OnabotulinumtoxinA: Still the Present for Chronic Migraine

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Current Understanding of Migraine Pathophysiology with Relevance for BT-A Treatment
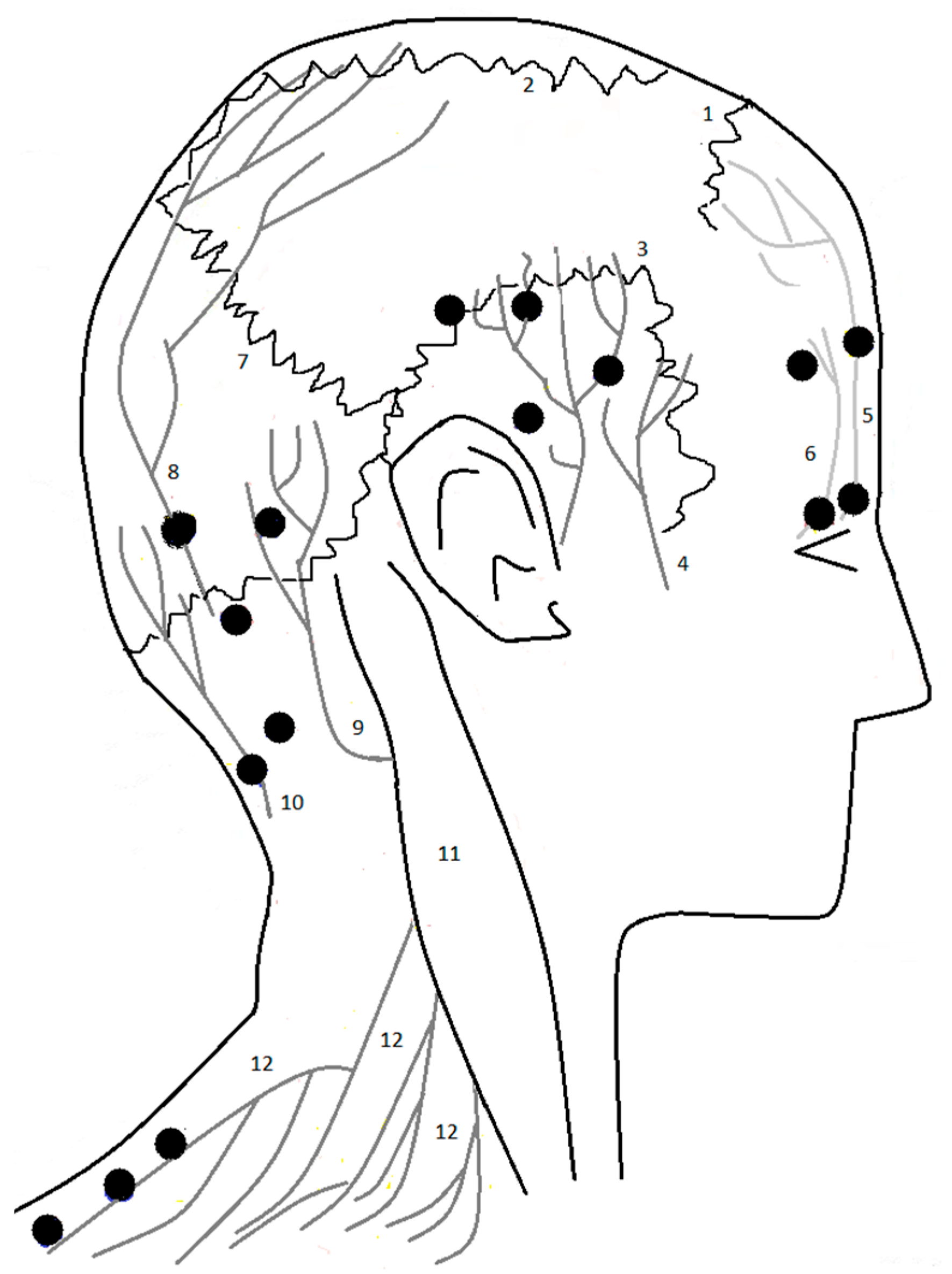
3.1. Anatomy
- The injection protocol used for CM;
- The ability of BT-A to inhibit cranial nociceptor activation toward both intracranial and extracranial stimuli.
3.2. Spotlights of Mechanisms in CM Justifying BT-A Use
3.2.1. Stimuli Potentially Activating Cranial Nociceptive Fibers
3.2.2. Consequences of the Generation of an Action Potential in the Cranial Nociceptors
3.2.3. Central Transmission of the Pain Signals
4. Putative Mechanisms of BT-A in Migraine
5. Clinical Use of BT-A in the Treatment of Chronic Migraine
5.1. Clinical Trials
5.1.1. PREEMPT-1 and PREEMPT-2 Protocols
5.1.2. Pooled Results of the PREEMPT-1 and PREEMPT-2 Protocols
5.1.3. Pooled Results of the Open-Label Phase of the PREEMPT-1 and PREEMPT-2 Protocols
5.1.4. Speed of Action of the BT-A from the PREEMPT-1 and PREEMPT-2 Protocols Pooled Analysis
5.1.5. BT-A vs. Topiramate
5.2. Real-Life Studies
5.3. Tolerability and Interactions
5.4. Current Role of BT-A in the Treatment of Chronic Migraine
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd Edition. Cephalalgia 2018, 38, 1–211. [Google Scholar] [CrossRef] [PubMed]
- Burch, R.C.; Buse, D.C.; Lipton, R.B. Migraine: Epidemiology, burden and comorbidity. Neurol. Clin. 2019, 37, 631–649. [Google Scholar] [CrossRef] [PubMed]
- Diener, H.C.; Holle, D.; Solbach, K.; Gaul, C. Medication-overuse headache: Risk factors, pathophysiology and management. Nat. Rev. Neurol. 2016, 12, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Hepp, Z.; Dodick, D.W.; Varon, S.F.; Chia, J.; Matthew, N.; Gillard, P.; Hansen, R.N.; Devine, E.B. Persistence and switching patterns of oral migraine prophylactic medications among patients with chronic migraine: A retrospective claims analysis. Cephalalgia 2017, 37, 470–485. [Google Scholar] [CrossRef] [Green Version]
- Carlsen, L.N.; Munksgaard, S.B.; Jensen, R.H.; Bendsten, L. Complete detoxification is the most effective treatment of medication-overuse headache: A randomized controlled open-label trial. Cephalalgia 2018, 38, 225–236. [Google Scholar] [CrossRef]
- Agostoni, E.C.; Barbanti, P.; Calabresi, P.; Colombo, B.; Cortelli, P.; Frediani, F.; Geppetti, P.; Grazzi, L.; Leone, M.; Martel-Letti, P.; et al. Italian chronic migraine group. Current and emerging evidence-based treatment options in chronic migraine: A narrative review. J. Headache Pain 2019, 20, 92. [Google Scholar] [CrossRef] [Green Version]
- Bramer, W.M.; Rethlefsen, M.L.; Kleijnen, J.; Franco, O.H. Optimal database combination for literature searches in systematic review: A prospective exploratory study. Syst. Rev. 2017, 6, 245. [Google Scholar] [CrossRef]
- Blumefeld, A.; Silberstein, S.D.; Dodick, D.W.; Aurora, S.K.; Turkel, C.C.; Binder, W.J. Method of injection of OnabotulinumtoxinA for chronic migraine: A safe, well-tolerated, and effective treatment paradigm based on the PREEMPT clinical program. Headache 2010, 50, 1406–1418. [Google Scholar] [CrossRef]
- Hobart, J.C.; Cano, S.J.; Warner, T.T.; Thompson, A.J. What sample sizes for reliability and validity studies in neurology? J. Neurol. 2012, 259, 2681–2694. [Google Scholar] [CrossRef]
- Edvinsson, J.C.A.; Viganò, A.; Alekseeva, A.; Alieva, E.; Arruda, R.; De Luca, C.; D’Ettore, N.; Frattale, I.; Kurnukhina, M.; Macerola, N.; et al. European Headache Federation School of Advanced Studies (EHF-SAS). The fifth cranial nerve in headaches. J. Headache Pain 2020, 21, 65. [Google Scholar] [CrossRef]
- Noseda, R.; Melo-Carrillo, A.; Nir, R.R.; Strassman, M.; Burstein, R. Non-trigeminal nociceptive innervation of the posterior dura: Implication to occipital headache. J. Neurosci. 2019, 39, 1867–1880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levy, D.; Labastida-Ramirez, A.; MaassenVanDenBrink, A. Current understanding of meningeal and cerebral vascular function underlying migraine headache. Cephalalgia 2019, 39, 1606–1622. [Google Scholar] [CrossRef] [PubMed]
- Schueler, M.; Messlinger, K.; Dux, M.; Neuhuber, W.L.; De Col, R. Extracranial projections of meningeal afferents and their impact on meningeal nociception and headache. Pain 2013, 154, 1622–1631. [Google Scholar] [CrossRef] [PubMed]
- Burstein, R.; Blake, P.; Schain, A.; Perry, C. Extracranial origin of headache. Curr. Opin. Neurol. 2017, 30, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Busch, V.; Jakob, W.; Juergens, T.; Schulte-Mattler, W.; Kaube, H.; May, A. Functional connectivity between trigeminal and occipital nerve blockade and nociceptive blink reflexes. Cephalalgia 2006, 26, 50–55. [Google Scholar] [CrossRef]
- Terrier, L.M.; Hadjikhani, N.; Destrieux, C. The trigeminal pathways. J. Neurol. 2022, 269, 3443–3460. [Google Scholar] [CrossRef]
- Matak, I.; Bolcskej, K.; Bach-Rojecky, L.; Helyes, Z. Mechanisms of botulinum toxin type A action on pain. Toxins 2019, 11, 459. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Levy, D.; Noseda, R.; Kainz, V.; Jakubowski, M.; Burstein, R. Activation of meningeal nociceptors by cortical spreading depression: Implication for migraine with aura. J. Neurosci. 2010, 30, 8807–8814. [Google Scholar] [CrossRef]
- Zhao, J.; Levy, D. Modulation of intracranial meningeal nocicpetor activity by cortical spreading depression: A reassessment. J. Neurophysiol. 2015, 113, 2778–2785. [Google Scholar] [CrossRef] [Green Version]
- Close, L.N.; Eftekhari, S.; Wang, M.; Charles, A.C.; Russo, A.F. Cortical spreading depression as a site of origin for migraine: Role of CGRP. Cephalalgia 2019, 39, 428–434. [Google Scholar] [CrossRef]
- Viana, F. Chemosensory properties of the trigeminal system. ACS Chem. Neurosci. 2011, 2, 38–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gafurov, O.; Koroleva, K.; Gianitullin, R. Antidromic spike propagation and dissimilar expression of P2X, 5-HT, and TRPV1 channels in peripheral vs. central sensory axons in meninges. Front. Cell Neurosci. 2021, 14, 6231134. [Google Scholar] [CrossRef]
- Ferrandiz-Huertas, C.; Mathivanan, S.; Wolf, C.J.; Devesa, I.; Ferrer-Montiel, A. Trafficking of thermoTRP channels. Membranes 2014, 4, 525–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramachandran, R. Neurogenic inflammation and its role in migraine. Semin Immunopathol. 2018, 40, 301–314. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, T.; Shibata, M.; Toriumi, H.; Iwashita, T.; Funakubo, M.; Sato, H.; Kuroi, T.; Ebine, T.; Koizumi, K.; Suzuki, N. Reduction of TRPV1 expression in the trigeminal system by botulinum neurotoxin type-A. Neurobiol. Dis. 2012, 48, 367–378. [Google Scholar] [CrossRef]
- Dux, M.; Vogler, B.; Kuhn, A.; Mackenzie, K.D.; Stratton, J.; Messlinger, K. The anti-CGRP antibody fremanezumab lowers CGRP release from rat dura mater and meningeal blood flow. Cells 2022, 11, 1768. [Google Scholar] [CrossRef]
- Schain, A.J.; Melo-Carrillo, A.; Stratton, J.; Strassman, A.M.; Burstein, R. CSD-induced arterial dilatation and plasma protein extravasation are unaffected by fremanezumab: Implications for CGRP’s role in migraine with aura. J. Neurosci. 2019, 39, 6001–6011. [Google Scholar] [CrossRef] [Green Version]
- Balcziak, L.K.; Russo, A.F. Dural immune cells, CGRP, and migraine. Front. Neurol. 2022, 13, 874193. [Google Scholar] [CrossRef]
- Levy, D.; Burstein, R.; Kainz, V.; Jakubovsky, M.; Strassman, A.M. Mast cells degranulation activates a pain pathway underlying migraine headache. Pain 2007, 130, 166–176. [Google Scholar] [CrossRef] [Green Version]
