Building Performance Evaluation of a New Hospital Building in the UK: Balancing Indoor Environmental Quality and Energy Performance

 ,
,  , , , ,
, , , ,  ,
,  ,
,
Abstract
1. Introduction
1.1. IAQ and Other Related IEQ Parameters
1.2. IEQ in Hospital Buildings
1.3. IEQ Performance Objectives in Hospital Buildings
1.4. Energy Related Performance and Potential Issues in Hospital Buildings
2. Method
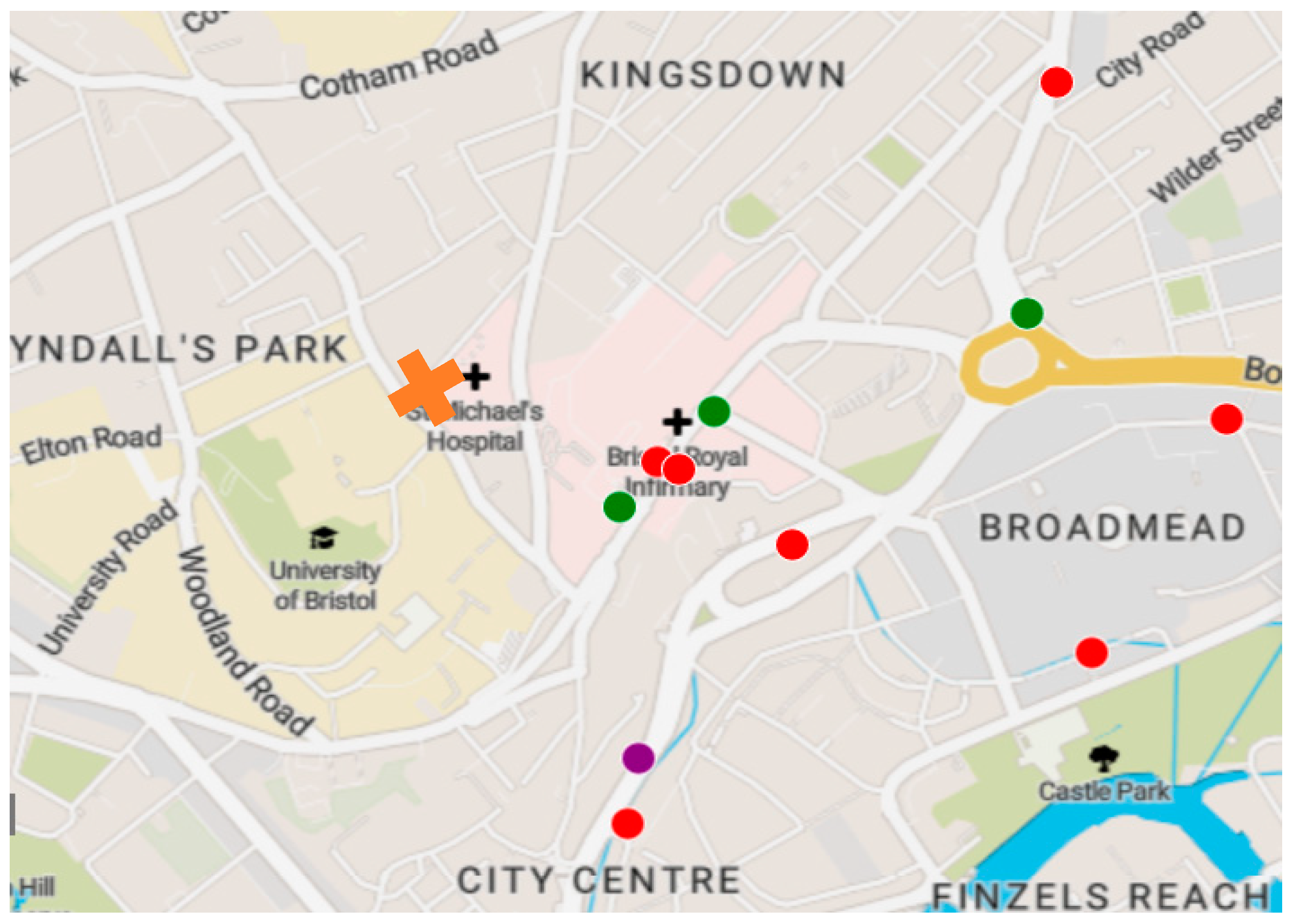
2.1. Case Study Context
2.2. Scope of Monitoring for the Case Study
