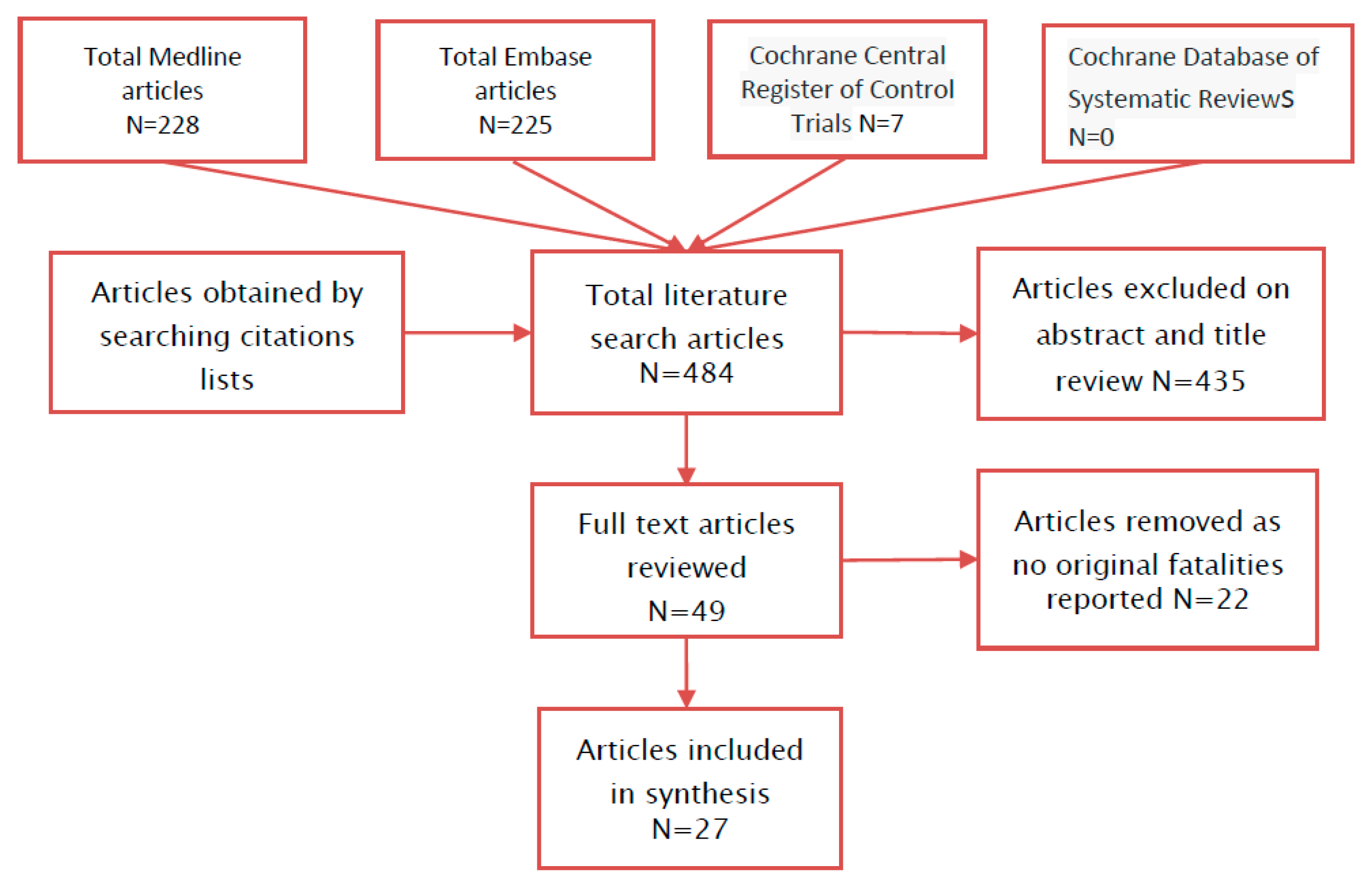
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Institute for Health Metrics and Evaluation. GDB Compare; Electronic Citation; Institute for Health Metrics and Evaluation: Seattle, WA, USA, 2015. [Google Scholar]
- Moder, K.G.; Hurley, D.L. Fatal hypernatremia from exogenous salt intake: Report of a case and review of the literature. Mayo Clin. Proc. 1990, 65, 1587–1594. [Google Scholar] [CrossRef]
- #Salt4Syria. Available online: http://www.salt4syria.com/challenge-accepted/category/take-the-challenge (accessed on 10 April 2017).