- Meng, J.; Ovsepian, S.V.; Wang, J.; Pickeringg, M.; Sasse, A.; Aoki, K.R.; Lawrence, G.W.; Dolly, J.O. Activation of TRPV1 mediates calcitonin gene-related peptide release, which excites trigeminal sensory neurons and is attenuated by a retargeted botulinum toxin with anti-nociceptive potential. J. Neurosci. 2009, 29, 4981–4992. [Google Scholar] [CrossRef] [Green Version]
- Edvinsson, J.C.A.; Warfringe, K.; Krause, D.N.; Blixt, F.W.; Sheykhzade, M.; Edvinsson, L.; Haanes, K.A. C-fibers may modulate adjacent Aδ-fibers through axon-axon CGRP signaling at nodes of Ranvier in the trigeminal system. J. Headache Pain 2019, 20, 105. [Google Scholar] [CrossRef] [Green Version]
- Messlinger, K.; Balcziak, L.K.; Russo, A.F. Cross-talking signaling in the trigeminal ganglion: Role of neuropeptides and other mediators. J. Neural Transm. 2020, 127, 431–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burstein, R.; Yamamura, H.; Malick, A.; Strassman, A.M. Chemical stimulation of the intracranial dural induces enhanced responses to facial stimulation in brain stem trigeminal neurons. J. Neurophysiol. 1998, 79, 964–982. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strassman, A.M.; Mineta, Y.; Vos, B.P. Distribution of fos-like immunoreactivity in the medullary and upper cervical dorsal horn produced by stimulation of dural blood vessels in the rat. J. Neurosci. 1994, 14, 3725–3735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burstein, R.; Cutrer, M.Y.; Yarnitsky, D. The development of cutaneous allodynia during a migraine attack: Clinical evidence for the sequential recruitment of spinal and supraspinal nociceptive neurons in migraine. Brain 2000, 123, 1703–1709. [Google Scholar] [CrossRef] [Green Version]
- Noseda, R.; Burstein, R. Migraine pathophysiology: Anatomy of the trigeminovascular pathway and associated neurological symptoms, CSD, sensitization and modulation of pain. Pain 2013, 154, 1. [Google Scholar] [CrossRef] [Green Version]
- Jakubowski, M.; McAllister, P.J.; Bajwa, Z.H.; Ward, T.N.; Smith, P.; Burstein, R. Exploding vs. imploding headache in migraine prophylaxis with Botulinum Toxin A. Pain 2006, 125, 286–295. [Google Scholar] [CrossRef]
- Kosaras, B.; Jakubowski, M.; Kainz, V.; Burstein, R. Sensory innervation of the calvarial bones of the mouse. J. Compar. Neurol. 2009, 515, 331–348. [Google Scholar] [CrossRef] [Green Version]
- Schueler, M.; Neuhuber, W.L.; De Col, R.; Messlinger, K. Innervation of rat and human dura mater and pericranial tissues in the parieto-temporal region by meningeal afferents. Headache 2014, 54, 996–1009. [Google Scholar] [CrossRef]
- Messlinger, K.; Russo, A.F. Current understanding of trigeminal ganglion structure and function in headache. Cephalalgia 2019, 39, 1661–1674. [Google Scholar] [CrossRef]
- Stovner, L.J.; Hagen, K.; Tronvik, E.; Gravdahl, G.B.; Burstein, R.; Dodick, D.W. FollowTheSutures: Piloting a new way to administer onabotulinumtoxinA for chronic migraine. Cephalalgia 2022, 42, 590–597. [Google Scholar] [CrossRef] [PubMed]
- Burstein, R.; Blumenfeld, A.M.; Silberstein, S.D.; Manack, A.A.; Brin, M.F. Mechanism of action of OnabtoulinumtoxinA in chronic migraine: A narrative review. Headache 2020, 60, 1259–1272. [Google Scholar] [CrossRef] [PubMed]
- Louveau, A.; Harz, J.; Nordheim Alme, M.; Salvador, A.F.; Dong, M.Q.; Viar, K.E.; Herod, G.; Knopp, J.; Setliff, J.; Lupi, A.L.; et al. CNS lymphatic drainage and neuroinflammation are regulated by meningeal lymphatic vasculature. Nat. Neurosci. 2018, 21, 1380–1391. [Google Scholar] [CrossRef]
- Hamark, C.; Berntsson, R.P.; Masuyer, G.; Gustafsson, R.; Stenmark, P.; Widmalm, G. Glycans confer specificity to the recognition of ganglioside receptors by botulinum neurotoxin. J. Am. Chem. Soc. 2017, 139, 218–230. [Google Scholar] [CrossRef] [PubMed]
- Dong, M.; Yeh, F.; Tepp, W.H.; Dean, C.; Johnson, E.A.; Janz, R.; Chapman, E.R. SV2 is the protein receptor for botulinum neurotoxin A. Science 2006, 312, 592–596. [Google Scholar] [CrossRef] [PubMed]
- Jacky, B.P.S.; Garaay, P.E.; Dupuy, J.; Nelson, J.B.; Cai, B.; Molina, Y.; Wang, J.; Steward, L.E.; Broide, R.S.; Francis, J.; et al. Identification of fibroblast growth factor receptor 3 (FGFR3) as a protein receptor for botulinum neurotoxin serotype A (BoNT/A). PLoS Pathog. 2013, 9, e1003369. [Google Scholar] [CrossRef] [Green Version]
- Meng, J.; Wang, J.; Lawrence, G.W.; Dolly, O.J. Molecular components required for resting and stimulated endocytosis of botulinum eurotoxins by glutamatergic and peptidergic neurons. FASEB J. 2013, 27, 3167–3180. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Coffield, J.A. Structural and functional interactions between transient receptor potential vanilloid subfamily 1 and botulinum neurotoxin serotype A. PLoS ONE 2016, 11, e0143024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muraro, L.; Tosatto, S.; Motterlini, L.; Rossetto, O.; Montecucco, C. The N-terminal half of the receptor domain of botulinum neurotoxin A binds to microdomains of the plasma membrane. Biochem. Biophys. Res. Commun. 2009, 380, 76–80. [Google Scholar] [CrossRef]
- Pirazzini, M.; Rossetto, O.; Eleopra, R.; Montecucco, C. Botulinum Neurotoxins: Biology, pharmacology, and toxicology. Pharmacaol. Rev. 2017, 69, 200–235. [Google Scholar] [CrossRef]
- Shoemaker, C.B.; Oyler, G.A. Persistence of botulinum neurotoxin inactivation of nerve function. Curr. Top Microbiol. Immunol. 2013, 364, 179–196. [Google Scholar] [PubMed] [Green Version]
- Whitemarsh, R.C.M.; Tepp, W.H.; Johnson, E.A.; Pellett, S. Persistence of botulinum neurotoxin a subtypes 1-5 in primary rat spinal cord cells. PLoS ONE 2014, 9, e90252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belinskaia, M.; Zurawski, T.; Kumar Kaza, S.; Antoniazzi, C.; Dolly, O.J.; Lawrence, G.W. NGF enhances CGRP release evoked by capsaicin from rat trigeminal neurons: Differential inhibitionn by SNAP-25-cleaving proteases. Int. J. Mol. Sci. 2022, 23, 892. [Google Scholar] [CrossRef]
- Neale, E.A.; Bowers, L.M.; Jia, M.; Bateman, K.E.; Williamson, L.C. Botulinum neurotoxin A blocks synaptic vesicle exocytosis but not endocytosis at the nerve terminal. J. Cell Biol. 1999, 147, 1249–1260. [Google Scholar] [CrossRef]
- Melo-Carrillo, A.; Strassman, A.M.; Schain, A.J.; Noseda, R.; Ashina, S.; Adams, A.; Brin, M.F.; Burstein, R. Exploring the effects of extracranial injections of botulinum toxin type A on prolonged intracranial meningeal nociceptors responses to cortical spreading depression in female rats. Cephalalgia 2019, 39, 1358–1365. [Google Scholar] [CrossRef] [PubMed]
- Burstein, R.; Zhang, X.C.; Levy, D.; Aoki, K.R.; Brin, M.F. Selective inhibition of meningeal nociceptors by botulinum neurotoxin type A: Therapeutic implications for migraine and other pains. Cephalalgia 2014, 34, 853–869. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.C.; Strassman, A.M.; Novack, V.; Brin, M.F.; Burstein, R. Extracranial injections of botulinum neurotoxin type A inhibit intracranial meningeal nociceptors’ responses to stimulation of TRPV1 and TRPA1 channels: Are we getting closer to solve this puzzle? Cephalalgia 2016, 36, 875–886. [Google Scholar]
- Durham, P.L.; Cady, R.; Cady, R. Regulation of calcitonin gene-related peptide secretion from trigeminal nerve cells by botulinum toxin type A: Implications for migraine therapy. Headache 2004, 44, 35–43. [Google Scholar] [CrossRef]
- Kitamura, Y.; Matsuka, Y.; Spigelman Im Ishihara, Y.; Yamamoto, Y.; Sonoyama, W.; Kamioka, H.; Yamashiro, T.; Ku-boki, T.; Oguma, K. Botulinum toxin type a (150 kDa) decreases exaggerated neurotransmitter release from trigeminal ganglion neurons and relieves neuropathy behaviours induced by infraorbital nerve constriction. Neuroscience 2009, 159, 1422–1429. [Google Scholar] [CrossRef]
