
Therapeutic Effect of Boron Neutron Capture Therapy on Boronophenylalanine Administration via Cerebrospinal Fluid Circulation in Glioma Rat Models

 ,
,  ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. C6 Glioma Model Orthotopic Rats
2.2. BNCT Effect on the CSF Administration Method of 10BPA
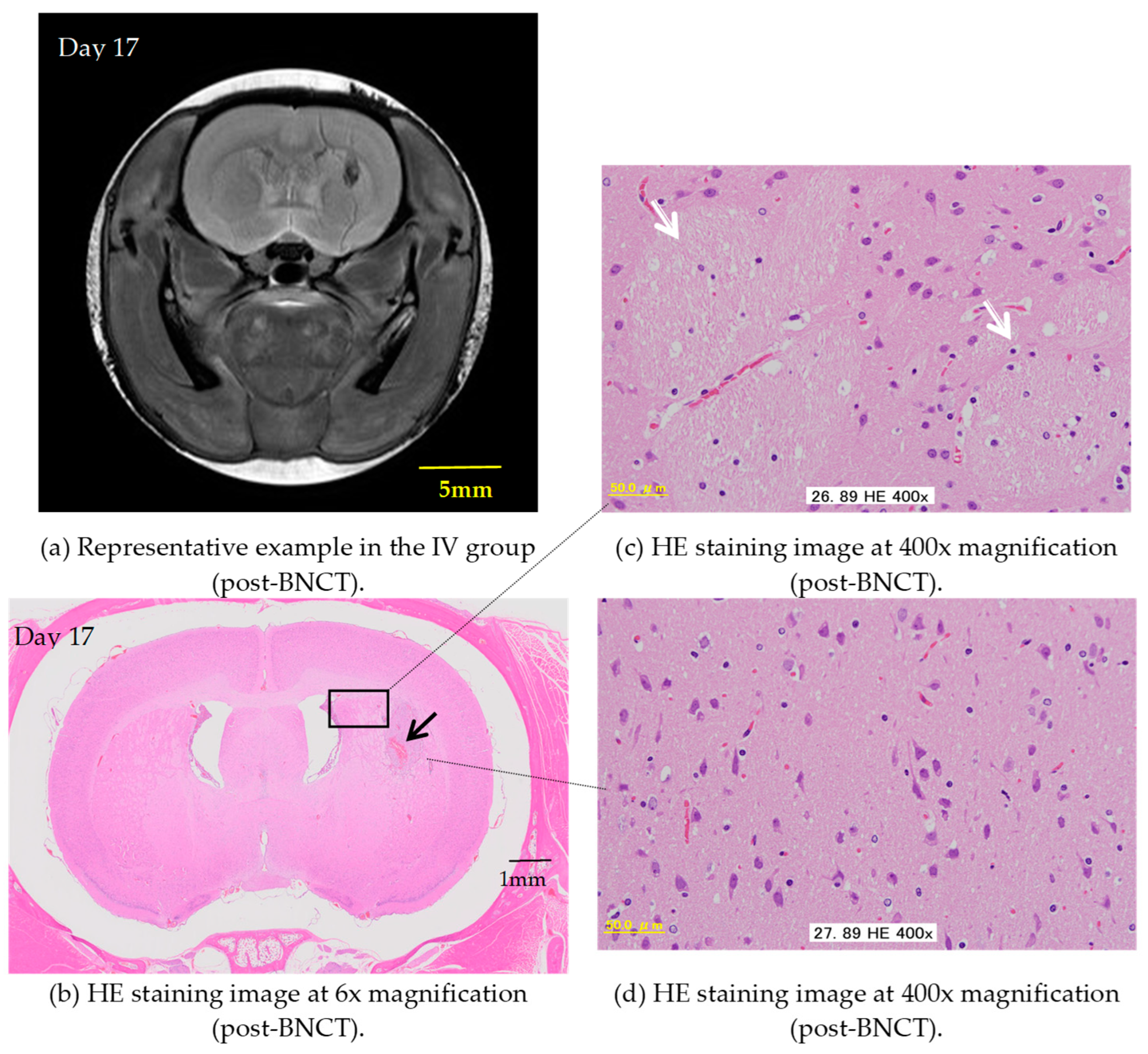
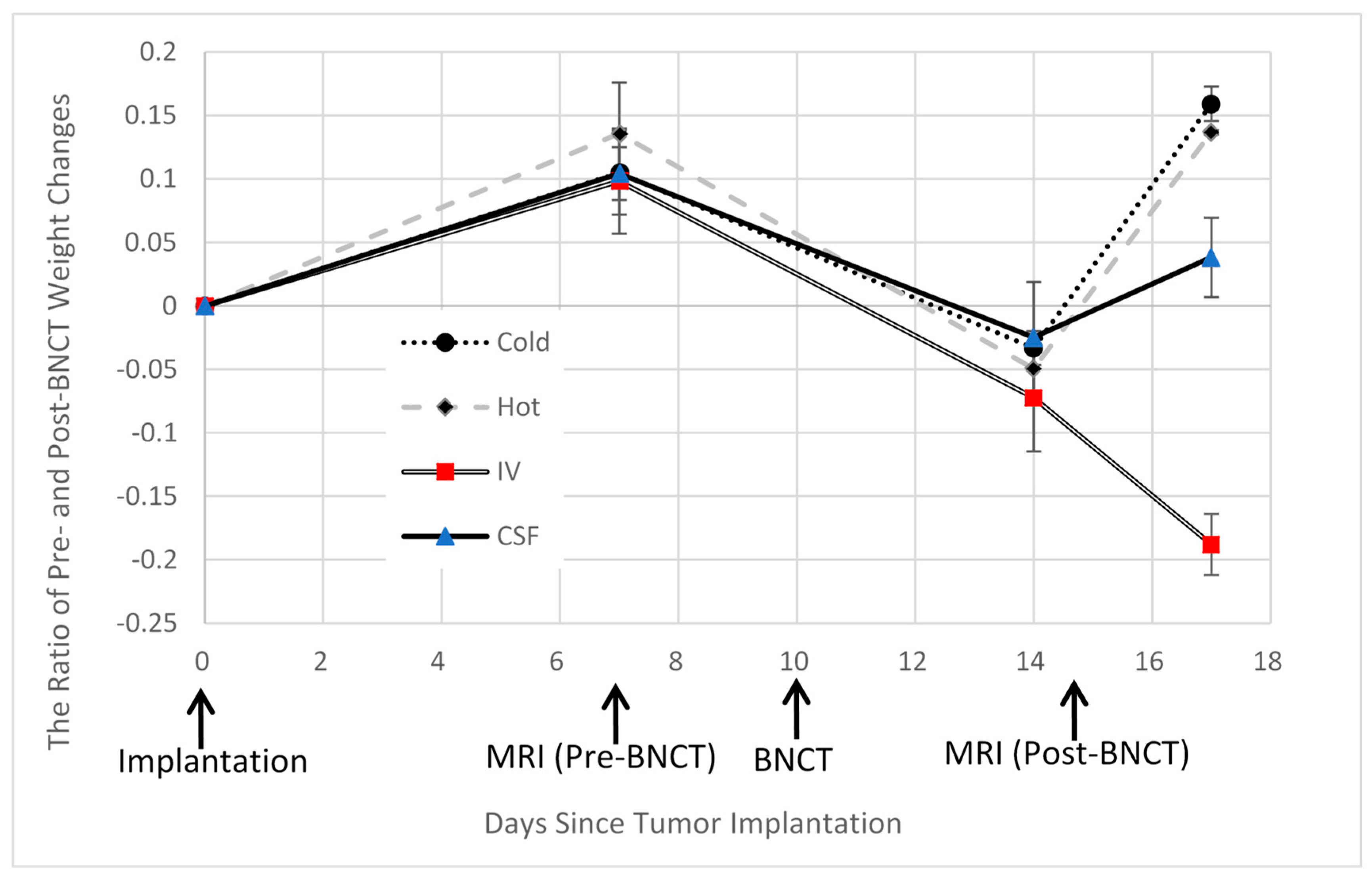
2.3. Pre- and Post-Treatment MRI Assessment
2.4. Hematoxylin and Eosin Staining of C6 Rat Glioma Brain Sections
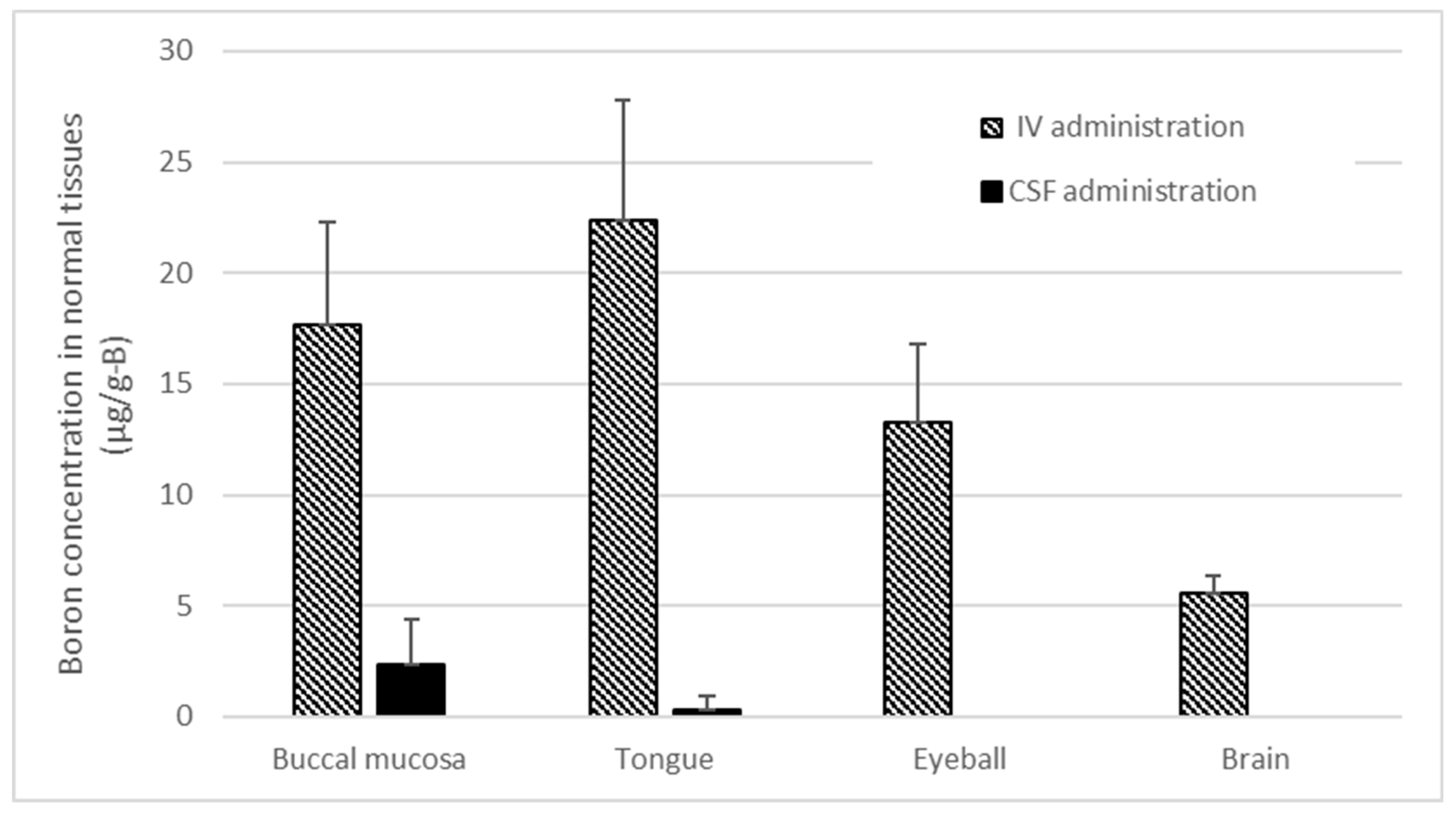
2.5. Boron Concentrations in Various Normal Tissues of Rat Heads Administered BPA via Both the CSF and IV Methods
2.6. Statistics
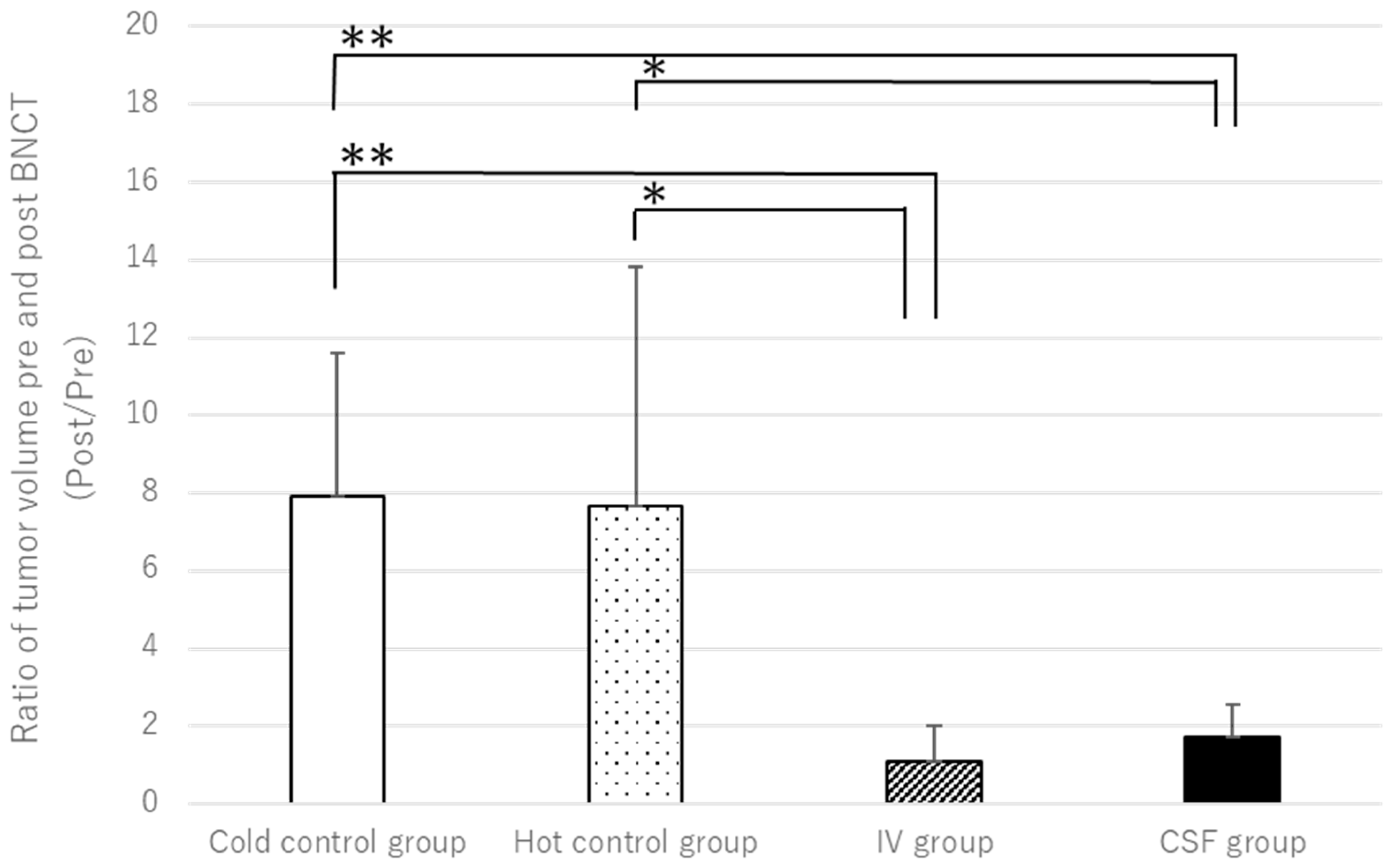
3. Results
4. Discussion
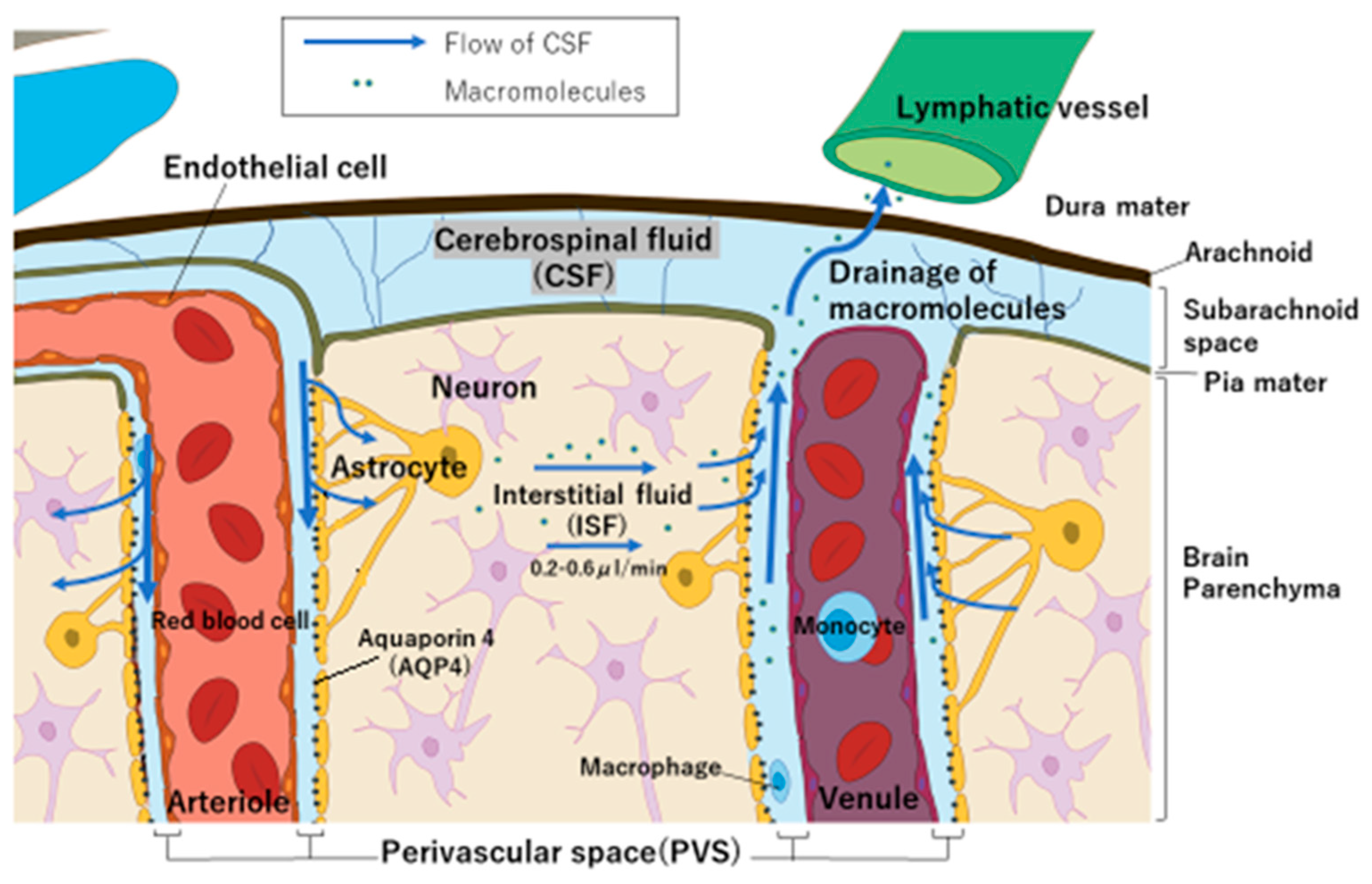
4.1. Why Does BPA Accumulate in Brain Tumors Despite Small Doses of CSF
4.2. Boron Concentration in Normal Tissues and the T/N Ratio in BNCT
4.3. BPA Pharmacokinetics and Pharmacodynamics in Brain Tissue
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pan, J.; Zhao, R.; Dong, C.; Yang, J.; Zhang, R.; Sun, M.; Ahmad, N.; Zhou, Y.; Liu, Y. Cudraflavone B induces human glioblastoma cells apoptosis via ER stress-induced autophagy. BMC Neurosci. 2023, 24, 10. [Google Scholar] [CrossRef] [PubMed]