- Engjom, T.; Kildahl-Andersen, O. An 83-year-old woman with coma and severe hypernatremia. Tidsskr. Nor. Laegeforen. 2008, 128, 316–317. [Google Scholar] [PubMed]
- Raya, A.; Giner, P.; Aranegui, P.; Guerrero, F.; Vazquez, G. Fatal acute hypernatremia caused by massive intake of salt. Arch. Intern. Med. 1992, 152, 640–646. [Google Scholar] [CrossRef] [PubMed]
- Turk, E.E.; Schulz, F.; Koops, E.; Gehl, A.; Tsokos, M. Fatal hypernatremia after using salt as an emetic—Report of three autopsy cases. Leg. Med. (Tokyo) 2005, 7, 47–50. [Google Scholar] [CrossRef] [PubMed]
- Johnston, J.G.; Robertson, W.O. Fatal ingestion of table salt by an adult. West. J. Med. 1977, 126, 141–143. [Google Scholar] [PubMed]
- Nunez Bacarreza, J.J.; Remolina Schlig, M.; Zuñiga Rivera, A.; Posadas Callejas, J. Severe hypernatremia due to sodium chloride intake. Med. Intensiv. 2008, 32, 258–259. [Google Scholar]
- Ofran, Y.; Lavi, D.; Opher, D.; Weiss, T.A.; Elinav, E. Fatal voluntary salt intake resulting in the highest ever documented sodium plasma level in adults (255 mmol L−1): A disorder linked to female gender and psychiatric disorders. J. Intern. Med. 2004, 256, 525–528. [Google Scholar] [CrossRef] [PubMed]
- Robertson, W.O. A further warning on the use of salt as an emetic agent. J. Pediatr. 1971, 79, 877. [Google Scholar] [CrossRef]
- Hey, A.; Hickling, K.G. Accidental salt poisoning. N. Z. Med. J. 1982, 95, 864. [Google Scholar] [PubMed]
- Hedouin, V.; Révuelta, E.; Bécart, A.; Tournel, G.; Deveaux, M.; Gosset, D. A case of fatal salt water intoxication following an exorcism session. Forensic Sci. Int. 1999, 99, 1–4. [Google Scholar] [CrossRef]
- Bird, C.A.; Gardner, A.W.; Roylance, P.J. Letter: Danger of saline emetics in first-aid for poisoning. Br. Med. J. 1974, 4, 103. [Google Scholar] [CrossRef] [PubMed]
- Ward, D.J. Fatal hypernatremia after a saline emetic. Br. Med. J. 1963, 2, 432. [Google Scholar] [CrossRef] [PubMed]
- Gresham, G.A.; Mashru, M.K. Fatal poisoning with sodium chloride. Forensic Sci. Int. 1982, 20, 87–88. [Google Scholar] [CrossRef]
- Laurence, B.H.; Hopkins, B.E. Hypernatraemia following a saline emetic. Med. J. Aust. 1969, 1, 1301–1303. [Google Scholar] [PubMed]
- Goodbody, R.A.; Middleton, J.E.; Gamlen, T.R. Saline emetics and hypernatraemia: Report on 2 fatalities. Med. Sci. Law 1975, 15, 261–264. [Google Scholar] [PubMed]
- Winter, M.; Taylor, D.J. Letter: Danger of saline emetics in first-aid for poisoning. Br. Med. J. 1974, 3, 802. [Google Scholar] [CrossRef] [PubMed]
- Roberts, C.J.; Noakes, M.J. Fatal outcome from administration of a salt emetic. Postgrad. Med. J. 1974, 50, 513–515. [Google Scholar] [CrossRef] [PubMed]
- Kupiec, T.C.; Goldenring, J.M.; Raj, V. A non-fatal case of sodium toxicity. J. Anal. Toxicol. 2004, 28, 526–528. [Google Scholar] [CrossRef] [PubMed]