- Gazerani, P.; Staahl, C.; Drewes, A.M.; Arendt-Nielsen, L. The effects of Botulinum Toxin type A on capsaicin-evoked pain, flare, and secondary hyperalgesia in an experimental human model of trigeminal sensitization. Pain 2006, 122, 315–325. [Google Scholar] [CrossRef]
- Gazerani, P.; Pedersen, N.S.; Staahl, C.; Drewes, A.M.; Arendt-Nielsen, L. Subcutaneous Botulinum toxin type A reduces capsaicin-induced trigeminal pain and vasomotor reactions in human skin. Pain 2009, 141, 60–69. [Google Scholar] [CrossRef] [PubMed]
- Matak, I.; Bach-Rojecky, L.; Filipović, B.; Lacković, Z. Behavioral and immunohistochemical evidence for central antinociceptive activity of botulinum toxin A. Neuroscience 2011, 186, 201–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filipovic, B.; Matak, I.; BachRojecky, L.; Lackovic, Z. Central action of peripherally applied botulinum toxin type A on pain and dural protein extravasation in rat model of trigeminal neuropathy. PLoS ONE 2012, 7, e29803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, C.; Xie, N.; Lian, Y.; Xu, H.; Chen, C.; Zheng, Y.; Chen, Y.; Zhang, H. Central antinoniceptive activity of peripherally applied botulinum toxin type A in lab rat model of trigeminal neuralgia. SpringerPlus 2016, 5, 431. [Google Scholar] [CrossRef] [Green Version]
- Restani, L.; Novelli, E.; Bottari, D.; Leone, P.; Barone, I.; Galli-Resta, L.; Strettoi En Caleo, M. Botulinum neurotoxin A impairs neurotransmission following retrograde transynaptic transport. Traffic 2012, 13, 1083–1089. [Google Scholar] [CrossRef] [Green Version]
- Lackovic, Z.; Filipovic, B.; Matak, I.; Helyes, Z. Activity of botulinum toxin type A in cranial dura: Implications from treatment of migraine and other headaches. Br. J. Pharmacol. 2016, 173, 279–291. [Google Scholar] [CrossRef] [Green Version]
- Aurora, S.K.; Dodick, D.W.; Turkel, C.C.; DeGryse, R.E.; Silberstein, S.D.; Lipton, R.B.; Diener, H.C.; Brin, M.F.; PREEMPT 1 Chronic Migraine Study Group. OnabotulinumtoxinA for treatment of chronic migraine: Results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 1 trial. Cephalalgia 2010, 30, 793–803. [Google Scholar] [CrossRef]
- Diener, H.C.; Dodick, D.W.; Aurora, S.K.; Turkel, C.C.; DeGryse, R.E.; Lipton, R.B.; Silberstein, S.D.; Brin, M.F.; PREEMPT 2 Chronic Migraine Study Group. OnabotulinumtoxinA for treatment of chronic migraine: Results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 2 trial. Cephalalgia 2010, 30, 804–814. [Google Scholar] [CrossRef]
- Dodick, D.W.; Turkel, C.C.; DeGryse, R.E.; Aurora, S.K.; Silberstein, S.D.; Lipton, R.B.; Diener, H.C.; Brin, M.F. Onabotuli-numtoxinA for treatment of chronic migraine: Pooled results from the double-blind, randomized, placebo-controlled phases of the PREEMPT clinical program. Headache 2010, 50, 921–936. [Google Scholar] [CrossRef]
- Lipton, R.B.; Varon, S.F.; Grosberg, B.; McAllister, P.J.; Freitag, F.; Aurora, S.K.; Dodick, D.W.; Silberstein, S.D.; Diener, H.C.; DeGryse, R.E.; et al. OnabotulinumtoxinA improves quality of life and reduces impact of chronic migraine. Neurology 2011, 77, 1465–1472. [Google Scholar] [CrossRef]
- Silberstein, S.D.; Blumemfeld, A.M.; Cady, R.K.; Turner, I.M.; Lipton, R.B.; Diener, H.C.; Aurora, S.K.; Sirimanne, M.; DeGryse, R.E.; Turkel, C.C.; et al. OnabotulinumtoxinA for treatment of chronic migraine: PREEMPT 24-week pooled subgroup analysis of patients who had acute headache medication overuse at baseline. J. Neurol. Sci. 2013, 133, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Aurora, S.K.; Winner, P.; Freeman, M.C.; Spierings, E.L.; Heiring, J.O.; DeGryse, R.E.; VanDenburgh, A.M.; Nolan, M.E.; Turkel, C.C. OnabotulinumtoxinA for treatment of chronic migraine: Pooled analyses of the 56-week PREEMPT clinical program. Headache 2011, 51, 1358–1373. [Google Scholar] [CrossRef] [PubMed]
- Lipton, R.B.; Rosen, N.L.; Ailani, J.; DeGryse, R.E.; Gillad, P.J.; Varon, S.F. OnabotulinumtoxinA improves quality of life and reduces impact of chronic migraine over one year of treatment: Pooled results from the PREEMPT random-ized clinical trial program. Cephalalgia 2016, 36, 899–908. [Google Scholar] [CrossRef]
- Matharu, M.; Halker, R.; Pozo-Rosich, P.; Manack, A.A.; Aurora, S.K. The impact of onabotulinumtoxinA on severe headache days: PREEMPT 56-week pooled analysis. J. Headache Pain 2017, 18, 78. [Google Scholar] [CrossRef] [Green Version]
- Silberstein, S.D.; Dodick, D.W.; Aurora, S.K.; Diener, H.C.; DeGryse, R.E.; Lipton, R.B.; Turkel, C.C. Per cent of patients with chronic migraine who responded per onabotulinumtoxinA treatment cycle: PREEMPT. J. Neurol. Neurosurg. Psychiatry 2015, 86, 996–1001. [Google Scholar] [CrossRef] [PubMed]
- Pijpers, J.A.; Kies, D.A.; Louter, M.A.; van Zwet, E.W.; Ferrari, M.D.; Terwindt, G.M. Acute withdrawal and botulinum toxin A in chronic migraine with medication overuse: A double-blind randomized controlled trial. Brain 2019, 142, 1203–1214. [Google Scholar] [CrossRef] [Green Version]
- Dodick, D.W.; Silberstein, S.D.; Lipton, R.B.; DeGreyse, R.E.; Adams, A.M.; Diener, H.C. Early onset of effect of OnabotulinumtoxinA for chronic migraine treatment: Analysis of PREEMPT data. Cephalalgia 2019, 39, 945–956. [Google Scholar] [CrossRef]
- Aurora, S.K.; Dodick, D.W.; Diener, H.C.; DeGryse, R.E.; Turkerl, C.C.; Lipton, R.B.; Silberstein, S.D. OnabotulinumtoxinA for chronic migraine: Efficacy, safety, and tolerability in patients who received all five treatment cycles in the PREEMPT clinical program. Acta Neurol. Scand. 2014, 129, 61–70. [Google Scholar] [CrossRef] [Green Version]
- Rothrock, J.F.; Adams, A.M.; Lipton, R.B.; Silberstein, S.D.; JoE; Zhao, X.; Blumenfeld, A.M. FORWARD Study Investigative Group. FORWARD Study: Evaluating the comparative effectiveness of OnabotulinumtoxinA and topiramate for headache prevention in adults with chronic migraine. Headache 2019, 59, 1700–1713. [Google Scholar]
- Blumenfeld, A.M.; Patel, A.T.; Turner, I.M.; Mullin, K.B.; Adams, A.M.; Rothrock, J.F. Patient-reported outcomes from a 1-year, real-world, head-to-head comparison of OnabotulinumtoxinA and topiramate for headache prevention in adults with chronic migraine. J. Prim. Care Community Health 2020, 11, 2150132720959936. [Google Scholar] [CrossRef]
- Khalil, M.; Zafar, H.W.; Quarshie, V.; Ahmed, F. Prospective analysis of the use of OnabotulinumtoxinA (BOTOX) in the treatment of chronic migraine; real-life data in 254 patients from Hull, UK. J. Headache Pain 2014, 15, 54. [Google Scholar] [CrossRef] [PubMed]
- Pedraza, M.I.; de la Cruz, C.; Ruiz, M.; Lopez-Mesonero, L.; Martinez, E.; de Lera, M.; Guerrero, A.L. OnobatulinumtoxinA treatment of chronic migraine: Experience in 52 patients treated with the PREEMPT paradigm. SpringerPlus 2015, 4, 176. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, F.; Zafar, H.W.; Buture, A.; Khalil, M. Does analgesic overuse matter? Response to OnabotulinumtoxinA in patients with chronic migraine with or without medication overuse. SpringerPlus 2015, 4, 589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cernuda-Morollon, E.; Ramon, C.; Larrosa, D.; Alvarez, R.; Riesco, N.; Pascual, J. Long-term experience with onabotulinumtoxinA in the treatment of chronic migraine: What happens after one year? Cephalalgia 2015, 35, 864–868. [Google Scholar] [CrossRef] [PubMed]
- Maasumi, K.; Thompson, N.R.; Kriegler, J.S.; Tepper, S.J. Effect of onabotulinumtoxinA injection on depression in chronic migraine. Headache 2015, 55, 1218–1224. [Google Scholar] [CrossRef] [PubMed]