- Salam, R.; Saliou, A.; Bielle, F.; Bertrand, M.; Antoniewski, C.; Carpentier, C.; Alentorn, A.; Capelle, L.; Sanson, M.; Huillard, E.; et al. Cellular senescence in malignant cells promotes tumor progression in mouse and patient Glioblastoma. Nat. Commun. 2023, 14, 441. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Camacho, A.; Flores-Vázquez, J.G.; Moscardini-Martelli, J.; Torres-Ríos, J.A.; Olmos-Guzmán, A.; Ortiz-Arce, C.S.; Cid-Sánchez, D.R.; Pérez, S.R.; Macías-González, M.D.S.; Hernández-Sánchez, L.C.; et al. Glioblastoma Treatment: State-of-the-Art and Future Perspectives. Int. J. Mol. Sci. 2022, 23, 7207. [Google Scholar] [CrossRef]
- Li, K.; Han, H.; Zhu, K.; Lee, K.; Liu, B.; Zhou, F.; Fu, Y.; He, Q. Real-time magnetic resonance imaging visualization and quantitative assessment of diffusion in the cerebral extracellular space of C6 glioma-bearing rats. Neurosci. Lett. 2013, 543, 84–89. [Google Scholar] [CrossRef]
- Hall, W.A.; Vallera, D.A. Efficacy of antiangiogenic targeted toxins against glioblastoma multiforme. Neurosurg. Focus 2006, 20, E23. [Google Scholar] [CrossRef]
- Barth, R.F.; Vicente, M.H.; Harling, O.K.; Kiger, W.S., 3rd; Riley, K.J.; Binns, P.J.; Wagner, F.M.; Suzuki, M.; Aihara, T.; Kato, I.; et al. Current status of boron neutron capture therapy of high grade gliomas and recurrent head and neck cancer. Radiat. Oncol. 2012, 7, 146. [Google Scholar] [CrossRef] [PubMed]
