Scaffolds for Wound Healing Applications


Abstract
:1. Introduction
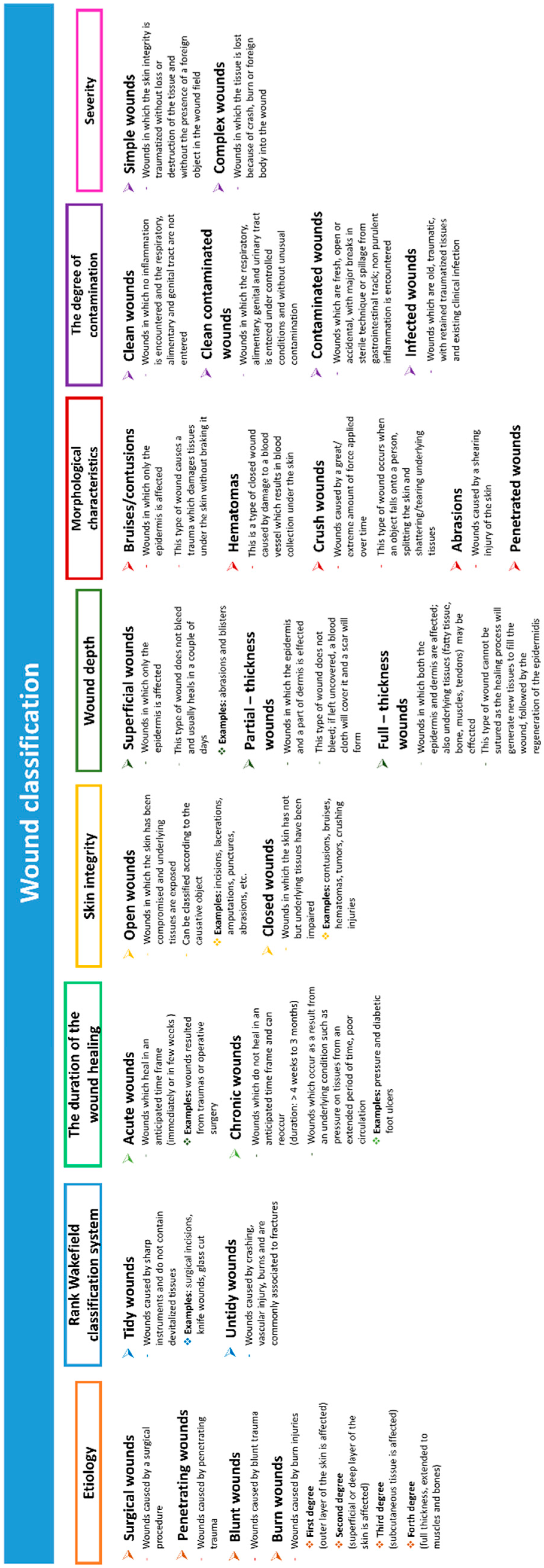
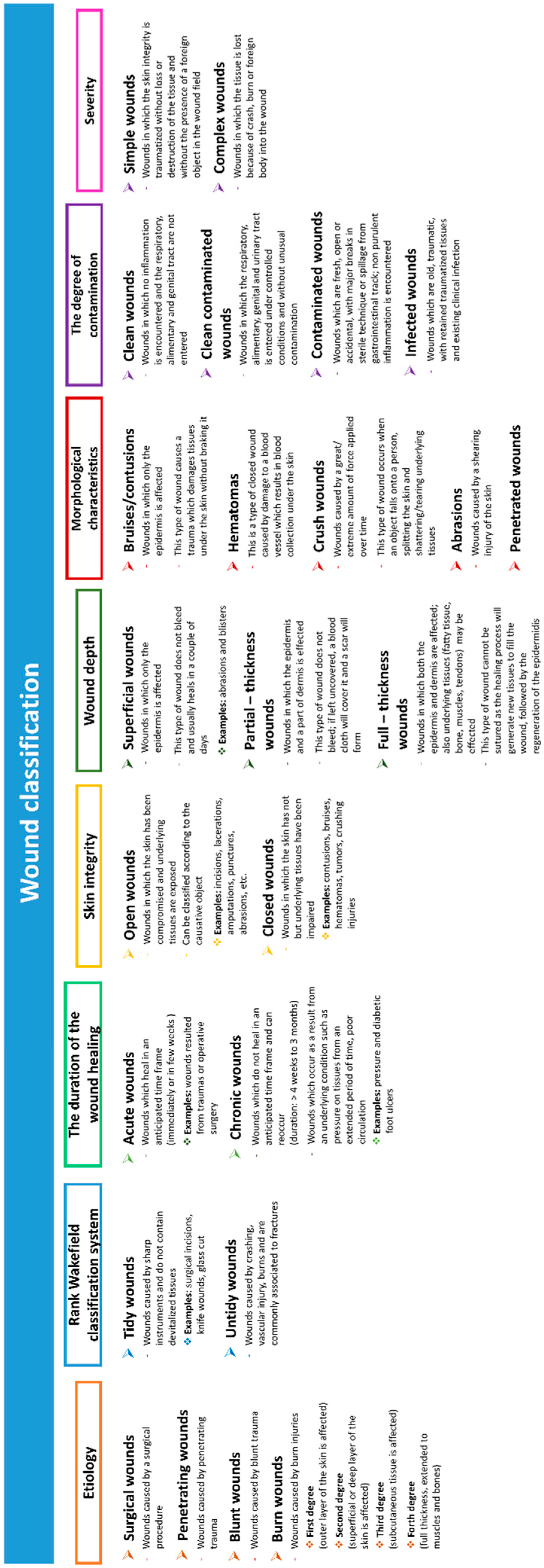
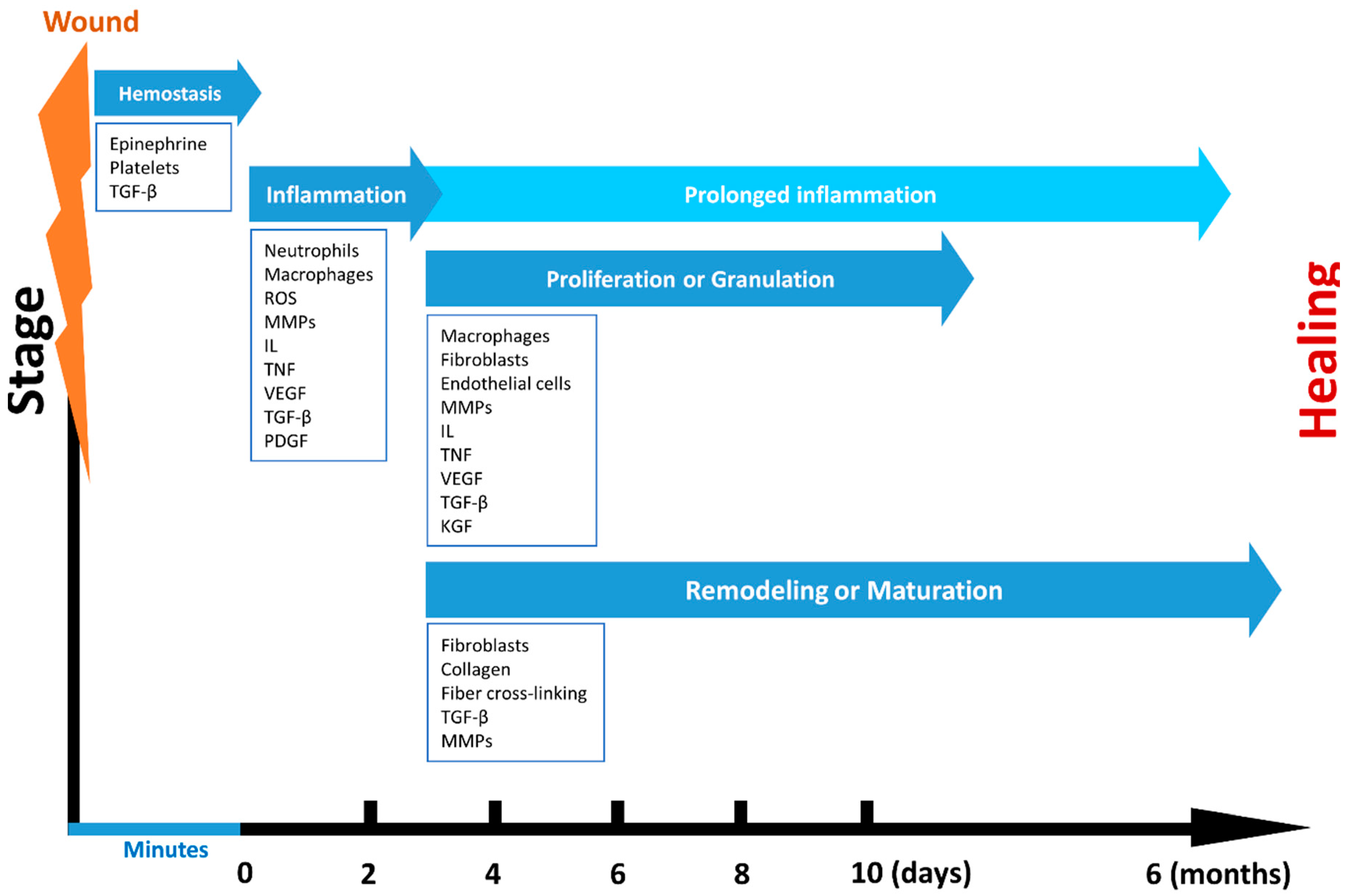
2. Wound Types and Wound Healing Processes
3. Wound Management
4. Current Polymeric Materials in Wound Healing
4.1. Natural Polymers
4.2. Synthetic Polymers
5. Engineered Scaffolds for Wound Healing
5.1. Physical and Mechanical Properties of Scaffolds for Wound Healing
5.2. Healing Properties
6. Conclusions and Future Prospects
Author Contributions
Funding
Conflicts of Interest
References
- Helary, C.; Abed, A.; Mosser, G.; Louedec, L.; Letourneur, D.; Coradin, T.; Giraud-Guille, M.M.; Meddahi-Pellé, A. Evaluation of dense collagen matrices as medicated wound dressing for the treatment of cutaneous chronic wounds. Biomater. Sci. 2015, 3, 373–382. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Cheng, F.; Liu, J.; Smått, J.H.; Gepperth, D.; Lastusaari, M.; Xu, C.; Hupa, L. Biocomposites of copper-containing mesoporous bioactive glass and nanofibrillated cellulose: Biocompatibility and angiogenic promotion in chronic wound healing application. Acta Biomater. 2016, 46, 286–298. [Google Scholar] [CrossRef] [PubMed]
- Karahaliloglu, Z.; Kilicay, E.; Denkbas, E.B. Antibacterial chitosan/silk sericin 3D porous scaffolds as a wound dressing material. Artif. Cell. Nanomed. Biotechnol. 2017, 45, 1172–1185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Radhakumary, C.; Antonty, M.; Sreenivasan, K. Drug loaded thermoresponsive and cytocompatible chitosan based hydrogel as a potential wound dressing. Carbohydr. Polym. 2011, 83, 705–713. [Google Scholar] [CrossRef]
- Zhong, S.P.; Zhang, Y.Z.; Lim, C.T. Tissue scaffolds for skin wound healing and dermal reconstruction. Wires. Nanomed. Nanobi. 2010, 2, 510–525. [Google Scholar] [CrossRef] [PubMed]
- Kampleitner, C.; Changi, K.; Felfel, R.M.; Scotchford, C.A.; Sottile, V.; Kluger, R.; Hoffmann, O.; Grant, D.M.; Epstein, M.M. Preclinical biological and physicochemical evaluation of two-photon engineered 3D biomimetic copolymer scaffolds for bone healing. Biomater. Sci. 2020, 8, 1683–1694. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Cheng, Y.; Chen, L.; Zhu, T.; Ye, K.; Jia, C.; Wang, H.; Zhu, M.; Fan, C.; Mo, X. In vitro and in vivo studies of electroactive reduced graphene oxide-modified nanofiber scaffolds for peripheral nerve regeneration. Acta Biomater. 2019, 84, 98–113. [Google Scholar] [CrossRef]
- Sensini, A.; Cristofolini, L.; Zucchelli, A.; Focarete, M.L.; Gualandi, C.; De Mori, A.; Kao, A.P.; Roldo, M.; Blunn, G.; Tozzi, G. Hierarchical electrospun tendon-ligament bioinspired scaffolds induce changes in fibroblasts morphology under static and dynamic conditions. J. Microsc. 2020, 277, 160–169. [Google Scholar] [CrossRef]
- Jafari, M.; Paknejad, Z.; Rad, M.R.; Motamedian, S.R.; Eghbal, M.J.; Nadjmi, N.; Khojasteh, A. Polymeric scaffolds in tissue engineering: A literature review. J. Biomed. Mater. Res. Part B 2017, 105, 431–459. [Google Scholar] [CrossRef]
- Zhang, J.; Song, C.; Han, Y.; Xi, Z.; Zhao, L.; Cen, L.; Yang, Y. Regulation of inflammatory response to polyglycolic acid scaffolds through incorporation of sodium tripolyphosphate. Eur. Polym. J. 2020, 122, 109349. [Google Scholar] [CrossRef]
- Rubio-Elizalde, I.; Bernáldez-Sarabia, J.; Moreno-Ulloa, A.; Vilanova, C.; Juárez, P.; Licea-Navarro, A.; Castro-Ceseña, A.B. Scaffolds based on alginate-PEG methyl ether methacrylate-Moringa oleifera-Aloe vera for wound healing applications. Carbohydr. Polym. 2019, 206, 455–467. [Google Scholar] [CrossRef] [PubMed]
- Joseph, B.; Augustine, R.; Kalarikkal, N.; Thomas, S.; Seantier, B.; Grohens, Y. Recent advances in electrospun polycaprolactone based scaffolds for wound healing and skin bioengineering applications. Mater. Today Commun. 2019, 19, 319–335. [Google Scholar] [CrossRef]