- Negro, A.; Curto, M.; Lionetto, L.; Crialesi, D.; Martelletti, P. OnabotulinumtoxinA 155 U in medication overuse headache: A two years prospective study. SpringerPlus 2015, 4, 826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guerzoni, S.; Pellesi, L.; Baraldi, C.; Pini, L.A. Increased efficacy of regularly repeated cycles with OnabotulinumtoxinA in MOH patients beyond the first year of treatment. J. Headache Pain 2016, 17, 48. [Google Scholar] [CrossRef] [Green Version]
- Vikelis, M.; Argyruou, A.A.; Dermitzakis, E.V.; Spingos, K.C.; Mitsikostas, D.D. Onabotulinumtoxin-A treatment in Greek patients with chronic migraine. J. Headache Pain 2016, 17, 84. [Google Scholar] [CrossRef] [Green Version]
- Aicua-Rapun, I.; Martìnez-Velasco, E.; Rojo, A.; Hernando, A.; Ruiz, M.; Carreres, A.; Porqueres Em Herrero, S.; Iglesias, F.; Guerrero, A.L. Real-life data in 115 chronic migraine patients treated with OnabotulinumtoxinA during more than one year. J. Headache Pain 2016, 17, 112. [Google Scholar] [CrossRef] [Green Version]
- Russo, M.; Manzoni, G.C.; Taga, A.; Genovese, A.; Veronesi, L.; Paquarella, C.; Sansebastiano, G.E.; Torelli, P. The use of onabotulinum toxin A (Botox®) in the treatment of chronic migraine at the Parma Headache Centre: A prospective observational study. Neurol. Sci. 2016, 37, 1127–1131. [Google Scholar] [CrossRef]
- Demiryurek, B.E.; Ertem, D.H.; Tekin, A.; Ceylan, M.; Aras, Y.G.; Gungen, B.D. Effects of onabotulinumtoxinA treatment on efficacy, depression, anxiety, and disability in Turkish patients with chronic migraine. Neurol. Sci. 2016, 37, 1779–1784. [Google Scholar] [CrossRef] [PubMed]
- Negro, A.; Curto, M.; Lionetto, L.; Martelletti, P. A two years open-label prospective study of OnabotulinumtoxinA 195 U in medication overuse headache: A real-world experience. J. Headache Pain 2015, 17, 1. [Google Scholar] [CrossRef] [PubMed]
- Aydinlar, E.I.; Dikmen, P.Y.; Kosak, S.; Kocaman, A.S. OnabotulinumtoxinA effectiveness on chronic migraine, negative emotional states and sleep quality: A single-center prospective cohort study. J. Headache Pain 2017, 18, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matharu, M.; Pascual, J.; Nilsson Remahl, I.; Straube, A.; Lum, A.; Davar, G.; Odom, D.; Bennett, L.; Proctor, C.; Gutierrez, L.; et al. Utilization and safety of onabotulinumtoxinA for the prophylactic treatment of chronic migraine from an observational study in Europe. Cephalalgia 2017, 37, 1384–1397. [Google Scholar] [CrossRef] [Green Version]
- Byun, J.I.; Sim, J.Y.; Kim, M. Prolonged effect of OnabotulinumtoxinA on chronic migraine in 87 koreans. J. Clin. Neurol. 2017, 13, 98–100. [Google Scholar] [CrossRef] [Green Version]
- Guerzoni, S.; Pellesi, L.; Baraldi, C.; Cainazzo, M.M.; Negro, A.; Martelletti, P.; Pini, L.A. Long-term treatment benefits and prolonged efficacy of OnabotulinumtoxinA in patients affected by chronic migraine and medication overuse headache over 3 years of therapy. Front. Neurol. 2017, 8, 586. [Google Scholar] [CrossRef] [Green Version]
- Dikmen, P.Y.; Kosak, S.; Aydinlar, E.I.; Kocaman, A.S. A single-center retrospective study of onabotulinumtoxinA for treatment of 245 chronic migraine patients: Survey results of a real-world experience. Acta Neur. Belg. 2018, 118, 475–484. [Google Scholar] [CrossRef]
- Blumenfeld, A.M.; Stark, R.J.; Freeman, M.C.; Orejudos, A.; Manack, A.A. Long-term study of the efficacy and safety of OnabotulinumtoxinA for the prevention of chronic migraine: COMPEL study. J. Headache Pain 2018, 19, 13. [Google Scholar] [CrossRef] [Green Version]
- Domínguez, C.; Pozo-Rosich, P.; Torres-Ferrús, M.; Hernández-Beltrán, N.; Jurado-Cobo, C.; González-Oria, C.; Santos, S.; Monzón, M.J.; Latorre, G.; Álvaro, L.C.; et al. OnabotulinumtoxinA in chronic migraine: Predictors of response. A prospective multicentre descriptive study. Eur. J. Neurol. 2018, 25, 411–416. [Google Scholar] [CrossRef]
- Vikelis, M.; Argryriou, A.A.; Dermitzakis, E.V.; Spingos, K.C.; Makris, N.; Kararizou, E. Sustained onabotulinumtoxinA therapeutic benefits in patients with chronic migraine over 3 years of treatment. J. Headache Pain 2018, 19, 87. [Google Scholar] [CrossRef]
- Blumenfeld, A.M.; Tepper, S.J.; Robbins, L.D.; Manack, A.A.; Buse, D.C.; Orejudos, A.; Silberstein, S. Effects of onabotulinumtoxinA treatment for chronic migraine on common comorbidities including depression and anxiety. J. Neurol. Neurosurg. Psychiatry 2019, 90, 353–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andreou, A.P.; Trimboli, M.; Al-Kaisy, A.; Murphy, M.; Palmisani, S.; Fenech, C.; Smith, T.; Lambru, G. Prospective real-world analysis of OnabotulinumtoxinA in chronic migraine post-National Institute for Health and Care Excellence UK technology appraisal. Eur. J. Neurol. 2018, 25, 1069–1083. [Google Scholar] [CrossRef]
- Caronna, E.; Gallardo, V.J.; Hernandez-Beltran, N.; Torres-Ferrus, M.; Pozo-Rosich, P. OnabotulinumtoxinA: An effective tool in the therapeutic arsenal for chronic migraine with medication overuse. Front. Neurol. 2018, 9, 808. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, F.; Gaul, C.; García-Moncó, J.C.; Sommer, K.; Martelletti, P. REPOSE Principal Investigators. An open-label prospective study of the real-life use of onabotulinumtoxinA for the treatment of chronic migraine: The REPOSE study. J. Headache Pain 2019, 20, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quintas, S.; Garcia-Azorin, D.; Heredia, P.; Talavera, B.; Gago-Viega, A.B.; Guerrero, A.L. Wearing off response to OnabotulinumtoxinA in chronic migraine: Analysis in a series of 193 patients. Pain Med. 2019, 20, 1815–1821. [Google Scholar] [CrossRef] [PubMed]
- Ching, J.; Tinsley, A.; Rothrock, J. Prognosis following discontinuation of OnabotulinumA therapy in “super-responding” chronic migraine patients. Headache 2018, 59, 1279–1285. [Google Scholar] [CrossRef]
- Alpuente, A.; Gallardo, V.J.; Torres-Ferrus, M.; Alvarez-Sabin, J.; Pozo-Rosich, P. Early efficacy and late gain in chronic and high frequency episodic migraine with onabotulinumtoxinA. Eur. J. Neurol. 2019, 26, 1464–1470. [Google Scholar] [CrossRef]
- Davies, B.; Gaul, C.; Martelletti, P.; Garcia-Moncò, J.C.; Brown, S. Real-life use of onabotulinumtoxinA for symptom relief in patients with chronic migraine: REPOSE study methodology and baseline data. J. Headache Pain 2017, 18, 93. [Google Scholar] [CrossRef] [Green Version]
- Santoro, A.; Copetti, M.; Miscio, A.M.; Leone, M.A.; Fontana, A. Chronic migraine long-term regular treatment with onabotulinumtoxinA: A retrospective real-life observational study up to 4 years of therapy. Neurol. Sci. 2020, 41, 1809–1820. [Google Scholar] [CrossRef] [Green Version]
- Stark, C.; Stark, R.; Limber, N.; Rodrigues, J.; Cordato, D.; Schwartz, R.; Jukic, R. Real-world effectiveness of onabotulinumtoxinA treatment for the prevention of headaches in adults with chronic migraine in Australia: A retrospective study. J. Headache Pain 2019, 20, 81. [Google Scholar] [CrossRef] [Green Version]
- De Tommaso, M.; Brighina, F.; Delussi, M. Effect of Botulinum Toxin A on allodynia in chronic migraine: An observational open-label two-years study. Eur. Neurol. 2019, 81, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Young, W.B.; Lopez, J.I.; Rothrock, J.F.; Orejundos, A.; Manack, A.A.; Lipton, R.B.; Blumenfeld, A.M. Effects of onabotulinumtoxinA treatment in patients with and without allodynia: Results of the COMPEL study. J. Headache Pain 2019, 20, 10. [Google Scholar] [CrossRef] [PubMed]
