Pain Reduction in Cervical Dystonia Following Treatment with IncobotulinumtoxinA: A Pooled Analysis

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Results
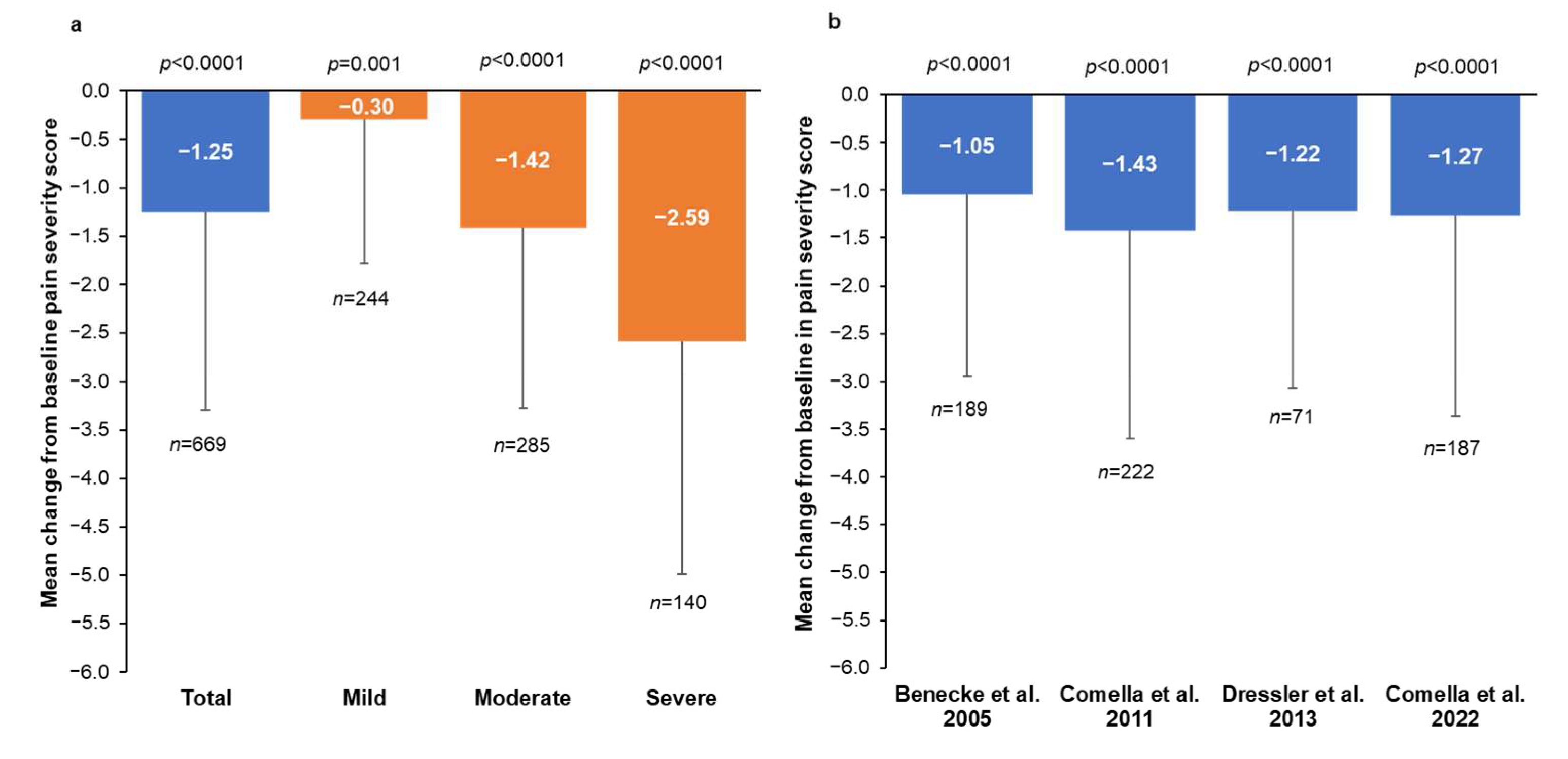
2.1. Change in Pain Severity from Baseline to Week 4
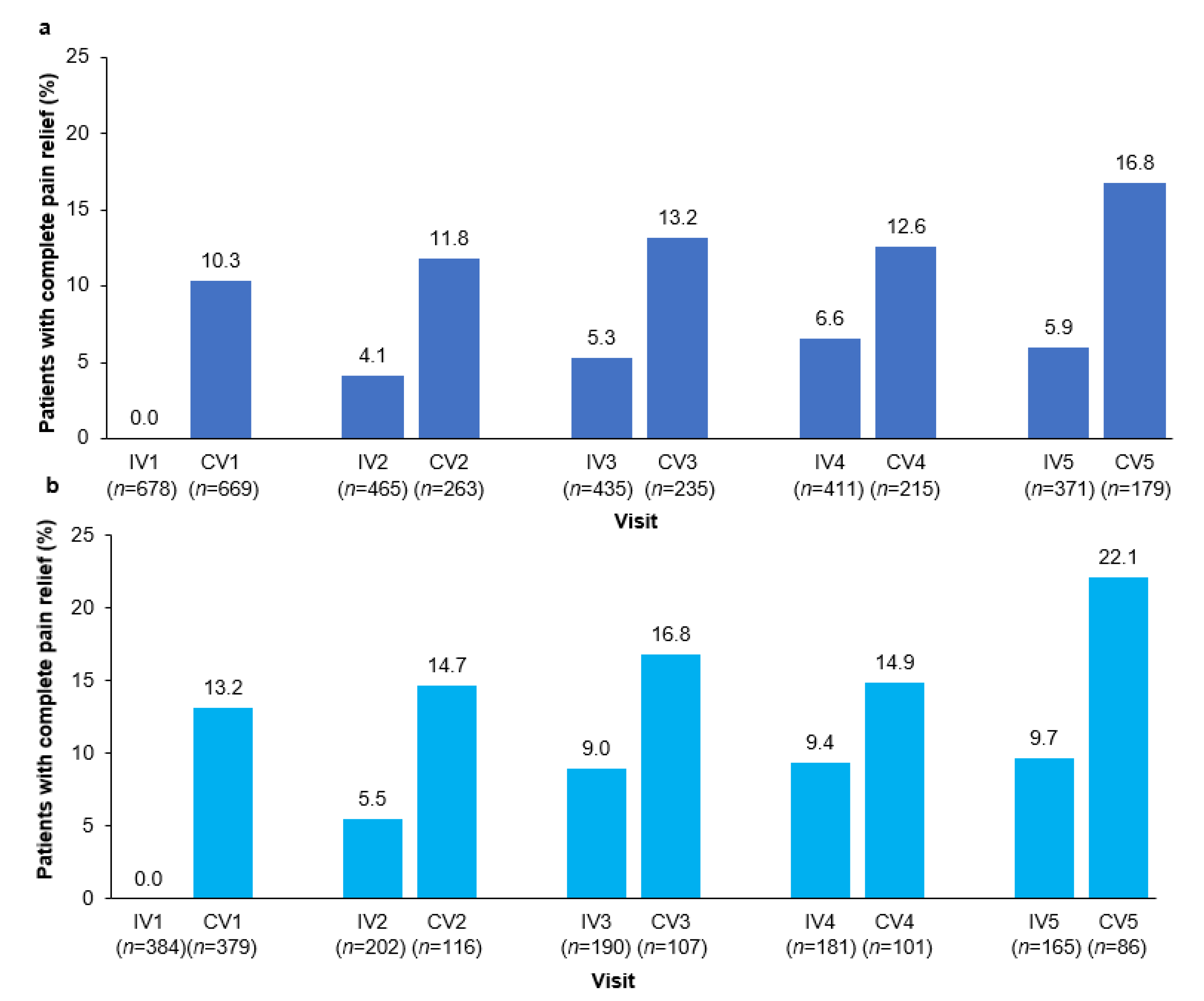
2.2. Pain Severity, Response Rates, and Complete Pain Relief Following Multiple Injection Cycles
2.3. Pain Severity Responses in Patients Not Taking Concomitant Pain Medication
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Studies Included in the Pooled Analysis
5.2. Analyses
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Albanese, A.; Kailash, K.P.; Cardoso, F.; Comella, C.; Defazio, G.; Fung, V.S.C.; Hallett, M.; Jankovic, J.; Jinnah, H.A.; Kaji, R.; et al. Isolated cervical dystonia: Diagnosis and classification. Mov. Disord. 2023, in press. [Google Scholar] [CrossRef] [PubMed]
- Medina, A.; Nilles, C.; Martino, D.; Pelletier, C.; Pringsheim, T. The prevalence of idiopathic or inherited isolated dystonia: A systematic review and meta-analysis. Mov. Disord. Clin. Pract. 2022, 9, 860–868. [Google Scholar] [CrossRef] [PubMed]
- Comella, C.; Bhatia, K. An international survey of patients with cervical dystonia. J. Neurol. 2015, 262, 837–848. [Google Scholar] [CrossRef] [PubMed]
- Girach, A.; Vinagre Aragon, A.; Zis, P. Quality of life in idiopathic dystonia: A systematic review. J. Neurol. 2019, 266, 2897–2906. [Google Scholar] [CrossRef]
- Charles, P.D.; Adler, C.H.; Stacy, M.; Comella, C.; Jankovic, J.; Manack Adams, A.; Schwartz, M.; Brin, M.F. Cervical dystonia and pain: Characteristics and treatment patterns from CD PROBE (Cervical Dystonia Patient Registry for Observation of OnabotulinumtoxinA Efficacy). J. Neurol. 2014, 261, 1309–1319. [Google Scholar] [CrossRef] [PubMed]
- Camargo, C.H.; Cattai, L.; Teive, H.A. Pain Relief in Cervical Dystonia with Botulinum Toxin Treatment. Toxins 2015, 7, 2321–2335. [Google Scholar] [CrossRef]
- Marciniec, M.; Szczepańska-Szerej, A.; Kulczyński, M.; Sapko, K.; Popek-Marciniec, S.; Rejdak, K. Pain in cervical dystonia and the antinociceptive effects of botulinum toxin: What is currently known? Rev. Neurosci. 2019, 30, 771–779. [Google Scholar] [CrossRef]
- Marciniec, M.; Szczepańska-Szerej, A.; Papuć, E.; Rejdak, K. Targeting pain in the long-term treatment of cervical dystonia with botulinum toxin A. Int. J. Neurosci. 2022, 132, 1026–1030. [Google Scholar] [CrossRef]
