
Off-the-Shelf Cord-Blood Mesenchymal Stromal Cells: Production, Quality Control, and Clinical Use

 , , , , , , , , , , , , , , and
, , , , , , , , , , , , , , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Tissue Procurement
2.2. GMP Facility
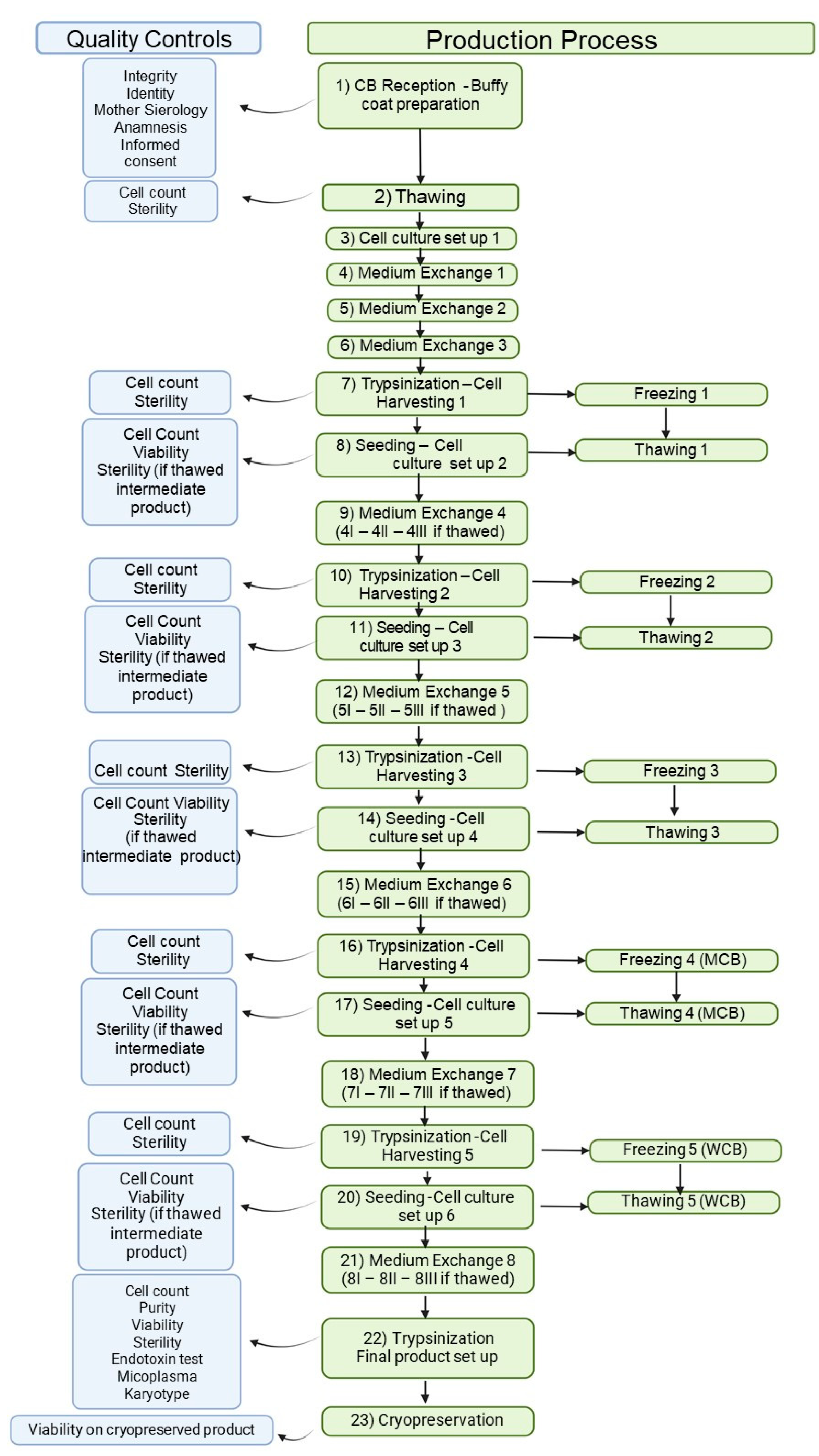
2.3. MSC(CB) Manufacturing Process
2.4. Quality Control Tests
2.4.1. Cell Count
2.4.2. Microbiological Contamination
2.4.3. Phenotyping and Viability (Flow Cytometry)
2.4.4. Karyotyping
2.4.5. Adventitious Virus Analysis
2.4.6. HLA Typing
2.4.7. CFU-F
2.4.8. Fold Expansion
2.5. Additional Tests
2.5.1. RNA Extraction and Real-Time qRT-PCR for Gene Expression
2.5.2. DNA Extraction and Real-Time qPCR
2.6. ATMP Stability in the Storage Conditions
2.7. ATMP Stability under Usage Conditions
2.8. Clinical Use of MSC(CB)s
3. Results
3.1. Tissue Procurement
3.2. GMP Facility, MSC(CB) Manufacturing Process and Quality Controls
3.3. Additional Tests
3.4. Stability
3.5. Clinical Use
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACD-A | Anticoagulant Citrate Dextrose Solution, Solution A |
| AIFA | Agenzia Italiana del Farmaco—Italian Drug Agency |
| ATMP | Advanced Therapy Medicinal Product |
| BM | bone marrow |
| CB | cord blood |
| CMV | cytomegalovirus |
| DMSO | dimethyl sulfoxide |
| EBV | Epstein–Barr virus |
| EU | endotoxin units |
| FBS | fetal bovine serum |
| FE | fold expansion |
| GMP | Good Manufacturing Practice |
| HAS | human serum albumin |
| LL | long-living |
| MCB | master cell bank |
| MSC | mesenchymal stromal cell |
| PI | propidium iodide |
| SL | short-living |
| WBC | working cell bank |
References
- Friedenstein, A.J.; Chailakhjan, R.K.; Lalykina, K.S. The Development of Fibroblast Colonies in Monolayer Cultures of Guinea-Pig Bone Marrow and Spleen Cells. Cell Tissue Kinet. 1970, 3, 393–403. [Google Scholar] [CrossRef]
- Zuk, P.A.; Zhu, M.; Mizuno, H.; Huang, J.; Futrell, J.W.; Katz, A.J.; Benhaim, P.; Lorenz, H.P.; Hedrick, M.H. Multilineage Cells from Human Adipose Tissue: Implications for Cell-Based Therapies. Tissue Eng. 2001, 7, 211–228. [Google Scholar] [CrossRef]
- Kaviani, A.; Perry, T.E.; Dzakovic, A.; Jennings, R.W.; Ziegler, M.M.; Fauza, D.O. The Amniotic Fluid as a Source of Cells for Fetal Tissue Engineering. J. Pediatr. Surg. 2001, 36, 1662–1665. [Google Scholar] [CrossRef]
