Iron Fortified Complementary Foods Containing a Mixture of Sodium Iron EDTA with Either Ferrous Fumarate or Ferric Pyrophosphate Reduce Iron Deficiency Anemia in 12- to 36-Month-Old Children in a Malaria Endemic Setting: A Secondary Analysis of a Cluster-Randomized Controlled Trial

 ,
,
Abstract
:1. Introduction
2. Subjects and Methods
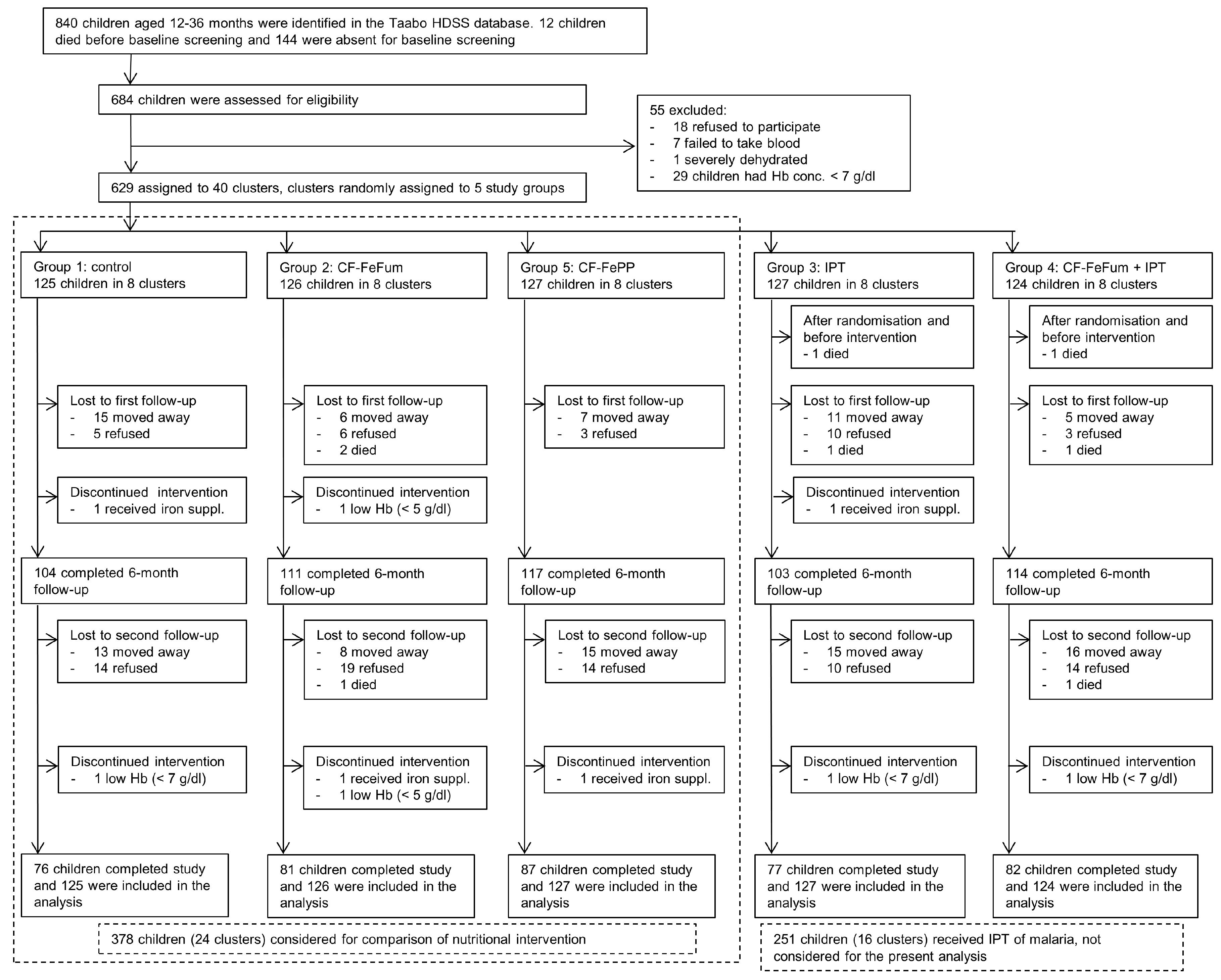
2.1. Study Site and Participants
2.2. Study Design and Procedure
2.3. CF Production, Preparation, and Child Feeding
2.4. Blinding of Treatments
2.5. Follow-Up
2.6. Laboratory Methods
2.7. Statistical Analysis
3. Results
3.1. Participant Characteristics and Compliance
3.2. Hb Concentration and Anemia Prevalence
3.3. PF and Prevalence of ID
3.4. P. falciparum Prevalence and Inflammation
4. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| AA | ascorbic acid |
| AGP | α-1-acid glycoprotein |
| CF | complementary food |
| CRP | C-reactive protein |
| FAO | Food and Agriculture Organization |
| Fe | iron |
| FeFum | ferrous fumarate |
| FePP | ferric pyrophosphate |
| Hb | hemoglobin |
| HDSS | health and demographic surveillance system |
| ID | iron deficiency |
| IDA | iron deficiency anemia |
| IPT | intermittent preventive treatment |
| NaFeEDTA | sodium iron ethylenediaminetetraacetate |
| PA | phytic acid |
| PF | plasma ferritin |
| RNI | reference nutrient intake |
| WHO | World Health Organization |
References
- World Health Organization (WHO). Worldwide Prevalence of Anaemia 1993–2005; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Righetti, A.A.; Koua, A.Y.G.; Adiossan, L.G.; Glinz, D.; Hurrell, R.F.; N’Goran, E.K.; Niamké, S.; Wegmüller, R.; Utzinger, J. Etiology of anemia among infants, school-aged children, and young non-pregnant women in different settings of south-central Côte d’Ivoire. Am. J. Trop. Med. Hyg. 2012, 87, 425–434. [Google Scholar] [CrossRef] [PubMed]
- Lozoff, B.; Georgieff, M.K. Iron deficiency and brain development. Semin. Pediatr. Neurol. 2006, 13, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Shafir, T.; Angulo-Barroso, R.; Jing, Y.; Angelilli, M.L.; Jacobson, S.W.; Lozoff, B. Iron deficiency and infant motor development. Early Hum. Dev. 2008, 84, 479–485. [Google Scholar] [CrossRef] [PubMed]
- Hurrell, R.; Egli, I. Iron bioavailability and dietary reference values. Am. J. Clin. Nutr. 2010, 91, 1461S–1467S. [Google Scholar] [CrossRef] [PubMed]
- Hurrell, R.F. Fortification: Overcoming technical and practical barriers. J. Nutr. 2002, 132 (Suppl. 4), 806S–812S. [Google Scholar] [PubMed]