- Rosales, R.L.; Cuffe, L.; Regnault, B.; Trosch, R.M. Pain in cervical dystonia: Mechanisms, assessment and treatment. Expert Rev. Neurother. 2021, 21, 1125–1134. [Google Scholar] [CrossRef]
- Erbguth, F.J. Pain in cervical dystonia. In Botulinum Toxin in Painful Diseases. Pain Headache; Jost, W.H., Ed.; Karger: Basel, Switzerland, 2003; Volume 14, pp. 54–70. [Google Scholar]
- Van den Dool, J.; Tijssen, M.A.; Koelman, J.H.; Engelbert, R.H.; Visser, B. Determinants of disability in cervical dystonia. Park. Relat. Disord. 2016, 32, 48–53. [Google Scholar] [CrossRef]
- Avenali, M.; De Icco, R.; Tinazzi, M.; Defazio, G.; Tronconi, L.; Sandrini, G.; Tassorelli, C. Pain in focal dystonias—A focused review to address an important component of the disease. Park. Relat. Disord. 2018, 54, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Albanese, A.; Asmus, F.; Bhatia, K.P.; Elia, A.E.; Elibol, B.; Filippini, G.; Gasser, T.; Krauss, J.K.; Nardocci, N.; Newton, A.; et al. EFNS guidelines on diagnosis and treatment of primary dystonias. Eur. J. Neurol. 2011, 18, 5–18. [Google Scholar] [CrossRef]
- Albanese, A.; Abbruzzese, G.; Dressler, D.; Duzynski, W.; Khatkova, S.; Marti, M.J.; Mir, P.; Montecucco, C.; Moro, E.; Pinter, M.; et al. Practical guidance for CD management involving treatment of botulinum toxin: A consensus statement. J. Neurol. 2015, 262, 2201–2213. [Google Scholar] [CrossRef] [PubMed]
- Contarino, M.F.; Van Den Dool, J.; Balash, Y.; Bhatia, K.; Giladi, N.; Koelman, J.H.; Lokkegaard, A.; Marti, M.J.; Postma, M.; Relja, M.; et al. Clinical practice: Evidence-based recommendations for the treatment of cervical dystonia with botulinum toxin. Front. Neurol. 2017, 8, 35. [Google Scholar] [CrossRef] [PubMed]
- Simpson, D.M.; Hallett, M.; Ashman, E.J.; Comella, C.L.; Green, M.W.; Gronseth, G.S.; Armstrong, M.J.; Gloss, D.; Potrebic, S.; Jankovic, J.; et al. Practice guideline update summary: Botulinum neurotoxin for the treatment of blepharospasm, cervical dystonia, adult spasticity, and headache: Report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology 2016, 86, 1818–1826. [Google Scholar] [CrossRef] [PubMed]
- Spiegel, L.L.; Ostrem, J.L.; Bledsoe, I.O. FDA Approvals and Consensus Guidelines for Botulinum Toxins in the Treatment of Dystonia. Toxins 2020, 12, 332. [Google Scholar] [CrossRef] [PubMed]
