
Application of 3D-Printed Bioinks in Chronic Wound Healing: A Scoping Review

 , and
, and 
Abstract
:1. Introduction

{kind=link}
{kind=link}
{kind=link}
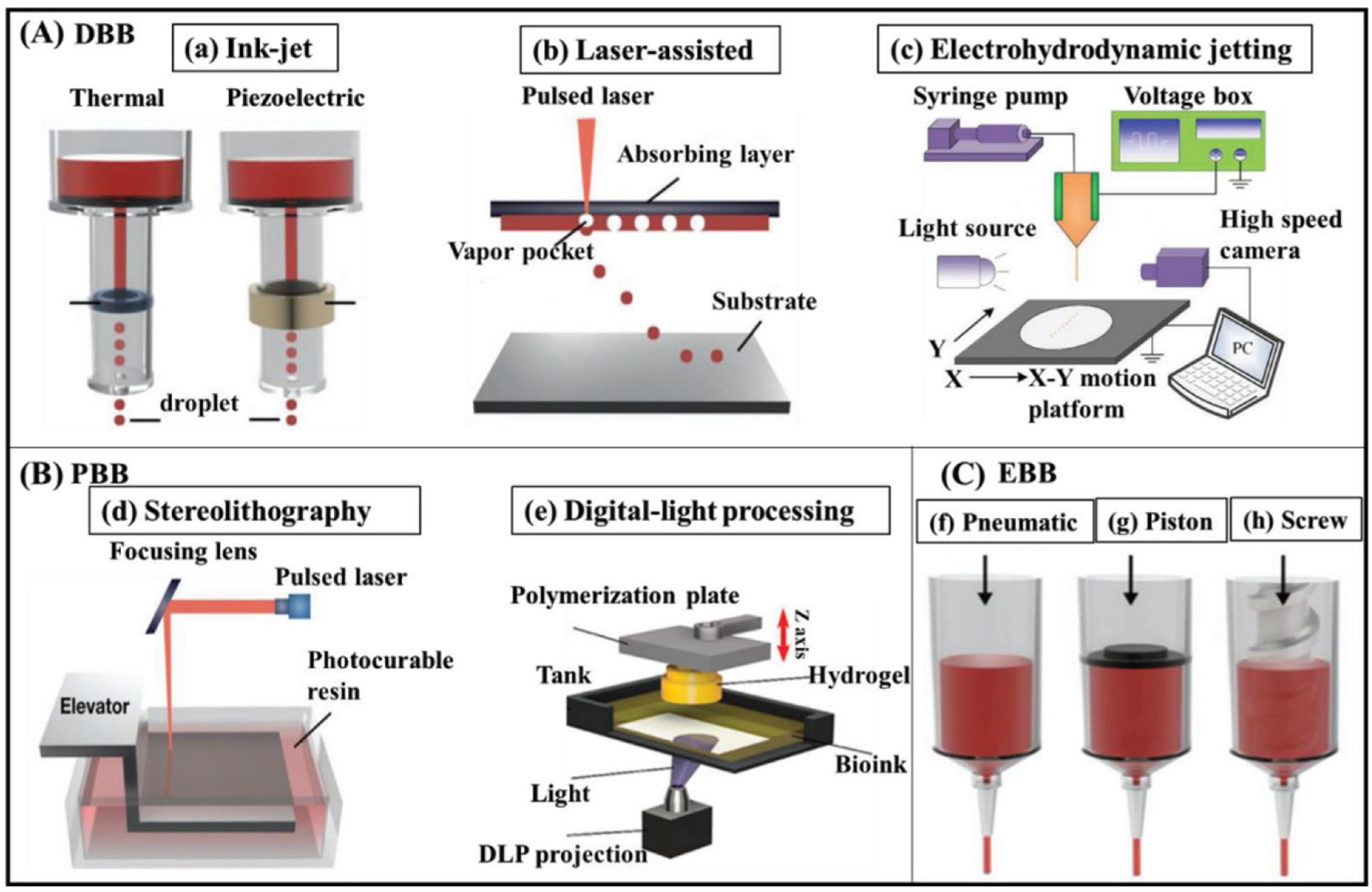
| Type of Bioprinting | Sub-Type | Definitions | Advantages | Limitations | Applications | References |
|---|---|---|---|---|---|---|
| Droplet-based Bioprinting (DBB) | Inkjet-based bioprinting | Inkjet-based bioprinting is a method that uses droplets to create tissue and organ constructs on a substrate. | low cost, high precision, fast fabrication speed, high resolution, and high throughput | High-viscosity ink has poor printability, small inkjet apertures, easy clogging, and high shear stress. | Fabrication of scaffold for tissue engineering | [19,34,35] |
| Laser-assisted bioprinting (LAB) | LAB uses the Laser-Induced Forward Transfer (LIFT) technique, where a pulsed laser beam is focused onto a bioink-coated substrate, creating a high-pressure bubble. | high resolution, no nozzle clogging, and non-contact printing | Thermal damage and slow gelation limit high-throughput printing and expensive equipment | Fabrication of scaffold for tissue engineering | [34,36] | |
| Electrohydrodynamic Jetting (EHDJ) | EHDJ uses high voltage to create an electric field that shapes bioink into a cone shape at the nozzle tip. | Preventing excessive pressure, protecting cell viability, high cell concentration, and high weight-to-volume ratio in bioink | Affecting cell viability and limited material propagation for larger droplet sizes (>400 µm) | Fabrication of scaffold for tissue engineering | [27,37] | |
| Photocuring-based Bioprinting (PBB) | stereolithography | Stereolithography (SLA) is a photochemical additive manufacturing technique that creates three-dimensional objects by curing a liquid photopolymer resin with a focused UV laser or light source. | High resolution, rapid printing with high cell viability (>85%), no shear stress on cells, and free clogging process | Requires transparent liquids for uniform crosslinking, cell contamination, and Restricted maximum cell density | Fabrication of scaffold for tissue engineering | [36,38,39] |
| Digital Light Processing (DLP) | DLP uses a digital light source to cure photosensitive polymers layer-by-layer using a dynamic mask that projects the desired pattern onto the bioink. | High-speed printing, production of complex structures without increasing time, Smoother 3D structures, and improving mechanical strength | Less suitable for applications requiring varying layer thicknesses, require complex setup and software for mask design and light pattern transmission | Fabrication of scaffold for tissue engineering | [30,40] | |
| Extrusion-based bioprinting (EBB) | Piston, Screw, Pneumatic-driven | Extrusion-based bioprinting techniques utilize the usage of a nozzle or syringe to extrude the bioink via piston, pressure, and screw-driven approach. | High-viscosity bioinks - Versatile for different bioink types - Better printing speed and mechanical strength compared to DBB | Limited printing resolution limits cell patterning and organization, and High shear stress | Fabrication of scaffold for tissue engineering | [24,41,42] |
2. Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction and Analysis
2.4. Data Charting and Synthesis
3. Results
3.1. Study Selection
3.2. Characteristics of Included Studies
3.3. Characteristics of the 3D Bioprinting Techniques
3.4. Bioink Composition and Characteristics
3.5. Applications and Effectiveness of 3D Bioprinted Bioinks
3.6. Summary of In Vivo Model Characteristics
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Jang, M.J.; Bae, S.; Jung, Y.-S.; Kim, J.C.; Kim, J.S.; Park, S.K.; Suh, J.S.; Yi, S.J.; Ahn, S.H.; O Lim, J.; et al. Enhanced wound healing using a 3D printed VEGF-mimicking peptide incorporated hydrogel patch in a pig model. Biomed. Mater. 2021, 16, 045013. [Google Scholar] [CrossRef] [PubMed]
- Kammona, O.; Tsanaktsidou, E.; Kiparissides, C. Recent Developments in 3D-(Bio)printed Hydrogels as Wound Dressings. Gels 2024, 10, 147. [Google Scholar] [CrossRef]
- Uchida, D.T.; Bruschi, M.L. 3D Printing as a Technological Strategy for the Personalized Treatment of Wound Healing. AAPS PharmSciTech 2023, 24, 41. [Google Scholar] [CrossRef] [PubMed]
- Yuan, N.; Shao, K.; Huang, S.; Chen, C. Chitosan, alginate, hyaluronic acid and other novel multifunctional hydrogel dressings for wound healing: A review. Int. J. Biol. Macromol. 2023, 240, 124321. [Google Scholar] [CrossRef] [PubMed]