- Ornello, R.; Guerzoni, S.; Baraldi, C.; Evangelista, L.; Frattale, I.; Marini, C.; Tiseo, C.; Pistoia, F.; Sacco, S. Sustained response to onabotulinumtoxin A in patients with chronic migraine: Real-life data. J. Headache Pain 2020, 21, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, W.B.; Lopez, J.I.; Rothrock, J.F.; Orejudos, A.; Manack, A.A.; Lipton, R.B.; Blumenfeld, A.M. Effects of onabotulinumtoxinA treatment in chronic migraine patients with and without daily headache at baseline: Results from the COMPEL Study. J. Headache Pain 2019, 20, 12. [Google Scholar] [CrossRef] [Green Version]
- Barad, M.; Sturgeon, J.A.; Fish, S.; Dexter, F.; Mackey, S.; Flood, P.D. Response to BotulinumtoxinA in a migraine cohort with multiple comorbidities and widespread pain. Reg. Anesth. Pain Med. 2019, 44, 660–668. [Google Scholar] [CrossRef]
- Diener, H.C.; Dodick, D.W.; Turkel, C.C.; Demos, G.; Degryse, R.E.; Earl, N.L.; Brin, M.F. Pooled analysis of the safety and tolerability of onabotulinumtoxinA in the treatment of chronic migraine. Eur. J. Neurol. 2014, 21, 851–859. [Google Scholar] [CrossRef] [Green Version]
- Winner, P.K.; Blumenfeld, A.M.; Eross, E.J.; Orejudos, A.C.; Mirjah, D.L.; Manack, A.A.; Brin, M.F. Long-term safety and tolerability of OnabotulinumtoxinA treatment in patients with chronic migraine: Results of the COMPEL study. Drug Saf. 2019, 42, 1013–1024. [Google Scholar] [CrossRef] [Green Version]
- Hepp, Z.; Rosen, N.L.; Gillard, P.G.; Varon, S.F.; Mathew, N.; Dodick, D.W. Comparative effectiveness of onabotulinumtoxinA versus oral migraine prophylactic medications on headache-related resource utilization in the management of chronic migraine: Retrospective analysis of a US-based insurance claims database. Cephalalgia 2016, 36, 862–874. [Google Scholar] [CrossRef]
- Rothrock, J.F.; Bloudek, L.M.; Houle, T.T.; Rothrpck, D.A.; Varon, S.F. Real-world economic impact of OnabotulinumtoxinA in patients with chronic migraine. Headache 2014, 54, 1565–1573. [Google Scholar] [CrossRef]
- Vernieri, F.; Paolucci, M.; Altamura, C.; Pasqualetti, P.; Mastrangelo, V.; Pierangeli, G.; Cevoli, S.; D’Amico, D.; Grazzi, L. Onabotulinumtoxin-A in chronic migraine: Should timing and definition of non-responder status be revised? Suggestions from a real-life Italian multicenter experience. Headache 2019, 59, 1300–1309. [Google Scholar] [CrossRef]
- Masters-Israilov, A.; Robbins, M.S. OnabotulinumtoxinA wear-off phenomenon in the treatment of chronic migraine. Headache 2019, 59, 1753–1761. [Google Scholar] [CrossRef]
- Ruscheweyh, R.; Athwal, B.; Gryglas-Dworak, A.; Frattale, I.; Latysheva, N.; Ornello, R.; Pozo-Rosich, P.; Sacco, S.; Torres-Ferrus, M.; Stark, C.D. Wear-off of OnabotulinumtoxinA effect over the treatment interval in chronic migraine: A retrospective chart review with analysis of headache diaries. Headache 2020, 60, 1673–1682. [Google Scholar] [CrossRef] [PubMed]
- Baraldi, C.; Ornello, R.; Favoni, V.; Sacco, S.; Cponnetto, V.; Pierangeli, G.; Cevoli, S.; Guerzoni, S. Chroni migraine and medication overuse headache worsening after OnabotulinumtoxinA withdrawn due to the severe acute respiratory syndrome-coronavirus-2 pandemic. Front. Neurol. 2021, 12, 647995. [Google Scholar] [CrossRef] [PubMed]
- Ornello, R.; Ahmed, F.; BNegro, A.; Miscio, A.M.; Santoro, A.; Alpuente, A.; Russo, A.; Silvestro, M.; Cevoli, S.; Brunelli, N.; et al. Early management of OnabotulinumtoxinA treatment in chronic migraine: Insights from a real-life European multicenter study. Pain Ther. 2021, 10, 637–650. [Google Scholar] [CrossRef]
- Ornello, R.; Ahmed, F.; BNegro, A.; Miscio, A.M.; Santoro, A.; Alpuente, A.; Russo, A.; Silvestro, M.; Cevoli, S.; Brunelli, N.; et al. Is there a gender difference in the response to onabotulinumtoxinA ion chronic migraine? Insights from a real-life European multicenter study on 2879 patients. Pain Ther. 2021, 10, 1605–1618. [Google Scholar] [CrossRef] [PubMed]
- Ornello, R.; Baraldi, C.; Ahmed, F.; Negro, A.; Miscio, A.M.; Santoro, A.; Alpuente, A.; Russo, A.; Silvestro, M.; Cevoli, S.; et al. Excellent response to OnabotulinumtoxinA: Different definitions, different predictors. Int. J. Environ. Res. Public Health 2022, 19, 10975. [Google Scholar] [CrossRef]
- Altamura, C.; Ornello, R.; Ahmed, F.; Negro, A.; Miscio, A.M.; Santoro, A.; Alpuente, A.; Russo, A.; Silvestro, M.; Cevoli, S.; et al. OnabotulinumtoxinA in elderly patients with chronic migraine: Insights from a real-life European multicenter study. J. Neurol. 2022. [Google Scholar] [CrossRef]
- Kara, M.; Sekizkardes, M.; Gürçay, E.; Akinci, A.; Özçakar, L. Ultrasound-guided perisutural botulinum toxin injection for chronic migraine headache. Initial report with technical description. Am. J. Phys. Med. Rehab. 2019, 98, e98–e100. [Google Scholar] [CrossRef]
- Kara, M.; Erdam, Y.S.; Doğan, Y.; Erdal, O.D.; D’Amico, V.; Özçakar, L. The chronicle of headache treatment throught human history from trepanation to perisutural botulinum toxin injections. Int. J. Neurosci. 2022, 1–4. [Google Scholar] [CrossRef]
- Murat, K.; Gürcay, E.; Gülümser, A.; Kaymak, B.; Sekizkardes, M.; Akinci, A.; Uludüz, D.; Özçakar, L. Botulinum toxin injections to cranial sutures for chronic migraine revwinding the technique using ultrasound imaging. Toxicon 2019, 172, 19–22. [Google Scholar]
- Kara, M.; Sekizkardes, K.M.; Özçakar, L. The effects/injections of botulinum toxin in chronic migraine headache. Acta Neurol. Scand. 2018, 138, 99. [Google Scholar] [CrossRef] [PubMed]
- De Matteis, E.; Guglielmetti, M.; Ornello, R.; Spuntarelli, V.; Martelletti, P.; Sacco, S. Targeting CGRP for migraine treatment: Mechanisms, antibodies, small molecules, perspectives. Expert. Rev. Neurother. 2020, 20, 627–641. [Google Scholar] [CrossRef]
- Ondo, W.G.; Simmons, J.H.; Shahid, M.H.; Hashem, V.; Hunter, C.; Jankovic, J. Onabotulinum toxin-A injections for sleep bruxism: A double-blind, placebo-controlled study. Neurology 2018, 90, e559–e564. [Google Scholar] [CrossRef] [PubMed]
- Guerzoni, S.; Baraldi, C.; Pani, L. The association between onabotulinumtoxinA and anti-CGRP monoclonal antibodies: A reliable option for the optimal treatment of chronic migraine. Neurol. Sci. 2022, 43, 5687–5695. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | Number of Patients | Time Point | Outcome | BT−A | Control | Mean Interchange Difference | p−Value |
|---|---|---|---|---|---|---|---|
| Aurora et al., 2010 (PREEMPT-1) [66] | 679: 341: BT-A 338: Placebo | 24 weeks | Change from baseline in the frequency of headache episodes | −5.2 | −5.3 | 0.1 (−1.12, 0.39) | 0.334 |
| Change from baseline in frequency of headache days | −7.8 | −6.4 | −1.4 (−2.40, −0.40) | 0.006 | |||
| Change from baseline in frequency of migraine days | −7.6 | −6.1 | −1.5 (−2.60, −0.59) | 0.002 | |||
| Change from baseline in frequency of migraine episodes | −4.8 | −4.9 | 0.1 (−1.21, 0.26) | 0.206 | |||
| Change from baseline in frequency of triptan intake | −3.3 | −2.5 | −0.8 (−1.69, −0.13 | 0.023 | |||
| Change from baseline of HIT-6 score | −4.7 | −2.4 | −2.3 (−3.25, −1.31) | <0.001 | |||
| Diener et al., 2010 (PREEMPT-2) [67] | 705: 347:BT-A 358: Placebo | 24 weeks | Change from baseline in frequency of headache days | −9 | −6.7 | −2.3 (−3.25, −1.31) | <0.001 |
| Change from baseline in frequency of migraine days | −8.7 | −6.3 | −2.4 (−3.31, −1.36) | <0.001 | |||
| Change from baseline in frequency of moderate/severe headache days | −8.3 | −5.8 | −2.5 (−3.37, −1.48) | <0.001 | |||
| Change from baseline in cumulative total headache hours on headache days | −132.4 | −90 | −42.4 (−58.23, −21.05) | <0.001 | |||
