
Going Micro in Leptospirosis Kidney Disease

 ,
,  and
and
Abstract
:1. Introduction
2. Epidemiology
3. Pathophysiology
3.1. Acute Kidney Injury in Leptospirosis
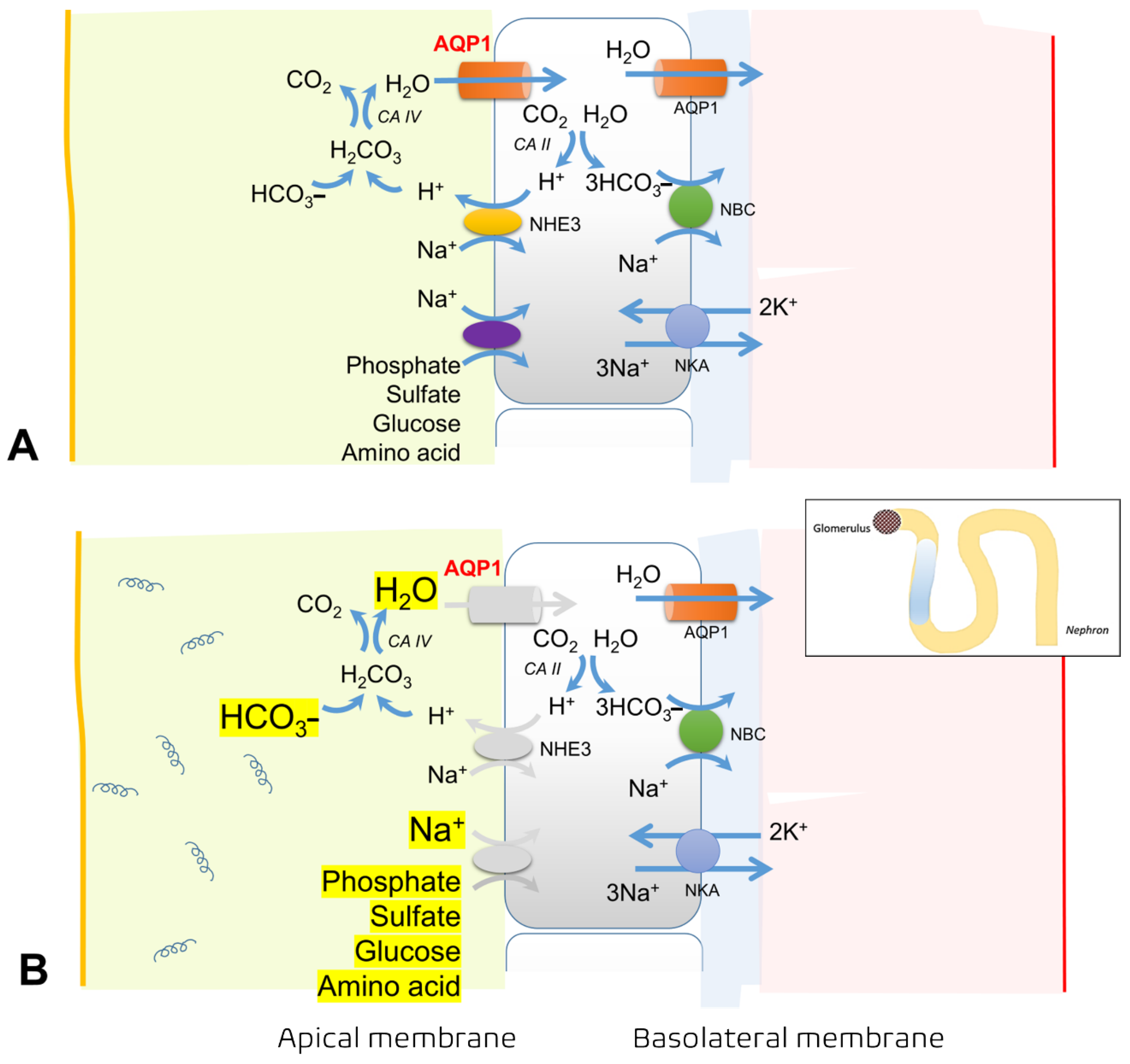
Tubular Dysfunction and Related Electrolyte Disturbances
3.2. Leptospirosis with Systemic Inflammatory Response Syndrome (SIRS)
3.3. Chronic Kidney Disease in Leptospirosis
4. Host Immunity Responses to Leptospira spp.
4.1. Leptospira and the Complement System
4.2. Leptospira and Neutrophils
4.3. Leptospira and Macrophages
4.4. Humoral Response to Leptospira
4.5. Adaptive Immune Response to Leptospira: T-Cells and Cytokines
5. Clinical Manifestations
6. Diagnosis
6.1. Clinical Diagnosis
6.2. Laboratory Diagnosis
6.2.1. Direct Microscopic Examination, Culture, and Antigen Detection
6.2.2. Anti-Leptospira Antibody Detection
7. Prognosis and Mortality
8. Treatments
8.1. Specific Treatments for Leptospirosis
8.2. Sepsis and Organ Failure in Leptospirosis
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tulsiani, S.M.; Lau, C.L.; Graham, G.C.; Van Den Hurk, A.F.; Jansen, C.C.; Smythe, L.D.; McKay, D.B.; Craig, S.B. Emerging tropical diseases in Australia. Part 1. Leptospirosis. Ann. Trop. Med. Parasitol. 2010, 104, 543–556. [Google Scholar] [CrossRef] [PubMed]
- Hinjoy, S.; Kongyu, S.; Doung-Ngern, P.; Doungchawee, G.; Colombe, S.D.; Tsukayama, R.; Suwancharoen, D. Environmental and behavioral risk factors for severe leptospirosis in Thailand. Trop. Med. Infect. Dis. 2019, 4, 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lau, C.L.; Townell, N.; Stephenson, E.; van den Berg, D.; Craig, S.B. Leptospirosis: An important zoonosis acquired through work, play and travel. Aust. J. Gen. Pract. 2018, 47, 105–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carter, M.E.; Cordes, D.O. Leptospirosis and other infections of Battus rattus and Rattus norvegicus. N. Z. Vet. J. 1980, 28, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.W.; Hung, C.C.; Wu, M.S.; Tian, Y.C.; Chang, C.T.; Pan, M.J.; Vandewalle, A. Toll-like receptor 2 mediates early inflammation by leptospiral outer membrane proteins in proximal tubule cells. Kidney Int. 2006, 69, 815–822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Budihal, S.V.; Perwez, K. Leptospirosis diagnosis: Competancy of various laboratory tests. J. Clin. Diagn. Res. 2014, 8, 199–202. [Google Scholar] [CrossRef]
- Costa, F.; Hagan, J.E.; Calcagno, J.; Kane, M.; Torgerson, P.; Martinez-Silveira, M.S.; Stein, C.; Abela-Ridder, B.; Ko, A.I. Global morbidity and mortality of leptospirosis: A systematic Review. PLoS Negl. Trop. Dis. 2015, 9, e0003898. [Google Scholar] [CrossRef] [Green Version]
- Hinjoy, S. Epidemiology of Leptospirosis from Thai National Disease Surveillance System, 2003–2012. Outbreak, Surveillance, and Investigation Reports (OSIR). Available online: http://www.osirjournal.net/index.php/osir/article/view/38 (accessed on 1 November 2021).
- Torgerson, P.R.; Hagan, J.E.; Costa, F.; Calcagno, J.; Kane, M.; Martinez-Silveira, M.S.; Goris, M.G.; Stein, C.; Ko, A.I.; Abela-Ridder, B. Global burden of leptospirosis: Estimated in terms of disability adjusted life years. PLoS Negl. Trop. Dis. 2015, 9, e0004122. [Google Scholar] [CrossRef] [Green Version]
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef]
- Yang, C.W.; Pan, M.J.; Wu, M.S.; Chen, Y.M.; Tsen, Y.T.; Lin, C.L.; Wu, C.H.; Huang, C.C. Leptospirosis: An ignored cause of acute renal failure in Taiwan. Am. J. Kidney Dis. 1997, 30, 840–845. [Google Scholar] [CrossRef]
- Yang, H.Y.; Yen, T.H.; Lin, C.Y.; Chen, Y.C.; Pan, M.J.; Lee, C.H.; Yu, C.C.; Wu, M.S.; Wu, S.S.; Weng, C.H.; et al. Early identification of leptospirosis as an ignored cause of multiple organ dysfunction syndrome. Shock 2012, 38, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Sitprija, V. Renal dysfunction in leptospirosis: A view from the tropics. Nat. Clin. Pract. Nephrol. 2006, 2, 658–659. [Google Scholar] [CrossRef] [PubMed]