- Yu, Q.; Wang, Q.; Zhang, L.; Deng, W.; Cao, X.; Wang, Z.; Sun, X.; Yu, J.; Xu, X. The applications of 3D printing in wound healing: The external delivery of stem cells and antibiosis. Adv. Drug Deliv. Rev. 2023, 197, 114823. [Google Scholar] [CrossRef]
- Sen, C.K.; Gordillo, G.M.; Roy, S.; Kirsner, R.; Lambert, L.; Hunt, T.K.; Gottrup, F.; Gurtner, G.C.; Longaker, M.T. Human skin wounds: A major and snowballing threat to public health and the economy. Wound Repair. Regen. 2009, 17, 763–771. [Google Scholar] [CrossRef]
- Heras, K.L.; Igartua, M.; Santos-Vizcaino, E.; Hernandez, R.M. Chronic wounds: Current status, available strategies and emerging therapeutic solutions. J. Control. Release 2020, 328, 532–550. [Google Scholar] [CrossRef]
- Armstrong, D.G.; Wrobel, J.; Robbins, J.M. Guest Editorial: Are Diabetes-Related Wounds and Amputations Worse than Cancer? Int. Wound J. 2007, 4, 286–287. [Google Scholar] [CrossRef]
- Feng, C.; Ouyang, J.; Tang, Z.; Kong, N.; Liu, Y.; Fu, L.; Ji, X.; Xie, T.; Farokhzad, O.C.; Tao, W. Germanene-Based Theranostic Materials for Surgical Adjuvant Treatment: Inhibiting Tumor Recurrence and Wound Infection. Matter 2020, 3, 127–144. [Google Scholar] [CrossRef]
- Masri, S.; Fauzi, M.B. Current Insight of Printability Quality Improvement Strategies in Natural-Based Bioinks for Skin Regeneration and Wound Healing. Polymers 2021, 13, 1011. [Google Scholar] [CrossRef]
- Zulkiflee, I.; Fauzi, M.B. Gelatin-Polyvinyl Alcohol Film for Tissue Engineering: A Concise Review. Biomedicines 2021, 9, 979. [Google Scholar] [CrossRef] [PubMed]
- Kačarević, P.; Rider, P.M.; Alkildani, S.; Retnasingh, S.; Smeets, R.; Jung, O.; Ivanišević, Z.; Barbeck, M. An Introduction to 3D Bioprinting: Possibilities, Challenges and Future Aspects. Materials 2018, 11, 2199. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Miller, K.; Ma, X.; Dewan, S.; Lawrence, N.; Whang, G.; Chung, P.; McCulloch, A.D.; Chen, S. Direct 3D bioprinting of cardiac micro-tissues mimicking native myocardium. Biomaterials 2020, 256, 120204. [Google Scholar] [CrossRef]
- Morais, A.R.D.V.; Alencar, D.N.; Júnior, F.H.X.; de Oliveira, C.M.; Marcelino, H.R.; Barratt, G.; Fessi, H.; Egito, E.S.T.D.; Elaissari, A. Freeze-drying of emulsified systems: A review. Int. J. Pharm. 2016, 503, 102–114. [Google Scholar] [CrossRef]
- Prasad, A.; Sankar, M.; Katiyar, V. State of Art on Solvent Casting Particulate Leaching Method for Orthopedic ScaffoldsFabrication. Mater. Today Proc. 2017, 4, 898–907. [Google Scholar] [CrossRef]
- Sigaux, N.; Pourchet, L.; Breton, P.; Brosset, S.; Louvrier, A.; Marquette, C. 3D Bioprinting:principles, fantasies and prospects. J. Stomatol. Oral Maxillofac. Surg. 2019, 120, 128–132. [Google Scholar] [CrossRef] [PubMed]
- Jammalamadaka, U.; Tappa, K. Recent Advances in Biomaterials for 3D Printing and Tissue Engineering. J. Funct. Biomater. 2018, 9, 22. [Google Scholar] [CrossRef] [PubMed]
- Moroni, L.; Burdick, J.A.; Highley, C.; Lee, S.J.; Morimoto, Y.; Takeuchi, S.; Yoo, J.J. Biofabrication Strategies for 3D in Vitro Models and Regenerative Medicine. Nat. Rev. Mater. 2018, 3, 21–37. [Google Scholar] [CrossRef] [PubMed]
- Javaid, M.; Haleem, A. 3D bioprinting applications for the printing of skin: A brief study. Sens. Int. 2021, 2, 100123. [Google Scholar] [CrossRef]
- Mabrouk, M.; Beherei, H.H.; Das, D.B. Recent progress in the fabrication techniques of 3D scaffolds for tissue engineering. Mater. Sci. Eng. C 2020, 110, 110716. [Google Scholar] [CrossRef]
- Tan, S.H.; Ngo, Z.H.; Sci, D.B.; Leavesley, D.I.; Liang, K. Recent Advances in the Design of Three-Dimensional and Bioprinted Scaffolds for Full-Thickness Wound Healing. Tissue Eng. Part B Rev. 2022, 28, 160–181. [Google Scholar] [CrossRef] [PubMed]
- Gu, Z.; Fu, J.; Lin, H.; He, Y. Development of 3D bioprinting: From printing methods to biomedical applications. Asian J. Pharm. Sci. 2019, 15, 529–557. [Google Scholar] [CrossRef] [PubMed]
- Weng, T.; Zhang, W.; Xia, Y.; Wu, P.; Yang, M.; Jin, R.; Xia, S.; Wang, J.; You, C.; Han, C.; et al. 3D bioprinting for skin tissue engineering: Current status and perspectives. J. Tissue Eng. 2021, 12, 20417314211028574. [Google Scholar] [CrossRef] [PubMed]
- Ozbolat, I.T.; Hospodiuk, M. Current advances and future perspectives in extrusion-based bioprinting. Biomaterials 2016, 76, 321–343. [Google Scholar] [CrossRef]
- Li, X.; Liu, B.; Pei, B.; Chen, J.; Zhou, D.; Peng, J.; Zhang, X.; Jia, W.; Xu, T. Inkjet Bioprinting of Biomaterials. Chem. Rev. 2020, 120, 10793–10833. [Google Scholar] [CrossRef]