- Dressler, D.; Adib Saberi, F.; Rosales, R.L. Botulinum toxin therapy of dystonia. J. Neural. Transm. 2021, 128, 531–537. [Google Scholar] [CrossRef]
- Benecke, R.; Jost, W.H.; Kanovsky, P.; Ruzicka, E.; Comes, G.; Grafe, S. A new botulinum toxin type A free of complexing proteins for treatment of cervical dystonia. Neurology 2005, 64, 1949–1951. [Google Scholar] [CrossRef]
- Comella, C.L.; Jankovic, J.; Truong, D.D.; Hanschmann, A.; Grafe, S.; U.S. XEOMIN Cervical Dystonia Study Group. Efficacy and safety of incobotulinumtoxinA (NT 201, XEOMIN®, botulinum neurotoxin type A, without accessory proteins) in patients with cervical dystonia. J. Neurol. Sci. 2011, 308, 103–109. [Google Scholar] [CrossRef]
- Evidente, V.G.; Fernandez, H.H.; LeDoux, M.S.; Brashear, A.; Grafe, S.; Hanschmann, A.; Comella, C.L. A randomized, double-blind study of repeated incobotulinumtoxinA (Xeomin(®)) in cervical dystonia. J. Neural. Transm. 2013, 120, 1699–1707. [Google Scholar] [CrossRef]
- Fernandez, H.H.; Pappert, E.J.; Comella, C.L.; Evidente, V.G.; Truong, D.D.; Verma, A.; Jankovic, J. Efficacy and safety of incobotulinumtoxinA in subjects previously treated with botulinum toxin versus toxin-naïve subjects with cervical dystonia. Tremor. Other Hyperkinet. Mov. 2013, 3, tre-03-140-2921-1. [Google Scholar] [CrossRef]
- Rodrigues, F.B.; Duarte, G.S.; Marques, R.E.; Castelão, M.; Ferreira, J.; Sampaio, C.; Moore, A.P.; Costa, J. Botulinum toxin type A therapy for cervical dystonia. Cochrane Database Syst. Rev. 2020, 11, CD003633. [Google Scholar] [CrossRef] [PubMed]
- Charles, P.D.; Manack Adams, A.; Davis, T.; Bradley, K.; Schwartz, M.; Brin, M.F.; Patel, A.T. Neck pain and cervical dystonia: Treatment outcomes from CD PROBE (Cervical Dystonia Patient Registry for Observation of OnabotulinumtoxinA Efficacy). Pain Pract. 2016, 16, 1073–1082. [Google Scholar] [CrossRef] [PubMed]
- Trosch, R.M.; Espay, A.J.; Truong, D.; Gil, R.; Singer, C.; LeWitt, P.A.; Lew, M.F.; Tagliati, M.; Adler, C.H.; Chen, J.J.; et al. Multicenter observational study of abobotulinumtoxinA neurotoxin in cervical dystonia: The ANCHOR-CD registry. J. Neurol. Sci. 2017, 376, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Trosch, R.M.; Misra, V.P.; Maisonobe, P.; Om, S. Impact of abobotulinumtoxinA on the clinical features of cervical dystonia in routine practice. Clin. Park Relat. Disord. 2020, 3, 100063. [Google Scholar] [CrossRef] [PubMed]