- Miyatake, S.-I.; Kuwabara, H.; Kajimoto, Y.; Kawabata, S.; Yokoyama, K.; Doi, A.; Tsuji, M.; Mori, H.; Ono, K.; Kuroiwa, T. Preferential recurrence of a sarcomatous component of a gliosarcoma after boron neutron capture therapy: Case report. J. Neuro-Oncol. 2006, 76, 143–147. [Google Scholar] [CrossRef]
- Barth, R.F.; Wu, G.; Vicente, M.d.G.H.; Grecula, J.C.; Gupta, N. Boron neutron capture therapy of cancer: Where do we stand now? Cancer Commun. 2024, 44, 889–892. [Google Scholar] [CrossRef] [PubMed]
- Cheng, X.; Li, F.; Liang, L. Boron Neutron Capture Therapy: Clinical Application and Research Progress. Curr. Oncol. 2022, 29, 7868–7886. [Google Scholar] [CrossRef]
- Kawabata, S.; Hiramatsu, R.; Kuroiwa, T.; Ono, K.; Miyatake, S.-I. Boron neutron capture therapy for recurrent high-grade meningiomas. J. Neurosurg. 2013, 119, 837–844. [Google Scholar] [CrossRef]
- Boumghar, R.; Belgaid, M. BNCT dosimetry for brain cancer based on the nuclear research reactor NUR and the modified MIRD phantom by introducing the eye lens: Simulation study. Radiat. Phys. Chem. 2023, 213, 111209. [Google Scholar] [CrossRef]
- Järvinen, J.; Pulkkinen, H.; Rautio, J.; Timonen, J.M. Amino Acid-Based Boron Carriers in Boron Neutron Capture Therapy (BNCT). Pharmaceutics 2023, 15, 2663. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.D.; Ye, M.; Levy, A.F.; Rothstein, J.D.; Bergles, D.E.; Searson, P.C. The blood-brain barrier: An engineering perspective. Front. Neuroeng. 2013, 6, 7. [Google Scholar] [CrossRef] [PubMed]