- Teles, F.; de Mendonça Uchôa, J.V.; Mirelli Barreto Mendonça, D.; Falcão Pedrosa Costa, A. Acute kidney injury in leptospirosis: The Kidney Disease Improving Global Outcomes (KDIGO) criteria and mortality. Clin. Nephrol. 2016, 86, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Kamath, R.; Swain, S.; Pattanshetty, S.; Nair, N.S. Studying risk factors associated with human leptospirosis. J. Glob. Infect. Dis. 2014, 6, 3–9. [Google Scholar]
- Leshem, E.; Segal, G.; Barnea, A.; Yitzhaki, S.; Ostfeld, I.; Pitlik, S.; Schwartz, E. Travel-related leptospirosis in Israel: A nationwide study. Am. J. Trop. Med. Hyg. 2010, 82, 459–463. [Google Scholar] [CrossRef] [Green Version]
- Seguro, A.C.; Lomar, A.V.; Rocha, A.S. Acute renal failure of leptospirosis: Nonoliguric and hypokalemic forms. Nephron 1990, 55, 146–151. [Google Scholar] [CrossRef]
- Fogelberg, K.; Ferrell, S.T. Vasculitis secondary to presumptive leptospirosis treated with long-term corticosteroids in a captive lesser kudu (Tragelaphus imberbis australis). J. Zoo. Wildl. Med. 2010, 41, 542–544. [Google Scholar] [CrossRef]
- George, P. Two uncommon manifestations of leptospirosis: Sweet’s syndrome and central nervous system vasculitis. Asian Pac. J. Trop. Med. 2011, 4, 83–84. [Google Scholar] [CrossRef] [Green Version]
- Panagopoulos, P.; Terzi, I.; Karanikas, M.; Galanopoulos, N.; Maltezos, E. Myocarditis, pancreatitis, polyarthritis, mononeuritis multiplex and vasculitis with symmetrical peripheral gangrene of the lower extremities as a rare presentation of leptospirosis: A case report and review of the literature. J. Med. Case Rep. 2014, 8, 150. [Google Scholar] [CrossRef] [Green Version]
- Yücel Koçak, S.; Kudu, A.; Kayalar, A.; Yilmaz, M.; Apaydin, S. Leptospirosis with acute renal failure and vasculitis: A case report. Arch. Rheumatol. 2018, 34, 229–232. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.L.; Wu, M.S.; Yang, C.W.; Huang, C.C. Leptospirosis associated with hypokalaemia and thick ascending limb dysfunction. Nephrol. Dial. Transplant. 1999, 14, 193–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cerqueira, T.B.; Athanazio, D.A.; Spichler, A.S.; Seguro, A.C. Renal involvement in leptospirosis—New insights into pathophysiology and treatment. Braz. J. Infect. Dis. 2008, 12, 248–252. [Google Scholar] [CrossRef] [Green Version]
- Araujo, E.R.; Seguro, A.C.; Spichler, A.; Magaldi, A.J.; Volpini, R.A.; De Brito, T. Acute kidney injury in human leptospirosis: An immunohistochemical study with pathophysiological correlation. Virchows Arch. 2010, 456, 367–375. [Google Scholar] [CrossRef] [PubMed]
- Sitprija, V. Altered fluid, electrolyte and mineral status in tropical disease, with an emphasis on malaria and leptospirosis. Nat. Clin. Pract. Nephrol. 2008, 4, 91–101. [Google Scholar] [CrossRef] [PubMed]
- Andrade, L.; Rodrigues, A.C.; Sanches, T.R., Jr.; Souza, R.B.; Seguro, A.C. Leptospirosis leads to dysregulation of sodium transporters in the kidney and lung. Am. J. Physiol. Renal. Physiol. 2007, 292, F586–F592. [Google Scholar] [CrossRef]
- Wu, M.S.; Yang, C.W.; Pan, M.J.; Chang, C.T.; Chen, Y.C. Reduced renal Na+-K+-Cl- co-transporter activity and inhibited NKCC2 mRNA expression by Leptospira shermani: From bedside to bench. Nephrol. Dial. Transplant. 2004, 19, 2472–2479. [Google Scholar] [CrossRef] [Green Version]
- Khositseth, S.; Sudjaritjan, N.; Tananchai, P.; Ong-ajyuth, S.; Sitprija, V.; Thongboonkerd, V. Renal magnesium wasting and tubular dysfunction in leptospirosis. Nephrol. Dial. Transplant. 2008, 23, 952–958. [Google Scholar] [CrossRef]
- El Hasbani, G.; Farooqui, S.R.; Kofahi, A.; Saeed, Y.; Tayeh, O.; Abu-Hishmeh, M.; Moran, H.; Troya-Maldonado, M.; Khanna, R.; Assaker, J.P.; et al. Unusual presentation of urban leptospirosis complicated by a septic shock. IDCases 2019, 17, e00574. [Google Scholar] [CrossRef]
- Bourquin, V.; Ponte, B.; Hirschel, B.; Pugin, J.; Martin, P.Y.; Saudan, P. Severe leptospirosis with multiple organ failure successfully treated by plasma exchange and high-volume hemofiltration. Case Rep. Nephrol. 2011, 2011, 817414. [Google Scholar] [CrossRef] [Green Version]
- Marshall, R.B. The route of entry of leptospires into the kidney tubule. J. Med. Microbiol. 1976, 9, 149–152. [Google Scholar] [CrossRef] [Green Version]