- Dressler, D.; Paus, S.; Seitzinger, A.; Gebhardt, B.; Kupsch, A. Long-term efficacy and safety of incobotulinumtoxinA injections in patients with cervical dystonia. J. Neurol. Neurosurg. Psychiatry 2013, 84, 1014–1019. [Google Scholar] [CrossRef]
- Comella, C.; Hauser, R.A.; Isaacson, S.H.; Truong, D.; Oguh, O.; Hui, J.; Molho, E.S.; Brodsky, M.; Furr-Stimming, E.; Comes, G.; et al. Efficacy and safety of two incobotulinumtoxinA injection intervals in cervical dystonia patients with inadequate benefit from standard injection intervals of botulinum toxin: Phase 4, open-label, randomized, noninferiority study. Clin. Park Relat. Disord. 2022, 6, 100142. [Google Scholar] [CrossRef]
- McCarberg, B.; Peppin, J. Pain pathways and nervous system plasticity: Learning and memory in pain. Pain Med. 2019, 20, 2421–2437. [Google Scholar] [CrossRef]
- Defazio, G.; Jankovic, J.; Giel, J.L.; Papapetropoulos, S. Descriptive epidemiology of cervical dystonia. Tremor. Other Hyperkinet. Mov. 2013, 3, tre-03-193-4374-2. [Google Scholar] [CrossRef]
- Dashtipour, K.; Mari, Z.; Jankovic, J.; Adler, C.H.; Schwartz, M.; Brin, M.F. Minimal clinically important change in patients with cervical dystonia: Results from the CD PROBE study. J. Neurol. Sci. 2019, 405, 116413. [Google Scholar] [CrossRef]
- Dworkin, R.H.; Turk, D.C.; Wyrwich, K.W.; Beaton, D.; Cleeland, C.S.; Farrar, J.T.; Haythornthwaite, J.A.; Jensen, M.P.; Kerns, R.D.; Ader, D.N.; et al. Interpreting the clinical importance of treatment outcomes in chronic pain clinical trials: IMMPACT recommendations. J. Pain 2008, 9, 105–121. [Google Scholar] [CrossRef] [PubMed]
- Truong, D.; Brodsky, M.; Lew, M.; Brashear, A.; Jankovic, J.; Molho, E.; Orlova, O.; Timerbaeva, S.; Global Dysport Cervical Dystonia Study Group. Long-term efficacy and safety of botulinum toxin type A (Dysport) in cervical dystonia. Park. Relat. Disord. 2010, 16, 316–323. [Google Scholar] [CrossRef] [PubMed]
- Colosimo, C.; Charles, D.; Misra, V.P.; Maisonobe, P.; Om, S.; INTEREST IN CD2 study group. Cumulative effects of long-term treatment with abobotulinumtoxinA in cervical dystonia: Findings from a prospective, observational study. J. Neurol. Sci. 2020, 416, 117015. [Google Scholar] [CrossRef] [PubMed]
- Charles, D.; Brashear, A.; Hauser, R.A.; Li, H.I.; Boo, L.M.; Brin, M.F.; CD 140 Study Group. Efficacy, tolerability, and immunogenicity of onabotulinumtoxinA in a randomized, double-blind, placebo-controlled trial for cervical dystonia. Clin. Neuropharmacol. 2012, 35, 208–214. [Google Scholar] [CrossRef]