- Gronthos, S.; Mankani, M.; Brahim, J.; Robey, P.G.; Shi, S. Postnatal Human Dental Pulp Stem Cells (DPSCs) in Vitro and in Vivo. Proc. Natl. Acad. Sci. USA 2000, 97, 13625–13630. [Google Scholar] [CrossRef]
- Igura, K.; Zhang, X.; Takahashi, K.; Mitsuru, A.; Yamaguchi, S.; Takahashi, T.A. Isolation and Characterization of Mesenchymal Progenitor Cells from Chorionic Villi of Human Placenta. Cytotherapy 2004, 6, 543–553. [Google Scholar] [CrossRef]
- Erices, A.; Conget, P.; Minguell, J.J. Mesenchymal Progenitor Cells in Human Umbilical Cord Blood. Br. J. Haematol. 2000, 109, 235–242. [Google Scholar] [CrossRef]
- McElreavey, K.D.; Irvine, A.I.; Ennis, K.T.; McLean, W.H.I. Isolation, Culture and Characterisation of Fibroblast-like Cells Derived from the Wharton’s Jelly Portion of Human Umbilical Cord. Biochem. Soc. Trans. 1991, 19, 29S. [Google Scholar] [CrossRef]
- Jaimes, Y.; Naaldijk, Y.; Wenk, K.; Leovsky, C.; Emmrich, F. Mesenchymal Stem Cell-Derived Microvesicles Modulate Lipopolysaccharides-Induced Inflammatory Responses to Microglia Cells. Stem Cells 2017, 35, 812–823. [Google Scholar] [CrossRef]
- Lecchi, L.; Rebulla, P.; Ratti, I.; Magri, M.; Garcea, F.; Marangoni, F.; Bertelé, T.; Giordano, R.; Sirchia, G. Outcomes of a Program to Evaluate Mother and Baby 6 Months after Umbilical Cord Blood Donation. Transfusion 2001, 41, 606–610. [Google Scholar] [CrossRef]
- Podestà, M.A.; Remuzzi, G.; Casiraghi, F. Mesenchymal Stromal Cell Therapy in Solid Organ Transplantation. Front. Immunol. 2021, 11, 618243. [Google Scholar] [CrossRef]
- Passweg, J.R.; Baldomero, H.; Chabannon, C.; Basak, G.W.; de la Cámara, R.; Corbacioglu, S.; Dolstra, H.; Duarte, R.; Glass, B.; Greco, R.; et al. Hematopoietic Cell Transplantation and Cellular Therapy Survey of the EBMT: Monitoring of Activities and Trends over 30 Years. Bone Marrow Transplant. 2021, 56, 1651–1664. [Google Scholar] [CrossRef]
- Gupta, A.O.; Wagner, J.E. Umbilical Cord Blood Transplants: Current Status and Evolving Therapies. Front. Pediatr. 2020, 8, 570282. [Google Scholar] [CrossRef]
- WMDA Total Number of Donors and Cord Blood Units. Available online: https://statistics.wmda.info/ (accessed on 11 May 2023).