- Food and Agriculture Organization (FAO)/World Health Organization (WHO). Guidelines on Food Fortification with Micronutrients; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- World Health Organization (WHO). Evaluation of Certain Food Additives and Contaminants; WHO Technical Report Series Fifty-Third Report of the Joint FAO/WHO Expert Committee on Food Additives; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Cercamondi, C.I.; Egli, I.M.; Ahouandjinou, E.; Dossa, R.; Zeder, C.; Salami, L.; Tjalsma, H.; Wiegerinck, E.; Tanno, T.; Hurrell, R.F.; et al. Afebrile Plasmodium falciparum parasitemia decreases absorption of fortification iron but does not affect systemic iron utilization: A double stable-isotope study in young Beninese women. Am. J. Clin. Nutr. 2010, 92, 1385–1392. [Google Scholar] [CrossRef] [PubMed]
- Glinz, D.; Hurrell, R.F.; Righetti, A.A.; Zeder, C.; Adiossan, L.G.; Tjalsma, H.; Utzinger, J.; Zimmermann, M.B.; N’Goran, E.K.; Wegmüller, R. In Ivorian school-age children, infection with hookworm does not reduce dietary iron absorption or systemic iron utilization, whereas afebrile Plasmodium falciparum infection reduces iron absorption by half. Am. J. Clin. Nutr. 2015, 101, 462–470. [Google Scholar] [CrossRef] [PubMed]
- Andang’o, P.E.; Osendarp, S.J.; Ayah, R.; West, C.E.; Mwaniki, D.L.; De Wolf, C.A.; Kraaijenhagen, R.; Kok, F.J.; Verhoef, H. Efficacy of iron-fortified whole maize flour on iron status of schoolchildren in Kenya: A randomised controlled trial. Lancet 2007, 369, 1799–1806. [Google Scholar] [CrossRef]
- Wegmüller, R.; Camara, F.; Zimmermann, M.B.; Adou, P.; Hurrell, R.F. Salt dual-fortified with iodine and micronized ground ferric pyrophosphate affects iron status but not hemoglobin in children in Côte d’Ivoire. J. Nutr. 2006, 136, 1814–1820. [Google Scholar] [PubMed]
- Zimmermann, M.B.; Wegmueller, R.; Zeder, C.; Chaouki, N.; Rohner, F.; Saissi, M.; Torresani, T.; Hurrell, R.F. Dual fortification of salt with iodine and micronized ferric pyrophosphate: A randomized, double-blind, controlled trial. Am. J. Clin. Nutr. 2004, 80, 952–959. [Google Scholar] [PubMed]
- Rohner, F.; Zimmermann, M.B.; Amon, R.J.; Vounatsou, P.; Tschannen, A.B.; N’Goran, E.K.; Nindjin, C.; Cacou, M.C.; Té-Bonlé, M.D.; Aka, H.; et al. In a randomized controlled trial of iron fortification, anthelmintic treatment, and intermittent preventive treatment of malaria for anemia control in Ivorian children, only anthelmintic treatment shows modest benefit. J. Nutr. 2010, 140, 635–641. [Google Scholar] [CrossRef] [PubMed]