- Jost, W.H.; Hefter, H.; Stenner, A.; Reichel, G. Rating scales for cervical dystonia: A critical evaluation of tools for outcome assessment of botulinum toxin therapy. J. Neural. Transm. 2013, 120, 487–496. [Google Scholar] [CrossRef]
- Costanzo, M.; Belvisi, D.; Berardelli, I.; Maraone, A.; Baione, V.; Ferrazzano, G.; Cutrona, C.; Leodori, G.; Pasquini, M.; Conte, A.; et al. Effect of botulinum toxin on non-motor symptoms in cervical dystonia. Toxins 2021, 13, 647. [Google Scholar] [CrossRef]
- Comella, C.; Ferreira, J.J.; Pain, E.; Azoulai, M.; Om, S. Patient perspectives on the therapeutic profile of botulinum neurotoxin type A in cervical dystonia. J. Neurol. 2021, 268, 903–912. [Google Scholar] [CrossRef]
- Pirio Richardson, S.; Jinnah, H.A. New approaches to discovering drugs that treat dystonia. Expert Opin. Drug Discov. 2019, 14, 893–900. [Google Scholar] [CrossRef]
- Jinnah, H.A.; Comella, C.L.; Perlmutter, J.; Lungu, C.; Hallett, M.; Dystonia Coalition Investigators. Longitudinal studies of botulinum toxin in cervical dystonia: Why do patients discontinue therapy? Toxicon 2018, 147, 89–95. [Google Scholar] [CrossRef]
- Müller, J.; Wissel, J.; Kemmler, G.; Voller, B.; Bodner, T.; Schneider, A.; Wenning, G.K.; Poewe, W. Craniocervical dystonia questionnaire (CDQ-24): Development and validation of a disease-specific quality of life instrument. J. Neurol. Neurosurg. Psychiatry 2004, 75, 749–753. [Google Scholar] [CrossRef]
- Hefter, H.; Benecke, R.; Erbguth, F.; Jost, W.; Reichel, G.; Wissel, J. An open-label cohort study of the improvement of quality of life and pain in de novo cervical dystonia patients after injections with 500 U botulinum toxin A (Dysport). BMJ Open 2013, 3, e001853. [Google Scholar] [CrossRef] [PubMed]
- Klingelhoefer, L.; Kaiser, M.; Sauerbier, A.; Untucht, R.; Wienecke, M.; Mammadova, K.; Falkenburger, B.; Gregor, O.; Chaudhuri, K.R.; Reichmann, H. Emotional well-being and pain could be a greater determinant of quality of life compared to motor severity in cervical dystonia. J. Neural. Transm. 2021, 128, 305–314. [Google Scholar] [CrossRef]
