
Impact of Three Different Processing Techniques on the Strength and Structure of Juvenile Ovine Pulmonary Homografts

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
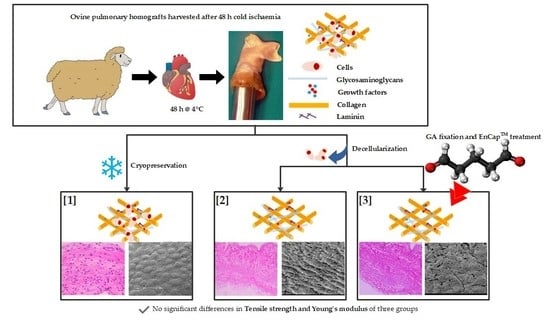
2.1. Study Design
2.2. Preparation of Homografts
2.3. Evaluation of Processed Homografts
2.3.1. Histological Analysis
2.3.2. Mechanical Properties
2.3.3. Statistical Analysis
3. Results
4. Discussions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Diaz, R.; Hernandez-Vaquero, D.; Alvarez-Cabo, R.; Avanzas, P.; Silva, J.; Moris, C.; Pascual, I. Long-term outcomes of mechanical versus biological aortic valve prosthesis: Systematic review and meta-analysis. J. Thorac. Cardiovasc. Surg. 2019, 158, 706–714.e18. [Google Scholar] [CrossRef]
- Hechadi, J.; Gerber, B.L.; Coche, E.; Melchior, J.; Jashari, R.; Glineur, D.; Noirhomme, P.; Rubay, J.; El Khoury, G.; de Kerchove, L. Stentless xenografts as an alternative to pulmonary homografts in the Ross operation. Eur. J. Cardiothorac. Surg. 2013, 44, e32–e39. [Google Scholar] [CrossRef]
- Romeo, J.L.R.; Papageorgiou, G.; van de Woestijne, P.C.; Takkenberg, J.J.M.; Westenberg, L.E.H.; van Beynum, I.; Bogers, A.; Mokhles, M.M. Downsized cryopreserved and standard-sized allografts for right ventricular outflow tract reconstruction in children: Long-term single-institutional experience. Interact. Cardiovasc. Thorac. Surg. 2018, 27, 257–263. [Google Scholar] [CrossRef]
- Tierney, E.S.; Gersony, W.M.; Altmann, K.; Solowiejczyk, D.E.; Bevilacqua, L.M.; Khan, C.; Krongrad, E.; Mosca, R.S.; Quaegebeur, J.M.; Apfel, H.D. Pulmonary position cryopreserved homografts: Durability in pediatric Ross and non-Ross patients. J. Thorac. Cardiovasc. Surg. 2005, 130, 282–286. [Google Scholar] [CrossRef]
- Goffin, Y.A.; van Hoeck, B.; Jashari, R.; Soots, G.; Kalmar, P. Banking of cryopreserved heart valves in Europe: Assessment of a 10-year operation in the European Homograft Bank (EHB). J. Heart Valve Dis. 2000, 9, 207–214. [Google Scholar]
- Smit, F.E.; Bester, D.; van den Heever, J.J.; Schlegel, F.; Botes, L.; Dohmen, P.M. Does prolonged post-mortem cold ischaemic harvesting time influence cryopreserved pulmonary homograft tissue integrity? Cell Tissue Bank. 2015, 16, 531–544. [Google Scholar] [CrossRef]
- Kitagawa, T.; Masuda, Y.; Tominaga, T.; Kano, M. Cellular biology of cryopreserved allograft valves. J. Med. Investig. 2001, 48, 123–132. [Google Scholar]
- Bester, D.; Botes, L.; van den Heever, J.J.; Kotze, H.; Dohmen, P.; Pomar, J.L.; Smit, F.E. Cadaver donation: Structural integrity of pulmonary homografts harvested 48 h post mortem in the juvenile ovine model. Cell Tissue Bank. 2018, 19, 743–754. [Google Scholar] [CrossRef]
- Shaddy, R.E.; Hawkins, J.A. Immunology and failure of valved allografts in children. Ann. Thorac. Surg. 2002, 74, 1271–1275. [Google Scholar] [CrossRef]
- Baskett, R.J.; Nanton, M.A.; Warren, A.E.; Ross, D.B. Human leukocyte antigen-DR and ABO mismatch are associated with accelerated homograft valve failure in children: Implications for therapeutic interventions. J. Thorac. Cardiovasc. Surg. 2003, 126, 232–239. [Google Scholar] [CrossRef]