2.3. Building Design Characteristics
2.4. Data Collection
3. Building performance results
3.1. IEQ Performance
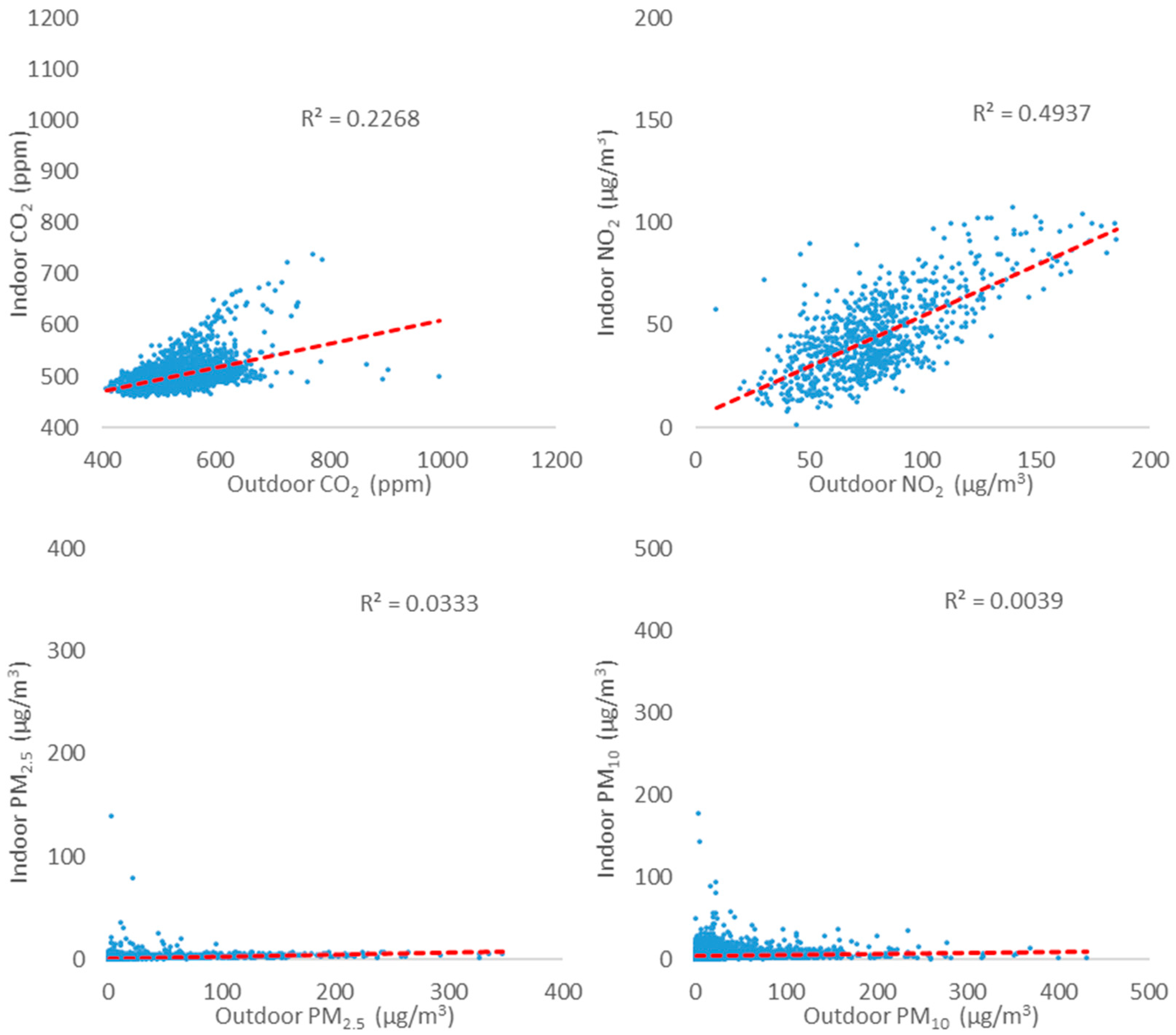
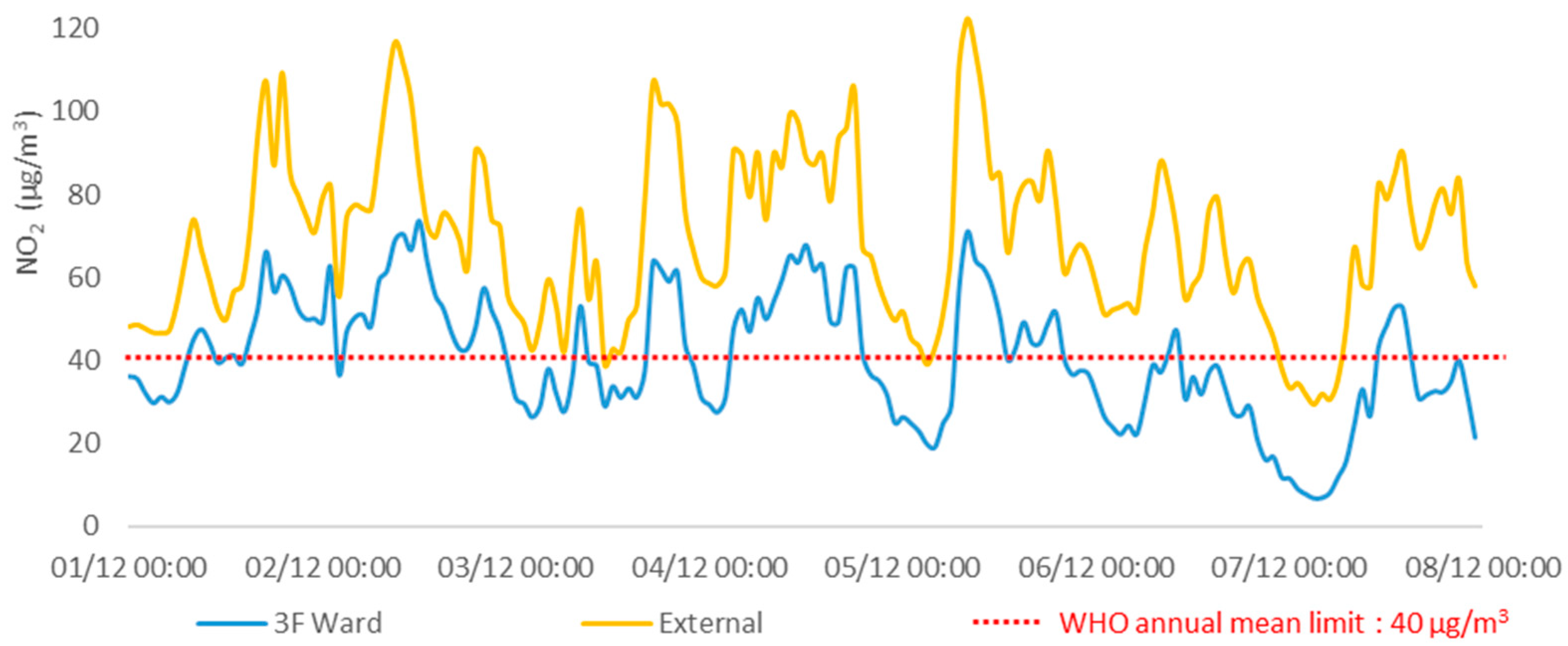
3.1.1. Indoor Air Quality
3.1.2. Thermal Comfort