- Glinz, D.; Hurrell, R.F.; Ouattara, M.; Zimmermann, M.B.; Brittenham, G.M.; Adiossan, L.G.; Righetti, A.A.; Seifert, B.; Diakité, V.G.; Utzinger, J.; et al. The effect of iron-fortified complementary food and intermittent preventive treatment of malaria on anaemia in 12- to 36-month-old children: A cluster-randomised controlled trial. Malar. J. 2015, 14, 347. [Google Scholar] [CrossRef] [PubMed]
- Fürst, T.; Silué, K.D.; Ouattara, M.; N’Goran, D.N.; Adiossan, L.G.; N’Guessan, Y.; Zouzou, F.; Koné, S.; N’Goran, E.K.; Utzinger, J. Schistosomiasis, soil-transmitted helminthiasis, and sociodemographic factors influence quality of life of adults in Côte d’Ivoire. PLoS Negl. Trop. Dis. 2012, 6, e1855. [Google Scholar] [CrossRef] [PubMed]
- Koné, S.; Baikoro, N.; N’Guessan, Y.; Jaeger, F.N.; Silué, K.D.; Fürst, T.; Hürlimann, E.; Ouattara, M.; Séka, M.C.; N’Guessan, N.A.; et al. Health & Demographic Surveillance System Profile: The Taabo Health and Demographic Surveillance System, Côte d’Ivoire. Int. J. Epidemiol. 2015, 44, 87–97. [Google Scholar] [CrossRef] [PubMed]
- Bassa, F.K.; Ouattara, M.; Silué, K.D.; Adiossan, L.G.; Baikoro, N.; Koné, S.; N’Cho, M.; Traoré, M.; Bonfoh, B.; Utzinger, J.; et al. Epidemiology of malaria in the Taabo health and demographic surveillance system, south-central Côte d’Ivoire. Malar. J. 2016, 15, 9. [Google Scholar] [CrossRef] [PubMed]
- Righetti, A.A.; Wegmüller, R.; Glinz, D.; Ouattara, M.; Adiossan, L.G.; N’Goran, E.K.; Utzinger, J.; Hurrell, R.F. Effects of inflammation and Plasmodium falciparum infection on soluble transferrin receptor and plasma ferritin concentration in different age groups: A prospective longitudinal study in Côte d’Ivoire. Am. J. Clin. Nutr. 2013, 97, 1364–1374. [Google Scholar] [CrossRef] [PubMed]
- Staubli Asobayire, F. Development of a Food Fortification Strategy to Combat Iron Deficiency in the Ivory Coast; ETH Zurich: Zürich, Switzerland, 2000; pp. 1–239. [Google Scholar]
- Wegmüller, R. Dual Fortification of Salt with Iodine and Iron in Africa; ETH Zurich: Zürich, Switzerland, 2005; pp. 1–211. [Google Scholar]
- World Health Organization (WHO). Iron Deficiency Anaemia: Assessment, Prevention and Control: A Guide for Programme Managers; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Word Health Organization (WHO). Assessing the Iron Status of Populations, 2nd ed.; Word Health Organization, Centers for Disease Control and Prevention: Geneva, Switzerland, 2007. [Google Scholar]
