
A Simplified Screening Model to Predict the Risk of Gestational Diabetes Mellitus in Caucasian and Latin American Pregnant Women

 , , , , , , , , , , , and
, , , , , , , , , , , and
Abstract
1. Introduction
2. Methods
2.1. Population
2.2. Gestational Diabetes Mellitus Diagnosis
2.3. Clinical and Laboratory Parameters
2.4. Lifestyle Evaluation
2.5. Genotype Analysis
2.6. Statistical Analyses
3. Results
3.1. Phenotype Data
3.2. Genotype Data
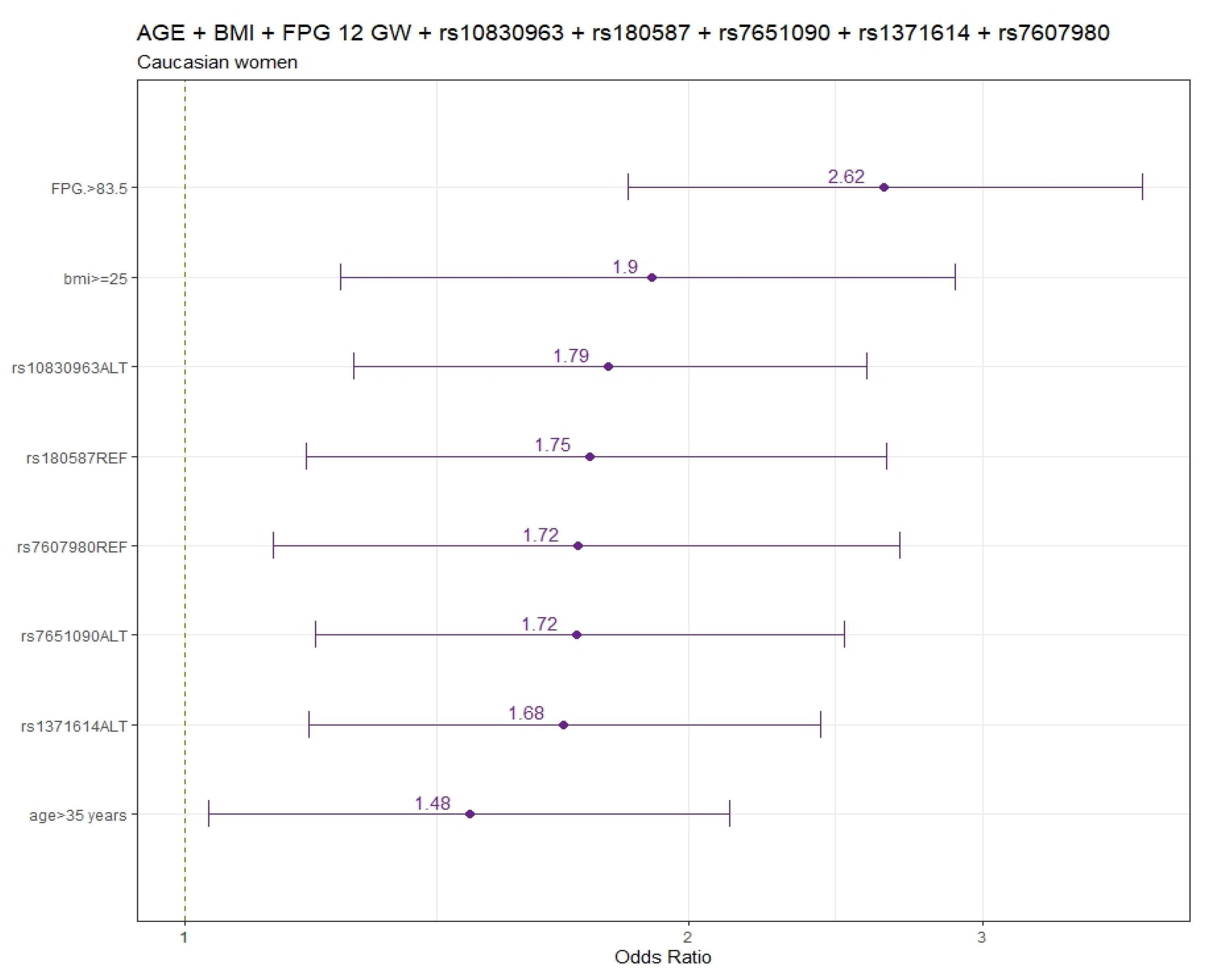
3.2.1. Caucasian Ethnicity Findings
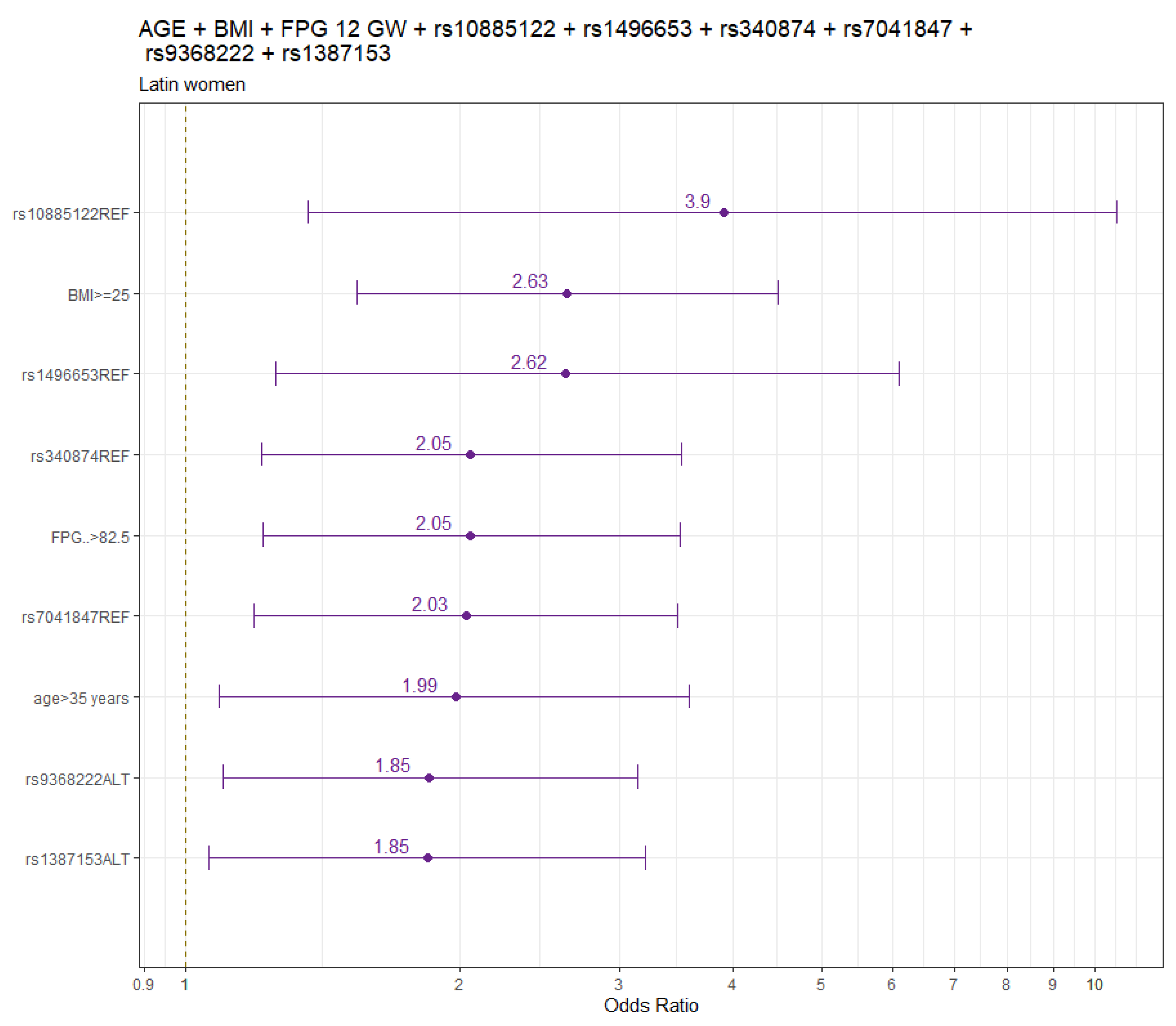
3.2.2. Latin American Ethnicity Findings
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Report of a World Health Organization Consultation. Diagnostic criteria and classification of hyperglycaemia first detected in pregnancy: A World Health Organization Guideline. Diabetes Res. Clin. Pract. 2014, 103, 341–363. [Google Scholar] [CrossRef]
- Wang, H.; Li, N.; Chivese, T.; Werfalli, M.; Sun, H.; Yuen, L.; Hoegfeldt, C.A.; Powe, C.E.; Immanuel, J.; Karuranga, S.; et al. IDF Diabetes Atlas Committee Hyperglycaemia in Pregnancy Special Interest Group. IDF Diabetes Atlas: Estimation of Global and Regional Gestational Diabetes Mellitus Prevalence for 2021 by International Association of Diabetes in Pregnancy Study Group’s Criteria. Diabetes Res. Clin. Pract. 2022, 183, 109050. [Google Scholar] [CrossRef] [PubMed]
- Sweeting, A.; Wong, J.; Murphy, H.R.; Ross, G.P. A Clinical Update on Gestational Diabetes Mellitus. Endocr. Rev. 2022, 43, 763–793. [Google Scholar] [CrossRef] [PubMed]
- HAPO Study Cooperative Research Group; Metzger, B.E.; Lowe, L.P.; Dyer, A.R.; Trimble, E.R.; Chaovarindr, U.; Coustan, D.R.; Hadden, D.R.; McCance, D.R.; Hod, M.; et al. Hyperglycemia and adverse pregnancy outcomes. N. Engl. J. Med. 2008, 358, 1991–2002. [Google Scholar] [CrossRef] [PubMed]