3.1.3. Acoustics
3.1.4. Lighting
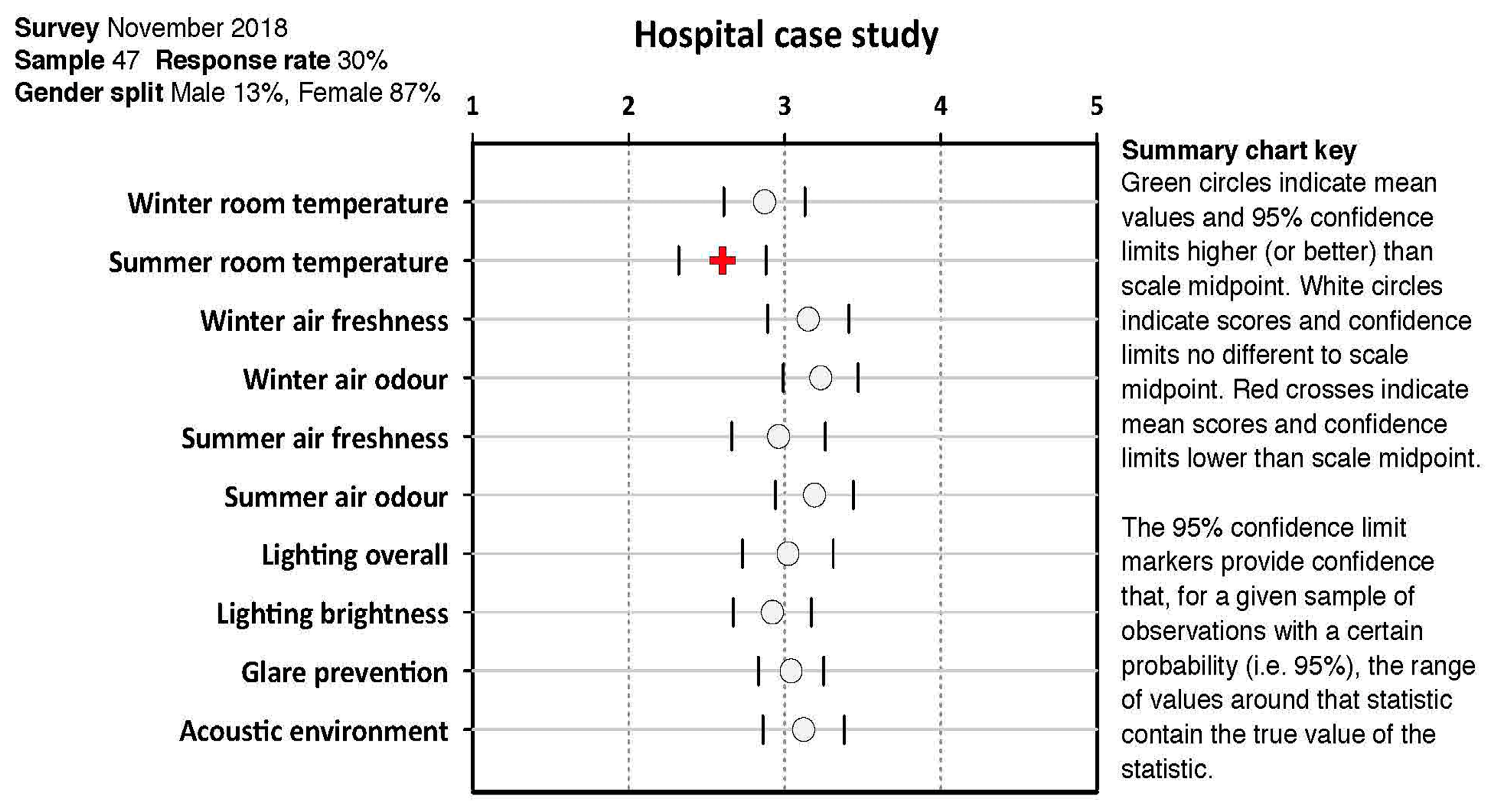
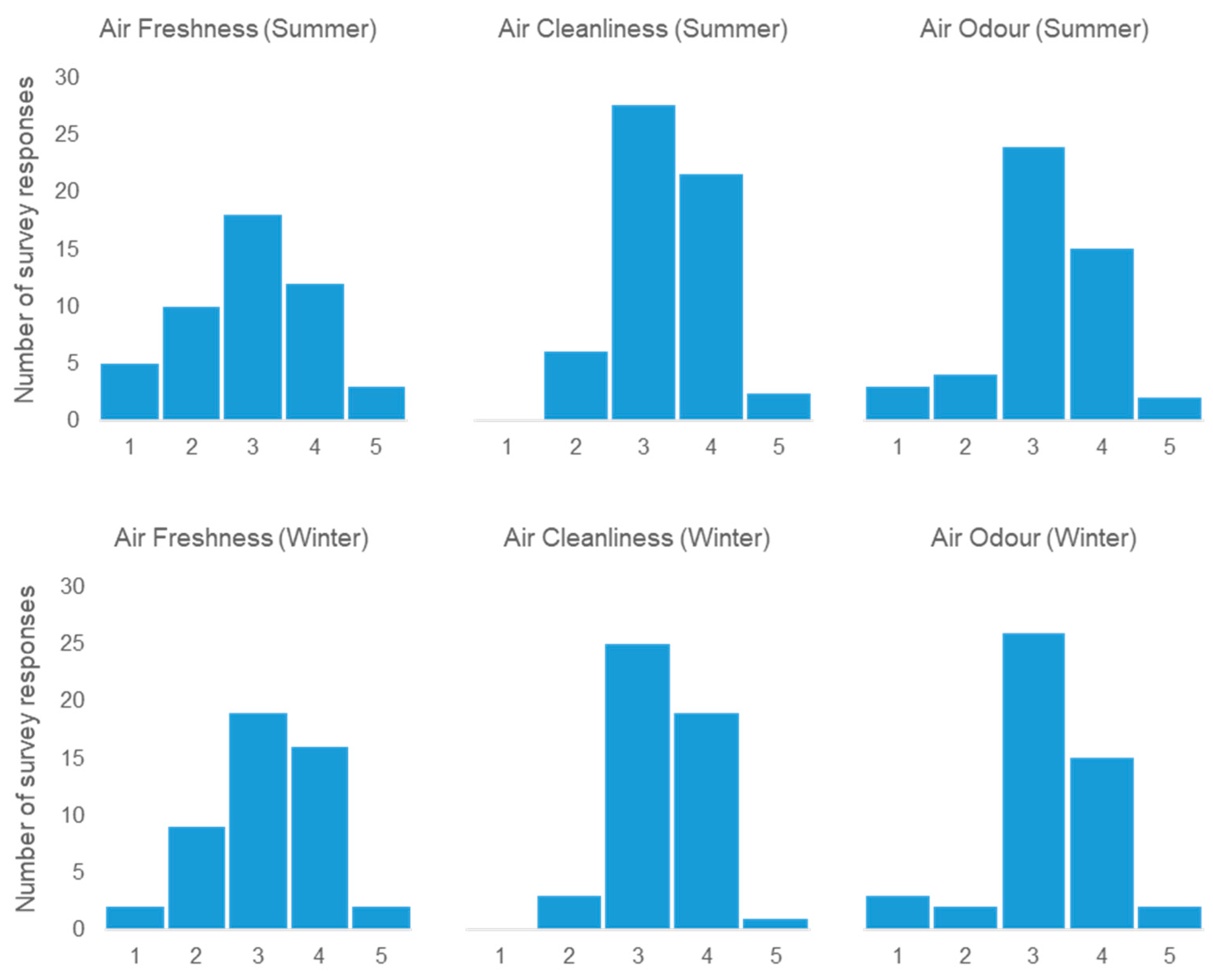
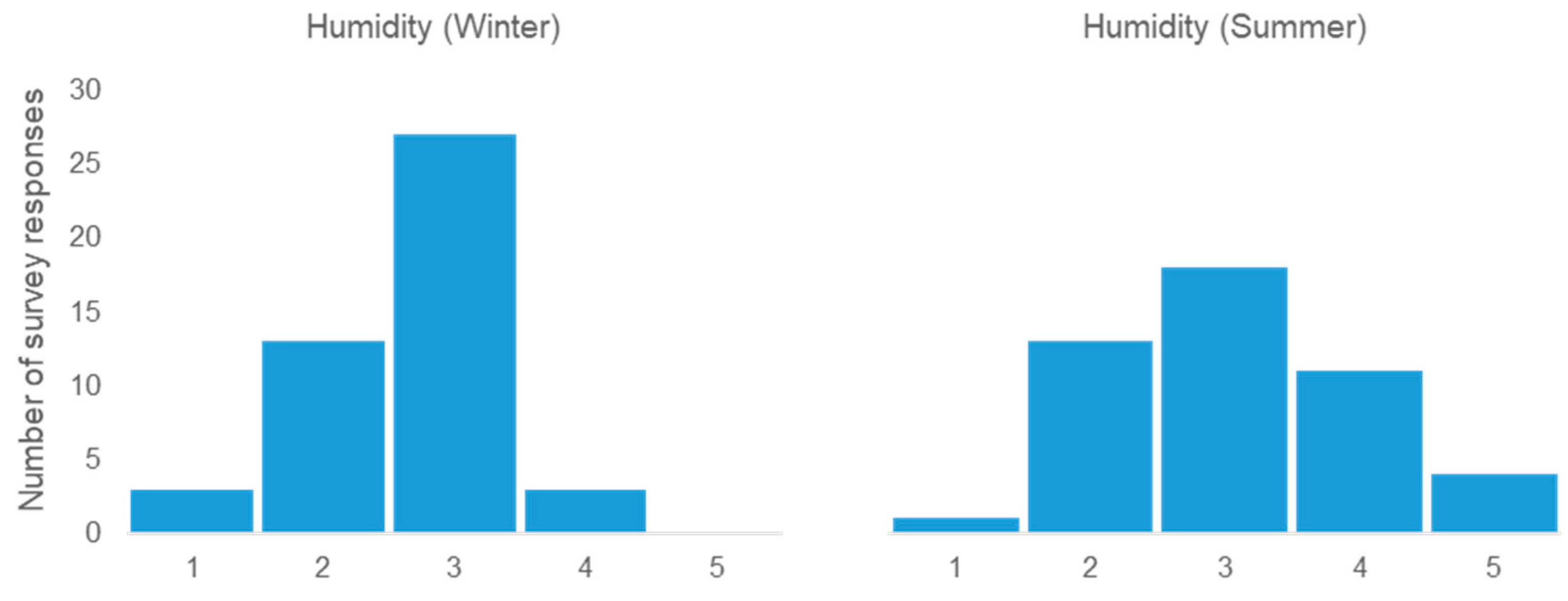
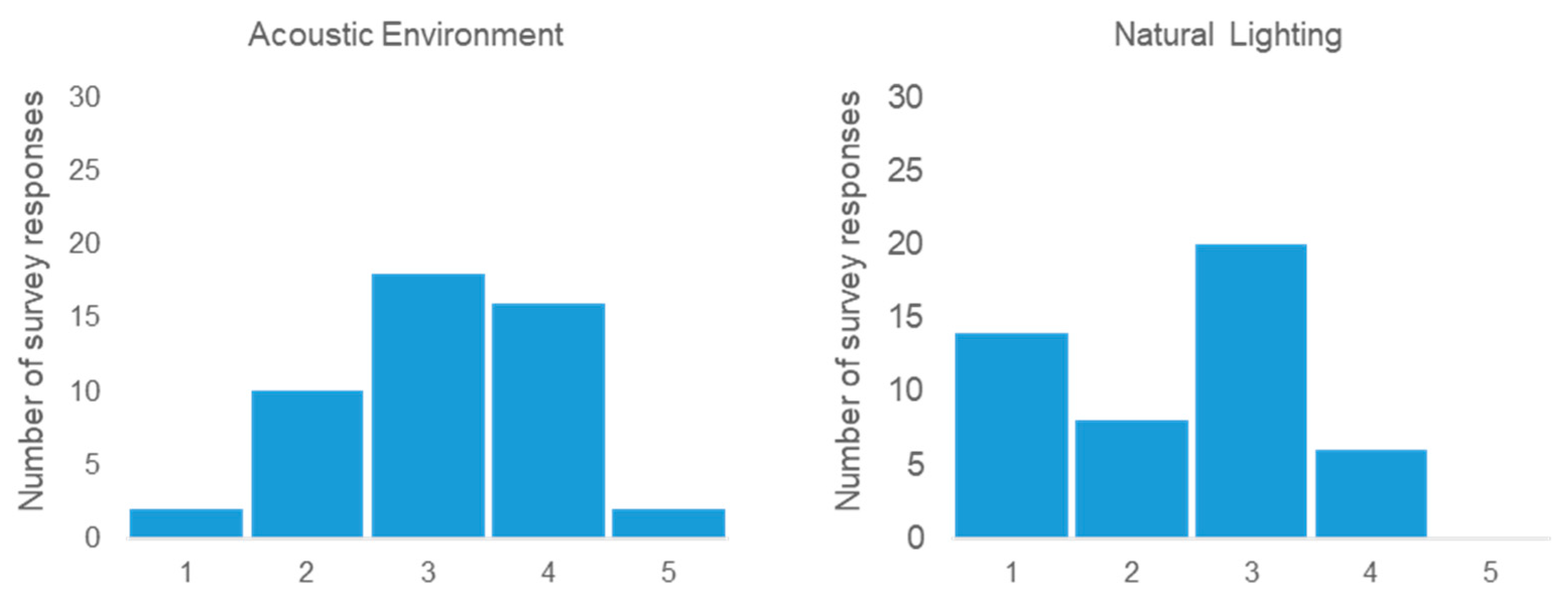
3.2. Occupant Feedback Results