- Glinz, D.; Kamiyango, M.; Phiri, K.S.; Munthali, F.; Zeder, C.; Zimmermann, M.B.; Hurrell, R.F.; Wegmüller, R. The effect of timing of iron supplementation on iron absorption and haemoglobin in post-malaria anaemia: A longitudinal stable isotope study in Malawian toddlers. Malar. J. 2014, 13, 397. [Google Scholar] [CrossRef] [PubMed]
- Bezwoda, W.R.; Bothwell, T.H.; Torrance, J.D.; MacPhail, A.P.; Charlton, R.W.; Kay, G.; Levin, J. The relationship between marrow iron stores, plasma ferritin concentrations and iron absorption. Scand. J. Haematol. 1979, 22, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Collings, R.; Harvey, L.J.; Hooper, L.; Hurst, R.; Brown, T.J.; Ansett, J.; King, M.; Fairweather-Tait, S.J. The absorption of iron from whole diets: A systematic review. Am. J. Clin. Nutr. 2013, 98, 65–81. [Google Scholar] [CrossRef] [PubMed]
- Pasricha, S.R.; Atkinson, S.H.; Armitage, A.E.; Khandwala, S.; Veenemans, J.; Cox, S.E.; Eddowes, L.A.; Hayes, T.; Doherty, C.P.; Demir, A.Y.; et al. Expression of the iron hormone hepcidin distinguishes different types of anemia in African children. Sci. Transl. Med. 2014, 6, 235re3. [Google Scholar] [CrossRef] [PubMed]
- Ganz, T. Macrophages and systemic iron homeostasis. J. Innate Immun. 2012, 4, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Drakesmith, H.; Prentice, A.M. Hepcidin and the iron-infection axis. Science 2012, 338, 768–772. [Google Scholar] [CrossRef] [PubMed]
- Skorokhod, O.A.; Caione, L.; Marrocco, T.; Migliardi, G.; Barrera, V.; Arese, P.; Piacibello, W.; Schwarzer, E. Inhibition of erythropoiesis in malaria anemia: Role of hemozoin and hemozoin-generated 4-hydroxynonenal. Blood 2010, 116, 4328–4337. [Google Scholar] [CrossRef] [PubMed]
- Pasricha, S.R.; Hayes, E.; Kalumba, K.; Biggs, B.A. Effect of daily iron supplementation on health in children aged 4–23 months: A systematic review and meta-analysis of randomised controlled trials. Lancet Glob. Health 2013, 1, 77–86. [Google Scholar] [CrossRef]
- De-Regil, L.M.; Suchdev, P.S.; Vist, G.E.; Walleser, S.; Pena-Rosas, J.P. Home fortification of foods with multiple micronutrient powders for health and nutrition in children under two years of age. Evid. Based Child Health 2013, 8, 112–201. [Google Scholar] [CrossRef] [PubMed]