- Pardridge, W.M. The Blood-Brain Barrier: Bottleneck in Brain Drug Development. J. Am. Soc. Exp. Neurotherapeutics 2005, 2, 3–14. [Google Scholar] [CrossRef]
- Cheng, W.; Ren, W.; Ye, P.; He, L.; Bao, D.; Yue, T.; Lai, J.; Wu, Y.; Wei, Y.; Wu, Z.; et al. Camouflaging nanoreactor traverse the blood-brain barrier to catalyze redox cascade for synergistic therapy of glioblastoma. Biomaterials 2024, 311, 1–15. [Google Scholar] [CrossRef]
- Marin, B.M.; Porath, K.A.; Jain, S.; Kim, M.; Conage-Pough, J.E.; Oh, J.H.; Miller, C.L.; Talele, S.; Kitange, G.J.; Tian, S.; et al. Heterogeneous delivery across the blood-brain barrier limits the efficacy of an EGFR-targeting antibody drug conjugate in glioblastoma. Neuro-Oncology 2021, 23, 2042–2053. [Google Scholar] [CrossRef]
- Jackson, C.M.; Choi, J.; Lim, M. Mechanisms of immunotherapy resistance: Lessons from glioblastoma. Nat. Immunol. 2019, 20, 1100–1109. [Google Scholar] [CrossRef]
- Kalbasi, A.; Ribas, A. Tumour- intrinsic resistance to immune checkpoint blockade. Reviews 2020, 20, 25–39. [Google Scholar] [CrossRef]
- Nishimura, K.; Kashiwagi, H.; Morita, T.; Fukuo, Y.; Okada, S.; Miura, K.; Matsumoto, Y.; Sugawara, Y.; Enomoto, T.; Suzuki, M.; et al. Efficient neutron capture therapy of glioblastoma with pteroyl-closo-dodecaborate-conjugated 4-(p-iodophenyl) butyric acid (PBC-IP). J. Control. Release 2023, 360, 249–259. [Google Scholar] [CrossRef] [PubMed]