- Yang, C.W.; Wu, M.S.; Pan, M.J.; Hsieh, W.J.; Vandewalle, A.; Huang, C.C. The Leptospira outer membrane protein LipL32 induces tubulointerstitial nephritis-mediated gene expression in mouse proximal tubule cells. J. Am. Soc. Nephrol. 2002, 13, 2037–2045. [Google Scholar] [CrossRef] [Green Version]
- Panpetch, W.; Chancharoenthana, W.; Bootdee, K.; Nilgate, S.; Finkelman, M.; Tumwasorn, S.; Leelahavanichkul, A. Lactobacillus rhamnosus L34 attenuates gut translocation-induced bacterial sepsis in murine models of leaky gut. Infect. Immun. 2017, 86, e00700–e00717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ondee, T.; Gillen, J.; Visitchanakun, P.; Somparn, P.; Issara-Amphorn, J.; Dang Phi, C.; Chancharoenthana, W.; Gurusamy, D.; Nita-Lazar, A.; Leelahavanichkul, A. Lipocalin-2 (Lcn-2) attenuates polymicrobial sepsis with LPS preconditioning (LPS tolerance) in FcGRIIb deficient lupus mice. Cells 2019, 8, 1064. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, C.W.; Wu, M.S.; Pan, M.J.; Hong, J.J.; Yu, C.C.; Vandewalle, A.; Huang, C.C. Leptospira outer membrane protein activates NF-kappaB and downstream genes expressed in medullary thick ascending limb cells. J. Am. Soc. Nephrol. 2000, 11, 2017–2026. [Google Scholar] [CrossRef] [PubMed]
- Haake, D.A.; Chao, G.; Zuerner, R.L.; Barnett, J.K.; Barnett, D.; Mazel, M.; Matsunaga, J.; Levett, P.N.; Bolin, C.A. The leptospiral major outer membrane protein LipL32 is a lipoprotein expressed during mammalian infection. Infect. Immun. 2000, 68, 2276–2285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.H.; Kim, K.A.; Park, Y.G.; Seong, I.W.; Kim, M.J.; Lee, Y.J. Identification and partial characterization of a novel hemolysin from Leptospira interrogans serovar lai. Gene 2000, 254, 19–28. [Google Scholar] [CrossRef]
- Li, S.; Wang, M.; Ojcius, D.M.; Zhou, B.; Hu, W.; Liu, Y.; Ma, Q.; Tang, G.; Wang, D.; Yan, J. Leptospira interrogans infection leads to IL-1β and IL-18 secretion from a human macrophage cell line through reactive oxygen species and cathepsin B mediated-NLRP3 inflammasome activation. Microbes Infect. 2018, 20, 254–260. [Google Scholar] [CrossRef]
- Mariathasan, S.; Monack, D.M. Inflammasome adaptors and sensors: Intracellular regulators of infection and inflammation. Nat. Rev. Immunol. 2007, 7, 31–40. [Google Scholar] [CrossRef]
- Wang, H.; Wu, Y.; Ojcius, D.M.; Yang, X.F.; Zhang, C.; Ding, S.; Lin, X.; Yan, J. Leptospiral hemolysins induce proinflammatory cytokines through Toll-like receptor 2-and 4-mediated JNK and NF-κB signaling pathways. PLoS ONE 2012, 7, e42266. [Google Scholar] [CrossRef]
- Fan, J.; Xie, K.; Wang, L.; Zheng, N.; Yu, X. Roles of inflammasomes in inflammatory kidney diseases. Mediat. Inflamm. 2019, 2019, 2923072. [Google Scholar] [CrossRef] [Green Version]
- Yang, C.W. Leptospirosis renal disease: Understanding the initiation by Toll-like receptors. Kidney Int. 2007, 72, 918–925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hotchkiss, R.S.; Coopersmith, C.M.; Karl, I.E. Prevention of lymphocyte apoptosis—A potential treatment of sepsis? Clin. Infect. Dis. 2005, 41 (Suppl. 7), S465–S469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raffray, L.; Giry, C.; Vandroux, D.; Kuli, B.; Randrianjohany, A.; Pequin, A.M.; Renou, F.; Jaffar-Bandjee, M.C.; Gasque, P. Major neutrophilia observed in acute phase of human leptospirosis is not associated with increased expression of granulocyte cell activation markers. PLoS ONE 2016, 11, e0165716. [Google Scholar] [CrossRef] [Green Version]
- Adiga, D.; Mittal, S.; Venugopal, H.; Mittal, S. Serial changes in complete blood counts in patients with leptospirosis: Our experience. J. Clin. Diagn. Res. 2017, 11, EC21–EC24. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.C.; Chen, Y.C.; Hung, C.C.; Chang, C.T.; Wu, M.S.; Phillips, A.O.; Yang, C.W. Leptospiral outer membrane protein induces extracellular matrix accumulation through a TGF-beta1/Smad-dependent pathway. J. Am. Soc. Nephrol. 2006, 17, 2792–2798. [Google Scholar] [CrossRef] [Green Version]