- Lee, C.H.; Hung, K.C.; Hsieh, M.J.; Chang, S.H.; Juang, J.H.; Hsieh, I.C.; Wen, M.S.; Liu, S.J. Core-shell insulin-loaded nanofibrous scaffolds for repairing diabetic wounds. Nanomed. Nanotechnol. Biol. Med. 2020, 24, 102123. [Google Scholar] [CrossRef] [PubMed]
- Ramalingam, R.; Chetna, D.; Leung, C.M.; Ezhilarasu, H.; Prasannan, P.; Ong, S.T.; Subramanian, S.; Kamruddin, M.; Lakshminarayanan, R.; Ramakrishna, S.; et al. Poly-ε-Caprolactone/Gelatin Hybrid Electrospun Composite Nanofibrous Mats Containing Ultrasound Assisted Herbal Extract: Antimicrobial and Cell Proliferation Study. Nanomaterials 2019, 9, 462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Talikowska, M.; Fu, X.; Lisak, G. Application of conducting polymers to wound care and skin tissue engineering: A review. Biosens. Bioelectron. 2019, 135, 50–63. [Google Scholar] [CrossRef]
- Boer, M.; Duchnik, E.; Maleszka, R.; Marchlewicz, M. Structural and biophysical characteristics of human skin in maintaining proper epidermal barrier function. Postep. Dermatol. Alergol. 2016, 33, 1–5. [Google Scholar] [CrossRef]
- Portela, R.; Leal, C.R.; Almeida, P.L.; Sobral, R.G. Bacterial cellulose: A versatile biopolymer for wound dressing applications. Microb. Biotechnol. 2019, 12, 586–610. [Google Scholar] [CrossRef]
- Boateng, J.S.; Matthews, K.H.; Stevens, H.N.E.; Eccleston, G.M. Wound Healing Dressings and Drug Delivery Systems: A Review. J. Pharm. Sci. 2008, 97, 2892–2923. [Google Scholar] [CrossRef]
- Velnar, T.; Bailey, T.; Smrkolj, V. The Wound Healing Process: An Overview of the Cellular and Molecular Mechanisms. J. Int. Med. Res. 2009, 37, 1528–1542. [Google Scholar] [CrossRef]
- Enoch, S.; Leaper, D.J. Basic science of wound healing. Surgery (Oxford) 2005, 23, 37–42. [Google Scholar] [CrossRef]
- Rowan, M.P.; Cancio, L.C.; Elster, E.A.; Burmeister, D.M.; Rose, L.F.; Natesan, S.; Chan, R.K.; Christy, R.J.; Chung, K.K. Burn wound healing and treatment: Review and advancements. Crit. Care 2015, 19, 243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Etulain, J. Platelets in wound healing and regenerative medicine. Platelets 2018, 29, 556–568. [Google Scholar] [CrossRef] [PubMed]
- Wilgus, T.A.; Roy, S.; McDaniel, J.C. Neutrophils and wound repair: Positive actions and negative reactions. Adv. Wound Care 2013, 2, 379–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kondo, T.; Ishida, Y. Molecular pathology of wound healing. Forensic Sci. Int. 2010, 203, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Darby, I.A.; Laverdet, B.; Bonté, F.; Desmoulière, A. Fibroblasts and myofibroblasts in wound healing. Clin. Cosmet. Investig. Dermatol. 2014, 7, 301–311. [Google Scholar] [CrossRef] [Green Version]
- Bao, P.; Kodra, A.; Tomic-Canic, M.; Golinko, M.S.; Ehrlich, H.P.; Brem, H. The role of vascular endothelial growth factor in wound healing. J. Surg. Res. 2009, 153, 347–358. [Google Scholar] [CrossRef] [Green Version]
- Werner, S. A Novel Enhancer of the Wound Healing Process. Am. J. Pathol. 2011, 179, 2144–2147. [Google Scholar] [CrossRef]
- Staiano-Coico, L.; Krueger, J.G.; Rubin, J.S.; D’limi, S.; Vallat, V.P.; Valentino, L.; Fahey, T.; Hawes, A.; Kingston, G.; Madden, M.R. Human keratinocyte growth factor effects in a porcine model of epidermal wound healing. J. Exp. Med. 1993, 178, 865–878. [Google Scholar] [CrossRef] [Green Version]
- George, A.J.; Thomas, W.G.; Hannan, R.D. The renin–angiotensin system and cancer: Old dog, new tricks. Nat. Rev. Cancer 2010, 10, 745–759. [Google Scholar] [CrossRef]
- Singer, A.J.; Clark, R.A.F. Cutaneous Wound Healing. N. Engl. J. Med. 1999, 341, 738–746. [Google Scholar] [CrossRef]