- Calias, P.; Banks, W.A.; Begley, D.; Scarpa, M.; Dickson, P. Intrathecal delivery of protein therapeutics to the brain: A critical reassessment. Pharmacol. Ther. 2014, 144, 114–122. [Google Scholar] [CrossRef]
- Geary, R.S.; Norris, D.; Yu, R.; Bennett, C.F. Pharmacokinetics, biodistribution and cell uptake of antisense oligonucleotides. Adv. Drug Deliv. Rev. 2015, 87, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Atwal, J.K.; Hildebrand, K. Widespread brain distribution and activity following i.c.v. infusion of anti-β-secretase (BACE1) in nonhuman primates. Br. J. Pharmacol. 2017, 174, 4173–4185. [Google Scholar]
- Louveau, A.; Smirnov, I.; Keyes, T.J.; Eccles, J.D.; Rouhani, S.J.; Peske, J.D.; Derecki, N.C.; Castle, D.; Mandell, J.W.; Lee, K.S.; et al. Structural and functional features of central nervous system lymphatic vessels. Nature 2015, 523, 337–341. [Google Scholar] [CrossRef]
- Kouzehgarani, G.N.; Feldsien, T.; Engelhard, H.H.; Mirakhur, K.K.; Phipps, C.; Nimmrich, V.; Clausznitzer, D.; Lefebvre, D.R. Harnessing cerebrospinal fluid circulation for drug delivery to brain tissues. Adv. Drug Deliv. Rev. 2021, 173, 20–59. [Google Scholar] [CrossRef]
- Kusaka, S.; Morizane, Y.; Tokumaru, Y.; Tamaki, S.; Maemunah, I.R.; Akiyama, Y.; Sato, F.; Murata, I. Cerebrospinal fluid-based boron delivery system may help increase the uptake boron for boron neutron capture therapy in veterinary medicine: A preliminary study with normal rat brain cells. Res. Vet. Sci. 2022, 148, 1–6. [Google Scholar] [CrossRef]