- Dabelea, D.; Hanson, R.L.; Lindsay, R.S.; Pettitt, D.J.; Imperatore, G.; Gabir, M.M.; Roumain, J.; Bennett, P.H.; Knowler, W.C. Intrauterine exposure to diabetes conveys risks for type 2 diabetes and obesity: A study of discordant sibships. Diabetes 2000, 49, 2208–2211. [Google Scholar] [CrossRef] [PubMed]
- Tam, W.H.; Ma, R.C.W.; Ozaki, R.; Li, A.M.; Chan, M.H.M.; Yuen, L.Y.; Lao, T.T.H.; Yang, X.; Ho, C.S.; Tutino, G.E.; et al. In Utero Exposure to Maternal Hyperglycemia Increases Childhood Cardiometabolic Risk in Offspring. Diabetes Care 2017, 40, 679–686. [Google Scholar] [CrossRef] [PubMed]
- Vounzoulaki, E.; Khunti, K.; Abner, S.C.; Tan, B.K.; Davies, M.J.; Gillies, C.L. Progression to type 2 diabetes in women with a known history of gestational diabetes: Systematic review and meta-analysis. BMJ 2020, 369, m1361. [Google Scholar] [CrossRef] [PubMed]
- Sweeting, A.N.; Appelblom, H.; Ross, G.P.; Wong, J.; Kouru, H.; Williams, P.F.; Sairanen, M.; Hyett, J.A. First trimester prediction of gestational diabetes mellitus: A clinical model based on maternal demographic parameters. Diabetes Res. Clin. Pract. 2017, 127, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Hayes, M.G.; Urbanek, M.; Hivert, M.-F.; Armstrong, L.L.; Morrison, J.; Guo, C.; Lowe, L.P.; Scheftner, D.A.; Pluzhnikov, A.; Levine, D.M.; et al. Identification of HKDC1 and BACE2 as genes influencing glycemic traits during pregnancy through genome-wide association studies. Diabetes 2013, 62, 3282–3291, Erratum in Diabetes 2013, 62, 3641. [Google Scholar] [CrossRef] [PubMed]
- Kwak, S.H.; Kim, S.-H.; Cho, Y.M.; Go, M.J.; Cho, Y.S.; Choi, S.H.; Moon, M.K.; Jung, H.S.; Shin, H.D.; Kang, H.M.; et al. A genome-wide association study of gestational diabetes mellitus in Korean women. Diabetes 2012, 61, 531–541. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Bao, W.; Rong, Y.; Yang, H.; Bowers, K.; Yeung, E.; Kiely, M. Genetic variants and the risk of gestational diabetes mellitus: A systematic review. Hum. Reprod. Update 2013, 19, 376–390. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Li, P. Genetic risk score to improve prediction and treatment in gestational diabetes mellitus. Front. Endocrinol. 2022, 13, 955821. [Google Scholar] [CrossRef] [PubMed]