- Hurrell, R.F. Iron fortification: Its efficacy and safety in relation to infections. Food Nutr. Bull. 2007, 28 (Suppl. 4), S585–S594. [Google Scholar] [CrossRef] [PubMed]
- Brittenham, G.M.; Andersson, M.; Egli, I.; Foman, J.T.; Zeder, C.; Westerman, M.E.; Hurrell, R.F. Circulating non-transferrin-bound iron after oral administration of supplemental and fortification doses of iron to healthy women: A randomized study. Am. J. Clin. Nutr. 2014, 100, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Jaeggi, T.; Kortman, G.A.; Moretti, D.; Chassard, C.; Holding, P.; Dostal, A.; Boekhorst, J.; Timmerman, H.M.; Swinkels, D.W.; Tjalsma, H.; et al. Iron fortification adversely affects the gut microbiome, increases pathogen abundance and induces intestinal inflammation in Kenyan infants. Gut 2014, 64, 731–742. [Google Scholar] [CrossRef] [PubMed]
- Suchdev, P.S.; Namaste, S.M.; Aaron, G.J.; Raiten, D.J.; Brown, K.H.; Flores-Ayala, R. Overview of the biomarkers reflecting inflammation and nutritional determinants of anemia (BRINDA) project. Adv. Nutr. 2016, 7, 349–356. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Groups | |||
|---|---|---|---|
| Control | CF-FeFum | CF-FePP | |
| Participants N = | |||
| Baseline | 125 | 126 | 127 |
| 6 months | 104 | 111 | 116 |
| 9 months | 76 | 81 | 87 |
| Height (cm, mean, SD) | |||
| Baseline | 79.2 ± 9.8 | 78.5 ± 7.5 | 78.6 ± 6.8 |
| 6 months | 86.2 ± 6.9 | 86.8 ± 6.9 | 85.8 ± 6.6 |
| 9 months | 89.0 ± 6.6 | 89.3 ± 6.5 | 89.0 ± 6.3 |
| Body weight (kg, mean, SD) | |||
| Baseline | 10.7 ± 2.3 | 10.8 ± 2.9 | 10.7 ± 2.5 |
| 6 months | 11.2 ± 2.0 | 11.1 ± 2.0 | 11.0 ± 1.8 |
| 9 months | 11.7 ± 2.1 | 11.5 ± 1.9 | 11.4 ± 1.7 |
| P. falciparum prevalence | |||
| Baseline | 62.1% | 57.7% | 66.1% |
| 6 months | 62.5% | 55.0% | 64.7% |
| 9 months | 44.7% | 46.9% | 47.1% |
| P. falciparum parasitemia (parasites/μL blood, geometric mean, 95% confidence interval) | |||
| Baseline | 1136 (729–1768) | 896 (524–1534) | 2182 (1409–3379) |
| 6 months | 3773 (2470–5762) | 2268 (1427–3605) | 2074 (1367–3146) |
| 9 months | 2820 (1460–5447) | 2718 (1662–4445) | 3130 (1913–5121) |
| CRP (mg/L, median, interquartile range 25th 75th) | |||
| Baseline | 2.8 (1.0–11.1) | 3.4 (1.4–8.7) | 5.9 (1.9–21.3) *ᴪ |
| 6 months | 5.1 (1.8–18.6) | 4.6 (1.2–20.4) | 4.8 (1.5–14.6) ** |
| 9 months | 2.6 (1.0–7.3) | 4.3 (1.0–13.2) | 3.2 (1.3–14.8) ᴪ |
| AGP (g/L, median, 25th 75th) | |||
| Baseline | 1.12 (0.90–1.40) | 1.27 (1.01–1.54) | 1.26 (0.96–1.65) |