- HCT Presentation Slides. Available online: https://bethematchclinical.org/medical-education-and-research/hct-presentation-slides/#/ (accessed on 11 May 2023).
- Bieback, K.; Netsch, P. Isolation, Culture, and Characterization of Human Umbilical Cord Blood-Derived Mesenchymal Stromal Cells. Methods Mol. Biol. 2016, 1416, 245–258. [Google Scholar] [CrossRef]
- Montemurro, T.; Viganò, M.; Ragni, E.; Barilani, M.; Parazzi, V.; Boldrin, V.; Lavazza, C.; Montelatici, E.; Banfi, F.; Lauri, E.; et al. Angiogenic and Anti-Inflammatory Properties of Mesenchymal Stem Cells from Cord Blood: Soluble Factors and Extracellular Vesicles for Cell Regeneration. Eur. J. Cell Biol. 2016, 95, 228–238. [Google Scholar] [CrossRef]
- Heo, J.S.; Choi, Y.; Kim, H.S.; Kim, H.O. Comparison of Molecular Profiles of Human Mesenchymal Stem Cells Derived from Bone Marrow, Umbilical Cord Blood, Placenta and Adipose Tissue. Int. J. Mol. Med. 2016, 37, 115–125. [Google Scholar] [CrossRef]
- Wagner, W.; Wein, F.; Seckinger, A.; Frankhauser, M.; Wirkner, U.; Krause, U.; Blake, J.; Schwager, C.; Eckstein, V.; Ansorge, W.; et al. Comparative Characteristics of Mesenchymal Stem Cells from Human Bone Marrow, Adipose Tissue, and Umbilical Cord Blood. Exp. Hematol. 2005, 33, 1402–1416. [Google Scholar] [CrossRef]
- Peltzer, J.; Aletti, M.; Frescaline, N.; Busson, E.; Lataillade, J.J.; Martinaud, C. Mesenchymal Stromal Cells Based Therapy in Systemic Sclerosis: Rational and Challenges. Front. Immunol. 2018, 9, 2013. [Google Scholar] [CrossRef]
- Barilani, M.; Palorini, R.; Votta, G.; Piras, R.; Buono, G.; Grassi, M.; Bollati, V.; Chiaradonna, F.; Lazzari, L. Central Metabolism of Functionally Heterogeneous Mesenchymal Stromal Cells. Sci. Rep. 2019, 9, 15420. [Google Scholar] [CrossRef]
- Barilani, M.; Lavazza, C.; Viganò, M.; Montemurro, T.; Boldrin, V.; Parazzi, V.; Montelatici, E.; Crosti, M.; Moro, M.; Giordano, R.; et al. Dissection of the Cord Blood Stromal Component Reveals Predictive Parameters for Culture Outcome. Stem Cells Dev. 2015, 24, 104–114. [Google Scholar] [CrossRef]
- Standards|FACT. Available online: https://factglobal.org/standards/ (accessed on 11 May 2023).
- Ministero della Salute Disposizioni Relative Ai Requisiti Di Qualità e Sicurezza Del Sangue e Degli Emocomponenti. Available online: https://www.gazzettaufficiale.it/eli/id/2015/12/28/15A09709/sg (accessed on 11 May 2023).
- Montemurro, T.; Viganò, M.; Budelli, S.; Montelatici, E.; Lavazza, C.; Marino, L.; Parazzi, V.; Lazzari, L.; Giordano, R. How We Make Cell Therapy in Italy. Drug Des. Devel. Ther. 2015, 9, 4825–4834. [Google Scholar] [CrossRef]
- European Medicines Agency Re-Establishment of Working Seeds and Working Cell Banks Using TSE Compliant Materials—Scientific Guideline. Available online: https://www.ema.europa.eu/en/re-establishment-working-seeds-working-cell-banks-using-tse-compliant-materials-scientific-guideline (accessed on 12 May 2023).