- De Pauw, J.; van der Velden, K.; Cox, R.; Truijen, S.; Cras, P.; Mercelis, R.; De Hertogh, W. Measuring disability in patients with cervical dystonia according to the International Classification of Functioning, Disability and Health. OTJR Occup. Particip. Health 2017, 37, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Marciniec, M.; Szczepańska-Szerej, A.; Rejdak, K. Cervical dystonia: Factors deteriorating patient satisfaction of long-term treatment with botulinum toxin. Neurol. Res. 2020, 42, 987–991. [Google Scholar] [CrossRef] [PubMed]
- Duane, D.D. Spasmodic torticollis: Clinical and biologic features and their implications for focal dystonia. Adv. Neurol. 1988, 50, 473–492. [Google Scholar]
- Kutvonen, O.; Dastidar, P.; Nurmikko, T. Pain in spasmodic torticollis. Pain 1997, 69, 279–286. [Google Scholar] [CrossRef]
- Consky, E.S.; Basinski, A.; Belle, L. The Toronto Western Spasmodic Torticollis Rating Scale (TWSTRS): Assessment of validity and inter-rater reliability. Neurology 1990, 40, 445. [Google Scholar]
- Consky, E.S.; Lang, A.E. Clinical assessment of patients with cervical dystonia. In Therapy with Botulinum Toxin; Jankovic, J., Hallet, M., Eds.; Marcel Dekker: New York, NY, USA, 1994; pp. 211–237. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Total (n = 678) | Pain Severity at Baseline a | ||
|---|---|---|---|---|
| Mild (n = 247) | Moderate (n = 291) | Severe (n = 140) | ||
| Age (years) | 53.6 ± 11.5 | 53.4 ± 11.8 | 53.7 ± 11.6 | 54.0 ± 10.8 |
| Female | 463 (68.3) | 152 (61.5) | 203 (69.8) | 108 (77.1) |
| Ethnicity | ||||
| White | 640 (94.4) | 242 (98.0) | 271 (93.1) | 127 (90.7) |
| Black or African American | 16 (2.4) | 2 (0.8) | 8 (2.8) | 6 (4.3) |
| Asian | 5 (0.7) | 0 | 3 (1.0) | 2 (1.4) |
| Other/missing | 17 (2.5) | 3 (1.2) | 9 (3.1) | 5 (3.5) |
| Height (cm) | 167.7 ± 9.0 | 168.2 ± 9.2 | 167.7 ± 8.9 | 166.5 ± 9.0 |
| Weight (kg) | 75.1 ± 16.2 | 75.3 ± 15.9 | 75.1 ± 15.9 | 74.9 ± 17.8 |
| Disease severity b | ||||
| Mild | 168 (24.8) | 81 (32.8) | 70 (24.1) | 17 (12.1) |
| Moderate | 365 (53.8) | 131 (53.0) | 162 (55.7) | 72 (51.4) |
| Severe | 145 (21.4) | 35 (14.2) | 59 (20.3) | 51 (36.4) |
| BoNT naïve | 123 (18.1) | 29 (11.7) | 57 (19.6) | 37 (26.4) |
| Years since CD diagnosis | 9.2 ± 7.9 | 9.2 ± 7.4 | 9.3 ± 8.0 | 9.0 ± 8.6 |
| Pain severity score | 4.26 ± 2.32 | 1.73 ± 1.06 | 4.91 ± 0.80 | 7.40 ± 0.83 |
| Study Name, NCT Number and Reference(s) | Phase | Study Design & Objectives | Patients & Indication | Treatments | Primary Efficacy Outcome Measure | Pain Measures |
|---|---|---|---|---|---|---|