- Kusaka, S.; Morizane, Y.; Tokumaru, Y.; Tamaki, S.; Maemunah, I.R.; Akiyama, Y.; Sato, F.; Murata, I. Boron Delivery to Brain Cells via Cerebrospinal Fluid (CSF) Circulation for BNCT in a Rat Melanoma Model. Biology 2022, 11, 397. [Google Scholar] [CrossRef] [PubMed]
- Kusaka, S.; Miyake, Y.; Tokumaru, Y.; Morizane, Y.; Tamaki, S.; Akiyama, Y.; Sato, F.; Murata, I. Boron Delivery to Brain Cells via Cerebrospinal Fluid (CSF) Circulation in BNCT of Brain-Tumor-Model Rats—Ex Vivo Imaging of BPA Using MALDI Mass Spectrometry Imaging. Life 2022, 12, 1786. [Google Scholar] [CrossRef]
- Kato, I.; Osaka University, Osaka, Japan. Private communication, 2024.
- Saito, S.; Ueda, J. Preclinical magnetic resonance imaging and spectroscopy in the fields of radiological technology, medical physics, and radiology. Radiol. Phys. Technol. 2024, 17, 47–59. [Google Scholar] [CrossRef] [PubMed]
- Mentis, A.F.A.; Dardiotis, E.; Chrousos, G.P. Apolipoprotein E4 and meningeal lymphatics in Alzheimer disease: A conceptual framework. Mol. Psychiatry 2021, 26, 1075–1097. [Google Scholar] [CrossRef]
- Mentis, A.-F.A.; Dardiotis, E.; Chrousos, G.P. APOE4-mediated Alzheimer disease and “Vascular”—“Meningeal Lymphatic” components: Towards a novel therapeutic era? Mol. Psychiatry 2021, 26, 5472–5474. [Google Scholar]