- Pastar, I.; Stojadinovic, O.; Yin, N.C.; Ramirez, H.; Nusbaum, A.G.; Sawaya, A.; Patel, S.B.; Khalid, L.; Isseroff, R.R.; Tomic-Canic, M. Epithelialization in Wound Healing: A Comprehensive Review. Adv. Wound Care. 2014, 3, 445–464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tonnesen, M.G.; Feng, X.; Clark, R.A.F. Angiogenesis in Wound Healing. J. Invest. Dermatol. Symp. Proc. 2000, 5, 40–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hardy, M.A. The Biology of Scar Formation. Phys. Ther. 1989, 69, 1014–1024. [Google Scholar] [CrossRef] [PubMed]
- Parrish, W.; Roides, B. Phisiology of blood components in wound healing: An appreciation of cellular co-operativity in platelet rich plasma action. J. Exer. Sports Orthoped. 2017, 4, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Jannesari, M.; Varshosaz, J.; Morshed, M.; Zamani, M. Composite poly(vinyl alcohol)/poly(vinyl acetate) electrospun nanofibrous mats as a novel wound dressing matrix for controlled release of drugs. Int. J. Nanomed. 2011, 6, 993–1003. [Google Scholar] [CrossRef] [Green Version]
- Day, R.M. 6-Functional requirements of wound repair biomaterials. In Advanced Wound Repair Therapies; Farrar, D., Ed.; Woodhead Publishing: Cambridge, UK, 2011; pp. 155–173. [Google Scholar]
- Field, C.K.; Kerstein, M.D. Overview of wound healing in a moist environment. Am. J. Surg. 1994, 167, 2S–6S. [Google Scholar] [CrossRef]
- Agarwal, A.; McAnulty, J.F.; Schurr, M.J.; Murphy, C.J.; Abbott, N.L. Polymeric materials for chronic wound and burn dressings. In Advanced Wound Repair Therapies; Farrar, D., Ed.; Woodhead Publishing: Cambridge, UK, 2011; pp. 186–208. [Google Scholar]
- Ovington, L.G. Advances in wound dressings. Clin. Dermatol. 2007, 25, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Howe, L.M. Soft Tissue Surgery, An Issue of Veterinary Clinics of North America: Small Animal Practice, 1st ed.; Elsevier: Amsterdam, The Netherlands, 2015. [Google Scholar]
- Elsner, J.J.; Shefy-Peleg, A.; Zilberman, M. Novel biodegradable composite wound dressings with controlled release of antibiotics: Microstructure, mechanical and physical properties. J. Biomed. Mater. Res. Part B 2010, 93, 425–435. [Google Scholar] [CrossRef]
- Shyna, S.; Shanti, K.A.; Prabha, D.N.; Lynda, V.T. A nonadherent chitosan-polyvinyl alcohol absorbent wound dressing prepared via controlled freeze-dry technology. Int. J. Biol. Macromol. 2020, 150, 129–140. [Google Scholar] [CrossRef]
- Salehi, M.; Niyakan, M.; Ehterami, A.; Haghi-Daredeh, S.; Nazarnezhad, S.; Abbaszadeh-Goudarzi, G.; Vaez, A.; Hashemi, S.F.; Rezaei, N.; Mousavi, S.R. Porous electrospun poly(ε-caprolactone)/gelatin nanofibrous mat containing cinnamon for wound healing application: In vitro and in vivo study. Biomed. Eng. Lett. 2020, 10, 149–161. [Google Scholar] [CrossRef]
- Abdelrahman, T.; Newton, H. Wound dressings: Principles and practice. Surgery (Oxford) 2011, 29, 491–495. [Google Scholar] [CrossRef]
- Ruszczak, Z. Effect of collagen matrices on dermal wound healing. Adv. Drug. Deliv. Rev. 2003, 55, 1595–1611. [Google Scholar] [CrossRef] [PubMed]
- Simões, D.; Miguel, S.P.; Ribeiro, M.P.; Coutinho, P.; Mendonça, A.G.; Correia, I.J. Recent advances on antimicrobial wound dressing: A review. Eur. J. Pharm. Biopharm. 2018, 127, 130–141. [Google Scholar] [CrossRef] [PubMed]
- Catanzano, O.; Boateng, J. Local Delivery of Growth Factors Using Wound Dressings. In Therapeutic Dressings and Wound Healing Applications; John Wiley & Sons, Ltd.: Chichester, UK, 2020; pp. 291–314. [Google Scholar]
- Paul, W.; Sharma, C. Chitosan and Alginate Wound Dressings: A Short Review. Trends Biomater. Artif. Organs 2004, 18, 18–23. [Google Scholar]
- Sill, T.J.; von Recum, H.A. Electrospinning: Applications in drug delivery and tissue engineering. Biomaterials 2008, 29, 1989–2006. [Google Scholar] [CrossRef]
- Kamoun, E.A.; Kenawy, E.-R.S.; Chen, X. A review on polymeric hydrogel membranes for wound dressing applications: PVA-based hydrogel dressings. J. Adv. Res. 2017, 8, 217–233. [Google Scholar] [CrossRef]