- Tian, Y.C.; Hung, C.C.; Li, Y.J.; Chen, Y.C.; Chang, M.Y.; Yen, T.H.; Hsu, H.H.; Wu, M.S.; Phillips, A.; Yang, C.W. Leptospira santorosai Serovar Shermani detergent extract induces an increase in fibronectin production through a Toll-like receptor 2-mediated pathway. Infect. Immun. 2011, 79, 1134–1142. [Google Scholar] [CrossRef] [Green Version]
- Fanton d’Andon, M.; Quellard, N.; Fernandez, B.; Ratet, G.; Lacroix-Lamandé, S.; Vandewalle, A.; Boneca, I.G.; Goujon, J.M.; Werts, C. Leptospira Interrogans induces fibrosis in the mouse kidney through Inos-dependent, TLR- and NLR-independent signaling pathways. PLoS Negl. Trop. Dis. 2014, 8, e2664. [Google Scholar] [CrossRef]
- Carrillo-Larco, R.M.; Altez-Fernandez, C.; Acevedo-Rodriguez, J.G.; Ortiz-Acha, K.; Ugarte-Gil, C. Leptospirosis as a risk factor for chronic kidney disease: A systematic review of observational studies. PLoS Negl. Trop. Dis. 2019, 13, e0007458. [Google Scholar] [CrossRef] [Green Version]
- Herath, N.J.; Kularatne, S.A.; Weerakoon, K.G.; Wazil, A.; Subasinghe, N.; Ratnatunga, N.V. Long term outcome of acute kidney injury due to leptospirosis? A longitudinal study in Sri Lanka. BMC Res. Notes 2014, 7, 398. [Google Scholar] [CrossRef] [Green Version]
- Haake, D.A.; Levett, P.N. Leptospirosis in humans. Curr. Top. Microbiol. Immunol. 2015, 387, 65–97. [Google Scholar]
- Fraga, T.R.; Barbosa, A.S.; Isaac, L. Leptospirosis: Aspects of innate immunity, immunopathogenesis and immune evasion from the complement system. Scand. J. Immunol. 2011, 73, 408–419. [Google Scholar] [CrossRef] [PubMed]
- Reis, E.A.; Hagan, J.E.; Ribeiro, G.S.; Teixeira-Carvalho, A.; Martins-Filho, O.A.; Montgomery, R.R.; Shaw, A.C.; Ko, A.I.; Reis, M.G. Cytokine response signatures in disease progression and development of severe clinical outcomes for leptospirosis. PLoS Negl. Trop. Dis. 2013, 7, e2457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kyriakidis, I.; Samara, P.; Papa, A. Serum TNF-α, sTNFR1, IL-6, IL-8 and IL-10 levels in Weil’s syndrome. Cytokine 2011, 54, 117–120. [Google Scholar] [CrossRef] [PubMed]
- Fraga, T.R.; Isaac, L.; Barbosa, A.S. Complement evasion by pathogenic Leptospira. Front. Immunol. 2016, 7, 623. [Google Scholar] [CrossRef] [PubMed]
- Zipfel, P.F.; Hallström, T.; Riesbeck, K. Human complement control and complement evasion by pathogenic microbes—Tipping the balance. Mol. Immunol. 2013, 56, 152–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbosa, A.S.; Abreu, P.A.; Vasconcellos, S.A.; Morais, Z.M.; Gonçales, A.P.; Silva, A.S.; Daha, M.R.; Isaac, L. Immune evasion of Leptospira species by acquisition of human complement regulator C4BP. Infect. Immun. 2009, 77, 1137–1143. [Google Scholar] [CrossRef] [Green Version]
- Zipfel, P.F. Complement and immune defense: From innate immunity to human diseases. Immunol. Lett. 2009, 126, 1–7. [Google Scholar] [CrossRef]
- da Silva, L.B.; Miragaia, L.; Breda, L.C.; Abe, C.M.; Schmidt, M.C.; Moro, A.M.; Monaris, D.; Conde, J.N.; Józsi, M.; Isaac, L.; et al. Pathogenic Leptospira species acquire factor H and vitronectin via the surface protein LcpA. Infect. Immun. 2015, 83, 888–897. [Google Scholar] [CrossRef] [Green Version]
- Amamura, T.A.; Fraga, T.R.; Vasconcellos, S.A.; Barbosa, A.S.; Isaac, L. Pathogenic leptorspira secreted proteases target the membrane attack complex: A potential role for thermolysin in complement inhibition. Front. Microbiol. 2017, 8, 958. [Google Scholar] [CrossRef] [Green Version]
- Verma, A.; Brissette, C.A.; Bowman, A.A.; Shah, S.T.; Zipfel, P.F.; Stevenson, B. Leptospiral endostatin-like protein A is a bacterial cell surface receptor for human plasminogen. Infect. Immun. 2010, 78, 2053–2059. [Google Scholar] [CrossRef] [Green Version]
- Siqueira, G.H.; Atzingen, M.V.; de Souza, G.O.; Vasconcellos, S.A.; Nascimento, A. Leptospira interrogans Lsa23 protein recruits plasminogen, factor H and C4BP from normal human serum and mediates C3b and C4b degradation. Microbiology 2016, 162, 295–308. [Google Scholar] [CrossRef]
