Botulinum Toxin Injection in Children with Hemiplegic Cerebral Palsy: Correction of Growth through Comparison of Treated and Unaffected Limbs


Abstract
:1. Introduction
2. Results
2.1. Study Participants
2.2. Changes in Medial Head of the Gastrocnemius Muscle Thickness After Injection
2.3. Changes in Fascicle Length After Injection
2.4. Changes in Fascicle Angle After Injection
3. Discussion
3.1. Changes in Medial Head of the Gastrocnemius Muscle Thickness After Injection
3.2. Changes in Fascicle Length After Injection
3.3. Changes in Fascicle Angle After Injection
3.4. Study Limitations
4. Conclusions
5. Materials and Methods
5.1. Participants
5.2. Procedure
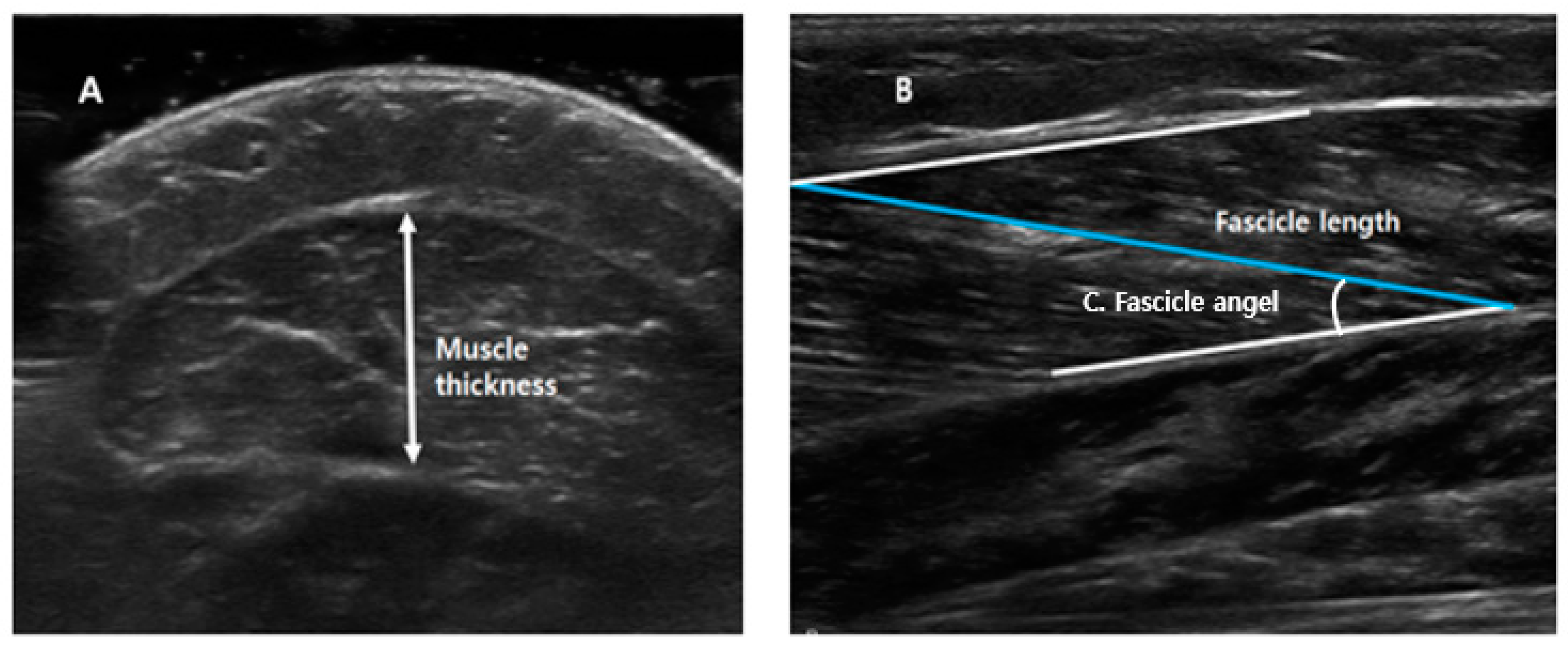
5.3. Assessment
5.4. Statistical Analysis
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Verschuren, O.; Smorenburg, A.R.P.; Luiking, Y.; Bell, K.; Barber, L.; Peterson, M.D. Determinants of muscle preservation in individuals with cerebral palsy across the lifespan: A narrative review of the literature. J. Cachexia Sarcopenia Muscle 2018, 9, 453–464. [Google Scholar] [CrossRef]
- Kruse, A.; Schranz, C.; Tilp, M.; Svehlik, M. Muscle and tendon morphology alterations in children and adolescents with mild forms of spastic cerebral palsy. BMC Pediatr. 2018, 18, 156. [Google Scholar] [CrossRef]
- Barrett, R.S.; Lichtwark, G.A. Gross muscle morphology and structure in spastic cerebral palsy: A systematic review. Dev. Med. Child Neurol. 2010, 52, 794–804. [Google Scholar] [CrossRef] [PubMed]
- Barber, L.; Barrett, R.; Lichtwark, G. Medial gastrocnemius muscle fascicle active torque-length and Achilles tendon properties in young adults with spastic cerebral palsy. J. Biomech. 2012, 45, 2526–2530. [Google Scholar] [CrossRef] [PubMed]
- Barber, L.; Hastings-Ison, T.; Baker, R.; Barrett, R.; Lichtwark, G. Medial gastrocnemius muscle volume and fascicle length in children aged 2 to 5 years with cerebral palsy. Dev. Med. Child Neurol. 2011, 53, 543–548. [Google Scholar] [CrossRef] [PubMed]
- Moreau, N.G.; Teefey, S.A.; Damiano, D.L. In vivo muscle architecture and size of the rectus femoris and vastus lateralis in children and adolescents with cerebral palsy. Dev. Med. Child Neurol. 2009, 51, 800–806. [Google Scholar] [CrossRef]
- Chen, Y.; He, L.; Xu, K.; Li, J.; Guan, B.; Tang, H. Comparison of calf muscle architecture between Asian children with spastic cerebral palsy and typically developing peers. PLoS ONE 2018, 13, e0190642. [Google Scholar] [CrossRef]