| Benecke et al., 2005 [19] | 3 | Randomized, double-blind, active-controlled, parallel-group, multicenter, non-inferiority study in the EU to investigate the safety and efficacy of incoBoNT-A compared to onaBoNT-A in patients with CD. | n = 463 Adults with CD (predominantly of the rotational form; i.e., spasmodic torticollis) who had shown stable responses in at least two previous onaBoNT-A injection sessions prior to study entry. Last injection session at least 10 weeks prior to randomization. Baseline TWSTRS severity score ≥10. | One i.m. injection session of incoBoNT-A (n = 231) or onaBoNT-A (n = 232), 70–300 U at baseline visit (dose equivalent to last two injection sessions). | Change in CD severity using the TWSTRS severity score from baseline to control visit on day 28 ± 7 after injection of study medication. Total study duration: 16 weeks. | TWSTRS disability subscale score (range 0–5); pain VAS score (0–100 mm) |
| NCT00407030 Comella et al., 2011 [20] Evidente et al., 2013 [21] | 3 | Prospective, double-blind, placebo-controlled, randomized, multicenter study in the USA with a double-blind parallel-group extension period to investigate the efficacy and safety of different doses of incoBoNT-A in the treatment of CD. | n = 233 (main period); n = 217 (extension period) Adults with CD of predominantly rotational form (i.e., spasmodic torticollis). At least 40% BoNT-A-treatment naïve Pre-treated subjects had to be stable and have their last BoNT injection at least 10 weeks prior to study entry. Baseline TWSTRS total score ≥20, TWSTRS severity score ≥10, TWSTRS disability score ≥3, TWSTRS pain score ≥1. | Main period: One injection session of IncoBoNT-A (120 U or 240 U; fixed total dose) or placebo. Extension period: Up to 5 additional injection cycles of IncoBoNT-A (120 U or 240 U; fixed total dose). Interval between injection sessions: 6–20 weeks. | Change in TWSTRS total score from baseline to Week 4 (±3 days) after injection. Total study duration: 88 weeks. | TWSTRS pain score (range 0–20) |
| NCT00541905 Dressler et al., 2013 [27] | 4 | Prospective, open-label, single-arm, multicenter study in Germany to investigate the long-term efficacy and safety of incoBoNT-A in patients with CD. | n = 76 Adults with CD of predominantly rotational form (i.e., spasmodic torticollis). Baseline TWSTRS total score ≥25, TWSTRS severity score ≥10 and TWSTRS disability score ≥3 25% naïve to