- Sun, A.H.; Liu, X.X.; Yan, J. Leptospirosis is an invasive infectious and systemic inflammatory disease. Biomed. J. 2020, 43, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Scharrig, E.; Carestia, A.; Ferrer, M.F.; Cédola, M.; Pretre, G.; Drut, R.; Picardeau, M.; Schattner, M.; Gómez, R.M. Neutrophil extracellular traps are involved in the innate immune response to infection with Leptospira. PLoS Negl. Trop. Dis. 2015, 9, e0003927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, P.; Li, S.J.; Ojcius, D.M.; Li, K.X.; Hu, W.L.; Lin, X.; Sun, A.H.; Yan, J. A novel Fas-binding outer membrane protein and lipopolysaccharide of Leptospira interrogans induce macrophage apoptosis through the Fas/FasL-caspase-8/-3 pathway. Emerg. Microbes Infect. 2018, 7, 135. [Google Scholar] [CrossRef] [Green Version]
- Garcia, L.E.; de Araújo Junior, E.C.; Melo, L.M.; Bragato, J.P.; Peiró, J.R.; Félix de Lima, V.M.; Marinho, M.; Arnold, D.R.; Lopes, F.L. Characterization of the microtranscriptome of macrophages infected with virulent, attenuated and saprophyte strains of Leptospira spp. PLoS Negl. Trop. Dis. 2018, 12, e0006621. [Google Scholar] [CrossRef] [PubMed]
- Silva, P.; Lauretti-Ferreira, F.; Caldas de Lima, M.; Lima, S.S.; Covarrubias, A.E.; De Franco, M.; Carvalho, E.; Ho, P.L.; da Costa, R.; Martins, E.; et al. Phagocytosis of Leptospira by leukocytes from mice with different susceptibility to leptospirosis and possible role of chemokines. BMC Microbiol. 2019, 19, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alia, S.N.; Joseph, N.; Philip, N.; Azhari, N.N.; Garba, B.; Masri, S.N.; Sekawi, Z.; Neela, V.K. Diagnostic accuracy of rapid diagnostic tests for the early detection of leptospirosis. J. Infect. Public Health 2019, 12, 263–269. [Google Scholar] [CrossRef]
- Rubbo, P.A.; Soupé-Gilbert, M.E.; Golongba, D.M.; Mbombo, F.; Girault, D.; Nakouné, E.; Lombart, J.P.; Breurec, S.; Goarant, C. Evidence of human leptospirosis cases in a cohort of febrile patients in Bangui, Central African Republic: A retrospective study, 2012–2015. BMC Infect. Dis. 2018, 18, 376. [Google Scholar] [CrossRef] [Green Version]
- Silveira, M.M.; Oliveira, T.L.; Schuch, R.A.; McBride, A.; Dellagostin, O.A.; Hartwig, D.D. DNA vaccines against leptospirosis: A literature review. Vaccine 2017, 35, 5559–5567. [Google Scholar] [CrossRef]
- Lin, X.; Xiao, G.; Luo, D.; Kong, L.; Chen, X.; Sun, D.; Yan, J. Chimeric epitope vaccine against Leptospira interrogans infection and induced specific immunity in guinea pigs. BMC Microbiol. 2016, 16, 241. [Google Scholar] [CrossRef] [Green Version]
- Yirsaw, A.W.; Gillespie, A.; Britton, E.; Doerle, A.; Johnson, L.; Marston, S.; Telfer, J.; Baldwin, C.L. Goat γδ T cell subpopulations defined by WC1 expression, responses to pathogens and cytokine production. Dev. Comp. Immunol. 2021, 118, 103984. [Google Scholar] [CrossRef] [PubMed]
- Ferrer, M.F.; Scharrig, E.; Alberdi, L.; Cedola, M.; Pretre, G.; Drut, R.; Song, W.C.; Gomez, R.M. Decay-accelerating factor 1 deficiency exacerbates leptospiral-induced murine chronic nephritis and renal fibrosis. PLoS ONE 2014, 9, e102860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volz, M.S.; Moos, V.; Allers, K.; Luge, E.; Mayer-Scholl, A.; Nöckler, K.; Loddenkemper, C.; Jansen, A.; Schneider, T. Specific CD4+ T-cell reactivity and cytokine release in different clinical presentations of leptospirosis. Clin. Vaccine Immunol. 2015, 22, 1276–1284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cagliero, J.; Villanueva, S.; Matsui, M. Leptospirosis pathophysiology: Into the storm of cytokines. Front. Cell. Infect. Microbiol. 2018, 8, 204. [Google Scholar] [CrossRef] [Green Version]
- Picardeau, M.; Bertherat, E.; Jancloes, M.; Skouloudis, A.N.; Durski, K.; Hartskeerl, R.A. Rapid tests for diagnosis of leptospirosis: Current tools and emerging technologies. Diag. Microbiol. Infect. Dis. 2014, 78, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Levett, P.N. Leptospirosis. Clin. Microbiol. Rev. 2001, 14, 296–326. [Google Scholar] [CrossRef] [Green Version]
- Faine, S.; World Health Organization. Guidelines for the Control of Leptospirosis; WHO Offset; WHO: Geneva, Switzerland, 1982; Volume 67, pp. 99–171. Available online: https://apps.who.int/iris/handle/10665/37219 (accessed on 1 February 2022).