- Assaf-Balut, C.; Garcia De La Torre, N.; Durán, A.; Fuentes, M.; Bordiú, E.; Del Valle, L.; Familiar, C.; Ortolá, A.; Jiménez, I.; Herraiz, M.A.; et al. A Mediterranean diet with additional extra virgin olive oil and pistachios reduces the incidence of gestational diabetes mellitus (GDM): A randomized controlled trial: The St. Carlos GDM prevention study. PLoS ONE 2017, 12, e0185873. [Google Scholar] [CrossRef] [PubMed]
- de la Torre, N.G.; Assaf-Balut, C.; Varas, I.J.; del Valle, L.; Durán, A.; Fuentes, M.; del Prado, N.; Bordiú, E.; Valerio, J.J.; Herraiz, M.A.; et al. Effectiveness of Following Mediterranean Diet Recommendations in the Real World in the Incidence of Gestational Diabetes Mellitus (GDM) and Adverse Maternal-Foetal Outcomes: A Prospective, Universal, Interventional Study with a Single Group. The St Carlos Study. Nutrients 2019, 11, 1210. [Google Scholar] [CrossRef] [PubMed]
- International Association of Diabetes and Pregnancy Study Groups Consensus Panel; Metzger, B.E.; Gabbe, S.G.; Persson, B.; Buchanan, T.A.; Catalano, P.A.; Damm, P.; Dyer, A.R.; de Leiva, A.; Hod, M.; et al. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care 2010, 33, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Schröder, H.; Fitó, M.; Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventós, R.; Ros, E.; Salaverría, I.; Fiol, M.; et al. A short screener is valid for assessing Mediterranean diet adherence among older Spanish men and women. J. Nutr. 2011, 141, 1140–1145. [Google Scholar] [CrossRef] [PubMed]