| 6 months | 1.13 (0.88–1.41) | 1.25 (0.92–1.54) | 1.10 (0.85–1.40) |
| 9 months | 1.07 (0.78–1.44) | 1.13 (0.85–1.36) | 1.06 (0.79–1.28) * |
| Prevalence of inflammation (CRP > 5 mg/L and/or AGP > 1 g/L) | |||
| Baseline | 65.8% | 76.8% | 76.4% |
| 6 months | 72.1% | 74.8% | 65.5% |
| 9 months | 57.3% | 64.2% | 57.5% |
| Groups | Overall Effects | Between Group Comparisons | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Control | CF-FeFum | CF-FePP | Time p = | Treatment p = | Time by Treatment Interaction p = | Control vs. CF-FeFum p = | Control vs. CF-FePP p = | CF-FeFum vs. CF-FePP p = | |
| Participants N = | |||||||||
| Baseline | 125 | 126 | 127 | ||||||
| 6 months | 104 | 111 | 116 | ||||||
| 9 months | 76 | 81 | 87 | ||||||
| Hb concentration (g/dL, mean, ±SD) | |||||||||
| Baseline | 9.8 ± 1.3 | 9.9 ± 1.2 | 9.6 ± 1.2 | <0.001 | 0.948 | 0.141 | |||
| 6 months | 9.9 ± 1.3 | 9.9 ± 1.3 | 10.0 ± 1.1 | 0.761 | 0.479 | 0.306 | |||
| 9 months | 10.3 ± 1.3 * | 10.4 ± 1.2 * | 10.5 ± 1.2 ** | 0.871 | 0.226 | 0.161 | |||
| Anemia (Hb < 11 g/dL) | |||||||||
| Baseline | 81.6% | 80.2% | 86.6% | <0.001 | 0.475 | 0.237 | |||
| 6 months | 79.8% | 77.5% | 81.9% | 0.216 | 0.953 | 0.746 | |||
| 9 months | 71.1% | 70.4% | 65.5%* | 0.083 | 0.036 a | 0.069 a | |||
| PF (μg/L, median, interquartile range 25th 75th) | |||||||||
| Baseline | 37.7 (18.3–72.4) | 36.2 (21.6–66.0) | 53.0 (28.4–115.7) | <0.001 | 0.068 | 0.458 | |||
| 6 months | 60.7 (35.1–114.0) *** | 102.4 (48.3–159.5) *** | 69.1 (41.8–139.7) *** | <0.003 a | 0.048 a | 0.214 | |||
| 9 months | 49.6 (26.2–96.0) ** | 66.5 (45.4–117.4) *** | 62.6 (41.1–107.2) *** | 0.072 a | 0.150 | 0.426 | |||
| ID (PF < 30 µg/L) | |||||||||
| Baseline | 37.4% | 40.0% | 26.7% | <0.001 | 0.004 | 0.068 | |||
| 6 months | 19.2% * | 5.4% *** | 8.6% *** | <0.003 a | 0.006 a | 0.368 | |||
| 9 months | 29.3% | 3.7% *** | 10.3% *** | <0.003 a | 0.003 a | 0.171 | |||
| IDA (PF < 30 μg/L and Hb < 11 g/dL) | |||||||||
| Baseline | 33.3% | 32.8% | 23.6% | <0.001 | 0.003 | 0.028 | |||
| 6 months | 15.4% ** | 3.6% *** | 4.3% *** | 0.036 a | 0.096 a | 0.689 | |||
| 9 months | 18.7% | 1.2% *** | 3.4% *** | 0.027 a | 0.018 a | 0.388 | |||
| ID and inflammation (PF < 30 μg/L and inflammation: CRP > 5 mg/L and/or AGP > 1 g/L) | |||||||||
| Baseline | 21.1% | 24.0% | 14.2% | <0.001 | 0.001 | 0.080 | |||
| 6 months | 11.5% * | 4.5% *** | 4.3% *** | 0.099 a | 0.096 a | 0.900 | |||