- Valentine, J.; Stannage, K.; Fabian, V.; Ellis, K.; Reid, S.; Pitcher, C.; Elliott, C. Muscle histopathology in children with spastic cerebral palsy receiving botulinum toxin type A. Muscle Nerve 2016, 53, 407–414. [Google Scholar] [CrossRef]
- Williams, S.A.; Elliott, C.; Valentine, J.; Gubbay, A.; Shipman, P.; Reid, S. Combining strength training and botulinum neurotoxin intervention in children with cerebral palsy: The impact on muscle morphology and strength. Disabil. Rehabil. 2013, 35, 596–605. [Google Scholar] [CrossRef]
- Read, F.A.; Boyd, R.N.; Barber, L.A. Longitudinal assessment of gait quality in children with bilateral cerebral palsy following repeated lower limb intramuscular Botulinum toxin-A injections. Res. Dev. Disabil. 2017, 68, 35–41. [Google Scholar] [CrossRef]
- Alexander, C.; Elliott, C.; Valentine, J.; Stannage, K.; Bear, N.; Donnelly, C.J.; Shipman, P.; Reid, S. Muscle volume alterations after first botulinum neurotoxin A treatment in children with cerebral palsy: A 6-month prospective cohort study. Dev. Med. Child Neurol. 2018, 60, 1165–1171. [Google Scholar] [CrossRef] [PubMed]
- Williams, S.A.; Reid, S.; Elliott, C.; Shipman, P.; Valentine, J. Muscle volume alterations in spastic muscles immediately following botulinum toxin type-A treatment in children with cerebral palsy. Dev. Med. Child Neurol. 2013, 55, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Lukban, M.B.; Rosales, R.L.; Dressler, D. Effectiveness of botulinum toxin A for upper and lower limb spasticity in children with cerebral palsy: A summary of evidence. J. Neural Transm. 2009, 116, 319–331. [Google Scholar] [CrossRef]
- Park, E.S.; Sim, E.; Rha, D.W.; Jung, S. Architectural changes of the gastrocnemius muscle after botulinum toxin type A injection in children with cerebral palsy. Yonsei Med. J. 2014, 55, 1406–1412. [Google Scholar] [CrossRef]
- Ryll, U.; Bastiaenen, C.; De Bie, R.; Staal, B. Effects of leg muscle botulinum toxin A injections on walking in children with spasticity-related cerebral palsy: A systematic review. Dev. Med. Child Neurol. 2011, 53, 210–216. [Google Scholar] [CrossRef]
- Pingel, J.; Nielsen, M.S.; Lauridsen, T.; Rix, K.; Bech, M.; Alkjaer, T.; Andersen, I.T.; Nielsen, J.B.; Feidenhansl, R. Injection of high dose botulinum-toxin A leads to impaired skeletal muscle function and damage of the fibrilar and non-fibrilar structures. Sci. Rep. 2017, 7, 1–14. [Google Scholar] [CrossRef]