- Koch, L.; Gruene, M.; Unger, C.; Chichkov, B. Laser Assisted Cell Printing. Curr. Pharm. Biotechnol. 2013, 14, 91–97. [Google Scholar]
- Mkhize, N.; Bhaskaran, H. Electrohydrodynamic Jet Printing: Introductory Concepts and Considerations. Small Sci. 2021, 2, 2100073. [Google Scholar] [CrossRef]
- de Armentia, S.L.; Fernández-Villamarín, S.; Ballesteros, Y.; del Real, J.C.; Dunne, N.; Paz, E. 3D Printing of a Graphene-Modified Photopolymer Using Stereolithography for Biomedical Applications: A Study of the Polymerization Reaction. Int. J. Bioprinting 2022, 8, 182–197. [Google Scholar] [CrossRef]
- Heinrich, M.A.; Liu, W.; Jimenez, A.; Yang, J.; Akpek, A.; Liu, X.; Pi, Q.; Mu, X.; Hu, N.; Schiffelers, R.M.; et al. 3D Bioprinting: From Benches to Translational Applications. Small 2019, 15, e1805510. [Google Scholar] [CrossRef]
- Seo, J.W.; Kim, G.M.; Choi, Y.; Cha, J.M.; Bae, H. Improving Printability of Digital-Light-Processing 3D Bioprinting via Photoabsorber Pigment Adjustment. Int. J. Mol. Sci. 2022, 23, 5428. [Google Scholar] [CrossRef]
- Li, Q.; Zhang, B.; Xue, Q.; Zhao, C.; Luo, Y.; Zhou, H.; Ma, L.; Yang, H.; Bai, D. A Systematic Thermal Analysis for Accurately Predicting the Extrusion Printability of Alginate-Gelatin-Based Hydrogel Bioinks. Int. J. Bioprinting 2021, 7, 108–123. [Google Scholar] [CrossRef]
- Matai, I.; Kaur, G.; Seyedsalehi, A.; McClinton, A.; Laurencin, C.T. Progress in 3D bioprinting technology for tissue/organ regenerative engineering. Biomaterials 2020, 226, 119536. [Google Scholar] [CrossRef] [PubMed]
- Manapat, J.Z.; Chen, Q.; Ye, P.; Advincula, R.C. 3D Printing of Polymer Nanocomposites via Stereolithography. Macromol. Mater. Eng. 2017, 302, 1600553. [Google Scholar] [CrossRef]
- Zhou, D.; Chen, J.; Liu, B.; Zhang, X.; Li, X.; Xu, T. Bioinks for jet-based bioprinting. Bioprinting 2019, 16, e00060. [Google Scholar] [CrossRef]
- Wu, D.; Xu, C. Predictive Modeling of Droplet Formation Processes in Inkjet-Based Bioprinting. J. Manuf. Sci. Eng. 2018, 140, 101007. [Google Scholar] [CrossRef]
- Dou, C.; Perez, V.; Qu, J.; Tsin, A.; Xu, B.; Li, J. A State-of-the-Art Review of Laser-Assisted Bioprinting and its Future Research Trends. ChemBioEng Rev. 2021, 8, 517–534. [Google Scholar] [CrossRef]
- Lei, Q.; He, J.; Li, D. Electrohydrodynamic 3D printing of layer-specifically oriented, multiscale conductive scaffolds for cardiac tissue engineering. Nanoscale 2019, 11, 15195–15205. [Google Scholar] [CrossRef]
- Lin, Y.; Huang, Y.; Chrisey, D.B. Metallic Foil-Assisted Laser Cell Printing. J. Biomech. Eng. 2011, 133, 025001. [Google Scholar] [CrossRef]
- Brown, M.S.; Kattamis, N.T.; Arnold, C.B. Time-resolved study of polyimide absorption layers for blister-actuated laser-induced forward transfer. J. Appl. Phys. 2010, 107, 083103. [Google Scholar] [CrossRef]
- Simulation and Validation of Droplet Generation Process for Revealing Three Design Constraints in Electrohydrodynamic Jet Printing. Micromachines 2019, 10, 94. [CrossRef]
- Ning, L.; Chen, X. A brief review of extrusion-based tissue scaffold bio-printing. Biotechnol. J. 2017, 12, 1600671. [Google Scholar] [CrossRef] [PubMed]
- Tian, S.; Zhao, H.; Lewinski, N. Key parameters and applications of extrusion-based bioprinting. Bioprinting 2021, 23, e00156. [Google Scholar] [CrossRef]
- Raja, I.S.; Kang, M.S.; Hong, S.W.; Bae, H.; Kim, B.; Hwang, Y.-S.; Cha, J.M.; Han, D.-W. State-of-the-art techniques for promoting tissue regeneration: Combination of three-dimensional bioprinting and carbon nanomaterials. Int. J. Bioprinting 2022, 9, 181–198. [Google Scholar] [CrossRef]
- Ali, A.S.; Wu, D.; Bannach-Brown, A.; Dhamrait, D.; Berg, J.; Tolksdorf, B.; Lichtenstein, D.; Dressler, C.; Braeuning, A.; Kurreck, J.; et al. 3D bioprinting of liver models: A systematic scoping review of methods, bioinks, and reporting quality. Mater. Today Bio 2024, 26, 100991. [Google Scholar] [CrossRef]
- Kyle, S.; Jessop, Z.M.; Al-Sabah, A.; Whitaker, I.S. ‘Printability’ of Candidate Biomaterials for Extrusion Based 3D Printing: State-of-the-Art. Adv. Healthc. Mater. 2017, 6, 1700264. [Google Scholar] [CrossRef]
- Gopinathan, J.; Noh, I. Recent trends in bioinks for 3D printing. Biomater. Res. 2018, 22, 11. [Google Scholar] [CrossRef] [PubMed]
- Deptuła, M.; Zawrzykraj, M.; Sawicka, J.; Banach-Kopeć, A.; Tylingo, R.; Pikuła, M. Application of 3D- printed hydrogels in wound healing and regenerative medicine. Biomed. Pharmacother. 2023, 167, 115416. [Google Scholar] [CrossRef]