| Percent of patients with severe (60) HIT-6 score | 66.3 | 76.5 | −10.2 (−16.9, −3.6) | 0.003 | |||
| Change from baseline in frequency of headache episodes | −5.3 | −4.6 | −0.7 (−1.65, −0.33) | 0.003 | |||
| Change from baseline in total HIT-6 scores | −4.9 | −2.4 | −2.5 (−3.54, −1.55) | <0.001 | |||
| Change from baseline in frequency of acute headache pain medication intakes (all categories) | −9.9 | −8.4 | −1.5 (−3.77, 0.49) | 0.132 | |||
| Change from baseline in frequency of triptan intake | −3 | −1.7 | −1.3 (−2.24, −0.6) | <0.001 | |||
| Dodick et al., 2010 (PREEMPT-1 and 2) [68] | 1384 688: BT-A 696: Placebo | 24 weeks | Change from baseline in frequency of headache days | −8.4 | −6.6 | −1.8 (−2.52, −1.13) | <0.001 |
| Change from baseline in frequency of migraine days | −8.2 | −6.2 | −2.0 (−2.67, −1.27) | <0.001 | |||
| Change from baseline in frequency of moderate/severe headache days | −7.7 | −5.8 | −1.9 (−2.62, −1.26) | <0.001 | |||
| Change from baseline in cumulative total headache hours on headache days | −119.7 | −80.5 | −39.2 (−48.40, −21.04) | <0.001 | |||
| Percent of patients with severe (≥60) HIT-6 score | 67.6% | 78.2% | −10.6% (−15.2%, −5.9%) | <0.001 | |||
| Change from baseline in frequency of headache episodes | −5.2 | −4.9 | −0.3 (−1.17, −0.17) | 0.009 | |||
| Change from baseline in frequency of migraine episodes | −4.9 | −4.5 | −0.4 (−1.20, −0.23) | 0.004 | |||
| Change from baseline in frequency of acute headache pain medication intakes (all categories) | −10.1 | −9.4 | −0.7 (−2.68, 0.69) | 0.247 | |||
| Change from baseline in frequency of triptan intake | −3.2 | −2.1 | −1.1 (−1.74, −0.61) | <0.001 | |||
| Change from baseline in total HIT-6 scores | −4.8 | .2.4 | −2.4 (−3.11, −1.72) | <0.001 | |||
| Change from baseline in MSQ score | |||||||
| Role function−restrictive | 17 | 8.6 | 8.4 (10.76, 6.01) | <0.001 | |||
| Role function−preventative | 13.1 | 6.4 | 6.7 (9.01, 4.35) | <0.001 | |||
| Emotional function | 17.9 | 9.5 | 8.4 (11.37, 5.56) | <0.001 | |||
| Lipton et al., 2011 (PREEMPT-1 and 2) [69] | 1384 688: BT-A 696: Placebo | 12 weeks | Change from the baseline in the HIT-6 score | −4.7 | −2.6 | 2.1 | <0.001 |
| Change from the baseline in the MSQ score (restrictive) | 16.2 | 9.9 | 6.3 | <0.001 | |||
| Change from the baseline in the MSQ score (preventive) | 13 | 8 | 5.0 | <0.001 | |||
| Change from the baseline in the MSQ score (functioning) | 18.3 | 11 | 7.3 | <0.001 | |||
| 24 weeks | Change from the baseline in the HIT-6 score | −4.8 | −2.4 | 2.4 | <0.001 | ||
| Change from the baseline in the MSQ score (restrictive) | 17 | 8.6 | 8.4 | <0.001 | |||
| Change from the baseline in the MSQ score (preventive) | 13.1 | 6.4 | 6.7 | <0.001 | |||
| Change from the baseline in the MSQ score (functioning) | 17.9 | 9.5 | 8.4 | <0.001 | |||
| Silberstein et al., 2013 (PREEMPT-1 and 2) [70] | 904 445: BT-A 459: Placebo | 24 weeks | Change from the baseline in the frequency of headache days | −8.2 (0.3) | −6.2 (0.31) | − | <0.001 |
| Change from the baseline in the frequency of migraine | −8.1 (0.3) | −6 (0.31) | − | <0.001 | |||
| Change from the baseline in the frequency of moderate/severe headache days | −7.7 (0.29) | −5.7 (0.31) | − | <0.001 | |||
| Change from the baseline in the total cumulative hours of headache on headache days | −114.5 (5.77) | −70.8 (6.08) | − | <0.001 | |||
| Percent of patients with severe (≥60) HIT-6 score | 71% | 81.9% | − | <0.001 | |||
| Change from the baseline in the frequency of headache episodes | −5.4 (0.26) | −5.1 (0.25) | − | 0.028 | |||
| Change from the baseline in the frequency of migraine episodes | −5.1 (0.25) | −4.8 (0.25) | − | 0.018 | |||
| Change from the baseline in the frequency of acute headache medication intakes | −13.1 (0.9) | −11.8 (0.89) | − | 0.21 | |||
| Change from the baseline in the total HIT-6 score | −4.7 | −2.2 | − | <0.001 | |||
| MSQ score (restrictive) | 16.9 | 7.6 | − | <0.001 | |||
| MSQ score (preventive) | 13.9 | 5.8 | − | <0.001 | |||
| MSQ score (functioning) | 18.3 | 8.7 | − | <0.001 | |||
| Change from the baseline in the frequency of triptan intake | −3.3 (0.22) | −2.4 (0.1) | − | <0.001 | |||
| Aurora et al., 2011 (PREEMPT-1 and 2) [71] | 1384 688: BoNT/A 696: Placebo | 56 weeks | Change from baseline in mean frequency of headache days | −11.7 (−12.17, −11.20) | −10.8 (−11.32, −10.31) | −0.9 (−1.53, −0.14) | 0.019 |
| Change from baseline in mean frequency of migraine days | −11.2 (−11.71, −10.74) | −10.3 (−10.82, −9.80) | −0.9 (−1.52, −0.14) 0.018 | 0.018 | |||
| Change from baseline in mean frequency of moderate/severe headache day | −10.7 (−11.18, −10.25) | −9.9 (−10.43, −9.44) | −0.8 (−1.41, −0.09) 0.027 | 0.027 | |||
| Change from baseline in cumulative total headache hours on headache days | −169.1 (−179.30, −158.81) | −145.7 (−155.94, −135.36) | −23.4 (−29.15, −2.78) 0.018 | 0.018 | |||
| Percent of patients with severe (60) HIT-6 score | 50.6% (46.9%, 54.3%) | 51.9% (48.2%, 55.6%) | −1.3% (−6.6%, 4.0%) | 0.632 | |||
| Change from baseline in mean frequency of headache episodes | −7.4 (−7.79, −6.97) | −7.5 (−7.91, −7.09) | 0.1 (−0.87, −0.04) | 0.075 | |||
| Change from baseline in mean frequency of migraine episodes | −6.8 (−7.21, −6.43) | −7.0 (−7.37, −6.58) | 0.2 (−0.80, −0.09) | 0.117 | |||
| Change from baseline in mean frequency of acute headache medication intakes | −15.4 (−16.74, −14.05) | −15.7 (−17.05, −14.33) | 0.3 (−1.76, −1.29) | 0.76 | |||
| Change from baseline in mean frequency of triptan intakes | −4.2 (−4.69, −3.67)−3.8 (−4.35, −3.27) | −3.8 (−4.35, −3.27) | −0.4 (−1.02, −0.06) 0.080 | 0.08 | |||
| Change from baseline in mean frequency of acute headache medication days | −8.4 (−9.08, −7.79) | −8.5 (−9.16, −7.82) | 0.1 (−1.19, 0.46) | 0.387 | |||
| Change from baseline in total HIT-6 scores | −7.7 (−8.24, −7.06) | −7.0 (−7.62, −6.40) | −0.6 (−1.49, 0.20) | 0.069 | |||
| Change from the baseline in the total MSQ score | |||||||
| MSQ score (restrictive) | 25.2 (27.27, 23.08) | 21.8 (23.93, 19.63) | 3.4 (6.41, 0.39) | 0.043 | |||
| MSQ score (preventive) | 19.0 (21.06, 17.01) | 17.3 (19.40, 15.26) | 1.7 (4.60, 1.20) | 0.293 | |||
| MSQ score (functioning) | 25.0 (27.41, 22.60) | 22.1 (24.66, 19.62) | 2.9 (6.36, −0.62) | 0.51 | |||
| Lipton et al., 2016 (PREEMPT-1 and 2) [72] | 1384 688: BoNT/A 696: Placebo | 36 weeks | Change from baseline in total HIT-6 scores | −7 | −5.8 | − | 0.002 |
| Percentage of patients with severe or substantial impact | 68% | 74% | − | 0.022 | |||
| Percentage of patients with a ≥5 points decrease in the HIT-6 score | 57% | 51% | − | 0.002 | |||
| Patients with a ≥50% decrease in the headache days | 56% | 53% | − | ||||
| Percentage of patients with ≥5–point decrease in HIT-6 score and ≥50% reduction in headache days | 40% | 35% | − | 0.022 | |||
| 48 weeks | Change from baseline in total HIT-6 scores | −7.1 | −6.1 | − | 0.022 | ||
| Percentage of patients with severe or substantial impact | 68% | 71% | − | >0.05 | |||
| Percentage of patients with a ≥5 points decrease in the HIT-6 score | 56% | 52% | − | >0.05 | |||
| Patients with a ≥50% decrease in the headache days | 61% | 57% | − | >0.05 | |||
| Percentage of patients with ≥5–point decrease in HIT-6 score and ≥50% reduction in headache days | 38% | 43% | − | >0.05 | |||
| 56 weeks | Change from baseline in total HIT-6 scores | −7.7 | −7 | − | >0.05 | ||
| Percentage of patients with severe or substantial impact | 68% | 66% | − | >0.05 | |||
| Percentage of patients with a ≥5 points decrease in the HIT-6 score | 59% | 57% | − | >0.05 | |||
| Patients with a ≥50% decrease in the headache days | 67% | 61% | − | 0.022 | |||