- Bianchera, A.; Catanzano, O.; Boateng, J.; Elviri, L. The Place of Biomaterials in Wound Healing. In Therapeutic Dressings and Wound Healing Applications; John Wiley & Sons, Ltd.: Chichester, UK, 2020; pp. 337–366. [Google Scholar]
- Skórkowska-Telichowska, K.; Czemplik, M.; Kulma, A.; Szopa, J. The local treatment and available dressings designed for chronic wounds. J. Am. Acad. Dermatol. 2013, 68, e117–e126. [Google Scholar] [CrossRef]
- Almazrooa, S.A.; Noonan, V.; Woo, S.-B. Resorbable collagen membranes: Histopathologic features. J. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 118, 236–240. [Google Scholar] [CrossRef] [Green Version]
- Maged, A.; Abdelkhalek, A.A.; Mahmoud, A.A.; Salah, S.; Ammar, M.M.; Ghorab, M.M. Mesenchymal stem cells associated with chitosan scaffolds loaded with rosuvastatin to improve wound healing. Eur. J. Pharm. Sci. 2019, 127, 185–198. [Google Scholar] [CrossRef]
- Rezaii, M.; Oryan, S.; Javeri, A. Curcumin nanoparticles incorporated collagen-chitosan scaffold promotes cutaneous wound healing through regulation of TGF-β1/Smad7 gene expression. Mater. Sci. Eng. C 2019, 98, 347–357. [Google Scholar] [CrossRef]
- Aljghami, M.E.; Saboor, S.; Amini-Nik, S. Emerging Innovative Wound Dressings. Ann. Biomed. Eng. 2019, 47, 659–675. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, J.F.; Knill, C.J.; Thorley, M. Natural polymers for healing wounds. In Recent Advances in Environmentally Compatible Polymers; Kennedy, J.F., Phillips, G.O., Williams, P.A., Eds.; Woodhead Publishing: Cambridge, UK, 2001; pp. 97–104. [Google Scholar]
- Hwang, M.R.; Kim, J.O.; Lee, J.H.; Kim, Y.I.; Kim, J.H.; Chang, S.W.; Jin, S.G.; Kim, J.A.; Lyoo, W.S.; Han, S.S.; et al. Gentamicin-Loaded Wound Dressing With Polyvinyl Alcohol/Dextran Hydrogel: Gel Characterization and In Vivo Healing Evaluation. AAPS Pharm. Sci. Technol. 2010, 11, 1092–1103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sell, S.A.; Wolfe, P.S.; Garg, K.; McCool, J.M.; Rodriguez, I.A.; Bowlin, G.L. The Use of Natural Polymers in Tissue Engineering: A Focus on Electrospun Extracellular Matrix Analogues. Polymers 2010, 2, 522–553. [Google Scholar] [CrossRef]
- Price, R.D.; Berry, M.G.; Navsaria, H.A. Hyaluronic acid: The scientific and clinical evidence. J. Plast. Reconstr. Aesthet. Surg. 2007, 60, 1110–1119. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Xue, Y.; Jia, B.; Bai, Y.; Zuo, Y.; Wang, S.; Zhao, Y.; Yang, W.; Tang, H. The preparation of hyaluronic acid grafted pullulan polymers and their use in the formation of novel biocompatible wound healing film. Carbohydr. Polym. 2018, 188, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Bracaglia, L.G.; Smith, B.T.; Watson, E.; Arumugasaamy, N.; Mikos, A.G.; Fisher, J.P. 3D printing for the design and fabrication of polymer-based gradient scaffolds. Acta Biomater. 2017, 56, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Dutta, R.C.; Dey, M.; Dutta, A.K.; Basu, B. Competent processing techniques for scaffolds in tissue engineering. Biotechnol. Adv. 2017, 35, 240–250. [Google Scholar] [CrossRef]
- Eberli, D. Tissue Engineering, 2nd ed.; Elsevier: Amsterdam, The Netherlands, 2010. [Google Scholar]
- Lanza, R.; Langer, R.; Vacanti, J.P. Principles of Tissue Engineering, 4th ed.; Elsevier: Amsterdam, The Netherlands, 2013. [Google Scholar]
- Dávila, J.L.; Freitas, M.S.; Neto, P.I.; Silveira, Z.C.; Silva, J.V.L.; d’Ávila, M.A. Fabrication of PCL/β-TCP scaffolds by 3D mini-screw extrusion printing. J. Appl. Polym. Sci. 2016, 133. [Google Scholar] [CrossRef]
- Hamid, Q.; Snyder, J.; Wang, C.; Timmer, M.; Hammer, J.; Guceri, S.; Sun, W. Fabrication of three-dimensional scaffolds using precision extrusion deposition with an assisted cooling device. Biofabrication 2011, 3, 034109. [Google Scholar] [CrossRef]