- Ryan, W.H.; Herbert, M.A.; Dewey, T.M.; Agarwal, S.; Ryan, A.L.; Prince, S.L.; Mack, M.J. The occurrence of postoperative pulmonary homograft stenosis in adult patients undergoing the Ross procedure. J. Heart Valve Dis. 2006, 15, 108–113; discussion 113-4. [Google Scholar] [PubMed]
- Cebotari, S.; Tudorache, I.; Ciubotaru, A.; Boethig, D.; Sarikouch, S.; Goerler, A.; Lichtenberg, A.; Cheptanaru, E.; Barnaciuc, S.; Cazacu, A.; et al. Use of fresh decellularized allografts for pulmonary valve replacement may reduce the reoperation rate in children and young adults: Early report. Circulation 2011, 124, S115–S123. [Google Scholar] [CrossRef] [PubMed]
- Erdbrügger, W.; Konertz, W.; Dohmen, P.M.; Posner, S.; Ellerbrok, H.; Brodde, O.E.; Robenek, H.; Modersohn, D.; Pruss, A.; Holinski, S.; et al. Decellularized xenogenic heart valves reveal remodeling and growth potential in vivo. Tissue Eng. 2006, 12, 2059–2068. [Google Scholar] [CrossRef] [PubMed]
- VeDepo, M.C.; Detamore, M.S.; Hopkins, R.A.; Converse, G.L. Recellularization of decellularized heart valves: Progress toward the tissue-engineered heart valve. J. Tissue Eng. 2017, 8, 2041731417726327. [Google Scholar] [CrossRef] [PubMed]
- Bourgine, P.E.; Pippenger, B.E.; Todorov, A.; Tchang, L.; Martin, I. Tissue decellularization by activation of programmed cell death. Biomaterials 2013, 34, 6099–6108. [Google Scholar] [CrossRef]
- Korossis, S.A.; Booth, C.; Wilcox, H.E.; Watterson, K.G.; Kearney, J.N.; Fisher, J.; Ingham, E. Tissue engineering of cardiac valve prostheses II: Biomechanical characterization of decellularized porcine aortic heart valves. J. Heart Valve Dis. 2002, 11, 463–471. [Google Scholar]
- Sheehy, E.J.; Cunniffe, G.M.; O’Brien, F.J. 5 Collagen-based biomaterials for tissue regeneration and repair. In Peptides and Proteins as Biomaterials for Tissue Regeneration and Repair; Barbosa, M.A., Martins, M.C.L., Eds.; Woodhead Publishing: Sawston, UK, 2018; pp. 127–150. [Google Scholar] [CrossRef]
- Oryan, A.; Kamali, A.; Moshiri, A.; Baharvand, H.; Daemi, H. Chemical crosslinking of biopolymeric scaffolds: Current knowledge and future directions of crosslinked engineered bone scaffolds. Int. J. Biol. Macromol. 2018, 107, 678–688. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.; Lim, H.G.; Lee, C.H.; Kim, Y.J. Effects of glutaraldehyde concentration and fixation time on material characteristics and calcification of bovine pericardium: Implications for the optimal method of fixation of autologous pericardium used for cardiovascular surgery. Interact. Cardiovasc. Thorac. Surg. 2017, 24, 402–406. [Google Scholar] [CrossRef] [PubMed]
- Padala, M. A heart valve is no stronger than its weakest link: The need to improve durability of pericardial leaflets. J. Thorac. Cardiovasc. Surg. 2018, 156, 207–208. [Google Scholar] [CrossRef] [PubMed]
- Strange, G.; Brizard, C.; Karl, T.R.; Neethling, L. An evaluation of Admedus’ tissue engineering process-treated (ADAPT) bovine pericardium patch (CardioCel) for the repair of cardiac and vascular defects. Expert Rev. Med. Devices 2015, 12, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Seifter, E.; Frater, R.W.M. Anticalcification Treatment for Aldehyde-Tanned Biological Tissue; Albert Einstein College of Medicine of Yeshiva University: Bronx, NY, USA, 1995; Available online: http://www.freepatentsonline.com/5476516.html (accessed on 2 October 2019).