- European Medicines Agency Minimising the Risk of Transmitting Animal Spongiform Encephalopathy Agents via Human and Veterinary Medicinal Products—Scientific Guideline. Available online: https://www.ema.europa.eu/en/minimising-risk-transmitting-animal-spongiform-encephalopathy-agents-human-veterinary-medicinal (accessed on 12 May 2023).
- Cavani, S.; Camurri, L.; Giardino, D.; Romana Grati, F.; Bernardini, L.; Angioni, A.; Battaglia, P.; Calzone, R.; Cardarelli, L.; Carella, M.; et al. Società Italiana Di Genetica Umana Gruppo Di Lavoro in Citogenetica SIGU LINEE GUIDA PER LA DIAGNOSI CITOGENETICA 2013 a Cura Del Gruppo Di Lavoro in Citogenetica SIGU Hanno Preso Parte Alla Stesura: Coordinatore: Antonio Novelli Revisione Del Testo: Bruno Dallapiccola. 2013. Available online: https://sigu.net/wp-content/uploads/2020/11/Linee_Guida_14_febbraio-2014.pdf (accessed on 14 May 2024).
- Viganò, M.; Budelli, S.; Lavazza, C.; Montemurro, T.; Montelatici, E.; De Cesare, S.; Lazzari, L.; Orlandi, A.R.; Lunghi, G.; Giordano, R. Tips and Tricks for Validation of Quality Control Analytical Methods in Good Manufacturing Practice Mesenchymal Stromal Cell Production. Stem Cells Int. 2018, 2018, 3038565. [Google Scholar] [CrossRef]
- Cherubini, A.; Rusconi, F.; Lazzari, L. Identification of the Best Housekeeping Gene for RT-QPCR Analysis of Human Pancreatic Organoids. PLoS ONE 2021, 16, e0260902. [Google Scholar] [CrossRef]
- Regulation (EC) No 1394/2007 of the European Parliament and of the Council of 13 November 2007 on Advanced Therapy Medicinal Products and Amending Directive 2001/83/EC and Regulation (EC) No 726/2004 (Text with EEA Relevance). Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32007R1394 (accessed on 14 May 2024).
- Directive 2001/83/EC of the European Parliament and of the Council of 6 November 2001 on the Community Code Relating to Medicinal Products for Human Use. Available online: https://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2001:311:0067:0128:en:PDF (accessed on 14 May 2024).
- Ministero della Salute Disposizioni in Materia Di Medicinali per Terapie Avanzate Preparati Base Non Ripetitiva. (15A01704) (GU n.56 Del 9-3-2015). Available online: https://www.gazzettaufficiale.it/atto/stampa/serie_generale/originario (accessed on 12 May 2023).
- Morello, W.; Budelli, S.; Bernstein, D.A.; Montemurro, T.; Montelatici, E.; Lavazza, C.; Ghio, L.; Edefonti, A.; Peruzzi, L.; Molino, D.; et al. First Clinical Application of Cord Blood Mesenchymal Stromal Cells in Children with Multi-Drug Resistant Nephrotic Syndrome. Stem Cell Res. Ther. 2022, 13, 420. [Google Scholar] [CrossRef]
- Sharma, A.; Badawy, S.M.; Suelzer, E.M.; Murthy, H.S.; Prasad, P.; Eissa, H.; Carpenter, P.A.; Hamadani, M.; Labopin, M.; Schoemans, H.; et al. Systematic Reviews in Hematopoietic Cell Transplantation and Cellular Therapy: Considerations and Guidance from the American Society for Transplantation and Cellular Therapy, European Society for Blood and Marrow Transplantation, and the Center for International Blood and Marrow Transplant Research Late Effects and Quality of Life Working Committee. Bone Marrow Transplant. 2021, 56, 786–797. [Google Scholar] [CrossRef]
- Rodríguez-Fuentes, D.E.; Fernández-Garza, L.E.; Samia-Meza, J.A.; Barrera-Barrera, S.A.; Caplan, A.I.; Barrera-Saldaña, H.A. Mesenchymal Stem Cells Current Clinical Applications: A Systematic Review. Arch. Med. Res. 2021, 52, 93–101. [Google Scholar] [CrossRef]