- Dockery, W.K. Fatal intentional salt poisoning associated with a radiopaque mass. Pediatrics 1992, 89, 964–965. [Google Scholar] [PubMed]
- Martos Sanchez, I.; Ros Pérez, P.; Otheo de Tejada, E.; Vázquez Martínez, J.L.; Pérez-Caballero, C.; Fernández Pineda, L. Fatal hypernatremia due to accidental administration of table salt. An. Esp. Pediatr. 2000, 53, 495–498. [Google Scholar] [PubMed]
- Scott, E.P.; Rotondo, C.C. Salt intoxication; accidental ingestion of a large amount of sodium chloride; report of a case with autopsy of a two year old infant. Ky. Med. J. 1947, 45, 107–109. [Google Scholar] [PubMed]
- Barer, J.; Hill, L.L.; Hill, R.M.; Martinez, W.M. Fatal poisoning from salt used as an emetic. Am. J. Dis. Child. 1973, 125, 889–890. [Google Scholar] [CrossRef] [PubMed]
- Streat, S. Fatal salt poisoning in a child. N. Z. Med. J. 1982, 95, 285–286. [Google Scholar] [PubMed]
- Finberg, L.; Kiley, J.; Luttrell, C.N. Mass accidental salt poisoning in infancy. A study of a hospital disaster. JAMA 1963, 184, 187–190. [Google Scholar] [CrossRef] [PubMed]
- Rogers, D.; Tripp, J.; Bentovim, A.; Robinson, A.; Berry, D.; Goulding, R. Papers and originals: Non-accidental poisoning: An extended syndrome of child abuse. Br. Med. J. 1976, 1, 793–796. [Google Scholar] [CrossRef] [PubMed]
- Meadow, R. Non-accidental salt poisoning. Arch. Dis. Child. 1993, 68, 448–452. [Google Scholar] [CrossRef] [PubMed]
- Smith, E.J.; Palevsky, S. Salt poisoning in a two-year-old child. Am. J. Emerg. Med. 1990, 8, 571–572. [Google Scholar] [CrossRef]
- ScienceLab.com. Material Safety Data Sheet. Sodium Chloride MSDS. Available online: http://www.sciencelab.com/msds.php?msdsId=9927593 (accessed on 11 April 2017).
- Hipgrave, D.B.; Chang, S.; Li, X.; Wu, Y. Salt and sodium intake in China. JAMA 2016, 315, 703–705. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.; Li, W.; Wang, Y.; Chen, H.; Bo, J.; Wang, X.; Liu, L. Validation and assessment of three methods to estimate 24-h urinary sodium excretion from spot urine samples in chinese adults. PLoS ONE 2016, 11, e0149655. [Google Scholar] [CrossRef] [PubMed]
- Sterns, R.H. Disorders of plasma sodium—Causes, consequences, and correction. N. Engl. J. Med. 2015, 372, 55–65. [Google Scholar] [CrossRef] [PubMed]
- Campbell, N.R.; Correa-Rotter, R.; Cappuccio, F.P.; Webster, J.; Lackland, D.T.; Neal, B.; MacGregor, G.A. Proposed nomenclature for salt intake and for reductions in dietary salt. J. Clin. Hypertens. (Greenwich) 2015, 17, 247–251. [Google Scholar] [CrossRef] [PubMed]
- Kelly, T.N.; He, J. Genomic epidemiology of blood pressure salt sensitivity. J. Hypertens. 2012, 30, 861–873. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food, Drug Administration. Select Committee on GRAS Substances (SCOGS) Opinion: Sodium Chloride. 2015. Available online: https://www.fda.gov/food/ingredientspackaginglabeling/gras/scogs/ucm260741.htm (accessed on 11 April 2017).