- Amiry-Moghaddam, M.; Ottersen, O.P. The Brain’s Glymphatic System: Current Controversies. Trends Neurosci. 2020, 43, 458–466. [Google Scholar]
- Amiry-Moghaddam, M.; Ottersen, O.P. The molecular basis of water transport in the brain. Nat. Rev. Neurosci. 2003, 4, 991–1001. [Google Scholar] [CrossRef] [PubMed]
- Kress, B.T.; Iliff, J.J.; Xia, M.; Wang, M.; Wei, H.S.; Zeppenfeld, D.; Xie, L.; Kang, H.; Xu, Q.; Liew, J.A.; et al. Impairment of Paravascular Clearance Pathways in the Aging Brain. Am. Neurol. Assoc. 2014, 76, 845–861. [Google Scholar] [CrossRef] [PubMed]
- Romanov, V.; Isohashi, K.; Alobthani, G.; Beshr, R.; Horitsugi, G.; Kanai, Y.; Naka, S.; Watabe, T.; Shimosegawa, E.; Hatazawa, J. Evaluation of the total distribution volume of 18F-FBPA in normal tissues of healthy volunteers by non-compartmental kinetic modeling. Ann. Nucl. Med. 2020, 34, 155–162. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Day 0 * | Day 7 | Day 10 | Day 17 | |||
|---|---|---|---|---|---|---|
| C6 Cell Transplantation | MRI (Pre-BNCT) | BNCT | MRI (Post-BNCT) | HE Staining | ||
| BPA | Irradiation | |||||
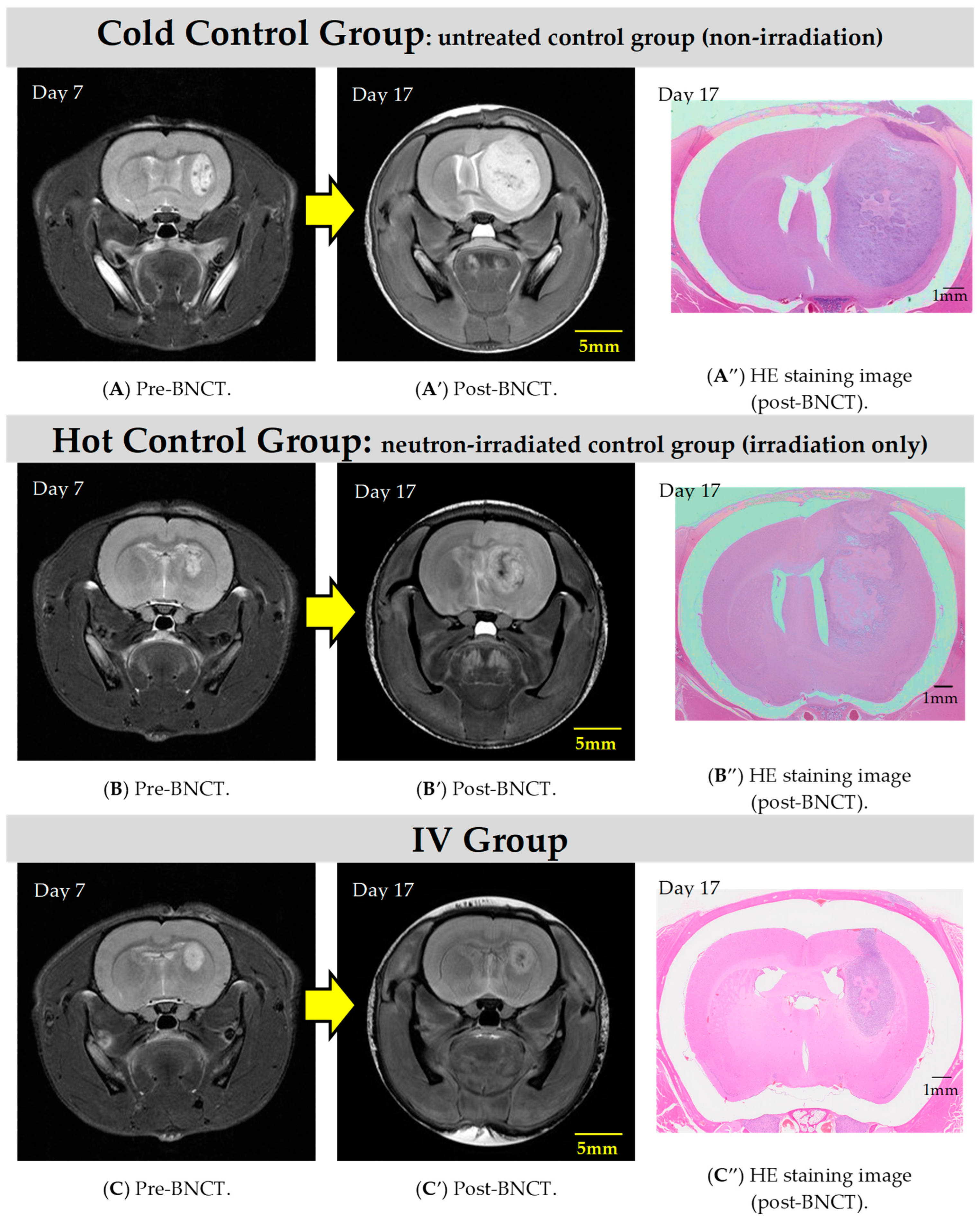
| Cold control group ** | ◯ | A | - | - | A′ | A″ |
| Hot control group *** | 〇 | B | - | 20 min | B′ | B″ |
| IV group | 〇 | C | 350 mg/kg | 20 min | C′ | C″ |
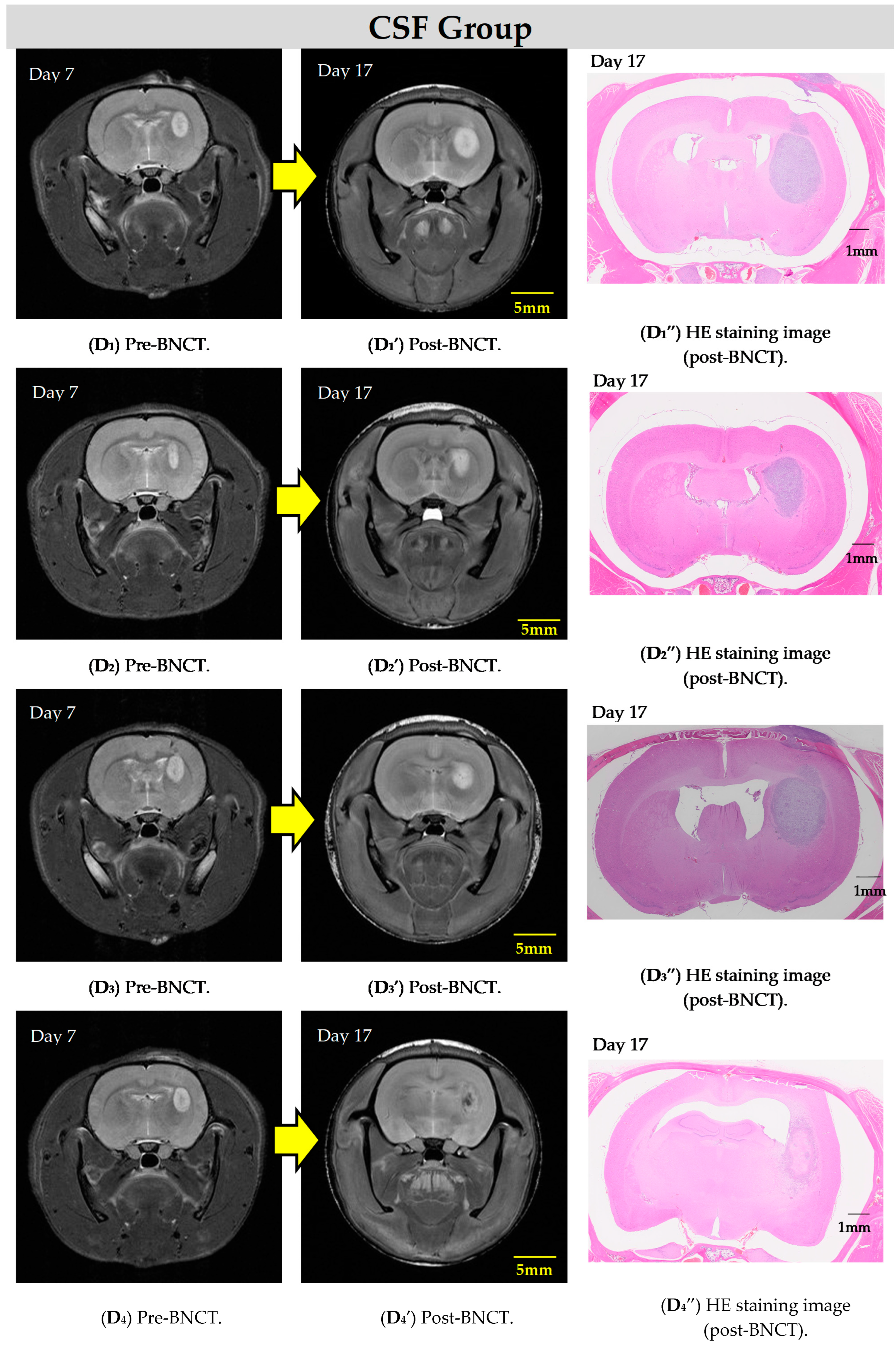