- Liu, P.; Chen, W.; Liu, C.; Tian, M.; Liu, P. A novel poly(vinyl alcohol)/poly(ethylene glycol) scaffold for tissue engineering with a unique bimodal open-celled structure fabricated using supercritical fluid foaming. Sci. Rep. 2019, 9. [Google Scholar] [CrossRef]
- Tsai, W.C.; Wang, Y. Progress of supercritical fluid technology in polymerization and its applications in biomedical engineering. Prog. Polym. Sci. 2019, 98, 101161. [Google Scholar] [CrossRef]
- Tsang, V.L.; Bhatia, S.N. Three-dimensional tissue fabrication. Adv. Drug Deliv. Rev. 2004, 56, 1635–1647. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, K.T.; West, J.L. Photopolymerizable hydrogels for tissue engineering applications. Biomaterials 2002, 23, 4307–4314. [Google Scholar] [CrossRef]
- Wu, E.C.; Zhang, S.; Hauser, C.A.E. Self-Assembling Peptides as Cell-Interactive Scaffolds. Adv. Funct. Mater. 2012, 22, 456–468. [Google Scholar] [CrossRef]
- Zhu, X.; Cui, W.; Li, X.; Jin, Y. Electrospun Fibrous Mats with High Porosity as Potential Scaffolds for Skin Tissue Engineering. Biomacromolecules 2008, 9, 1795–1801. [Google Scholar] [CrossRef]
- Jin, G.; Prabhakaran, M.P.; Ramakrishna, S. Stem cell differentiation to epidermal lineages on electrospun nanofibrous substrates for skin tissue engineering. Acta Biomater. 2011, 7, 3113–3122. [Google Scholar] [CrossRef]
- Zhao, X.; Sun, X.; Yildirimer, L.; Lang, Q.; Lin, Z.Y.W.; Zheng, R.; Zhang, Y.; Cui, W.; Annabi, N.; Khademhosseini, A. Cell infiltrative hydrogel fibrous scaffolds for accelerated wound healing. Acta Biomater. 2017, 49, 66–77. [Google Scholar] [CrossRef] [Green Version]
- Shu, M.; Long, S.; Huang, Y.; Li, D.; Li, H.; Li, X. High strength and antibacterial polyelectrolyte complex CS/HS hydrogel films for wound healing. Soft Matter. 2019, 15, 7686–7694. [Google Scholar] [CrossRef]
- Uzun, M.; Anand, S.C.; Shah, T. In Vitro Characterisation and Evaluation of Different Types of Wound Dressing Materials. J. Biomed. Eng. Technol. 2013, 1, 1–7. [Google Scholar] [CrossRef]
- Yang, T.-L. Chitin-based Materials in Tissue Engineering: Applications in Soft Tissue and Epithelial Organ. Int. J. Mol. Sci. 2011, 12, 1936–1963. [Google Scholar] [CrossRef] [Green Version]
- Baker, B.M.; Trappmann, B.; Wang, W.Y.; Sakar, M.S.; Kim, I.L.; Shenoy, V.B.; Burdick, J.A.; Chen, C.S. Cell-mediated fibre recruitment drives extracellular matrix mechanosensing in engineered fibrillar microenvironments. Nat. Mater. 2015, 14, 1262–1268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soman, P.; Kelber, J.A.; Lee, J.W.; Wright, T.N.; Vecchio, K.S.; Klemke, R.L.; Chen, S. Cancer cell migration within 3D layer-by-layer microfabricated photocrosslinked PEG scaffolds with tunable stiffness. Biomaterials 2012, 33, 7064–7070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, T.T.; Foushee, A.M.D.; Johnson, M.C.; Jockheck-Clark, A.R.; Stahl, J.M. Development of Electrospun Chitosan-Polyethylene Oxide/Fibrinogen Biocomposite for Potential Wound Healing Applications. Nanoscale Res. Lett. 2018, 13, 88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shefa, A.A.; Taz, M.; Hossain, M.; Kim, Y.S.; Lee, S.Y.; Lee, B.T. Investigation of efficiency of a novel, zinc oxide loaded TEMPO-oxidized cellulose nanofiber based hemostat for topical bleeding. Int. J. Biol. Macromol. 2019, 126, 786–795. [Google Scholar] [CrossRef]
- Ehterami, A.; Salehi, M.; Farzamfar, S.; Vaez, A.; Samadian, H.; Sahrapeyma, H.; Mirzaii, M.; Ghorbani, S.; Goodarzi, A. In vitro and in vivo study of PCL/COLL wound dressing loaded with insulin-chitosan nanoparticles on cutaneous wound healing in rats model. Int. J. Biol. Macromol. 2018, 117, 601–609. [Google Scholar] [CrossRef]
- Song, A.; Rane, A.A.; Christman, K.L. Antibacterial and cell-adhesive polypeptide and poly(ethylene glycol) hydrogel as a potential scaffold for wound healing. Acta Biomater. 2012, 8, 41–50. [Google Scholar] [CrossRef] [Green Version]