- Ellis, W.; Montgomery, J.; Cassells, J. Dihydrostreptomycin treatment of bovine carriers of Leptospira interrogans serovar Hardjo. Res. Vet. Sci. 1985, 39, 292–295. [Google Scholar] [CrossRef]
- Hornsby, R.L.; Alt, D.P.; Nally, J.E. Isolation and propagation of leptospires at 37 °C directly from the mammalian host. Sci. Rep. 2020, 10, 9620. [Google Scholar] [CrossRef]
- Goris, M.G.; Boer, K.R.; Duarte, T.A.; Kliffen, S.J.; Hartskeerl, R.A. Human leptospirosis trends, the Netherlands, 1925–2008. Emerg. Infect. Dis. 2013, 19, 371–378. [Google Scholar] [CrossRef]
- Wilson, M.R.; Naccache, S.N.; Samayoa, E.; Biagtan, M.; Bashir, H.; Yu, G.; Salamat, S.M.; Somasekar, S.; Federman, S.; Miller, S.; et al. Actionable diagnosis of neuroleptospirosis by next-generation sequencing. N. Engl. J. Med. 2014, 370, 2408–2417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villumsen, S.; Pedersen, R.; Krogfelt, K.A.; Jensen, J.S. Expanding the diagnostic use of PCR in leptospirosis: Improved method for DNA extraction from blood cultures. PLoS ONE 2010, 5, e12095. [Google Scholar] [CrossRef]
- Merien, F.; Portnoi, D.; Bourhy, P.; Charavay, F.; Berlioz-Arthaud, A.; Baranton, G. A rapid and quantitative method for the detection of Leptospira species in human leptospirosis. FEMS Microbiol. Lett. 2005, 249, 139–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez, L.J.; Lanka, S.; DeShambo, V.J.; Fredrickson, R.L.; Maddox, C.W. A Validated multiplex real-time PCR assay for the diagnosis of infectious Leptospira spp.: A novel assay for the detection and differentiation of strains from both pathogenic groups I and II. Front. Microbiol. 2020, 11, 457. [Google Scholar] [CrossRef] [PubMed]
- Blanco, R.M.; Romero, E.C. Evaluation of nested polymerase chain reaction for the early detection of Leptospira spp. DNA in serum samples from patients with leptospirosis. Diag. Microbiol. Infect. Dis. 2014, 78, 343–346. [Google Scholar] [CrossRef]
- Jouglard, S.D.; Simionatto, S.; Seixas, F.K.; Nassi, F.L.; Dellagostin, O.A. Nested polymerase chain reaction for detection of pathogenic leptospires. Can. J. Microbiol. 2006, 52, 747–752. [Google Scholar] [CrossRef]
- Gasem, M.H.; Hadi, U.; Alisjahbana, B.; Tjitra, E.; Hapsari, M.; Lestari, E.S.; Aman, A.T.; Lokida, D.; Salim, G.; Kosasih, H.; et al. Leptospirosis in Indonesia: Diagnostic challenges associated with atypical clinical manifestations and limited laboratory capacity. BMC Infect. Dis. 2020, 20, 179. [Google Scholar] [CrossRef] [PubMed]
- Widiasih, D.A.; Lindahl, J.F.; Artama, W.T.; Sutomo, A.H.; Kutanegara, P.M.; Mulyani, G.T.; Widodo, E.; Djohan, T.S.; Unger, F. Leptospirosis in ruminants in Yogyakarta, Indonesia: A serological survey with mixed methods to identify risk factors. Trop. Med. Infect. Dis. 2021, 6, 84. [Google Scholar] [CrossRef]
- Koizumi, N.; Nakajima, C.; Harunari, T.; Tanikawa, T.; Tokiwa, T.; Uchimura, E.; Furuya, T.; Mingala, C.N.; Villanueva, M.A.; Ohnishi, M.; et al. A new loop-mediated isothermal amplification method for rapid, simple, and sensitive detection of Leptospira spp. in urine. J. Clin. Microbiol. 2012, 50, 2072–2074. [Google Scholar] [CrossRef] [Green Version]
- Agampodi, S.B.; Vinetz, J.M. Next-generation sequencing analysis of pathogenic leptospira: A way forward for understanding infectious disease dynamics in low/middle-income, disease-endemic settings. Am. J. Trop. Med. Hyg. 2021, 104, 1625–1627. [Google Scholar] [CrossRef]
- Musso, D.; La Scola, B. Laboratory diagnosis of leptospirosis: A challenge. J. Microbiol. Immunol. Infect. 2013, 46, 245–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marquez, A.; Djelouadji, Z.; Lattard, V.; Kodjo, A. Overview of laboratory methods to diagnose Leptospirosis and to identify and to type leptospires. Int. Microbiol. 2017, 20, 184–193. [Google Scholar] [PubMed]
- Goris, M.G.; Leeflang, M.M.; Loden, M.; Wagenaar, J.F.; Klatser, P.R.; Hartskeerl, R.A.; Boer, K.R. Prospective evaluation of three rapid diagnostic tests for diagnosis of human leptospirosis. PLoS Negl. Trop. Dis. 2013, 7, e2290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- OiE Terrestrial Manual. Chapter 3.1.12. Leptospirosis. Available online: https://www.oie.int/fileadmin/Home/fr/Health_standards/tahm/3.01.12_LEPTO.pdf (accessed on 1 February 2022).