- Carlberg, D.J.; Borek, H.A.; Syverud, S.A.; Holstege, C.P. Survival of acute hypernatremia due to massive soy sauce ingestion. J. Emerg. Med. 2013, 45, 228–231. [Google Scholar] [CrossRef] [PubMed]
- Karppanen, H.; Mervaala, E. Sodium Intake and Hypertension. Prog. Cardiovasc. Dis. 2006, 49, 59–75. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Afshin, A.; Benowitz, N.L.; Bittner, V.; Daniels, S.R.; Franch, H.A.; Jacobs, D.R., Jr.; Kraus, W.E.; Kris-Etherton, P.M.; Krummel, D.A.; et al. Population approaches to improve diet, physical activity, and smoking habits: A scientific statement from the American heart association. Circulation 2012, 126, 1514–1563. [Google Scholar] [CrossRef] [PubMed]
- Pinjuh Markota, N.; Rumboldt, M.; Rumboldt, Z. Emphasized warning reduces salt intake: A randomized controlled trial. J. Am. Soc. Hypertens. 2015, 9, 214–220. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| 1. | ((toxic* or intoxic* or overdos*) adj5 salt).mp |
| 2. | ((toxic* or intoxic* or overdos*) adj5 Na).mp |
| 3. | ((toxic* or intoxic* or overdos*) adj5 sodium).mp |
| 4. | ((salt* or Na or sodium) adj5 overdos*).mp |
| 5. | hypernatremia.mp |
| 6. | hypernatremia/ |
| 7. | 1 or 2 or 3 or 4 or 5 or 6 |
| 8. | ((dietar* or intake* or food* or consumption or consume* or ingest*) adj5 sodium).mp |
| 9. | ((dietar* or intake* or food* or consumption or consume* or ingest*) adj5 salt).mp |
| 10. | ((dietar* or intake* or food* or consumption or consume* or ingest*) adj5 Na).mp |
| 11. | 8 or 9 or 10 |
| 12. | 7 and 11 |
| 13. | Limit 12 to humans |
| First Author Year of Publication | Age (Years) | Gender | Explanation of Overdose | Estimated Dose Ingested Sodium (g) * | Highest Reported Blood Level of Sodium (mmol/L) ** | Co-Ingestion of Other Potential Toxins | Chronic Illness |
|---|---|---|---|---|---|---|---|
| Engjom 2008 [4] | 83 | Female | Mistaken for sugar | 13.6–20.4 g | 223 | None stated | Hypertension, dementia |
| Raya 1992 [5] | 36 | Female | Exorcism ritual | 273 g | 246 | Sodium bicarbonate * | None stated |
| Turk 2005 [6] | 34 | Female | Health care professional administered emetic | 80 g | 196 | None stated | “Psychomotor retardation” |
| 69 | Male | Health care professional administered emetic | 39.4–81.6 g | 175 | Single table of unprescribed “neuroleptic” | Schizophrenia | |
| Moder 1990 [2] | 41 | Male | Mistaken for sugar | 27.1–34.8 g | 209 | None stated | Downs Syndrome, lymphoma, hepatitis B, seizures |
| Johnston 1977 [7] | 45 | Female | Mistaken for sugar | 30.6–40.8 g | 190 | None stated | Prader-Willi Syndrome, hypertension obesity, impaired glucose tolerance |
| Bacarreza 2008 [8] | 33 | Female | Not known | 50 g | 203 | None stated | Alcohol abuse |
| Ofran 2004 [9] | 20 | Female | Exorcism ritual | <400 g | 255 | None stated | Depression |
| Robertson 1971 [10] | 23 | Female | Emetic | Not stated | 214 | Chlordiazepoxide overdose | None stated |
| Hey 1982 [11] | 56 | Female | Emetic | 27.2–47.2 g | 214 | “trivial” overdose | Not stated |
| Hedouin 1999 [12] | 19 | Female | Exorcism ritual | Not stated | 153 | None stated | Hydrocephalus, seizures |
| Bird 1974 [13] | 35 | Female | Emetic | 20.4 g | 200 | “Overdose” | “Psychiatric patient” |
| Ward 1963 [14] | 74 | Male | Emetic | 13.6–24.4 g | 174 | Accidental overdose of imipramine and perphenazine | “Mild depression” |
| Gresham 1982 [15] | 48 | Female | Emetic | 6.8–10.2 g | 166 | “Extra dose” of chlorpromazine | Past leucotomy, depression |