- Ajmal, G.; Bonde, G.V.; Mittal, P.; Khan, G.; Pandey, V.K.; Bakade, B.V.; Mishra, B. Biomimetic PCL-gelatin based nanofibers loaded with ciprofloxacin hydrochloride and quercetin: A potential antibacterial and anti-oxidant dressing material for accelerated healing of a full thickness wound. Int. J. Pharm. 2019, 567, 118480. [Google Scholar] [CrossRef]
- Bhullar, S.K.; Ruzgar, D.G.; Fortunato, G.; Aneja, G.K.; Orhan, M.; Saber-Samandari, S.; Sadighi, M.; Ahadian, S.; Ramalingam, M.A. Facile Method for Controlled Fabrication of Hybrid Silver Nanoparticle-Poly(-caprolactone) Fibrous Constructs with Antimicrobial Properties. J. Nanosci. Nanotechnol. 2019, 19, 6949–6955. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, R.; Saito, Y.; Fujiwara, Y.; Jo, J.-I.; Tabata, Y. Preparation of fibrin hydrogels to promote the recruitment of anti-inflammatory macrophages. Acta Biomater. 2019, 89, 152–165. [Google Scholar] [CrossRef]
- Wang, P.; Huang, S.; Hu, Z.; Yang, W.; Lan, Y.; Zhu, J.; Hancharou, A.; Guo, R.; Tang, B. In situ formed anti-inflammatory hydrogel loading plasmid DNA encoding VEGF for burn wound healing. Acta Biomater. 2019, 100, 191–201. [Google Scholar] [CrossRef]
- Sen, S.; Basak, P.; Sinha, B.P.; Maurye, P.; Jaiswal, K.K.; Das, P.; Mandal, T.K. Anti-inflammatory effect of epidermal growth factor conjugated silk fibroin immobilized polyurethane ameliorates diabetic burn wound healing. Int. J. Biol. Macromol. 2020, 143, 1009–1032. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Cells | Functions in Wound Healing | Ref. |
|---|---|---|
| Platelets | Thrombus formation Rich reservoirs of inflammatory mediators (including cytokines) Stimulus for inflammation | [22] |
| Neutrophils | First cells to infiltrate the injury site Phagocytosis and intracellular killing of invading bacteria | [23] |
| Macrophages | Clear debris and necrotic tissue, phagocytose and killing of invading bacteria Rich reservoirs of inflammatory mediators (including cytokines) Stimulate fibroblast division, collagen production and angiogenesis | [24] |
| Fibroblasts | Produce many components of the ECM (e.g., collagen, fibronectin, hyaluronic acid, etc.) Synthesize granulation tissue | [25] |
| Growth factors | ||
| VEGF (Vascular endothelial growth factor) | Stimulates the angiogenesis in granulation tissue Stimulates endothelial cell proliferation | [26] |
| FGFS (Fibroblast growth factors) | Proliferation of fibroblasts and epithelial cells, matrix deposition, wound contraction, angiogenesis Accelerates the formation of granulation tissue | [27] |
| KGFS (Keratinocyte growth factors) | Proliferation and migration of keratinocytes | [28] |
| PDGF (Platelet-derived growth factor) | Mitogenic for both endothelial cells and fibroblasts Chemoattractant for neutrophils and fibroblasts Fibroblast proliferation and collagen metabolism The only growth factor currently approved by the FDA | [24] |
| EGF (Epidermal growth factor) | Differentiation, proliferation, migration and adhesion of keratinocytes Formation of granulation tissue | [24] |
| IL-1 (Interleukin-1) | Neutrophil chemotaxis Fibroblast proliferation | [24] |
| TGF-Β (Transforming growth factor-β) | Mitogenic for fibroblasts Chemotactic for macrophages Indirect stimulation of angiogenesis and collagen metabolism | [24] |
| Physical | Chemical | Technological |
|---|---|---|
| Maintain proper moisture at the wound bed Permeable to water and gas Ability to absorb exudates and blood at wound site Mechanical protection Adaptability to wound type and body shape Protecting/acting against infectious agents Maintaining temperature To be easily applied and removed with minimal frequency | Biocompatible Suitable degradation rate Non-toxic Non-inflammatory Non-allergenic Antimicrobial action | Economical process of preparation High reproducibility Mechanical stability Easy sterilization Long shelf life |