- Bal, A.E.; Gravekamp, C.; Hartskeerl, R.A.; De Meza-Brewster, J.; Korver, H.; Terpstra, W.J. Detection of leptospires in urine by PCR for early diagnosis of leptospirosis. J. Clin. Microbiol. 1994, 32, 1894–1898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ganoza, C.A.; Matthias, M.A.; Saito, M.; Cespedes, M.; Gotuzzo, E.; Vinetz, J.M. Asymptomatic renal colonization of humans in the peruvian Amazon by Leptospira. PLoS Negl. Trop. Dis. 2010, 4, e612. [Google Scholar] [CrossRef]
- Sukmark, T.; Lumlertgul, N.; Peerapornratana, S.; Khositrangsikun, K.; Tungsanga, K.; Sitprija, V.; Srisawat, N.; Thai-Lepto AKI study group. Thai-Lepto-on-admission probability (THAI-LEPTO) score as an early tool for initial diagnosis of leptospirosis: Result from Thai-Lepto AKI study group. PLoS Negl. Trop. Dis. 2018, 12, e0006319. [Google Scholar] [CrossRef] [Green Version]
- McBride, A.J.; Athanazio, D.A.; Reis, M.G.; Ko, A.I. Leptospirosis. Curr. Opin. Infect. Dis. 2005, 18, 376–386. [Google Scholar] [CrossRef]
- Dupont, H.; Dupont-Perdrizet, D.; Perie, J.L.; Zehner-Hansen, S.; Jarrige, B.; Daijardin, J.B. Leptospirosis: Prognostic factors associated with mortality. Clin. Infect. Dis. 1997, 25, 720–724. [Google Scholar] [CrossRef]
- Limothai, U.; Lumlertgul, N.; Sirivongrangson, P.; Kulvichit, W.; Tachaboon, S.; Dinhuzen, J.; Chaisuriyong, W.; Peerapornratana, S.; Chirathaworn, C.; Praditpornsilpa, K.; et al. The role of leptospiremia and specific immune response in severe leptospirosis. Sci. Rep. 2021, 11, 14630. [Google Scholar] [CrossRef]
- Ko, A.I.; Galvão Reis, M.; Ribeiro Dourado, C.M.; Johnson, W.D.; Riley, L.W., Jr. Urban epidemic of severe leptospirosis in Brazil. Salvador Leptospirosis Study Group. Lancet 1999, 354, 820–825. [Google Scholar] [CrossRef]
- Raoult, D.; Jeandel, P.; Mailloux, M.; Rougier, Y. Thrombocytopenia and renal failure in leptospirosis. Am. J. Trop. Med. Hyg. 1983, 32, 1464. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.L.; Jiang, X.C.; Zhang, X.Y.; Li, W.J.; Hu, B.Y.; Zhao, G.P.; Guo, X.K. Thrombocytopenia in the experimental leptospirosis of guinea pig is not related to disseminated intravascular coagulation. BMC Infect. Dis. 2006, 6, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duarte, D.B.; Lacerda, M.; Ribeiro, Y.; Ribeiro, M.; Frederico, M.A.; Oliveira, M. Kidney biomarkers in tropical infections: An update. Pathog. Glob. Health 2020, 114, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Srisawat, N.; Wen, X.; Lee, M.; Kong, L.; Elder, M.; Carter, M.; Unruh, M.; Finkel, K.; Vijayan, A.; Ramkumar, M.; et al. Urinary biomarkers and renal recovery in critically ill patients with renal support. Clin. J. Am. Soc. Nephrol. 2011, 6, 1815–1823. [Google Scholar] [CrossRef]
- Srisawat, N.; Praditpornsilpa, K.; Patarakul, K.; Techapornrung, M.; Daraswang, T.; Sukmark, T.; Khositrangsikun, K.; Fakthongyoo, A.; Oranrigsupak, P.; Praderm, L.; et al. Neutrophil gelatinase associated lipocalin (NGAL) in leptospirosis acute kidney injury: A multicenter study in Thailand. PLoS ONE 2015, 10, e0143367. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, A.; Beck, M.; Malmström, J.; Lam, H.; Claassen, M.; Campbell, D.; Aebersold, R. Absolute quantification of microbial proteomes at different states by directed mass spectrometry. Mol. Syst. Biol. 2011, 7, 510. [Google Scholar] [CrossRef]
- Panich, T.; Chancharoenthana, W.; Somparn, P.; Issara-Amphorn, J.; Hirankarn, N.; Leelahavanichkul, A. Urinary exosomal activating transcriptional factor 3 as the early diagnostic biomarker for sepsis-induced acute kidney injury. BMC Nephrol. 2017, 18, 10. [Google Scholar] [CrossRef] [Green Version]
- Panaphut, T.; Domrongkitchaiporn, S.; Vibhagool, A.; Thinkamrop, B.; Susaengrat, W. Ceftriaxone compared with sodium penicillin G for treatment of severe leptospirosis. Clin. Infect. Dis. 2003, 36, 1507–1513. [Google Scholar] [CrossRef] [Green Version]