- Zhou, L.; Yao, S. Recent Advances in Therapeutic CRISPR-Cas9 Genome Editing: Mechanisms and Applications. Mol. Biomed. 2023, 4, 10. [Google Scholar] [CrossRef]
- Colter, D.C.; Class, R.; DiGirolamo, C.M.; Prockop, D.J. Rapid Expansion of Recycling Stem Cells in Cultures of Plastic-Adherent Cells from Human Bone Marrow. Proc. Natl. Acad. Sci. USA 2000, 97, 3213–3218. [Google Scholar] [CrossRef]
- Galipeau, J.; Sensébé, L. Mesenchymal Stromal Cells: Clinical Challenges and Therapeutic Opportunities. Cell Stem Cell 2018, 22, 824–833. [Google Scholar] [CrossRef]
- Markov, V.; Kusumi, K.; Tadesse, M.G.; William, D.A.; Hall, D.M.; Lounev, V.; Carlton, A.; Leonard, J.; Cohen, R.I.; Rappaport, E.F.; et al. Identification of Cord Blood-Derived Mesenchymal Stem/Stromal Cell Populations with Distinct Growth Kinetics, Differentiation Potentials, and Gene Expression Profiles. Stem Cells Dev. 2007, 16, 53–73. [Google Scholar] [CrossRef]
- Lee, R.H.; Pulin, A.A.; Seo, M.J.; Kota, D.J.; Ylostalo, J.; Larson, B.L.; Semprun-Prieto, L.; Delafontaine, P.; Prockop, D.J. Intravenous HMSCs Improve Myocardial Infarction in Mice Because Cells Embolized in Lung Are Activated to Secrete the Anti-Inflammatory Protein TSG-6. Cell Stem Cell 2009, 5, 54. [Google Scholar] [CrossRef]
- de Witte, S.F.H.; Luk, F.; Sierra Parraga, J.M.; Gargesha, M.; Merino, A.; Korevaar, S.S.; Shankar, A.S.; O’Flynn, L.; Elliman, S.J.; Roy, D.; et al. Immunomodulation by Therapeutic Mesenchymal Stromal Cells (MSC) Is Triggered Through Phagocytosis of MSC By Monocytic Cells. Stem Cells 2018, 36, 602–615. [Google Scholar] [CrossRef]
- Galleu, A.; Riffo-Vasquez, Y.; Trento, C.; Lomas, C.; Dolcetti, L.; Cheung, T.S.; Von Bonin, M.; Barbieri, L.; Halai, K.; Ward, S.; et al. Apoptosis in Mesenchymal Stromal Cells Induces in Vivo Recipient-Mediated Immunomodulation. Sci. Transl. Med. 2017, 9, eaam7828. [Google Scholar] [CrossRef]
- Vasaghi, A.; Dehghani, A.; Khademalhosseini, Z.; Maharlooei, M.K.; Monabati, A.; Attar, A. Parameters That Influence the Isolation of Multipotent Mesenchymal Stromal Cells from Human Umbilical Cord Blood. Hematol. Oncol. Stem Cell Ther. 2013, 6, 1–8. [Google Scholar] [CrossRef]
- Oliver-Vila, I.; Coca, M.I.; Grau-Vorster, M.; Pujals-Fonts, N.; Caminal, M.; Casamayor-Genescà, A.; Ortega, I.; Reales, L.; Pla, A.; Blanco, M.; et al. Evaluation of a Cell-Banking Strategy for the Production of Clinical Grade Mesenchymal Stromal Cells from Wharton’s Jelly. Cytotherapy 2016, 18, 25–35. [Google Scholar] [CrossRef]
- Raileanu, V.N.; Whiteley, J.; Chow, T.; Kollara, A.; Mohamed, A.; Keating, A.; Rogers, I.M. Banking Mesenchymal Stromal Cells from Umbilical Cord Tissue: Large Sample Size Analysis Reveals Consistency Between Donors. Stem Cells Transl. Med. 2019, 8, 1041–1054. [Google Scholar] [CrossRef]
- Sypecka, M.; Bzinkowska, A.; Sulejczak, D.; Dabrowski, F.; Sarnowska, A. Evaluation of the Optimal Manufacturing Protocols and Therapeutic Properties of Mesenchymal Stem/Stromal Cells Derived from Wharton’s Jelly. Int. J. Mol. Sci. 2022, 24, 652. [Google Scholar] [CrossRef]
- Muñoz-Domínguez, N.; Carreras-Sánchez, I.; López-Fernández, A.; Vives, J. Optimisation of Processing Methods to Improve Success in the Derivation of Human Multipotent Mesenchymal Stromal Cells from Cryopreserved Umbilical Cord Tissue Fragments. Cryobiology 2022, 108, 34–41. [Google Scholar] [CrossRef]