- Multani, I.; Manji, J.; Hastings-Ison, T.; Khot, A.; Graham, K. Botulinum Toxin in the Management of Children with Cerebral Palsy. Pediatr. Drugs 2019, 21, 261–281. [Google Scholar] [CrossRef]
- Salari, M.; Sharma, S.; Jog, M.S. Botulinum toxin induced atrophy: An uncharted territory. Toxins (Basel) 2018, 10, 313. [Google Scholar] [CrossRef]
- Kawano, A.; Yanagizono, T.; Kadouchi, I.; Umezaki, T.; Chosa, E. Ultrasonographic evaluation of changes in the muscle architecture of the gastrocnemius with botulinum toxin treatment for lower extremity spasticity in children with cerebral palsy. J. Orthop Sci. 2018, 23, 389–393. [Google Scholar] [CrossRef]
- Noble, J.J.; Fry, N.R.; Lewis, A.P.; Keevil, S.F.; Gough, M.; Shortland, A.P. Lower limb muscle volumes in bilateral spastic cerebral palsy. Brain Dev. 2014, 36, 294–300. [Google Scholar] [CrossRef]
- Mohagheghi, A.A.; Khan, T.; Meadows, T.H.; Giannikas, K.; Baltzopoulos, V.; Maganaris, C.N. Differences in gastrocnemius muscle architecture between the paretic and non-paretic legs in children with hemiplegic cerebral palsy. Clin. Biomech. 2007, 22, 718–724. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Total (N = 14) |
|---|---|
| Sex (n) | |
| Male | 10 (71.43%) |
| Female | 4 (28.57%) |
| Age (mean), years | 4.57 (SD = 2.28) |
| Body weight (mean), kg | 21.17 (SD = 8.24) |
| History of previous BoNT-A injection (n) | 9 (64.29%) |
| GMFCS level, (n) | |
| I | 12 (85.71%) |
| II | 2 (14.29%) |
| Type (n) | |
| Right hemiplegia | 9 (64.29%) |
| Left hemiplegia | 5 (35.71%) |
| Location of injection * | n |
|---|---|
| Medial head of gastrocnemius muscle † | 14 (100%) |
| Lateral head of gastrocnemius muscle | 8 (57.14%) |
| Triceps posterior muscle | 6 (42.86%) |
| Peroneus longus muscle | 2 (14.29%) |
| Soleus muscle | 1 (7.14%) |
| Upper extremity muscles | 3 (21.43%) |
| Toxin Injected Affected Side, Mean (SD) | Unaffected Side, Mean (SD) | |||||
|---|---|---|---|---|---|---|
| −10° | 0° | 10° | −10° | 0° | 10° | |
| Baseline MT (cm) | 1.33 (0.22) | 1.34 (0.21) | 1.35 (0.21) | 1.51 (0.24) | 1.49 (0.24) | 1.50 (0.26) |
| After 4 weeks MT (cm) | 1.24 (0.18) | 1.26 (0.20) | 1.25 (0.21) | 1.54 (0.22) | 1.52 (0.22) | 1.54 (0.22) |
| After 12 weeks MT (cm) | 1.25 (0.27) | 1.26 (0.27) | 1.27 (0.29) | 1.69 (0.27) †,†† | 1.67 (0.24) †,†† | 1.68 (0.22) †,†† |
| Baseline FL (cm) | 4.36 (0.79) | 4.68 (0.87) | 4.98 (0.96) | 4.97 (0.89) | 5.21 (0.88) | 5.66 (1.06) |
| After 4 weeks FL (cm) | 4.60 (0.92) | 4.95 (0.99) * | 5.29 (1.09) | 5.22 (1.13) * | 5.57 (1.14) * | 6.03 (1.19) * |