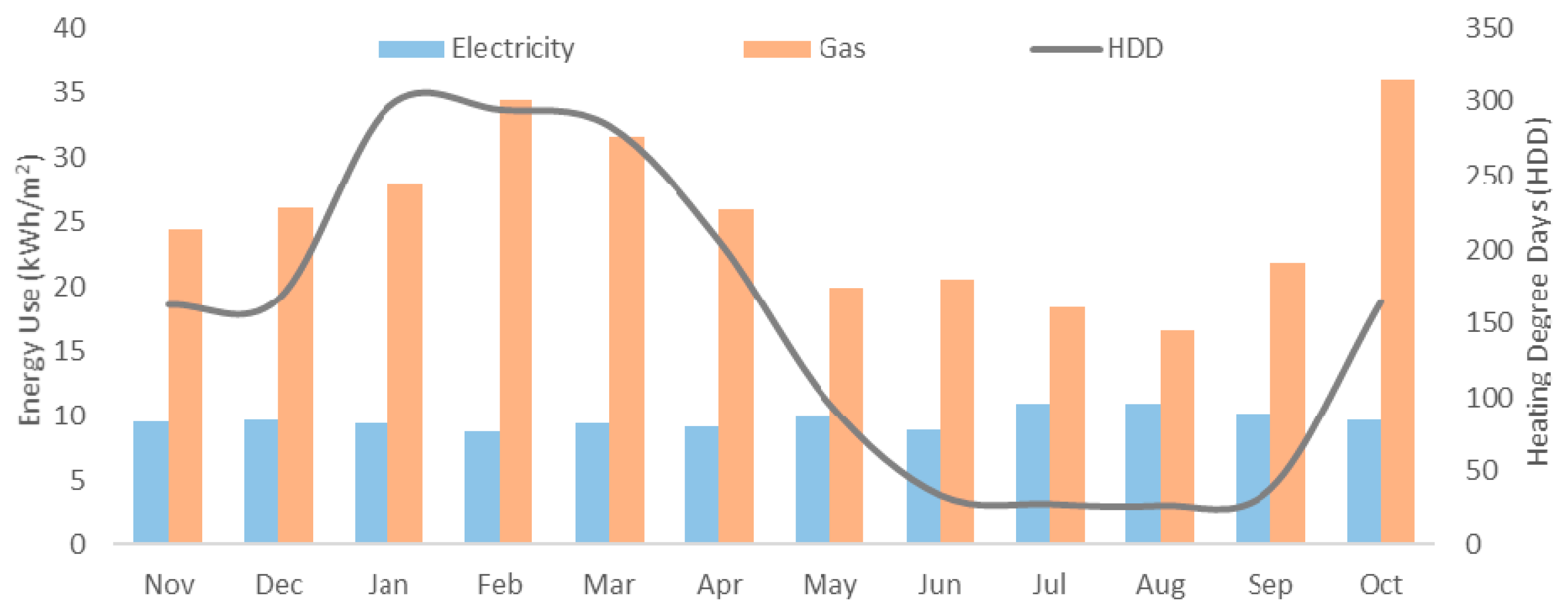
3.3. Energy Performance
4. Discussion
4.1. IEQ
4.2. Energy
4.3. Lessons Learned
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Walton, H.; Dajnak, D.; Beevers, S.; Williams, M.; Watkiss, P.; Hunt, A. Understanding Health Impacts of Air Pollution in London; King’s College London: London, UK, 2015. [Google Scholar]
- Department of Health. Health Technical Memorandum 07-02: EnCO2de 2015—Making Energy Work in Healthcare; Department of Health: London, UK, 2015.