- Masri, S.; Zawani, M.; Zulkiflee, I.; Salleh, A.; Fadilah, N.I.M.; Maarof, M.; Wen, A.P.Y.; Duman, F.; Tabata, Y.; Aziz, I.A.; et al. Cellular Interaction of Human Skin Cells towards Natural Bioink via 3D-Bioprinting Technologies for Chronic Wound: A Comprehensive Review. Int. J. Mol. Sci. 2022, 23, 476. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.D.J.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Évid. Synth. 2020, 18, 2119–2126. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Schmitt, T.; Katz, N.; Kishore, V. A Feasibility Study on 3D Bioprinting of Microfat Constructs Towards Wound Healing Applications. Front. Bioeng. Biotechnol. 2021, 9, 707098. [Google Scholar] [CrossRef] [PubMed]
- Manso, G.M.d.C.; Elias-Oliveira, J.; Guimarães, J.B.; Pereira, S.; Rodrigues, V.F.; Burger, B.; Fantacini, D.M.C.; de Souza, L.E.B.; Rodrigues, H.G.; Bonato, V.L.D.; et al. Xenogeneic mesenchymal stem cell biocurative improves skin wounds healing in diabetic mice by increasing mast cells and the regenerative profile. Regen. Ther. 2023, 22, 79–89. [Google Scholar] [CrossRef]
- Bajuri, M.Y.; Kim, J.; Yu, Y.; Hameed, M.S.S. New Paradigm in Diabetic Foot Ulcer Grafting Techniques Using 3D-Bioprinted Autologous Minimally Manipulated Homologous Adipose Tissue (3D-AMHAT) with Fibrin Gel Acting as a Biodegradable Scaffold. Gels 2023, 9, 66. [Google Scholar] [CrossRef] [PubMed]
- Ullah, F.; Javed, F.; Mushtaq, I.; Rahman, L.-U.; Ahmed, N.; Din, I.U.; Alotaibi, M.A.; Alharthi, A.I.; Ahmad, A.; Bakht, M.A.; et al. Development of highly-reproducible hydrogel based bioink for regeneration of skin-tissues via 3-D bioprinting technology. Int. J. Biol. Macromol. 2023, 230, 123131. [Google Scholar] [CrossRef] [PubMed]
- Xia, S.; Weng, T.; Jin, R.; Yang, M.; Yu, M.; Zhang, W.; Wang, X.; Han, C. Curcumin-incorporated 3D bioprinting gelatin methacryloyl hydrogel reduces reactive oxygen species-induced adipose-derived stem cell apoptosis and improves implanting survival in diabetic wounds. Burn. Trauma 2022, 10, tkac001. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Qin, C.; Wu, J.; Zhang, H.; Zhuang, H.; Zhang, M.; Zhang, Z.; Ma, L.; Wang, X.; Ma, B.; et al. 3D Printing of Strontium Silicate Microcylinder-Containing Multicellular Biomaterial Inks for Vascularized Skin Regeneration. Adv. Healthc. Mater. 2021, 10, 2100523. [Google Scholar] [CrossRef]
- Masri, S.; Fadilah, N.I.M.; Hao, L.Q.; Maarof, M.; Tabata, Y.; Hiraoka, Y.; Fauzi, M.B. Multifunctionalised skin substitute of hybrid gelatin-polyvinyl alcohol bioinks for chronic wound: Injectable vs. 3D bioprinting. Drug Deliv. Transl. Res. 2023, 14, 1005–1027. [Google Scholar] [CrossRef]
- Masri, S.; Maarof, M.; Aziz, I.A.; Idrus, R.; Fauzi, M.B. Performance of hybrid gelatin-PVA bioinks integrated with genipin through extrusionbased 3D bioprinting: An in vitro evaluation using human dermal fibroblasts. Int. J. Bioprinting 2023, 9, 422–442. [Google Scholar] [CrossRef]
- Albanna, M.; Binder, K.W.; Murphy, S.V.; Kim, J.; Qasem, S.A.; Zhao, W.; Tan, J.; El-Amin, I.B.; Dice, D.D.; Marco, J.; et al. In Situ Bioprinting of Autologous Skin Cells Accelerates Wound Healing of Extensive Excisional Full-Thickness Wounds. Sci. Rep. 2019, 9, 1–15. [Google Scholar] [CrossRef]
- Negut, I.; Dorcioman, G.; Grumezescu, V. Scaffolds for Wound Healing Applications. Polymers 2020, 12, 2010. [Google Scholar] [CrossRef] [PubMed]
- Aazmi, A.; Zhang, D.; Mazzaglia, C.; Yu, M.; Wang, Z.; Yang, H.; Huang, Y.Y.S.; Ma, L. Biofabrication methods for reconstructing extracellular matrix mimetics. Bioact. Mater. 2024, 31, 475–496. [Google Scholar] [CrossRef]
- Da Silva, K.; Kumar, P.; Choonara, Y.E.; du Toit, L.C.; Pillay, V. Three-dimensional printing of extracellular matrix (ECM)-mimicking scaffolds: A critical review of the currentECMmaterials. J. Biomed. Mater. Res. Part A 2020, 108, 2324–2350. [Google Scholar] [CrossRef] [PubMed]
- Schwab, A.; Levato, R.; D’este, M.; Piluso, S.; Eglin, D.; Malda, J. Printability and Shape Fidelity of Bioinks in 3D Bioprinting. Chem. Rev. 2020, 120, 11028–11055. [Google Scholar] [CrossRef]
- Teixeira, M.C.; Lameirinhas, N.S.; Carvalho, J.P.F.; Valente, B.F.A.; Luís, J.; Pires, L.; Oliveira, H.; Oliveira, M.; Silvestre, A.J.D.; Vilela, C.; et al. Alginate-Lysozyme Nanofibers Hydrogels with Improved Rheological Behavior, Printability and Biological Properties for 3D Bioprinting Applications. Nanomaterials 2022, 12, 2190. [Google Scholar] [CrossRef]
- Khoeini, R.; Nosrati, H.; Akbarzadeh, A.; Eftekhari, A.; Kavetskyy, T.; Khalilov, R.; Ahmadian, E.; Nasibova, A.; Datta, P.; Roshangar, L.; et al. Natural and Synthetic Bioinks for 3D Bioprinting. Adv. NanoBiomed Res. 2021, 1, 2000097. [Google Scholar] [CrossRef]