- Broxmeyer, H.E.; Lee, M.R.; Hangoc, G.; Cooper, S.; Prasain, N.; Kim, Y.J.; Mallett, C.; Ye, Z.; Witting, S.; Cornetta, K.; et al. Hematopoietic Stem/Progenitor Cells, Generation of Induced Pluripotent Stem Cells, and Isolation of Endothelial Progenitors from 21- to 23.5-Year Cryopreserved Cord Blood. Blood 2011, 117, 4773–4777. [Google Scholar] [CrossRef]
- Broxmeyer, H.E.; Srour, E.F.; Hangoc, G.; Cooper, S.; Anderson, S.A.; Bodine, D.M. High-Efficiency Recovery of Functional Hematopoietic Progenitor and Stem Cells from Human Cord Blood Cryopreserved for 15 Years. Proc. Natl. Acad. Sci. USA 2003, 100, 645–650. [Google Scholar] [CrossRef]
- Mojsilović, S.; Jauković, A.; Kukolj, T.; Obradović, H.; Ðordević, I.O.; Petrović, A.; Bugarski, D. Tumorigenic Aspects of MSC Senescence-Implication in Cancer Development and Therapy. J. Pers. Med. 2021, 11, 1133. [Google Scholar] [CrossRef]
- Coppé, J.P.; Desprez, P.Y.; Krtolica, A.; Campisi, J. The Senescence-Associated Secretory Phenotype: The Dark Side of Tumor Suppression. Annu. Rev. Pathol. 2010, 5, 99–118. [Google Scholar] [CrossRef]
- Barilani, M.; Lovejoy, C.; Piras, R.; Abramov, A.Y.; Lazzari, L.; Angelova, P.R. Age-Related Changes in the Energy of Human Mesenchymal Stem Cells. J. Cell. Physiol. 2022, 237, 1753–1767. [Google Scholar] [CrossRef]
- Barilani, M.; Cherubini, A.; Peli, V.; Polveraccio, F.; Bollati, V.; Guffanti, F.; Del Gobbo, A.; Lavazza, C.; Giovanelli, S.; Elvassore, N.; et al. A Circular RNA Map for Human Induced Pluripotent Stem Cells of Foetal Origin. EBioMedicine 2020, 57, 102848. [Google Scholar] [CrossRef]
- Hemeda, H.; Giebel, B.; Wagner, W. Evaluation of Human Platelet Lysate versus Fetal Bovine Serum for Culture of Mesenchymal Stromal Cells. Cytotherapy 2014, 16, 170–180. [Google Scholar] [CrossRef]
- Ratushnyy, A.; Ezdakova, M.; Buravkova, L. Secretome of Senescent Adipose-Derived Mesenchymal Stem Cells Negatively Regulates Angiogenesis. Int. J. Mol. Sci. 2020, 21, 1802. [Google Scholar] [CrossRef]
- Xie, Y.; Chen, F.; Jia, L.; Chen, R.; Zhang, V.W.; Zhong, X.; Wang, D. Mesenchymal Stem Cells from Different Sources Show Distinct Therapeutic Effects in Hyperoxia-Induced Bronchopulmonary Dysplasia in Rats. J. Cell. Mol. Med. 2021, 25, 8558–8566. [Google Scholar] [CrossRef]
- Peltzer, J.; Montespan, F.; Thepenier, C.; Boutin, L.; Uzan, G.; Rouas-Freiss, N.; Lataillade, J.J. Heterogeneous Functions of Perinatal Mesenchymal Stromal Cells Require a Preselection before Their Banking for Clinical Use. Stem Cells Dev. 2015, 24, 329–344. [Google Scholar] [CrossRef]
- Li, C.H.; Zhao, J.; Zhang, H.Y.; Wang, B. Banking of Perinatal Mesenchymal Stem/Stromal Cells for Stem Cell-Based Personalized Medicine over Lifetime: Matters Arising. World J. Stem Cells 2023, 15, 105–119. [Google Scholar] [CrossRef]
- Sanabria-de la Torre, R.; Quiñones-Vico, M.I.; Fernández-González, A.; Sánchez-Díaz, M.; Montero-Vílchez, T.; Sierra-Sánchez, Á.; Arias-Santiago, S. Alloreactive Immune Response Associated to Human Mesenchymal Stromal Cells Treatment: A Systematic Review. J. Clin. Med. 2021, 10, 2991. [Google Scholar] [CrossRef]
- Hao, D.; Ma, B.; He, C.; Liu, R.; Farmer, D.L.; Lam, K.S.; Wang, A. Surface Modification of Polymeric Electrospun Scaffolds via a Potent and High-Affinity Integrin A4β1 Ligand Improved the Adhesion, Spreading and Survival of Human Chorionic Villus-Derived Mesenchymal Stem Cells: A New Insight for Fetal Tissue Engineering. J. Mater. Chem. B 2020, 8, 1649–1659. [Google Scholar] [CrossRef]