- Manning, A.K.; Hivert, M.-F.; A Scott, R.; Grimsby, J.L.; Bouatia-Naji, N.; Chen, H.; Rybin, D.; Liu, C.-T.; Bielak, L.F.; Prokopenko, I.; et al. A genome-wide approach accounting for body mass index identifies genetic variants influencing fasting glycemic traits and insulin resistance. Nat. Genet. 2012, 44, 659–669. [Google Scholar] [CrossRef]
- Huerta-Chagoya, A.; Vázquez-Cárdenas, P.; Moreno-Macías, H.; Tapia-Maruri, L.; Rodríguez-Guillén, R.; López-Vite, E.; García-Escalante, G.; Escobedo-Aguirre, F.; Parra-Covarrubias, A.; Cordero-Brieño, R.; et al. Genetic determinants for gestational diabetes mellitus and related metabolic traits in Mexican women. PLoS ONE 2015, 10, e0126408. [Google Scholar] [CrossRef] [PubMed]
- Lowe, W.L., Jr.; Scholtens, D.M.; Sandler, V.; Hayes, M.G. Genetics of Gestational Diabetes Mellitus and Maternal Metabolism. Curr. Diab. Rep. 2016, 16, 15. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Cui, L.; Tam, W.H.; Ma, R.C.W.; Wang, C.C. Genetic variants associated with gestational diabetes mellitus: A meta-analysis and subgroup analysis. Sci. Rep. 2016, 6, 30539. [Google Scholar] [CrossRef]
- Ding, M.; Chavarro, J.; Olsen, S.; Lin, Y.; Ley, S.H.; Bao, W.; Rawal, S.; Grunnet, L.G.; Thuesen, A.C.B.; Mills, J.L.; et al. Genetic variants of gestational diabetes mellitus: A study of 112 SNPs among 8722 women in two independent populations. Diabetologia 2018, 61, 1758–1768. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Levi, A.; Barabash, A.; Valerio, J.; de la Torre, N.G.; Mendizabal, L.; Zulueta, M.; de Miguel, M.P.; Diaz, A.; Duran, A.; Familiar, C.; et al. Genetic variants for prediction of gestational diabetes mellitus and modulation of susceptibility by a nutritional intervention based on a Mediterranean diet. Front. Endocrinol. 2022, 13, 1036088. [Google Scholar] [CrossRef] [PubMed]
- International Diabetes Federation. IDF Diabetes Atlas, 9th ed.; International Diabetes Federation: Brussels, Belgium, 2019; Available online: https://www.diabetesatlas.org/en (accessed on 4 February 2024).