- Mao, H.; Yang, L.; Zhu, H.; Wu, L.; Ji, P.; Yang, J.; Gu, Z. Recent advances and challenges in materials for 3D bioprinting. Prog. Nat. Sci. 2020, 30, 618–634. [Google Scholar] [CrossRef]
- Lee, S.C.; Gillispie, G.; Prim, P.; Lee, S.J. Physical and Chemical Factors Influencing the Printability of Hydrogel-based Extrusion Bioinks. Chem. Rev. 2020, 120, 10834–10886. [Google Scholar] [CrossRef]
- Kiyotake, E.A.; Douglas, A.W.; Thomas, E.E.; Nimmo, S.L.; Detamore, M.S. Development and quantitative characterization of the precursor rheology of hyaluronic acid hydrogels for bioprinting. Acta Biomater. 2019, 95, 176–187. [Google Scholar] [CrossRef]
- Shie, M.-Y.; Lee, J.-J.; Ho, C.-C.; Yen, S.-Y.; Ng, H.Y.; Chen, Y.-W. Effects of Gelatin Methacrylate Bio-ink Concentration on Mechano-Physical Properties and Human Dermal Fibroblast Behavior. Polymers 2020, 12, 1930. [Google Scholar] [CrossRef]
- Wang, Y.; Yuan, X.; Yao, B.; Zhu, S.; Zhu, P.; Huang, S. Tailoring bioinks of extrusion-based bioprinting for cutaneous wound healing. Bioact. Mater. 2022, 17, 178–194. [Google Scholar] [CrossRef]
- Wang, C.-Y.; Chiu, Y.-C.; Lee, A.K.-X.; Lin, Y.-A.; Lin, P.-Y.; Shie, M.-Y. Biofabrication of Gingival Fibroblast Cell-Laden Collagen/Strontium-Doped Calcium Silicate 3D-Printed Bi-Layered Scaffold for Osteoporotic Periodontal Regeneration. Biomedicines 2021, 9, 431. [Google Scholar] [CrossRef] [PubMed]
- Ding, X.; Yu, Y.; Li, W.; Zhao, Y. In situ 3D-bioprinting MoS2 accelerated gelling hydrogel scaffold for promoting chronic diabetic wound healing. Matter 2023, 6, 1000–1014. [Google Scholar] [CrossRef]
- Kim, J. Characterization of Biocompatibility of Functional Bioinks for 3D Bioprinting. Bioengineering 2023, 10, 457. [Google Scholar] [CrossRef]
- Maniţă, P.G.; García-Orue, I.; Santos-Vizcaíno, E.; Hernández, R.M.; Igartua, M. 3D Bioprinting of Functional Skin Substitutes for Chronic Wound Treatment: From Current Achievements to Future Goals. SSRN Electron. J. 2020. [Google Scholar] [CrossRef]
- Turner, P.R.; Murray, E.; McAdam, C.J.; McConnell, M.A.; Cabral, J.D. Peptide Chitosan/Dextran Core/Shell Vascularized 3D Constructs for Wound Healing. ACS Appl. Mater. Interfaces 2020, 12, 32328–32339. [Google Scholar] [CrossRef] [PubMed]
- Jara, C.P.; Nogueira, G.; Morari, J.; Prado, T.P.D.; Bezerra, R.d.M.; Velloso, L.A.; Velander, W.; de Araújo, E.P. An older diabetes-induced mice model for studying skin wound healing. PLoS ONE 2023, 18, e0281373. [Google Scholar] [CrossRef]
- Levin, A.A.; Karalkin, P.A.; Koudan, E.V.; Senatov, F.S.; Parfenov, V.A.; Lvov, V.A.; Petrov, S.V.; Pereira, F.D.A.S.; Kovalev, A.V.; Osidak, E.O.; et al. Commercial articulated collaborative in situ 3D bioprinter for skin wound healing. Int. J. Bioprinting 2023, 9, 380–393. [Google Scholar] [CrossRef]
- Palma, M.B.; Paolin, E.; de Melo, I.M.F.; Souza, F.D.A.L.; Teixeira, A.C.; Vieira, L.D.; Naro, F.; Graziano, A.; Soares, A.F. Biological Evidence of Improved Wound Healing Using Autologous Micrografts in a Diabetic Animal Model. Diabetology 2023, 4, 294–311. [Google Scholar] [CrossRef]
- Mohammadrezaei, D.; Podina, L.; Silva, J.D.; Kohandel, M. Cell Viability Prediction and Optimization in Extrusion-Based Bi-oprinting via Neural Network-Based Bayesian Optimization Models. Biofabrication 2024, 16, 025016. [Google Scholar] [CrossRef]
- Ma, Y.; Deng, B.; He, R.; Huang, P. Advancements of 3D bioprinting in regenerative medicine: Exploring cell sources for organ fabrication. Heliyon 2024, 10, e24593. [Google Scholar] [CrossRef] [PubMed]
- Apelgren, P.; Amoroso, M.; Säljö, K.; Lindahl, A.; Brantsing, C.; Orrhult, L.S.; Markstedt, K.; Gatenholm, P.; Kölby, L. Long-term in vivo integrity and safety of 3D-bioprinted cartilaginous constructs. J. Biomed. Mater. Res. Part B Appl. Biomater. 2020, 109, 126–136. [Google Scholar] [CrossRef] [PubMed]
- Yaneva, A.; Shopova, D.; Bakova, D.; Mihaylova, A.; Kasnakova, P.; Hristozova, M.; Semerdjieva, M. The Progress in Bioprinting and Its Potential Impact on Health-Related Quality of Life. Bioengineering 2023, 10, 910. [Google Scholar] [CrossRef] [PubMed]
- Alzoubi, L.; Aljabali, A.A.A.; Tambuwala, M.M. Empowering Precision Medicine: The Impact of 3D Printing on Personalized Therapeutic. AAPS PharmSciTech 2023, 24, 228. [Google Scholar] [CrossRef]
- Mamo, H.B.; Adamiak, M.; Kunwar, A. 3D printed biomedical devices and their applications: A review on state-of-the-art technologies, existing challenges, and future perspectives. J. Mech. Behav. Biomed. Mater. 2023, 143, 105930. [Google Scholar] [CrossRef]