| Laurence 1969 [16] | 35 | Female | Emetic | 69 g | 184 | Overdose thioridazine | None stated |
| Goodbody 1975 [17] | 35 | Female | Emetic and lavage | >17.7 g | 226 *** | “Minor” overdose sodium amytal | None stated |
| 44 | Female | Emetic | Not stated | 151 | Overdose sodium amytal | None stated | |
| Winter 1974 [18] | 21 | Female | Emetic and lavage | 118–236 g | 227 | Amitriptyline, imipramine, chlorpromazine, diazepam and nitrazepam overdose | Psychiatric disease |
| Roberts 1974 [19] | 26 | Female | Emetic | 27–60 g | 172 | Salicylate overdose | Depression |
| First Author, Year of Publication | Age (Years) (Months) (Weeks) (Days) | Gender | Explanation of Overdose | Estimated Dose Ingested Sodium (g) * | Highest Reported Serum Level of Sodium (mmol/L) ** | Co-Ingestion of Other Potential Toxins | Chronic Illness |
|---|---|---|---|---|---|---|---|
| Dockery 1992 [21] | 5 years | Female | Parental administration | 11.4 g | 220 | None stated | “Poor growth” |
| Turk 2005 [6] | 4 years | Female | Emesis | Not stated | 245 | None stated | Low body weight |
| Martos Sanchez 2000 [22] | 20 months | Female | Mistaken for sugar | 9.12 g | 195 | None stated | None stated |
| 7 months | Female | Accidental | 5.03 g | 178 | None stated | None stated | |
| Scott 1947 [23] | 2 years | Male | Mistaken for sugar | <7 g | Not stated | None stated | Gastrointestinal strictures |
| Barer 1973 [24] | 3 years | Male | Emetic and lavage | Not stated | 188 | Aspirin overdose | None stated |
| Streat 1982 [25] | 2 years | Female | Emetic | Not stated | 204 | Pheniramine overdose | None stated |
| Finberg 1963 [26] | 7 days | Male | Mistaken for sugar | Not stated | Not stated | None stated | Prematurity |
| 2 months | Female | Mistaken for sugar | Not stated | Not stated | None stated | Congenital neuroblastoma | |
| 3 weeks | Male | Mistaken for sugar | Not stated | Not stated | None stated | None stated | |
| 5 days | Female | Mistaken for sugar | Not stated | Not stated | None stated | None stated | |
| 2 days | Female | Mistaken for sugar | Not stated | Not stated | None stated | None stated | |
| 1 day | Female | Mistaken for sugar | Not stated | 244 | None stated | None stated | |
| Rogers 1976 [27] | 1 year | Female | Parental administration | Not stated | 200 | None stated | Repeated abscesses |
| Meadow 1993 [28] *** | 1.5–9 months | Half were female | Parental administration | Not stated | Not stated | Not stated | Not stated |
| Smith 1990 [29] | 26 months | Not stated | Emetic for minor overdose | 6.8–13.6 g | 217 | None stated | None stated |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campbell, N.R.C.; Train, E.J. A Systematic Review of Fatalities Related to Acute Ingestion of Salt. A Need for Warning Labels? Nutrients 2017, 9, 648. https://doi.org/10.3390/nu9070648
Campbell NRC, Train EJ. A Systematic Review of Fatalities Related to Acute Ingestion of Salt. A Need for Warning Labels? Nutrients. 2017; 9(7):648. https://doi.org/10.3390/nu9070648
Chicago/Turabian StyleCampbell, Norm R. C., and Emma J. Train. 2017. "A Systematic Review of Fatalities Related to Acute Ingestion of Salt. A Need for Warning Labels?" Nutrients 9, no. 7: 648. https://doi.org/10.3390/nu9070648
APA StyleCampbell, N. R. C., & Train, E. J. (2017). A Systematic Review of Fatalities Related to Acute Ingestion of Salt. A Need for Warning Labels? Nutrients, 9(7), 648. https://doi.org/10.3390/nu9070648