| Percentage of patients with ≥5–point decrease in HIT-6 score and ≥50% reduction in headache days | 49% | 43% | − | 0.022 | |||
| Mataharu et al., 2017 [73] | 1384 688: BoNT/A 696: Placebo | 24 weeks | Percentage of reduction in the severe headache days | 41.1% | 31.1% | − | 0.011 |
| 56 weeks | Percentage of reduction in the severe headache days | 64.6% | 65.6% | − | 0.792 | ||
| Silberstein et al., 2014 (PREEMPT-1 and 2) [74] | 1384 688: BoNT/A 696: Placebo | 12 weeks | Percentage of patients with a ≥50% reduction in the frequency of headache days | 49.3% | − | − | − |
| Percentage of patients with a ≥50% reduction in the frequency of moderate/severe days | 53.1% | − | − | − | |||
| Percentage of patients with a ≥50% reduction in the cumulative hours of headache on headache days | 54.2% | − | − | − | |||
| Percentage of patients with a ≥5 points reduction in the HIT-6 score | 57.6% | − | − | − | |||
| Pijpers et al., 2019 [75] | 179 90: BT-A 89: placebo | 12 weeks | Change from baseline in mean frequency of headache days | −5.6 | −4.4 | − | 0.7 |
| Change from baseline in mean frequency of migraine days | −6.2 | −7 | − | 0.38 | |||
| Change from baseline in moderate/severe headache days | −4.9 | −5.4 | − | 0.55 | |||
| Change in hours of headache | −20.8 | −13.3 | − | 0.66 | |||
| Transformation of chronic migraine to episodic migraine | 62.5% | 57% | − | 0.29 | |||
| 25% responder rate | 48.3% | 37.8% | − | 0.16 | |||
| 50% responder rate | 18.1% | 20.4% | − | 0.69 | |||
| Succeed to withdraw from medication | 89.7% | 89.8% | − | 0.89 | |||
| Change from the baseline in the HIT-6 score | −0.8 | −0.8 | − | 0.96 | |||
| Change from the baseline in the MIDAS score | 18.7 | 24 | − | 0.67 | |||
| Dodick et al., 2019 (PREEMPT-1 and 2) [76] | 1384 688: BT-A 696: Placebo | 1 week | Change from the baseline in the number of headache days per week | −0.9 ± 2.2 | −0.7 ± 2.1 | − | 0.046 |
| 3 week | Change from the baseline in the number of headache days per week | −1.6 ± 2.2 | −1.1 ± 2.2 | − | <0.001 | ||
| 4 week | Change from the baseline in the number of headache days per week | −1.6 ± 2.2 | −1.2 ± 2.2 | − | <0.001 | ||
| Aurora et al., 2014 (PREEMPT-1 and 2) [77] | 1384 688: BT-A 696: Placebo | 24 weeks | Change from the baseline in the frequency of headache days | −8.8 (−9.4, −8.2) | −6.5 (−7.1, −5.9) | − | <0.001 |
| Change from the baseline in the frequency of migraine days | −8.6 (−9.2, −8.0) | −6.2 (−6.7, −5.5) | − | <0.001 | |||
| Change from baseline in moderate/severe headache days | −8.2 (−8.7, −7.6) | −5.8 (−6.4, −5.2) | − | <0.001 | |||
| Change from the baseline in the cumulative headache hours on headache days | −121.8 (−135.9, −112.2) | −82.0 (−91.9, −67.3) | − | <0.001 | |||
| Change from the baseline in the frequency of headache episodes | −5.9 (−6.1, −5.2) | −4.8 (−5.4, −4.4) | − | <0.001 | |||
| Change from the baseline in the frequency of migraine episodes | −5.5 (−5.8, −4.9) | −4.4 (−5.0, −4.1) | − | <0.001 | |||
| Change in the frequency of medication intake for headache | −10.4 (−11.8, −8.7) | −9.3 (−11.0, −8.0) | − | 0.293 | |||
| Change from the baseline in the frequency of triptan intake | −3.4 (−3.8, −2.8) | −2.1 (−2.8, −1.6) | − | <0.001 | |||
| 56 weeks | Change from the baseline in the frequency of headache days | −12.0 (−12.6, −11.5) | −11.1 (−11.8, −10.5) | − | 0.035 | ||
| Change from the baseline in the frequency of migraine days | −11.6 (−12.2, −11.0) | −10.7 (−11.3, −10.0) | − | 0.038 | |||
| Change from baseline in moderate/severe headache days | −11.0 (−11.5, −10.4) | −10.1 (−10.7, −9.5) | − | 0.042 | |||
| Change from the baseline in the cumulative headache hours on headache days 166.8 (182.7, 158.2) | −166.8 (−182.7, −158.2) | −151.2 (−160.5, −134.3) | − | 0.063 | |||
| Change from the baseline in the frequency of headache episodes | −8.1 (−8.3, −7.4) | −7.5 (−8.3, −7.3) | − | 0.057 | |||
| Change from the baseline in the frequency of migraine episodes | −7.5 (−7.7, −6.8) | −7.0 (−7.8, −6.8) | − | 0.088 | |||
| Change in the frequency of medication intake for headache | −16.1 (−17.4, −14.1) | −16.1 (−18.2, −14.8) | − | 0.939 | |||
| Change from the baseline in the frequency of triptan intake | −4.6 (−5.1, −3.9) | −4.2 (−5.0, −3.7) | − | 0.166 | |||
| Rothrock et al., 2019 [78] | 282 140: BT−A 142: topiramate 50−100 mg | 32 weeks | Percentage of ≥50% responders | 40% | 12% | 4.9 [95% CI, 2.7 ÷ 9.1] | 0.015 |
| Blumenfeld et al., 2020 [79] | 282 140: BT−A 142: topiramate 50−100 mg | 32 weeks | Mean decrease in the HIT−6 score compared to the baseline | − | − | –4.25 [95% CI: –5.77, –2.73] | <0.001 |
| Mean total score of the PHQ−9 | − | − | –1.86 [95% CI: –2.63, –1.10]; | <0.001 |
| Study | Number of Patients | Length | Efficacy | Baseline | Last Time-Point | p-Value |
|---|---|---|---|---|---|---|
| Khalil et al., 2014 [80] | 254 | Variable | Headache days per month | 27 (22,30) | 18 (10,25) | <0.001 |
| Migraine days per month | 15 (10,19) | 7 (3,12) | <0.001 | |||
| Crystal clear days per month | 3 (0,8) | 12 (5,20) | <0.001 | |||
| Mild headache days per month | 10 (7,15) | 8 (4,13) | <0.001 | |||
| Days with painkillers per month | 12 (7,20) | 6 (2,12) | <0.001 | |||
| Days with triptans per month | 5 (0,8) | 2 (0,6) | <0.001 | |||
| Days off work per month | 4 (3,6) | 1 (0,4) | <0.001 | |||
| Pedraza et al., 2015 [81] | 52 | 12 weeks | Headache days per month | 23.4 ± 6.3 | 12.8 ± 9.6 | <0.001 |
| Migraine days per month | 13.9 ± 7.3 | 5.3 ± 5.5 | <0.001 | |||
| Days with painkillers per month | 17.7 ± 9.2 | 8.7 ± 8 | <0.001 | |||
| Days with triptans per month | 5.1 ± 6.9 | 2.1 ± 3.6 | <0.001 | |||
| Ahmed et al., 2015 [82] | 215 without medication overuse | 12 weeks | Headache days per month | 26 (20,30) | 17 (11,28) | <0.001 |
| Migraine days per month | 14 (10,20) | 8 (4,12) | <0.001 | |||
| Crystal clear days per month | 4 (0,10) | 13 (3,19) | <0.001 | |||
| Days with painkillers per month | 8 (2,10) | 4 (0,8) | <0.001 | |||
| Days with triptans per month | 2 (0,5) | 0 (0,4) | <0.001 | |||
| Days off work per month | 3 (3,5) | 1 (0,3) | <0.001 | |||
| 215 without medication overuse | Headache days per month | 28 (24,30) | 20 (12,26) | <0.001 | ||
| Migraine days per month | 16 (12,20) | 9 (5,15) | <0.001 | |||
| Crystal clear days per month | 2 (0,6) | 10 (4,18) | <0.001 | |||
| Days with painkillers per month | 20 (16,28) | 10 (5,18) | <0.001 | |||
| Days with triptans per month | 6 (3,12) | 2 (0,7) | <0.001 | |||
| Days off work per month | 4 (2,8) | 2 (0,4) | <0.001 | |||
| Cernuda-Morollon et al., 2015 [83] | 132 | 12 months | Responders | 74.2% | ||
| Maasumi et al., 2015 [84] | 359 | 6 months | Patients with a ≥6 points decrease in the HIT-6 score | 108 (30.1%) | ||
| Negro et al., 2015 [85] | 132 | 24 months | Headache days per month | 22.3 ± 4.1 | 7.3 ± 2.1 | <0.001 |
| Migraine days per month | 21.4 ± 4.3 | 6.8 ± 2.3 | <0.001 | |||
| Days with painkillers per month | 20.8 ± 4.5 | 5.3 ± 1.7 | <0.001 | |||
| HIT-6 score | 69.4 ± 4.9 | 52 ± 5.6 | <0.001 | |||
| Patients with severe (≥60) HIT-6 score | 93.9% | 22% | <0.0001 | |||
| Guerzoni et al. 2015 [86] | 57 | 24 months | Headache index | 0.98 ± 0.09 | 0.65 ± 0.36 | <0.0001 |
| Analgesic consumption | 1.79 ± 1.59 | 0.61 ± 0.42 | <0.0001 | |||
| Visual analogue scale for pain (VAS) score | 7.98 ± 1.26 | 4.25 ± 1.48 | <0.001 | |||
| HIT-6 score | 63.94 ± 6.91 | 52.28 ± 8.69 | <0.001 | |||
| Vikelis et al., 2016 [87] | 119 | 9 months | Headache days per month | 21.3 ± 5.4 | 7.7 ± 4.8 | <0.001 |
| Peak headache days per month | 11.9 ± 5.5 | 3.7 ± 3.3 | <0.001 | |||
| Days with a VAS > 4 per month | 4–30 | 0–18 | <0.001 | |||