- Ramezani, M.; Ripin, Z.M. 4D Printing in Biomedical Engineering: Advancements, Challenges, and Future Directions. J. Funct. Biomater. 2023, 14, 347. [Google Scholar] [CrossRef]
| No. | Study | Country | Study Design | 3D Bioprinting Technique | Bioink Components | Wound Type | Assay Conducted | Key Outcomes | Study Limitations |
|---|---|---|---|---|---|---|---|---|---|
| 1 | [52] | USA | In vitro | Extrusion | Methacrylated Collagen (CMA) | Chronic wounds | Alamar blue assay | Sustained cytokine release, High cell viability, maintained print fidelity and stability | Limited in vivo data |
| 2 | [53] | Brazil | In vivo | Extrusion | Alginate Hydrogel | Chronic diabetic ulcers | Bioluminescence assay | Accelerated wound healing, increased mast cells, improved regenerative profile | Short-term study, limited to mice |
| 3 | [54] | Malaysia | Single-arm pilot study | Extrusion | Fibrin gel | Diabetic foot ulcers | Not stated (Clinical study) | 70% complete healing within 12 weeks, significant wound size reduction, no adverse events | Small sample size, lack of control group, short follow-up period |
| 4 | [55] | Pakistan | In vivo | Extrusion | polyethylene oxide-co-Chitosan-co-poly (methylmethacrylic acid) (PEO-CS-PMMA), Nicotinamide | Full-thickness skin defect | Not stated | High reproducibility, improved mechanical properties, increased cell viability | lack of detailed methodology and analysis of biological interactions |
| 5 | [56] | China | In vitro and in vivo | Extrusion | Gelatin methacryloyl (GelMA), Curcumin | Diabetic wounds | Live/dead assay Apoptosis assay Western blot Caspase-3 activity assay | Reduced ROS, decreased apoptosis; improved ADSC cell survival, accelerated wound healing | Limited in vivo studies, need for long-term analysis, lack of comparison with other materials |
| 6 | [57] | China | In vitro and in vivo | Extrusion | SS-GAM (Strontium Silicate-Gellan Gum-Sodium Alginate—Methyl Cellulose) | Acute and chronic wounds | Live/dead assay Proliferation assay | Blood vessel formation, graft-host integration, enhanced cell proliferation, wound repair in vivo | short-term study |
| 7 | [58] | Malaysia | In vitro | Extrusion | Gelatin, Polyvinyl alcohol (PVA), Genipin | Potential for Chronic wounds | Live/dead assay Cell proliferation assay 3D cell migration In vitro wound scratch assay Immunocytochemistry DPPH and ABTS assay | Improved printability, high cell viability, increased wound healing rates | Limited in vivo studies, need for comparison with other materials |
| 8 | [59] | Malaysia | In vitro | Extrusion | Gelatin, Polyvinyl alcohol (PVA), Genipin | Potential for Chronic wounds | Live/dead assay Proliferation assay Scratch wound assays | Improved rheological properties, high cell viability (>90%), enhanced wound healing, reduced inflammation, optimal WVTR, slow biodegradation rate | Limited in vivo studies |
| 9 | [60] | USA | In vivo | Mobile in situ skin inkjet-based bioprinting with integrated imaging technology | Fibrin gel: fibrinogen- collagen | Acute and chronic wounds | Not stated | Improved wound closure, re-epithelialization, reduced contraction, formation of healthy, mature skin | potential for variability in outcomes due to the manual aspects of the bioprinting process and the limited sample size |
| Study | Cell-Laden Bioink | Type of Polymer | 3D Bioprinter Model | 3D Bioprinting Technique | Type of Construct | Nozzle Size (mm) | Printing Speed (mm/s) | Printing Pressure (kPa) | Crosslinking Method | Printing Environment | Printing Shape | Crosslink Time (Min) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| [52] | Microfat-laden Methacrylated Collagen (CMA) | Natural | REGEMAT3D (Granada, Spain) | Extrusion | Collagen construct | 0.965 | 5 | Not Available | UV crosslinking | Room temperature | Cube | 1 |
| [53] | MSCs-Laden Alginate Hydrogel | Natural | Available by the startup In Situ Cell Therapy | Extrusion | Hydrogel | Not Available | Not Available | Not Available | Not Available | Not Available | Not Available | Not Available |
| [54] | Autologous adipose tissue and fibrin gel | Natural | Dr. INVIVO clean chamber 3D bioprinter (ROKIT Healthcare, Seoul, Republic of Korea) | Extrusion | Graft | Not Available | Not Available | Not Available | Fibrin gel crosslinking | Clean chamber | According to wound size | Not Available |
| [55] | Fibroblast-PEO-CS-PMMA | Synthetic | Not Available | Extrusion | Hydrogel | 0.25 | 5–8 | 20–45 | Thermal initiation and chemical crosslinking with carbohydrazide (CH) | 37 °C | Skin-tissue constructs | 600 |