- Hong, S.-M.; Steadman, P. An Analysis of Display Energy Certificated for Public Buildings, 2008-2012; Chartered Institution of Building Services Engineers (CIBSE): London, UK, 2013. [Google Scholar]
- Sheppy, M.; Pless, S.; Kung, F. Healthcare Energy End-Use Monitoring; National Renewable Energy Laboratory (NREL): Golden, Colorado, 2014. [Google Scholar]
- Wyon, D.P.; Wargocki, P. How Indoor Environment Affects Performance. ASHRAE J. 2013, 55, 46–52. [Google Scholar]
- Chatzidiakou, L.; Mumovic, D.; Dockrell, J. The Effects of Thermal Conditions and Indoor Air Quality on Health, Comfort and Cognitive Performance of Students; The Bartlett, UCL Faculty of the Built Environment, UCL Institute for Environmental Design and Engineering: London, UK, 2014. [Google Scholar]
- Al Horr, Y.; Arif, M.; Katafygiotou, M.; Mazroei, A.; Kaushik, A.; Elsarrag, E. Impact of indoor environmental quality on occupant well-being and comfort: A review of the literature. Int. J. Sustain. Built Environ. 2016, 5, 1–11. [Google Scholar] [CrossRef]
- Tuohy, P.G.; Murphy, G.B. Are current design processes and policies delivering comfortable low carbon buildings? Arch. Sci. Rev. 2015, 58, 39–46. [Google Scholar] [CrossRef]
- Fabbri, K.; Tronchin, L. Indoor Environmental Quality in Low Energy Buildings. Energy Procedia 2015, 78, 2778–2783. [Google Scholar] [CrossRef]
- Phillips, T.J.; Levin, H. Indoor environmental quality research needs for low-energy homes. Sci. Technol. Built Environ. 2015, 21, 80–90. [Google Scholar] [CrossRef]
- Xie, H.; Kang, J.; Tompsett, R. The impacts of environmental noise on the academic achievements of secondary school students in Greater London. Appl. Acoust. 2011, 72, 551–555. [Google Scholar] [CrossRef]
- Public Health England. Health Matters: Air Pollution; Public Health England: London, UK, 2018.
- IOM (Institute of Medicine). Clearing the Air: Asthma and Indoor Air Exposures; National Academy Press: Washington, DC, USA, 2000. [Google Scholar]
- COMEAP. The Mortality Effects of Long-Term Exposure to Particulate Air Pollution in the UK; Health Protection Agency and Committee on the Medical Effects of Air Pollutants: London, UK, 2010. [Google Scholar]
- COMEAP. Nitrogen Dioxide: Effects on Mortality; Public Health England and Committee on the Medical Effects of Air Pollutants: London, UK, 2018.
- BCC; AQCL. Health Impacts of Air Pollution in Bristol; Bristol City Council has Commissioned Air Quality Consultants Ltd.: Bristol, UK, 2017. [Google Scholar]
- COMEAP. Review of the UK Air Quality Index: A Report by the Committee on the Medical Effects of Air Pollutants; Health Protection Agency, The Committee on the Medical Effects of Air Pollutant: London, UK, 2011. [Google Scholar]
- Larsen, T.S.; Daniels, O.; Jensen, R.L. Evaluation of the Indoor Environment in 8 Danish Passive Houses; In Proceedings of the Passivhus Norden 2012, Trondheim, Norway, 2012.