| Polymer | Advantages | Disadvantages | Role in Wound Healing | Ref. |
|---|---|---|---|---|
| Alginate | Biocompatible Resistance in acidic media Biodegradable Relative low cost Low toxicity Gelling properties | Overstimulation of fibroblasts | Ability to absorb fluids Maintains wound moist Promotes granulation tissue formation Stimulates monocytes to produce elevated levels of cytokines | [50,51] |
| Collagen | Major protein component of the ECM Good biocompatibility High mechanical strength Good cell recognition | Contamination by viral Difficult to process High cost when resulting from recombinant technologies | Indispensable structural supportive role in connective tissue Cell adhesion properties as it binds with extracellular integrin receptors through arginine/glycine/aspartate binding sites | [52,53] |
| Chitosan/ Chitin | Biocompatible Biodegradable Nonantigenic Nontoxic Oxygen permeability | Poor stability | Improves fibroblasts, macrophages, and inflammatory cells functions Antimicrobial activity Rapid bone regeneration at initial stages Enhances the granulation of wound Its degradation products take part in the makeup the ECM and cartilage | [49,50,54] |
| Cellulose | Biocompatible The most abundant molecules in nature Plant origin cellulose can be isolated with cheap procedures | Expensive purifying processes | Stimulates PDGF, FGF and EGF, which increase granulation tissue formation and vascularization | [50,55] |
| Dextran (Dex) | Biocompatible Colloidal Hydrophilic Inert in biological systems Hardly affects the cell viability. | Limited solubility | Accelerates polymerization of fibrin in vivo Stimulates the structure of the fibrin clot Stimulates macrophages | [56,57] |
| Fibrin/fibroin | High mechanical strength excellent Biocompatibility Minimal adverse effects on the immune system | Inflammation Degradation | Clot formation Contributes to bleeding stopping The basis for cells migration during wound healing Substrate for platelets, endothelial cells, fibroblasts, and macrophages | [50] |
| Gelatin | Denatured form of collagen Excellent biodegradability Non-antigenicity Cost efficiency | It dissolves as a colloidal sol at or above 37 °C, and gels near room temperature Gelatin is frequently cross-linked/combined with other polymers | Facilitates cell adhesion and proliferation | [58] |
| HA | Forms a smaller part of the ECM Biocompatible Soluble in water Nonallergenic | Rapid enzymatic degradation in physiological media | Stimulates fibroblast proliferation and collagen deposition Enhances keratinocyte proliferation | [59,60] |
| Polyvinyl alcohol (PVA) | Biocompatible Nontoxic Hydrophilic Water soluble pH sensitive |
| PLA | Biocompatible Biodegradable The degradation products are absorbed by the body through natural metabolic pathways Nontoxic Hydrophobic Structurally stable |
| PGA | Biocompatible Biodegradable (by hydrolysis; it produces CO2 and lowers the local pH leading to cell and tissue necrosis. More hydrophilic than PLA High tensile strength |
| Polyurethane (PU) | Biocompatible Degradation rate can be adapted Potential side effects of degradation products Tough and durable |
| PLGA | Biocompatible Biodegradable Degradation rate can be controlled by adjusting monomer ratios |
| PCL | Biocompatible Biodegradable Slower degradation rate than other polyesters Hydrophobic Semicrystalline Good elastic properties |
| PEG | Biocompatible Nonbiodegradable Bioinert Hydrophilic Resistant to protein adsorption |
| Polydimethylsiloxane (PDMS) | Bioinert Nonbiodegradable Compatible with blood Low toxicity Hydrophobic surface Antiadhesive properties Exceptional elasticity when lightly cross-linked Good thermal stability |