- Fu, J.; Retnakaran, R. The life course perspective of gestational diabetes: An opportunity for the prevention of diabetes and heart disease in women. eClinicalMedicine 2022, 45, 101294. [Google Scholar] [CrossRef] [PubMed]
- Hod, M.; Kapur, A.; Sacks, D.A.; Hadar, E.; Agarwal, M.; Di Renzo, G.C.; Roura, L.C.; McIntyre, H.D.; Morris, J.L.; Divakar, H. The International Federation of Gynecology and Obstetrics (FIGO) Initiative on gestational diabetes mellitus: A pragmatic guide for diagnosis, management, and care. Int. J. Gynaecol. Obstet. 2015, 131 (Suppl. S3), S173–S211. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Diagnostic Criteria and Classification of Hyperglycemia First Detected in Pregnancy; Worlds Health Organization: Geneva, Switzerland, 2013; Available online: https://apps-who.int/ris/handle/10665/85975 (accessed on 18 February 2024).
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2020. Diabetes Care 2020, 43 (Suppl. S1), S14–S31. [Google Scholar] [CrossRef] [PubMed]
- Lamri, A.; Mao, S.; Desai, D.; Gupta, M.; Paré, G.; Anand, S.S. Fine-tuning of Genome-Wide Polygenic Risk Scores and Prediction of Gestational Diabetes in South Asian Women. Sci. Rep. 2020, 10, 8941. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Jia, Y.; Li, Y.; Gu, X.; Wan, G.; Zhang, P.; Zhang, Y.; Jiang, L. Genetic determinants of gestational diabetes mellitus: A case-control study in two independent populations. Acta Diabetol. 2020, 57, 843–852. [Google Scholar] [CrossRef] [PubMed]
- Kawai, V.K.; Levinson, R.T.; Adefurin, A.; Kurnik, D.; Collier, S.P.; Conway, D.; Stein, C.M. A genetic risk score that includes common type 2 diabetes risk variants is associated with gestational diabetes. Clin. Endocrinol. 2017, 87, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Zulueta, M.; Gallardo-Rincón, H.; Martinez-Juarez, L.A.; Lomelin-Gascon, J.; Ortega-Montiel, J.; Montoya, A.; Mendizabal, L.; Arregi, M.; Martinez-Martinez, M.d.L.A.; Romero, E.d.S.C.; et al. Development and validation of a multivariable genotype-informed gestational diabetes prediction algorithm for clinical use in the Mexican population: Insights into susceptibility mechanisms. BMJ Open Diabetes Res. Care 2023, 11, e003046. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Cheong, H.S.; Park, B.-L.; Baik, S.H.; Park, S.; Lee, S.W.; Kim, M.-H.; Chung, J.H.; Choi, J.S.; Kim, M.-Y.; et al. Melatonin receptor 1 B polymorphisms associated with the risk of gestational diabetes mellitus. BMC Med. Genet. 2011, 12, 82. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Wu, Y.; Li, H.; Qi, Q.; Langenberg, C.; Loos, R.J.; Lin, X. MTNR1B rs10830963 is associated with fasting plasma glucose, HbA1C and impaired beta-cell function in Chinese Hans from Shanghai. BMC Med. Genet. 2010, 11, 59. [Google Scholar] [CrossRef] [PubMed]