- Succi, J.E.; Buffolo, E.; Salles, C.A.; Casagrande, I.S.J.; Neto, J.V.; de Mendonça, J.T.; Filho, R.V.; Jaramillo, I.A. Valve replacement with aortic glutaraldehyde preserved homografts: A multicenter study. Braz. J. Cardiovasc. Surg. 1986, 1, 20–23. [Google Scholar] [CrossRef]
- Laker, L.; Dohmen, P.M.; Smit, F.E. Synergy in a detergent combination results in superior decellularized bovine pericardial extracellular matrix scaffolds. J. Biomed. Mater. Res. B Appl. Biomater. 2020, 108, 2571–2578. [Google Scholar] [CrossRef] [PubMed]
- Bester, D.; Smit, F.E.; van den Heever, J.J.; Botes, L.; Dohmen, P.M.C.E. Detoxification and Stabilization of Implantable or Transplantable Biological Material. EU Patent 16792990.0-1455, 28 July 2016. [Google Scholar]
- Dijkman, P.E.; Driessen-Mol, A.; Frese, L.; Hoerstrup, S.P.; Baaijens, F.P. Decellularized homologous tissue-engineered heart valves as off-the-shelf alternatives to xeno- and homografts. Biomaterials 2012, 33, 4545–4554. [Google Scholar] [CrossRef]
- Crapo, P.M.; Gilbert, T.W.; Badylak, S.F. An overview of tissue and whole organ decellularization processes. Biomaterials 2011, 32, 3233–3243. [Google Scholar] [CrossRef]
- Bancroft, J.D.; Stevens, A. Theory and Practice of Histological Techniques, 3rd ed.; Churchill Livingstone: Edinburgh, UK, 1991. [Google Scholar]
- Spurr, A.R. A low-viscosity epoxy resin embedding medium for electron microscopy. J. Ultrastruct. Res. 1969, 26, 31–43. [Google Scholar] [CrossRef]
- Thubrikar, M.J.; Deck, J.D.; Aouad, J.; Nolan, S.P. Role of mechanical stress in calcification of aortic bioprosthetic valves. J. Thorac. Cardiovasc. Surg. 1983, 86, 115–125. [Google Scholar] [CrossRef]
- Ross, D.N. Homograft replacement of the aortic valve. Lancet 1962, 280, 487. [Google Scholar] [CrossRef]
- Barratt-Boyes, B.G. Homograft aortic valve replacement. N. Z. Med. J. 1965, 64, 41–43. [Google Scholar] [CrossRef]
- Angell, W.W.; Oury, J.H.; Lamberti, J.J.; Koziol, J. Durability of the viable aortic allograft. J. Thorac. Cardiovasc. Surg. 1989, 98, 48–55; discussion 55–56. [Google Scholar] [CrossRef]
- O’Brien, M.F.; McGiffin, D.C.; Stafford, E.G.; Gardner, M.A.; Pohlner, P.F.; Mclachlan, G.J.; Gall, K.; Smith, S.; Murphy, E. Allograft aortic valve replacement: Long-term comparative clinical analysis of the viable cryopreserved and antibiotic 4 degrees C stored valves. J. Card. Surg. 1991, 6, 534–543. [Google Scholar] [CrossRef]
- O’Brien, M.F.; Stafford, E.G.; Gardner, M.A.; Pohlner, P.G.; Tesar, P.J.; Cochrane, A.D.; Mau, T.K.; Gall, K.L.; Smith, S.E. Allograft aortic valve replacement: Long-term follow-up. Ann. Thorac. Surg. 1995, 60, S65–S70. [Google Scholar] [CrossRef]
- Lopes, S.A.; da Costa, F.D.; de Paula, J.B.; Dohmen, P.; Phol, F.; Vilani, R.; Roderjan, J.G.; Vieira, E.D. Decellularized heterografts versus cryopreserved homografts: Experimental study in sheep model. Braz. J. Cardiovasc. Surg. 2009, 24, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, R.N.; Jonas, R.A.; Schoen, F.J. Pathology of explanted cryopreserved allograft heart valves: Comparison with aortic valves from orthotopic heart transplants. J. Thorac. Cardiovasc. Surg. 1998, 115, 118–127. [Google Scholar] [CrossRef]
- Radosevich, J.A.; Ma, Y.X.; Salwen, H.R.; Rosen, S.T.; Lee, I.; Gould, V.E. Monoclonal antibody 44-3A6 as a probe for a novel antigen found on human lung carcinomas with glandular differentiation. Cancer Res. 1985, 45, 5808–5812. [Google Scholar] [CrossRef] [PubMed]