- Song, H.; Chang, W.; Lim, S.; Seo, H.-S.; Shim, C.Y.; Park, S.; Yoo, K.-J.; Kim, B.-S.; Min, B.-H.; Lee, H.; et al. Tissue Transglutaminase Is Essential for Integrin-Mediated Survival of Bone Marrow-Derived Mesenchymal Stem Cells. Stem Cells 2007, 25, 1431–1438. [Google Scholar] [CrossRef]
- Volkert, G.; Jahn, A.; Dinkel, C.; Fahlbusch, F.; Zürn, C.; Hilgers, K.F.; Rascher, W.; Hartner, A.; Marek, I. Contribution of the A8 Integrin Chain to the Expression of Extracellular Matrix Components. Cell Commun. Adhes. 2014, 21, 89–98. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Starting Material ID | #1 | #2 | #3 |
|---|---|---|---|
| Banking exclusion criteria | Low cellularity | Low volume | Low volume |
| Volume (mL) | 91.5 | 59.5 | 51.3 |
| Total nucleated cells (×103/µL) | 10.5 | 8.5 | 9.8 |
| % Monocyte | 4.3 | 6.2 | 6.3 |
| Gestational age (weeks) | 40 | 41 | 40 |
| 1st minute Apgar score | 10/10 | 9/10 | 9/10 |
| 5th minute Apgar score | 10/10 | 10/10 | 10/10 |
| Type of delivery | CS | ND | CS |
| Child gender | M | F | F |
| Child weight at birth (kg) | 3.40 | 2.96 | 3.28 |
| Product | Supplier | Reference | Specification |
|---|---|---|---|
| Human albumin 200 g/L | Kedrion, Lucca, Italy | A.I.C. 022515163 | Blood product for human use (any Marketing Authorization Holder—MAH). |
| ACD-A | Terumo BTC, Tokyo, Japan | 40804 | Class 2 medical device manufactured according to Directive 93/42/EEC. |
| Citrate phosphate dextrose CPD | SALF SpA Bergamo, Italy | A.I.C. 031328 | Medicinal product for human use. |
| DMSO | Cryoserv—Mylan Institutional Canonsburg, PA, USA | 67457-178-50 | Manufactured according with GMP, sterile and with endotoxin level < 0.5 EU/mL. |
| FBS Australian | ThermoFisher Scientific Thermo Fisher Waltham, MA, USA | 10101-145 | EDQM-certified of suitability gamma irradiated sterile serum with an endotoxin level < 0.5 EU/mL. |
| PBS | MacoPharma, Tourcoing, France | 0120020 | Xeno-free solution tampon, sterile and with endotoxin level < 0.5 IU/mL. |
| Physiological Solution NaCl 0.9% | Baxter, Milano, Italy | A.I.C. 035715010 | Medicinal product for human use e.v. |
| TrypLE Select | Thermo Fisher Scientific Thermo Fisher Waltham, MA, USA | 12563-011 | A sterile free of any animal origin element trypsin with endotoxin level < 1.0 EU/mL. |
| αMEM 675 mL | MacoPharma, Tourcoing, France | 0110020 | A sterile xeno-free medium with endotoxin level < 0.5 UI/mL. |
| Test Name | Method | U.M. | Result | Specifications | |
|---|---|---|---|---|---|
| Release test | Purity | Flow cytometry (Ph. Eu. 2.7.24) | CD45− CD90+ CD105+ cells (%) § | 97.3 ± 2.7 | ≥90 |
| Contaminants | CD45+ cells (%) § | 0.6 ± 0.5 | ≤2 | ||
| Viability | PI- cells (%) | 92.7 ± 4.6 | ≥80 | ||
| Sterility | Ph. Eu. 2.6.27 | / | Sterile | Sterile | |
| Bacterial endotoxin testing | Ph. Eu. 2.6.14 | EU/mL | 0.245 ± 0.0 | <0.25 | |
| Mycoplasma | Ph. Eu. 2.6.7 | / | No growth | No growth | |
| Karyotype | Q-banding (SIGU guidelines) | / | 46,XX/46,XY | 46,XX/46,XY | |
| Additional test * | Extended immunophenotype | Flow cytometry (Ph. Eu. 2.7.24) | CD45− CD73+ CD105+ cells (%) | 96.5 ± 4.0 | none |
| CD45− CD73+ CD90+ cells (%) | 95.8 ± 5.3 | none | |||
| Viability (restricted) | Flow cytometry (Ph. Eu. 2.7.24) | CD45− CD90+ PI- cells (%) | 91.8 ± 5.2 | none | |
| Post-thawing viability | Flow cytometry (Ph. Eu. 2.7.24) | PI- cells (%) | ± | ≥80 | |