- Bouatia-Naji, N.; Bonnefond, A.; Cavalcanti-Proença, C.; Sparsø, T.; Holmkvist, J.; Marchand, M.; Delplanque, J.; Lobbens, S.; Rocheleau, G.; Durand, E.; et al. The MTNR1B rs10830963 Variant in Interaction with Pre-Pregnancy BMI is a Pharmacogenetic Marker for the Initiation of Antenatal Insulin Therapy in Gestational Diabetes Mellitus. Int. J. Mol. Sci. 2018, 19, 3734. [Google Scholar] [CrossRef] [PubMed]
- Bouatia-Naji, N.; Bonnefond, A.; Cavalcanti-Proença, C.; Sparsø, T.; Holmkvist, J.; Marchand, M.; Delplanque, J.; Lobbens, S.; Rocheleau, G.; Durand, E.; et al. A variant near MTNR1B is associated with increased fasting plasma glucose levels and type 2 diabetes risk. Nat. Genet. 2009, 41, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Salem, S.D.; Saif-Ali, R.; Ismail, I.S.; Al-Hamodi, Z.; Poh, R.; Muniandy, S. IGF2BP2 alternative variants associated with glutamic acid decarboxylase antibodies negative diabetes in Malaysian subjects. PLoS ONE 2012, 7, e45573. [Google Scholar] [CrossRef] [PubMed]
- Mancina, R.M.; Burza, M.A.; Maglio, C.; Pirazzi, C.; Sentinelli, F.; Incani, M.; Montalcini, T.; Pujia, A.; Congiu, T.; Loche, S.; et al. The COBLL1 C allele is associated with lower serum insulin levels and lower insulin resistance in overweight and obese children. Diabetes Metab. Res. Rev. 2013, 29, 413–416. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Caucasian Group | Latin American | |||||||
|---|---|---|---|---|---|---|---|---|
| Total (n = 1069) | GDM (n = 172) | NGT (n = 897) | p | Total (n = 519) | GDM (n = 83) | NGT (n = 436) | p | |
| Age (years) | 33 ± 4 | 34 ± 5 | 33 ± 4 | 0.083 | 30.9 ± 5.6 | 33 ± 5 | 30.6 ± 4 | <0.001 |
| Family history of T2DM | 293 (27.4) | 61 (35.5) | 248 (27.6) | 0.169 | 127 (24.5) | 18 (21.7) | 109 (25.0) | 0.051 |
| Family history of MetS | 243 (22.7) | 42 (24.4) | 201 (22.4) | 0.115 | 72 (13.9) | 11 (13.3) | 61 (14.0) | 0.053 |
| Previous history of GDM | 40 (3.7) | 12 (7.0) | 28 (3.1) | 0.017 | 16 (3.1) | 9 (10.8) | 7 (1.6) | <0.001 |
| Previous history of Miscarriage | 288 (26.9) | 54 (31.4) | 234 (26.1) | 0.001 | 236 (45.5) | 38 (45.8) | 198 (45.4) | 0.166 |
| Primiparous | 542 (50.7) | 85 (49.4) | 457 (50.9) | 0.757 | 141 (27.2) | 22 (26.5) | 119 (27.3) | 0.282 |
| Pre-pregnancy BMI (kg/m2) | 22.3 ± 3.4 | 23.6 ± 4.0 | 21.9 ± 3.2 | <0.001 | 23.9 ± 3.7 | 25.0 ±3.8 | 23.6 ± 3.5 | 0.002 |
| FPG (mg/dL) | 80 ± 6 | 82 ± 6 | 79 ± 6 | <0.001 | 80.4 ± 6.1 | 82 ± 6 | 80 ± 6 | 0.042 |
| MEDAS score | 5.0 ± 1.7 | 5.0 ± 1.6 | 5.0 ± 1.7 | 0.892 | 4.6 ± 1.8 | 4.7 ± 1.8 | 4.6 ± 1.8 | 0.529 |
| AUC | Threshold | Sensitivity | Specificity | PPV | NPV | |
|---|---|---|---|---|---|---|