- Radosevich, J.A.; Haines, G.K.; Elseth, K.M.; Shambaugh, G.E.; Maker, V.K. A new method for the detection of viable cells in tissue sections using 3-[4,5-dimethylthiazol-2-yl]-2,5-diphenyltetrazolium bromide (MTT): An application in the assessment of tissue damage by surgical instruments. Virchows Archiv. B Cell Pathol. Incl. Mol. Pathol. 1993, 63, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Schenke-Layland, K.; Madershahian, N.; Riemann, I.; Starcher, B.; Halbhuber, K.J.; Konig, K.; Stock, U.A. Impact of cryopreservation on extracellular matrix structures of heart valve leaflets. Ann. Thorac. Surg. 2006, 81, 918–926. [Google Scholar] [CrossRef]
- Bibevski, S.; Ruzmetov, M.; Fortuna, R.S.; Turrentine, M.W.; Brown, J.W.; Ohye, R.G. Performance of SynerGraft Decellularized Pulmonary Allografts Compared With Standard Cryopreserved Allografts: Results From Multiinstitutional Data. Ann. Thorac. Surg. 2017, 103, 869–874. [Google Scholar] [CrossRef]
- Liao, J.; Joyce, E.M.; Sacks, M.S. Effects of decellularization on the mechanical and structural properties of the porcine aortic valve leaflet. Biomaterials 2008, 29, 1065–1074. [Google Scholar] [CrossRef]
- Zhou, J.; Fritze, O.; Schleicher, M.; Wendel, H.P.; Schenke-Layland, K.; Harasztosi, C.; Hu, S.; Stock, U.A. Impact of heart valve decellularization on 3-D ultrastructure, immunogenicity and thrombogenicity. Biomaterials 2010, 31, 2549–2554. [Google Scholar] [CrossRef]
- Converse, G.L.; Armstrong, M.; Quinn, R.W.; Buse, E.E.; Cromwell, M.L.; Moriarty, S.J.; Lofland, G.K.; Hilbert, S.L.; Hopkins, R.A. Effects of cryopreservation, decellularization and novel extracellular matrix conditioning on the quasi-static and time-dependent properties of the pulmonary valve leaflet. Acta Biomater. 2012, 8, 2722–2729. [Google Scholar] [CrossRef]
- Somers, P.; de Somer, F.; Cornelissen, M.; Thierens, H.; van Nooten, G. Decellularization of heart valve matrices: Search for the ideal balance. Artif. Cells Blood Substit. Immobil. Biotechnol. 2012, 40, 151–162. [Google Scholar] [CrossRef] [PubMed]
- Flynn, L.E. The use of decellularized adipose tissue to provide an inductive microenvironment for the adipogenic differentiation of human adipose-derived stem cells. Biomaterials 2010, 31, 4715–4724. [Google Scholar] [CrossRef] [PubMed]
- Brown, B.N.; Freund, J.M.; Han, L.; Rubin, J.P.; Reing, J.E.; Jeffries, E.M.; Wolf, M.T.; Tottey, S.; Barnes, C.A.; Ratner, B.D.; et al. Comparison of three methods for the derivation of a biologic scaffold composed of adipose tissue extracellular matrix. Tissue Eng. Part C Methods 2011, 17, 411–421. [Google Scholar] [CrossRef] [PubMed]
- Laker, L.; Dohmen, P.M.; Smit, F.E. The sequential effects of a multifactorial detergent based decellularization process on bovine pericardium. Biomed. Phys. Eng. Express 2020, 6, 065011. [Google Scholar] [CrossRef]
- Burch, P.T.; Kaza, A.K.; Lambert, L.M.; Holubkov, R.; Shaddy, R.E.; Hawkins, J.A. Clinical performance of decellularized cryopreserved valved allografts compared with standard allografts in the right ventricular outflow tract. Ann. Thorac. Surg. 2010, 90, 1301–1305; discussion 1306. [Google Scholar] [CrossRef]