- Brett-Major, D.M.; Coldren, R. Antibiotics for leptospirosis. Cochrane Database Syst. Rev. 2012, 2, CD008264. [Google Scholar] [CrossRef]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; Mcintyre, L.; Ostermann, M.; Prescott, H.C.; et al. Executive summary: Surviving Sepsis Campaign: International Guidelines for the Management of Sepsis and Septic Shock 2021. Crit. Care Med. 2021, 49, 1974–1982. [Google Scholar] [CrossRef]
- Mallat, J.; Meddour, M.; Durville, E.; Lemyze, M.; Pepy, F.; Temime, J.; Vangrunderbeeck, N.; Tronchon, L.; Thevenin, D.; Tavernier, B. Decrease in pulse pressure and stroke volume variations after mini-fluid challenge accurately predicts fluid responsiveness. Br. J. Anaesth. 2015, 115, 449–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murugan, R.; Kellum, J.A. Fluid balance and outcome in acute kidney injury: Is fluid really the best medicine? Crit. Care Med. 2012, 40, 1970–1972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kellum, J.A.; Bellomo, R.; Kramer, D.J.; Pinsky, M.R. Etiology of metabolic acidosis during saline resuscitation in endotoxemia. Shock 1998, 9, 364–368. [Google Scholar] [CrossRef]
- Kraut, J.A.; Madias, N.E. Lactic acidosis. N. Engl. J. Med. 2014, 371, 2309–2319. [Google Scholar] [CrossRef] [PubMed]
- Hoste, E.A.; Colpaert, K.; Vanholder, R.C.; Lameire, N.H.; De Waele, J.J.; Blot, S.I.; Colardyn, F.A. Sodium bicarbonate versus THAM in ICU patients with mild metabolic acidosis. J. Nephrol. 2005, 18, 303–307. [Google Scholar] [PubMed]
- Andrade, L.; Cleto, S.; Seguro, A.C. Door-to-dialysis time and daily hemodialysis in patients with leptospirosis: Impact on mortality. Clin. J. Am. Soc. Nephrol. 2007, 2, 739–744. [Google Scholar] [CrossRef] [PubMed]
- Chancharoenthana, W.; Tiranathanagul, K.; Srisawat, N.; Susantitaphong, P.; Leelahavanichkul, A.; Praditpornsilpa, K.; Tungsanga, K.; Eiam-Ong, S. Enhanced vascular endothelial growth factor and inflammatory cytokine removal with online hemodiafiltration over high-flux hemodialysis in sepsis-related acute kidney injury patients. Ther. Apher. Dial. 2013, 17, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Phu, N.H.; Hien, T.T.; Mai, N.T.; Chau, T.T.; Chuong, L.V.; Loc, P.P.; Winearls, C.; Farrar, J.; White, N.; Day, N. Hemofiltration and peritoneal dialysis in infection-associated acute renal failure in Vietnam. N. Engl. J. Med. 2002, 347, 895–902. [Google Scholar] [CrossRef]
- Chancharoenthana, W.; Leelahavanichkul, A. Acute kidney injury spectrum in patients with chronic liver disease: Where do we stand? World J. Gastroenterol. 2019, 25, 3684–3703. [Google Scholar] [CrossRef]
- Nadim, M.K.; Kellum, J.A.; Davenport, A.; Wong, F.; Davis, C.; Pannu, N.; Tolwani, A.; Bellomo, R.; Genyk, Y.S.; ADQI Workgroup. Hepatorenal syndrome: The 8th International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit. Care 2012, 16, R23. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Direct Methods | Indirect Methods |
|---|---|
| Microscopy | Genus-specific antibody tests |
| DFM, phase contrast | IHA, ELISA, Leptospirosis IgM dipstick, MCAT |
| Staining | Serovar-specific antibody test |
| Warthin-Starry silver stain, immunohistochemistry, immunofluorescence, immunoperoxidase | MAT |
| Isolations of leptospires | |
| DNA hybridization or DNA probe | |
| Animal inoculation | |
| DNA amplification | |
| PCR, LAMP, NGS, qPCR |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chancharoenthana, W.; Leelahavanichkul, A.; Schultz, M.J.; Dondorp, A.M. Going Micro in Leptospirosis Kidney Disease. Cells 2022, 11, 698. https://doi.org/10.3390/cells11040698
Chancharoenthana W, Leelahavanichkul A, Schultz MJ, Dondorp AM. Going Micro in Leptospirosis Kidney Disease. Cells. 2022; 11(4):698. https://doi.org/10.3390/cells11040698
Chicago/Turabian StyleChancharoenthana, Wiwat, Asada Leelahavanichkul, Marcus J. Schultz, and Arjen M. Dondorp. 2022. "Going Micro in Leptospirosis Kidney Disease" Cells 11, no. 4: 698. https://doi.org/10.3390/cells11040698