| After 12 weeks FL (cm) | 4.79 (0.95) † | 5.17 (1.07) † | 5.50 (1.04) † | 5.66 (1.17) †,†† | 5.93 (1.06) †,†† | 6.32 (1.15) †,†† |
| Baseline FA (°) | 14.03 (1.59) | 13.24 (1.61) | 12.40 (1.47) | 15.39 (2.60) | 14.52 (2.12) | 13.58 (1.81) |
| After 4 weeks FA (°) | 13.62 (1.90) | 12.50 (1.70) | 11.79 (1.99) | 13.88 (2.54) * | 12.87 (2.12) * | 12.00 (1.64) * |
| After 12 weeks FA (°) | 12.85 (1.53) | 11.61 (1.07) † | 11.46 (1.02) | 12.99 (2.18) † | 12.34 (2.07) † | 11.40 (1.18) † |
| Muscle architecture | −10° | 0° | 10° |
|---|---|---|---|
| Muscle thickness (%) Baseline, mean (SD) | 88.38 (7.80) | 89.84 (6.37) | 90.53 (6.92) |
| After 4 weeks, mean (SD) | 80.51 (7.87) * | 82.69 (7.63) | 81.41 (8.58) * |
| After 12 weeks, mean (SD) | 74.76 (15.03) † | 76.09 (15.04) † | 75.62 (15.50) † |
| Fascicle length (%) Baseline, mean (SD) | 88.88 (8.04) | 89.85 (7.85) | 87.96 (6.11) |
| After 4 weeks, mean (SD) | 88.81 (11.78) | 89.36 (9.77) | 87.91 (9.77) |
| After 12 weeks, mean (SD) | 84.88 (7.87) | 86.93 (7.36) | 87.05 (7.40) |
| Fascicle angle (%) Baseline, mean (SD) | 93.90 (21.45) | 92.56 (15.83) | 92.03 (11.20) |
| After 4 weeks, mean (SD) | 99.89 (16.83) | 98.51 (14.85) | 99.37 (17.98) |
| After 12 weeks, mean (SD) | 100.40 (13.22) | 95.87 (13.47) | 103.36 (18.30) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yi, Y.G.; Jang, D.-H.; Lee, D.; Oh, J.-Y.; Han, M.-H. Botulinum Toxin Injection in Children with Hemiplegic Cerebral Palsy: Correction of Growth through Comparison of Treated and Unaffected Limbs. Toxins 2019, 11, 688. https://doi.org/10.3390/toxins11120688
Yi YG, Jang D-H, Lee D, Oh J-Y, Han M-H. Botulinum Toxin Injection in Children with Hemiplegic Cerebral Palsy: Correction of Growth through Comparison of Treated and Unaffected Limbs. Toxins. 2019; 11(12):688. https://doi.org/10.3390/toxins11120688
Chicago/Turabian StyleYi, You Gyoung, Dae-Hyun Jang, Dongwoo Lee, Ja-Young Oh, and Mi-Hyang Han. 2019. "Botulinum Toxin Injection in Children with Hemiplegic Cerebral Palsy: Correction of Growth through Comparison of Treated and Unaffected Limbs" Toxins 11, no. 12: 688. https://doi.org/10.3390/toxins11120688
APA StyleYi, Y. G., Jang, D.-H., Lee, D., Oh, J.-Y., & Han, M.-H. (2019). Botulinum Toxin Injection in Children with Hemiplegic Cerebral Palsy: Correction of Growth through Comparison of Treated and Unaffected Limbs. Toxins, 11(12), 688. https://doi.org/10.3390/toxins11120688