| CSF group | 〇 | D | 16 mg/kg | 20 min | D′ | D″ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kusaka, S.; Voulgaris, N.; Onishi, K.; Ueda, J.; Saito, S.; Tamaki, S.; Murata, I.; Takata, T.; Suzuki, M. Therapeutic Effect of Boron Neutron Capture Therapy on Boronophenylalanine Administration via Cerebrospinal Fluid Circulation in Glioma Rat Models. Cells 2024, 13, 1610. https://doi.org/10.3390/cells13191610
Kusaka S, Voulgaris N, Onishi K, Ueda J, Saito S, Tamaki S, Murata I, Takata T, Suzuki M. Therapeutic Effect of Boron Neutron Capture Therapy on Boronophenylalanine Administration via Cerebrospinal Fluid Circulation in Glioma Rat Models. Cells. 2024; 13(19):1610. https://doi.org/10.3390/cells13191610
Chicago/Turabian StyleKusaka, Sachie, Nikolaos Voulgaris, Kazuki Onishi, Junpei Ueda, Shigeyoshi Saito, Shingo Tamaki, Isao Murata, Takushi Takata, and Minoru Suzuki. 2024. "Therapeutic Effect of Boron Neutron Capture Therapy on Boronophenylalanine Administration via Cerebrospinal Fluid Circulation in Glioma Rat Models" Cells 13, no. 19: 1610. https://doi.org/10.3390/cells13191610
APA StyleKusaka, S., Voulgaris, N., Onishi, K., Ueda, J., Saito, S., Tamaki, S., Murata, I., Takata, T., & Suzuki, M. (2024). Therapeutic Effect of Boron Neutron Capture Therapy on Boronophenylalanine Administration via Cerebrospinal Fluid Circulation in Glioma Rat Models. Cells, 13(19), 1610. https://doi.org/10.3390/cells13191610