BoNT-A. Pre-treated patients had shown stable response and the most recent treatment was ≥10 weeks prior to first injection. | Main period: One injection session Flexible dosing: ≤300 U total dose; ≤50 U per injection site. Extension period: Four additional injection sessions. Interval between injection sessions: 10–24 weeks. | Change in TWSTRS total score from baseline to Week 4 after 1st injection. Total study duration: 51–121 weeks. | TWSTRS pain score (range 0–20) |
| NCT01486264 Comella et al., 2022 [28] | 4 | Prospective, open-label, randomized, multicenter, non-inferiority study in the USA (CD-FLEX) evaluating two dosing schedules of incoBoNT-A in patients with CD. | n = 282 Adults with CD who reported therapeutic benefit from previous BoNT treatment. All pre-treated with at least two successful BoNT injections; most recent treatment at least 12 weeks before enrolment. | Short Flex: injection interval 8 ± 2 weeks (n = 142) Long Flex: injection interval 14 ± 2 weeks (n = 140). Initial dose comparable to most recent BoNT dose (±10%) and to remain stable thereafter. Up to 11 injection cycles 10 visits. | Change in CD severity using the TWSTRS severity score from baseline to 4 weeks after 8th injection Overall mean duration was 452.4 days for the Short Flex group and 691.0 days for the Long Flex group. Mean duration of cycles was 55.1 days for the Short Flex group and 86.4 days for the Long Flex group (full analysis set). | TWSTRS pain score (range 0–20) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albanese, A.; Wissel, J.; Jost, W.H.; Castagna, A.; Althaus, M.; Comes, G.; Scheschonka, A.; Vacchelli, M.; Jinnah, H.A. Pain Reduction in Cervical Dystonia Following Treatment with IncobotulinumtoxinA: A Pooled Analysis. Toxins 2023, 15, 333. https://doi.org/10.3390/toxins15050333
Albanese A, Wissel J, Jost WH, Castagna A, Althaus M, Comes G, Scheschonka A, Vacchelli M, Jinnah HA. Pain Reduction in Cervical Dystonia Following Treatment with IncobotulinumtoxinA: A Pooled Analysis. Toxins. 2023; 15(5):333. https://doi.org/10.3390/toxins15050333
Chicago/Turabian StyleAlbanese, Alberto, Jörg Wissel, Wolfgang H. Jost, Anna Castagna, Michael Althaus, Georg Comes, Astrid Scheschonka, Matteo Vacchelli, and Hyder A. Jinnah. 2023. "Pain Reduction in Cervical Dystonia Following Treatment with IncobotulinumtoxinA: A Pooled Analysis" Toxins 15, no. 5: 333. https://doi.org/10.3390/toxins15050333