| [56] | ADSCs (Adipose-Derived Stem Cells)-Gelatin Methacryloyl (GelMA) | Natural | BioArchitect Pro (Regenovo, Hangzhou, China) | Extrusion | Hydrogel | 0.21 | 5 | 200 | Blue light | 20 °C nozzle, 18 °C platform | Circular mesh structure | 0.33–0.5 |
| [57] | HDF-HUVEC-GAM-SS | Natural | BioScaffolder 3.2 (GeSiM, Radeberg, Germany) | Extrusion | Hydrogel | 0.25 | Not Available | 230–280 | Ionic crosslinking with 1.6% CaCl2 | Room temperature | hexagonal prism, 8mm side length, 1.4mm thickness | 60 |
| [58] | HDF-Gelatin-PVA | Hybrid (Natural and Synthetic) | Biogens XI (3D Gens, Shah Alam, Malaysia) | Extrusion | Hydrogel | 0.3 | 5–10 | 150–200 | Chemical crosslinking with Genipin | 23 ± 2 °C, Sterile | Layer-by-layer 3D structures, Grid-like patterns | 3 |
| [59] | HDF-Gelatin-PVA | Hybrid (Natural and Synthetic) | Biogens XI (3D Gens, Malaysia) | Extrusion | Hydrogel | 0.3 | 4000 | Not Available | Chemical crosslinking with Genipin | 23 ± 2 °C, Sterile | Grid-like patterns, 2.5 cm × 0.3 mm | Not Available |
| [60] | Fibroblasts-Keratinocytes-Fibrin Gel | Fibrinogen, collagen Natural | Custom-designed mobile bioprinter | inkjet | Hydrogel | 0.26 | 1130.09–9417.45 | 6.89 | Chemical crosslinking with Thrombin-induced gelation | Sterile, mobile operating room setup | Tailored to individual wound topography | 15 |
| Study | Cell-Laden Bioink | Cell Type | Cell Density | Max Cell Viability (%) | Bioink Preparation Method | Bioink Properties (e.g., Viscosity, Stiffness) | Biodegradability |
|---|---|---|---|---|---|---|---|
| [52] | Microfat-laden methacrylated collagen (CMA) | Adipose stromal cells (ASCs), Endothelial progenitor cells (EPCs) | 1 × 106 cells/gram | maintained for up to 10 days | Mixing | Not specified | Not specified |
| [53] | MSCs- Laden Alginate Hydrogel | Mesenchymal stem cells (MSCs, derived from the human umbilical cord) | 1 × 105 cells/cm² | Not specified | Mixing | Not specified | Not specified |
| [54] | Autologous adipose tissue and fibrin gel | Adipose stem cells | Not specified | Not specified | Mixed autologous adipose tissue with fibrin gel | Not specified | Biodegradable scaffold |
| [55] | Fibroblast-PEO-CS-PMMA Nicotinamide | Human Dermal Fibroblasts (HDFs) | 0.1 × 106 cells/mL | 92% | Free radical copolymerization | Viscosity: 500–550 Pa·s, Thermal stability | 85% weight loss |
| [56] | Gelatin methacryloyl (GelMA), Curcumin | Adipose-derived stem cells (ADSCs) | 5 × 105 cells/mL | 90% | Mixing ADSCs with GelMA and Cur, crosslinked with blue light | High porosity, suitable mechanical properties | Yes |
| [57] | Strontium silicate microcylinders, Alginate, Gelatin | human umbilical vascular endothelial cells (HUVECs), human dermal fibroblasts (HDFs), murine umbilical vein endothelial cells (MUVEC), BALB/3T3 fibroblast | 1 × 104 cells/mL | Not specified | Mixing and ionic crosslinking | High viscosity, cell adhesion, high cellular activity, excellent proliferation, good mechanical strength | Not specified |
| [58] | HDF-Gelatin,(PVA) | Human dermal fibroblasts (HDFs) | 1.5 × 106 cells/mL | >90% | Mixed cells with hydrogel, chemical crosslinking with genipin | Appropriate mechanical properties, high porosity | 0.02 ± 0.005 mg/h |
| [59] | HDF-Gelatin-PVA | Human dermal fibroblasts (HDFs) | 1.5 × 106 cells/mL | >90% | Mixed cells with hydrogel, chemical crosslinking with genipin | High viscosity, optimal WVTR, slow biodegradation rate, excellent interconnected porosity, achieve optimum printability | Slow, 0.018 ± 0.08 mg/h |
| [60] | Fibroblasts-Keratinocytes- Fibrin Gel | Dermal fibroblasts, epidermal keratinocytes | 3.75 × 106 cells/mL fibroblasts, 7.5 × 106 cells/mL keratinocytes | High viability | Fibrinogen/collagen solution with cells printed directly onto the wound, followed by thrombin printing to form a gel | Suitable support for cellular viability, rapid crosslinking | Not specified |
| Study | Objective/Novelty | Print Fidelity and Stability | Biological Functionality | Additional Findings |
|---|---|---|---|---|
| [52] | First application of 3D bioprinting using microfat tissue with a collagen-based bioink | Maintained over time | Release proinflammatory cytokines, Temporal release of IL-6, IL-8, FGF-2, supports wound healing | Potential for weekly application of custom-designed autologous microfat grafts with bandage changes |
| [53] | Use of xenogeneic MSCs in biocuratives | Stable in the wound environment | Promotes M2 macrophage polarization, supports wound healing, promotes an anti-inflammatory environment (Increased TGF-β, IL-33, M2 markers) | Potential for restoring mast cells in diabetic skin |