- Brown, J.W.; Elkins, R.C.; Clarke, D.R.; Tweddell, J.S.; Huddleston, C.B.; Doty, J.R.; Fehrenbacher, J.W.; Takkenberg, J.J.M. Performance of the CryoValve SG human decellularized pulmonary valve in 342 patients relative to the conventional CryoValve at a mean follow-up of four years. J. Thorac. Cardiovasc. Surg. 2010, 139, 339–348. [Google Scholar] [CrossRef]
- Sarikouch, S.; Horke, A.; Tudorache, I.; Beerbaum, P.; Westhoff-Bleck, M.; Boethig, D.; Repin, O.; Maniuc, L.; Ciubotaru, A.; Haverich, A.; et al. Decellularized fresh homografts for pulmonary valve replacement: A decade of clinical experience. Eur. J. Cardiothorac. Surg. 2016, 50, 281–290. [Google Scholar] [CrossRef]
- Boethig, D.; Horke, A.; Hazekamp, M.; Meyns, B.; Rega, F.; van Puyvelde, J.; Hübler, M.; Schmiady, M.; Ciubotaru, A.; Stellin, G.; et al. A European study on decellularized homografts for pulmonary valve replacement: Initial results from the prospective ESPOIR Trial and ESPOIR Registry data. Eur. J. Cardiothorac. Surg. 2019, 56, 503–509. [Google Scholar] [CrossRef]
- Da Costa, F.D.A.; Costa, A.C.; Prestes, R.; Domanski, A.C.; Balbi, E.M.; Ferreira, A.D.; Lopes, S.V. The early and midterm function of decellularized aortic valve allografts. Ann. Thorac. Surg. 2010, 90, 1854–1860. [Google Scholar] [CrossRef]
- Botes, L.; Laker, L.; Dohmen, P.M.; Van den Heever, J.J.; Jordaan, C.J.; Lewies, A.; Smit, F.E. Advantages of decellularized bovine pericardial scaffolds compared to glutaraldehyde fixed bovine pericardial patches demonstrated in a 180-day implant ovine study. Cell Tissue Bank. 2022. [Google Scholar] [CrossRef]
- Umashankar, P.R.; Mohanan, P.V.; Kumari, T.V. Glutaraldehyde treatment elicits toxic response compared to decellularization in bovine pericardium. Toxicol. Int. 2012, 19, 51–58. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Cryopreserved | Decellularized | Decellularized Plus EnCapTM-Treated | p-Values | |
|---|---|---|---|---|---|
| Leaflet | TS (MPa) | 3.72 (3.12–5.01) | 1.83 (0.01–5.65) | 4.96 (4.34–6.76) | 0.23 |
| YM (MPa) | 23.34 (14.12–28.87) | 22.10 (0.10–55.27) | 41.11 (27.76–52.52) | 0.40 | |
| Wall | TS (MPa) | 1.80 (1.35–2.65) | 1.89 (1.57–2.38) | 1.90 (1.18–2.09) | 0.96 |
| YM (MPa) | 1.97 (1.22–3.18) | 2.32 (1.82–2.88) | 2.21 (1.99–3.58) | 0.75 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van den Heever, J.J.; Jordaan, C.J.; Lewies, A.; Goedhals, J.; Bester, D.; Botes, L.; Dohmen, P.M.; Smit, F.E. Impact of Three Different Processing Techniques on the Strength and Structure of Juvenile Ovine Pulmonary Homografts. Polymers 2022, 14, 3036. https://doi.org/10.3390/polym14153036
van den Heever JJ, Jordaan CJ, Lewies A, Goedhals J, Bester D, Botes L, Dohmen PM, Smit FE. Impact of Three Different Processing Techniques on the Strength and Structure of Juvenile Ovine Pulmonary Homografts. Polymers. 2022; 14(15):3036. https://doi.org/10.3390/polym14153036
Chicago/Turabian Stylevan den Heever, Johannes J, Christiaan J Jordaan, Angélique Lewies, Jacqueline Goedhals, Dreyer Bester, Lezelle Botes, Pascal M Dohmen, and Francis E Smit. 2022. "Impact of Three Different Processing Techniques on the Strength and Structure of Juvenile Ovine Pulmonary Homografts" Polymers 14, no. 15: 3036. https://doi.org/10.3390/polym14153036
APA Stylevan den Heever, J. J., Jordaan, C. J., Lewies, A., Goedhals, J., Bester, D., Botes, L., Dohmen, P. M., & Smit, F. E. (2022). Impact of Three Different Processing Techniques on the Strength and Structure of Juvenile Ovine Pulmonary Homografts. Polymers, 14(15), 3036. https://doi.org/10.3390/polym14153036