| Adventitious viruses | PCR (Ph. Eu. 2.6.21) | CMV-DNA | n.d. | n.d. | |
| EBV-DNA | n.d. | n.d. | |||
| Respiratory viruses RNA/DNA | n.d. | n.d. | |||
| HLA typing | Sequence-Specific Oligonucleotide Probe (SSOP) Hybridization Assays (EFI standards, current edition) | HLA-A-B-DR donor | Correspondence to the donor HLA | Correspondence to the donor HLA |
| Demographics | |
|---|---|
| Female gender (N; %) | 18; 42.8 |
| Age (years) * | 12 (0.5–60) |
| Subjects < 18 years of age (N; %) | 33; 78.5 |
| Weight (kg) * | 42 (2.7–83.6) |
| Subjects ≥ 18 years of age * | 57.1 (41.2–80) |
| Subjects < 18 years of age * | 34.7 (2.7–83.6) |
| Disease (n of total subject; n of subjects > 18 years of age) | |
| GvHD | 8; 8 |
| NS | 33; 1 |
| BPD | 1; 0 |
| Treatment | |
| Cell dose (×106)/KG * | 1.6 (1–10) |
| Cell dose (×106)/kg in subjects ≥ 18 years of age * | 1.7 (1.4–3) |
| Intravenous administration (n) | 41 |
| Subjects who received 3 administrations (n; %) | 30; 71.4 |
| Interval between treatments (days) * | 8 (3–42) |
| Patient No. | Age | Diagnosis | GVHD Grading, Type (and Site) | Treatment before MSC(CB) Infusion | Infusions (No.) | Response (Site of Response) | Treatment after MSC(CB) Infusion | State at 18-Month Follow-Up |
|---|---|---|---|---|---|---|---|---|
| 1 | 52 | NHL | Grade IV aGvHD (gut) | Steroid + MMF + ECP | 2 | CR | ECP suspension; steroid reduction | Cutaneous cGVHD |
| 2 | 49 | NHL | Grade IV aGvHD (skin; gut) | Steroid + MMF + ECP | 3 | PR (limited to gut) | MMF reduction | OS |
| 3 | 22 | MDS | Grade IV aGvHD (skin; gut) | Steroid | 4 | PR (limited to skin) | none | D (1) |
| 4 | 51 | AML | OS | CyA + steroid + ECP | 3 | PR (limited to skin) | CyA + steroid + ECP | D (3.5) |
| 5 | 20 | AML | IV (gut) | Steroid; Rituximab; Etanercept; ATG | 2 | NR | None | D (10) |
| 6 | 22 | MDS | IV (skin; gut) | Steroid | 3 | NR | None | D (1) |
| 7 | 50 | MM | IV (gut) | Steroid + MMF + ECP | 3 | CR | ECP suspension; steroid and MMF reduction | D (3.5) |
| 8 | 59 | AML | OS | CyA + steroid + ECP | 3 | PR (limited to skin) | CyA + steroid +ECP | OS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montemurro, T.; Lavazza, C.; Montelatici, E.; Budelli, S.; La Rosa, S.; Barilani, M.; Mei, C.; Manzini, P.; Ratti, I.; Cimoni, S.; et al. Off-the-Shelf Cord-Blood Mesenchymal Stromal Cells: Production, Quality Control, and Clinical Use. Cells 2024, 13, 1066. https://doi.org/10.3390/cells13121066
Montemurro T, Lavazza C, Montelatici E, Budelli S, La Rosa S, Barilani M, Mei C, Manzini P, Ratti I, Cimoni S, et al. Off-the-Shelf Cord-Blood Mesenchymal Stromal Cells: Production, Quality Control, and Clinical Use. Cells. 2024; 13(12):1066. https://doi.org/10.3390/cells13121066
Chicago/Turabian StyleMontemurro, Tiziana, Cristiana Lavazza, Elisa Montelatici, Silvia Budelli, Salvatore La Rosa, Mario Barilani, Cecilia Mei, Paolo Manzini, Ilaria Ratti, Silvia Cimoni, and et al. 2024. "Off-the-Shelf Cord-Blood Mesenchymal Stromal Cells: Production, Quality Control, and Clinical Use" Cells 13, no. 12: 1066. https://doi.org/10.3390/cells13121066
APA StyleMontemurro, T., Lavazza, C., Montelatici, E., Budelli, S., La Rosa, S., Barilani, M., Mei, C., Manzini, P., Ratti, I., Cimoni, S., Brasca, M., Prati, D., Saporiti, G., Astori, G., Elice, F., Giordano, R., & Lazzari, L. (2024). Off-the-Shelf Cord-Blood Mesenchymal Stromal Cells: Production, Quality Control, and Clinical Use. Cells, 13(12), 1066. https://doi.org/10.3390/cells13121066