| Days with any acute headache medication per month | 16.2 ± 7.8 | 5.2 ± 4.3 | <0.001 | |||
| Aicua-Rapun et al., 2016 [88] | 115 | 12 weeks | Patients remitting from CM to episodic migraine | 68.7% | - | - |
| Patients stopping other preventive treatments for migraine | 42.5% | - | - | |||
| Patients discontinuing MOH | 61.9% | - | - | |||
| Russo et al., 2016 [89] | 52 | 6 months | Headache days per month | 20 (15,30) | 18 (10,30) | 0.002 |
| Days with painkillers per month | 17.5 (15,28.8) | 15 (9.3,28) | 0.016 | |||
| Painkillers per month | 20 (15,41.8) | 15 (7,31) | 0.014 | |||
| 9 months | Headache days | 19 (15,26.3) | 14.5 (10,25.8) | 0.011 | ||
| Days with painkillers per month | 15 (15,25) | 9 (5.5,17.5) | 0.015 | |||
| Painkillers per month | 20 (15,41.3) | 12 (7.5,24) | 0.005 | |||
| Demiryurek et al., 2015 [90] | 124 | 4 weeks | Headache days per month | 18.78 ± 2.06 | 5.80 ± 4.17 | |
| Admissions to the emergency department | 2.72 ± 1.28 | 0.47 ± 0.89 | <0.001 | |||
| Painkillers per month | 2.35 ± 0.88 | 0.67 ± 0.57 | <0.001 | |||
| VAS score | 8.90 ± 0.75 | 3.80 ± 2.17 | <0.001 | |||
| Duration of attacks | 2.63 ± 0.66 | 0.96 ± 0.66 | <0.001 | |||
| Frequency of attacks | 5.05 ± 1.20 | 1.55 ± 1.48 | <0.001 | |||
| 12 weeks | Headache days per month | 18.78 ± 2.06 | 12.38 ± 3.98 | <0.001 | ||
| Admissions to the emergency department | 2.72 ± 1.28 | 1.27 ± 1.06 | <0.001 | |||
| Painkillers per month | 2.35 ± 0.88 | 1.18 ± 0.56 | <0.001 | |||
| VAS score | 8.90 ± 0.75 | 6.53 ± 1.44 | <0.001 | |||
| Duration of attacks | 2.63 ± 0.66 | 1.90 ± 0.68 | <0.001 | |||
| Frequency of attacks | 5.05 ± 1.20 | 3.37 ± 1.38 | <0.001 | |||
| MIDAS score | 17.40 ± 4.92 | 8.22 ± 5.29 | <0.001 | |||
| Negro et al., 2015 [91] | 172 | 24 months | Headache days per month | 22.2 ± 4.9 | 4.1 ± 1.0 | <0.05 |
| Migraine days per month | 21.6 ± 4.8 | 3.8 ± 1.0 | <0.05 | |||
| Painkillers per month | 21.0 ± 5.1 | 3.7 ± 1.3 | <0.05 | |||
| HIT-6 score | 67.9 ± 4.2 | 49 ± 6.7 | <0.05 | |||
| Aydinlar et al., 2017 [92] | 190 | 12 months | Headache days | 15.0 (12.0–25.0) | 5.0 (2.0–10.0) | 0.017 |
| VAS score | 8.0 (7.0–9.0) | 7.0(5.0–7.0) | 0.023 | |||
| Painkillers per month | 20.0 (15.0–30.0) | 5.5(2.0–10.0) | <0.001 | |||
| MIDAS score | 57.0 (35.5–75.0) | 10.0(2.0–15.0) | 0.002 | |||
| DASS-21 depression | 85 | 7 | 0.002 | |||
| DASS-21 anxiety | 85 | 7 | 0.002 | |||
| DASS-21 stress | 85 | 7 | 0.002 | |||
| PSIQ | 9.0 (5.0–12.0) | 4.0 (1.0–7.0) | 0.002 | |||
| Matharu et al., 2017 [93] | 1160 | 15 months | ||||
| Byun J et al., 2017 [94] | 100 | 4 weeks | Good responders | 12.6% | - | - |
| Guerzoni et al., 2017 [95] | 90 | 36 months | Headache days per month | 0.98 ± 0.16 | 0.49 ± 0.29 | <0.001 |
| VAS score | 7.66 ± 1.56 | 3.31 ± 1.25 | <0.001 | |||
| Painkillers per month | 1.98 ± 1.69 | 0.49 ± 0.29 | <0.001 | |||
| HIT-6 score | 65.1 ± 6.24 | 57.15 ± 5.7 | <0.001 | |||
| Dikmen et al., 2018 [96] | 144 | 3 months | Headache days per month | 18.80 ± 5.53 | 5.77 ± 5.06 | 0.001 |
| MIDAS-score | 53.62 ± 24.84 | 16.17 ± 16.91 | 0.001 | |||
| Blumenfeld et al., 2018 [97] | 716 | 108 weeks | Headache days per month | 22.0 [4.8] | 11.3 ± 7.4 | <0.0001 |
| Patients with a ≥50% reduction in headache days | - | 61.1% | - | |||
| Dominguez et al., 2018 [98] | 725 | 12 months | Headache days per month | 21.8 ± 6.4 | 8.4 ± 5.7 | <0.01 |
| Migraine days per month | 13.8 ± 7.0 | 6.0 ± 4.7 | <0.01 | |||
| Painkillers per month | 17.0 ± 9.9 | 6.3 ± 8.3 | <0.01 | |||
| Triptans per month | 9.3 ± 8.7 | 4.8 ± 4.0 | <0.01 | |||
| Admissions to the ED for headache | 2.2 ± 2.6 | 0.9 ± 1.8 | <0.01 | |||
| VAS score | 7.6 ± 1.1 | 4.6 ± 2.1 | <0.01 | |||
| MIDAS score | 35.9 ± 29.6 | 9.1 ± 6.6 | <0.01 | |||
| Responders | - | 79.3% | - | |||
| Vikelis et al., 2018 [99] | 56 | 36 months | Headache days per month | 21.5 ± 5.1 | 3.4 ± 1.7 | <0.001 |
| Days with moderate/severe headache per month | 11.7 ± 5.7 | 2.5 ± 1.1 | 0.052 | |||
| Days with painkiller per month | 16.5 ± 7.3 | 2.8 ± 1.3 | <0.001 | |||
| Blumenfeld et al., 2018 [100] | 715 | 108 weeks | Headache days per month | −10.6 ± 7.4 | <0.001 | |
| Change in the PHQ-9 scores | −4.5 | <0.001 | ||||
| Change in the GAD-7 scores | −2.8 | <0.001 | ||||
| Andreou et al., 2018 [101] | 200 | 108 weeks | Headache days per month | 23 (17,30) | 8 (5,11.3) | <0.001 |
| Migraine days per month | 13 (9,18) | 4 (0,8) | <0.001 | |||
| Days with painkillers | 10 (4,16) | 3 (3.3,18.8) | <0.001 | |||
| Headache-free days per month | 0 (0,5) | 20.3 (10.7,22) | <0.001 | |||
| HIT-6 score | 70 (66,72) | 62 (56.5,66) | <0.001 | |||
| Caronna et al., 2018 [102] | 139 | 12 weeks | Headache frequency per month | 27.3 ± 4.7 | 15.4 ± 9.9 | <0.001 |
| Patients with daily headache | 71.2% | 23.2% | <0.001 | |||
| Migraine days per month | 13.4 ± 8.1 | 6.5 ± 5.7 | <0.001 | |||
| Headache days per month | 13.8 ± 9.0 | 8.9 ± 8.1 | <0.001 | |||
| Patients with daily painkiller intake | 66.2% | 13.7% | <0.001 | |||
| Ahmed et al., 2019 [103] | 633 | 21 months | Change of the headache days per month | −13.1 | <0.001 | |
| Change of the MSQ restrictive | 33.6 | <0.001 | ||||
| Change of the MSQ preventive | 28.9 | <0.001 | ||||
| Change of the MSQ emotional | 34.9 | <0.001 | ||||
| Change of the EQ-5D score | 0.2 | <0.001 | ||||
| Quitas et al., 2019 [104] | 193 | 24 weeks | Patients displaying a wear-off phenomenon | - | 23.3% | - |
| Ching et al., 2019 [105] | 131 | 24 weeks | Patients referring a worsening after BT-A stoppage | - | 20% | - |
| Alpuente et al., 2019 [106] | 105 | 108 weeks | Headache days per month | 13.6 ± 8.2 | 8.5 ± 8.3 | <0.001 |
| Migraine days per month | 11.0 ± 6.5 | 5.2 ± 4.7 | <0.001 | |||
| Headache frequency | 24.4 ± 7.1 | 13.9 ± 10.0 | <0.001 | |||
| MIDAS score | 84.1 ± 79.7 | 54.1 ± 53.9 | <0.001 | |||
| Oral preventive drugs | 2.3 ± 1.1 | 1.3 ± 0.9 | <0.001 | |||
| Santoro et al., 2020 [108] | 109 | 208 weeks | Headache days per month | 25.5 ± 5.8 | 6.3 ± 3.3 | <0.001 |
| Migraine hours per month | 538.6 ± 176.1 | 36.4 ± 29.0 | <0.001 | |||
| Stark et al., 2019 [109] | 211 | 24 weeks | Patients with a ≥50% response | 74% (68–80%) | ||
| Reduction in the migraine days per month | − 9.4 ± 7.6 | |||||
| Reduction in the HIT-6 score | − 11.8 (12.2) | |||||
| Ornello et al., 2020 [112] | 115 | 60 weeks | Headache days | 30 (25–30) | 15 (7–25) | <0.001 |
| Migraine days | 30 (25–30) | 15 (7–25) | <0.001 | |||
| NRS score | 8 (7–9) | 5 (4–7) | <0.001 | |||
| HIT-6 score | 65 (60–69) | 62 (56–65) | <0.001 | |||
| MIDAS score | 87.5 (42.5–123.5) | 12 (3.5–51.5) | 0.001 | |||
| Barad et al., 2019 [114] | 402 | 36 weeks | Percentage of patients reporting a reduced headache frequency | 62% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baraldi, C.; Lo Castro, F.; Ornello, R.; Sacco, S.; Pani, L.; Guerzoni, S. OnabotulinumtoxinA: Still the Present for Chronic Migraine. Toxins 2023, 15, 59. https://doi.org/10.3390/toxins15010059
Baraldi C, Lo Castro F, Ornello R, Sacco S, Pani L, Guerzoni S. OnabotulinumtoxinA: Still the Present for Chronic Migraine. Toxins. 2023; 15(1):59. https://doi.org/10.3390/toxins15010059
Chicago/Turabian StyleBaraldi, Carlo, Flavia Lo Castro, Raffaele Ornello, Simona Sacco, Luca Pani, and Simona Guerzoni. 2023. "OnabotulinumtoxinA: Still the Present for Chronic Migraine" Toxins 15, no. 1: 59. https://doi.org/10.3390/toxins15010059
APA StyleBaraldi, C., Lo Castro, F., Ornello, R., Sacco, S., Pani, L., & Guerzoni, S. (2023). OnabotulinumtoxinA: Still the Present for Chronic Migraine. Toxins, 15(1), 59. https://doi.org/10.3390/toxins15010059