| Age | 0.535 | 0.167 | 0.4207 | 0.6491 | 0.187 | 0.8539 |
| Age + Pre-pregnancy BMI | 0.574 | 0.199 | 0.2561 | 0.8538 | 0.2516 | 0.857 |
| Age + Pre-Pregnancy BMI + FPG 12 GW | 0.644 | 0.180 | 0.561 | 0.6795 | 0.250 | 0.8892 |
| Age + Pre-pregnancy BMI + rs10830963 + rs7651090 + rs180587 + rs7607980 + rs1371614 + rs3783347 | 0.684 | 0.137 | 0.7439 | 0.5333 | 0.2346 | 0.9162 |
| Age + Pre-pregnancy BMI + FPG 12 GW+ rs10830963 + rs180587 + rs7607980 + rs7651090 + rs1371614 | 0.714 | 0.159 | 0.6646 | 0.6901 | 0.2919 | 0.9149 |
| AUC | Threshold | Sensitivity | Specificity | PPV | NPV | |
|---|---|---|---|---|---|---|
| Age | 0.543 | 0.182 | 0.7494 | 0.7916 | 0.217 | 0.8521 |
| Age + pre-pregnancy BMI | 0.651 | 0.134 | 0.6914 | 0.5831 | 0.2448 | 0.9071 |
| Age + pre-pregnancy BMI + FPG 12 GW | 0.685 | 0.133 | 0.7975 | 0.4771 | 0.225 | 0.9254 |
| Age + pre-pregnancy BMI + rs10830963 + rs7651090 + rs7607980 + rs1371614 + rs180587 + rs3783347 | 0.745 | 0.156 | 0.6914 | 0.5831 | 0.2446 | 0.9065 |
| Age + pre-pregnancy BMI + FPG 12 GW + rs10885122 + rs1496653 + rs340874 + rs7041847 + rs9368222 + rs1387153 | 0.760 | 0.195 | 0.6203 | 0.8072 | 0.3792 | 0.9174 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arnoriaga-Rodríguez, M.; Serrano, I.; Paz, M.; Barabash, A.; Valerio, J.; del Valle, L.; O’Connors, R.; Melero, V.; de Miguel, P.; Diaz, Á.; et al. A Simplified Screening Model to Predict the Risk of Gestational Diabetes Mellitus in Caucasian and Latin American Pregnant Women. Genes 2024, 15, 482. https://doi.org/10.3390/genes15040482
Arnoriaga-Rodríguez M, Serrano I, Paz M, Barabash A, Valerio J, del Valle L, O’Connors R, Melero V, de Miguel P, Diaz Á, et al. A Simplified Screening Model to Predict the Risk of Gestational Diabetes Mellitus in Caucasian and Latin American Pregnant Women. Genes. 2024; 15(4):482. https://doi.org/10.3390/genes15040482
Chicago/Turabian StyleArnoriaga-Rodríguez, María, Irene Serrano, Mateo Paz, Ana Barabash, Johanna Valerio, Laura del Valle, Rocio O’Connors, Verónica Melero, Paz de Miguel, Ángel Diaz, and et al. 2024. "A Simplified Screening Model to Predict the Risk of Gestational Diabetes Mellitus in Caucasian and Latin American Pregnant Women" Genes 15, no. 4: 482. https://doi.org/10.3390/genes15040482
APA StyleArnoriaga-Rodríguez, M., Serrano, I., Paz, M., Barabash, A., Valerio, J., del Valle, L., O’Connors, R., Melero, V., de Miguel, P., Diaz, Á., Familiar, C., Moraga, I., Pazos-Guerra, M., Martínez-Novillo, M., Rubio, M. A., Marcuello, C., Ramos-Leví, A., Matia-Martín, P., & Calle-Pascual, A. L. (2024). A Simplified Screening Model to Predict the Risk of Gestational Diabetes Mellitus in Caucasian and Latin American Pregnant Women. Genes, 15(4), 482. https://doi.org/10.3390/genes15040482