| Polyethylen oxide (PEO) | Non-toxic Biocompatible Non-immunogenic Hydrophilic Flexible |
| Polyvinyl pyrrolidone (PVP) | Biocompatible Biodegradable Environmental stability Low cytotoxicity High chemical and thermal resistance Affinity to complex hydrophilic and hydrophobic substances Very good solubility in water and organic solvents |
| Conventional | Advantages | Disadvantages | Suitable Materials | Ref. |
|---|---|---|---|---|
| Solvent casting/particulate leaching | Control over porosity and crystallinity Minimal material needed | Residual solvents and limited mechanical features Pores not interconnected | PU PCL PLA | [63,64] |
| Extrusion | Control over porosity Obtaining 3D scaffolds | It uses pastes/pallets and a volatile solvent High temperatures or pressure needed | PCL PLA Calcium phosphates | [65,66] |
| Molding | Control over porosity | High temperature for nonamorphous polymer | HA PLGA Gelatin | [64] |
| Freeze-drying | High temperature and separate leaching phase not mandatory | Lower porosity than in other methods | PLGA PGA | [63] |
| Gas foaming | Free of harsh organic solvents and control over porosity | Limited mechanical features and poor pore interconnectivity | PLGA | [63] |
| Supercritical fluid processing | Controllable cellular structure and exemption of toxic organic solvents The blowing agent is non-toxic, non-flammable, chemical stable Its low critical temperature can protect heat-labile compounds from thermal degradation | Time consuming | PVA PEG | [67,68] |
| Fiber bonding | High surface to volume ratio and high porosity | Limited application to some polymers | PGA | [63] |
| Fused deposition modeling | Control over pore size, morphology, and interconnectivity Can have a linear print speed of 10–50 mm/s | Temperatures used are generally too high for the inclusion of cells or bioactive molecules | PCL TCP | [69] |
| ADVANCED | ||||
| Rapid prototyping - 3D plotting - 3D printing - Stereolithography -Selective laser sintering | Excellent control over geometry and porosity | Limited application to some polymers and the use of expensive equipment | PCL PLGA PVA PEEK PDLLA | [63] |
| Electrospinning | Control over porosity and crystallinity; diameter and orientation of fibers can be manipulated | Pore size decrease with fiber thickness | PCL Collagen PLA EVOH Chitin | [63] |
| In situ photopolymerization | Spatial and temporal control over polymerization, fast curing rates (< a second - few minutes) at room or physiological temperatures, and minimal heat production hydrogels can be created in situ from aqueous precursors To form complex shapes | Biological sensible molecules can degrade Limited material choice Limited mechanical properties of scaffolds | Polyurethane PEGMA PHBV Polyacrylamide | [64,70] |
| High internal phase emulsion (HIPE) | Good pore morphology | High processing temperatures Limited polymers | Biodegradable polymers | [64] |
| Self-assembling peptides | Compatible with in vitro cultures Peptides can be assembled into complex architectures (fibers, sheets, spheres) | The use of expensive materials The scaffold size is limited | RAD16-II RAD16-I EAK16-II KLD12 P11-4 MAX1 | [64,71] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Negut, I.; Dorcioman, G.; Grumezescu, V. Scaffolds for Wound Healing Applications. Polymers 2020, 12, 2010. https://doi.org/10.3390/polym12092010
Negut I, Dorcioman G, Grumezescu V. Scaffolds for Wound Healing Applications. Polymers. 2020; 12(9):2010. https://doi.org/10.3390/polym12092010
Chicago/Turabian StyleNegut, Irina, Gabriela Dorcioman, and Valentina Grumezescu. 2020. "Scaffolds for Wound Healing Applications" Polymers 12, no. 9: 2010. https://doi.org/10.3390/polym12092010
APA StyleNegut, I., Dorcioman, G., & Grumezescu, V. (2020). Scaffolds for Wound Healing Applications. Polymers, 12(9), 2010. https://doi.org/10.3390/polym12092010