| [54] | Use of 3D-AMHAT with fibrin gel for diabetic foot ulcers (DFUs) | High print fidelity and stability | Promoted wound healing with high-quality skin reconstruction | Significant wound size reduction, no adverse events, enhanced quality of healed skin |
| [55] | Use of PEO-CS-PMMA bioink with nicotinamide for skin regeneration | High print fidelity and stability | Enhanced skin regeneration | Effective DNA interaction |
| [56] | First study to incorporate curcumin in a 3D printed GelMA scaffold for diabetic wound healing | High print fidelity and stability | Reduced ROS, decreased apoptosis, improved ADSC survival, improved wound healing | Curcumin significantly downregulated AGER and inhibited ROS production and apoptosis in ADSCs |
| [57] | Combination of strontium silicate (SS) with bioink for vascularized skin regeneration | High print fidelity and stability | Enhanced cell proliferation, increased expression of angiogenic genes (VEGF, VE-cad, HIF-1α, eNOS-1), blood vessel formation, graft-host integration, and skin reconstruction | Improved mechanical properties |
| [58] | Comparison of injectable vs. 3D bioprinted hydrogels | High print fidelity and stability | Enhanced wound healing, antioxidant properties, improved cell migration, Promoted cell proliferation and adhesion | High antioxidant capacity |
| [59] | Detailed evaluation of hybrid bioinks’ physicochemical properties | High print fidelity and stability | Enhanced wound healing, antioxidant properties, improved cell migration, Promoted cell proliferation | Improved rheological properties, High antioxidant capacity, optimal WVTR, slow biodegradation rate, suitable for wound healing |
| [60] | Use of a mobile bioprinter with integrated imaging technology to create bilayered skin constructs directly on wounds, potentially improving wound healing outcomes compared to traditional methods. | High-precision delivery to specific locations of the wound | Rapid wound closure, formation of normal skin, reduced contraction | Early formation of defined epidermis and mature dermis layers in bioprinted wounds compared to cell-sprayed wounds |
| Study | Model | Sex | Age | Defect Area | Defect Size (cm2) | Time of Sacrifice (days) | Health Status | Post-Operative Care |
|---|---|---|---|---|---|---|---|---|
| [53] | C57BL/6 mice | >24 Male | 8 weeks | Dorsal surface, Back skin | 1 cm2 | 15 Days | Diabetic (T1D) induced by STZ | The pathogen-free condition housing room was set to a 12 h light/dark cycle with a temperature of about 22 °C |
| [54] | patients | Seven male, three female | 48.7 ± 14.9 year | Foot ulcers | 27.00 ± 43.99 cm2 | Not applicable | Type II diabetes mellitus | 12 weeks of follow-up. No keloid formation, scarring, tissue contracture, or infection noted |
| [56] | Nu/nu athymic nude mice | 30 mice, Not specified | 6 weeks | Dorsal surface/Full skin defect | 1.5 cm2 | 14 and 21 days | diabetic (STZ-induced) | Covered with Vaseline gauze and transparent film, changed every 2 days |
| [57] | C57BL/6 mice | 25 Male | 7–8 weeks | Dorsal surface | 1.5 cm2 diameter, circular full thickness | 15 days | Diabetic (T1D) induced by STZ | The wound site was covered by a scaffold and bound up by sterile gauze and medical transparent dressing |
| [60] | outbred athymic Nu/nu nude mice, Specific Pathogen Free (SPF) Yorkshire pigs | 36 female mice, six pigs | Not specified | Dorsal surface | 7.5 cm2 for murine model, 100 cm2 for porcine model | 6 weeks for a murine model; 8 weeks for a porcine model | Specific Pathogen Free (SPF) Yorkshire pigs, female outbred athymic nude (Nu/nu) mice | Bandaging with sterile gauze and surgical tape, dressing changes every 3 days under anesthesia |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abuhamad, A.Y.; Masri, S.; Fadilah, N.I.M.; Alamassi, M.N.; Maarof, M.; Fauzi, M.B. Application of 3D-Printed Bioinks in Chronic Wound Healing: A Scoping Review. Polymers 2024, 16, 2456. https://doi.org/10.3390/polym16172456
Abuhamad AY, Masri S, Fadilah NIM, Alamassi MN, Maarof M, Fauzi MB. Application of 3D-Printed Bioinks in Chronic Wound Healing: A Scoping Review. Polymers. 2024; 16(17):2456. https://doi.org/10.3390/polym16172456
Chicago/Turabian StyleAbuhamad, Asmaa Y., Syafira Masri, Nur Izzah Md Fadilah, Mohammed Numan Alamassi, Manira Maarof, and Mh Busra Fauzi. 2024. "Application of 3D-Printed Bioinks in Chronic Wound Healing: A Scoping Review" Polymers 16, no. 17: 2456. https://doi.org/10.3390/polym16172456