| 9 months | 14.7% | 2.5% ** | 2.3% ** | 0.033 a | 0.021 a | 0.919 | |||
| Anemia, ID, and inflammation (Hb < 11 g/dL and PF < 30 µg/L and inflammation: CRP > 5 mg/L and/or AGP > 1 g/L) | |||||||||
| Baseline | 18.7% | 20.8% | 13.4% | <0.001 | 0.003 | 0.040 | |||
| 6 months | 10.6% | 2.7% ** | 3.4% *** | 0.048 a | 0.090 a | 0.513 | |||
| 9 months | 12.0% | 1.2% ** | 1.1% ** | 0.063 a | 0.048 a | 0.944 | |||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Glinz, D.; Wegmüller, R.; Ouattara, M.; Diakité, V.G.; Aaron, G.J.; Hofer, L.; Zimmermann, M.B.; Adiossan, L.G.; Utzinger, J.; N’Goran, E.K.; et al. Iron Fortified Complementary Foods Containing a Mixture of Sodium Iron EDTA with Either Ferrous Fumarate or Ferric Pyrophosphate Reduce Iron Deficiency Anemia in 12- to 36-Month-Old Children in a Malaria Endemic Setting: A Secondary Analysis of a Cluster-Randomized Controlled Trial. Nutrients 2017, 9, 759. https://doi.org/10.3390/nu9070759
Glinz D, Wegmüller R, Ouattara M, Diakité VG, Aaron GJ, Hofer L, Zimmermann MB, Adiossan LG, Utzinger J, N’Goran EK, et al. Iron Fortified Complementary Foods Containing a Mixture of Sodium Iron EDTA with Either Ferrous Fumarate or Ferric Pyrophosphate Reduce Iron Deficiency Anemia in 12- to 36-Month-Old Children in a Malaria Endemic Setting: A Secondary Analysis of a Cluster-Randomized Controlled Trial. Nutrients. 2017; 9(7):759. https://doi.org/10.3390/nu9070759
Chicago/Turabian StyleGlinz, Dominik, Rita Wegmüller, Mamadou Ouattara, Victorine G. Diakité, Grant J. Aaron, Lorenz Hofer, Michael B. Zimmermann, Lukas G. Adiossan, Jürg Utzinger, Eliézer K. N’Goran, and et al. 2017. "Iron Fortified Complementary Foods Containing a Mixture of Sodium Iron EDTA with Either Ferrous Fumarate or Ferric Pyrophosphate Reduce Iron Deficiency Anemia in 12- to 36-Month-Old Children in a Malaria Endemic Setting: A Secondary Analysis of a Cluster-Randomized Controlled Trial" Nutrients 9, no. 7: 759. https://doi.org/10.3390/nu9070759
APA StyleGlinz, D., Wegmüller, R., Ouattara, M., Diakité, V. G., Aaron, G. J., Hofer, L., Zimmermann, M. B., Adiossan, L. G., Utzinger, J., N’Goran, E. K., & Hurrell, R. F. (2017). Iron Fortified Complementary Foods Containing a Mixture of Sodium Iron EDTA with Either Ferrous Fumarate or Ferric Pyrophosphate Reduce Iron Deficiency Anemia in 12- to 36-Month-Old Children in a Malaria Endemic Setting: A Secondary Analysis of a Cluster-Randomized Controlled Trial. Nutrients, 9(7), 759. https://doi.org/10.3390/nu9070759