- Maivel, M.; Kurnitski, J.; Kalamees, T. Field survey of overheating problems in Estonian apartment buildings. Arch. Sci. Rev. 2015, 58, 1–10. [Google Scholar] [CrossRef]
- Logue, J.M.; McKone, T.E.; Sherman, M.H.; Singer, B.C. Hazard assessment of chemical air contaminants measured in residences. Indoor Air 2011, 21, 92–109. [Google Scholar] [CrossRef]
- Abadie, M.; Wargocki, P. Indoor Air Quality Design and Control in Low-energy Residential Buildings, Subtask 1, Defining the metrics; IEA EBC Annex 68, The Technical University of Denmark and International Energy Agency, INIVE EEIG: Lozenberg, Belgium, 2017. [Google Scholar]
- De Giuli, V.; Zecchin, R.; Salmaso, L.; Corain, L.; De Carli, M. Measured and perceived indoor environmental quality: Padua Hospital case study. Build. Environ. 2013, 59, 211–226. [Google Scholar] [CrossRef]
- Fifield, L.-J. Monitoring UK Hospital Building Type Performance. PhD Thesis, Loughborough University, Loughborough, UK, 2016. [Google Scholar]
- Public Health England (PHE). Heatwave Plan for England: Protecting Health and Reducing Harm from Severe Heat and Heatwaves; Public Health England: London, UK, 2018. [Google Scholar]
- Alan, S.C.; Lomas, K.J.; Giridharan, R.; Fair, A. Building resilience to overheating into 1960’s UK hospital buildings within the constraint of the national carbon reduction target: Adaptive strategies. Build. Environ. 2012, 55, 73–95. [Google Scholar]
- British Lung Foundation. Toxic Air at the Door of the NHS; British Lung Foundation: London, UK, 2018. [Google Scholar]
- Castres, P.; Dajnak, D.; Lott, M.; Watts, N. Most London hospitals and clinics exceed air pollution limits. Br. Med J. 2017, 357, j2855. [Google Scholar] [CrossRef] [PubMed]
- BSI. BS EN 16798-1:2019 Energy Performance of Buildings: Ventilation for Buildings. British Standards Institution: London, UK, 2019. [Google Scholar]
- BSI. Indoor Environmental Input Parameters for Design and Assessment of Energy Performance of Buildings Addressing Indoor Air Quality, Thermal Environment, Lighting and Acoustics; British Standards Institution: London, UK, 2007. [Google Scholar]
- Department of Health. Heating and Ventilation Systems Health Technical Memorandum 03-01: Specialised Ventilation for Healthcare Premises; Department of Health: London, UK, 2007. [Google Scholar]
- IEA; TUD. Indoor Air Quality Design and Control in Low-Energy Residential Buildings-Annex 68|Subtask 1: Defining the Metrics; INIVE EEIG for International Energy Agency and The Technical University of Denmark: Lozenberg, UK, 2017. [Google Scholar]
- PHE. Indoor Air Quality Guidelines for Selected Volatile Organic Compounds (VOCs) in the UK.; Public Health England: London, UK, 2019.
- WHO. WHO Air Quality Guidelines for Particulate Matter, Ozone, Nitrogen Dioxide and Sulfur Dioxide; World Health Organisation Regional Office for Europe: Copenhagen, Denmark, 2005. [Google Scholar]
- WHO. WHO Guidelines for Indoor Air Quality: Selected Pollutants; World Health Organisation Regional Office for Europe: Copenhagen, Denmark, 2010. [Google Scholar]
- Department of Health. Acoustics Health Technical Memorandum 08-01; Department of Health: London, UK, 2013.
- BRECSU. Energy Consumption Guide 72: Energy Consumption in Hospitals; Building Research Energy Conservation Support Unit (BRECSU): Watford, UK, 1996. [Google Scholar]
- CIBSE. TM 46: Energy Benchmarks; Chartered Institute of Building Services Engineers (CIBSE): London, UK, 2008. [Google Scholar]
- NHS. Digital, Estates Returns Information Collection. 2018. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/estates-returns-information-collection (accessed on 22 January 2019).
- Burman, E.; Hong, S.-M.; Paterson, G.; Kimpian, J.; Mumovic, D. A comparative study of benchmarking approaches for non-domestic buildings: Part 2—Bottom-up approach. Int. J. Sustain. Built Environ. 2014, 3, 247–261. [Google Scholar] [CrossRef]
- Morgenstern, P.; Raslan, R.; Ruyssevelt, P. Reducing Hospital Electricity Use: An End-Use Perspective. In Proceedings of the 9th International Conference on Improving Energy Efficiency in Commercial Buildings and Smart Communities, Frankfurt, Germany, 16–18 March 2016. [Google Scholar]
- DCLG. Approved Document L2A: Conservation of Fuel and Power in New Buildings Other Than Dwellings; Department for Communities and Local Government: London, UK, 2013. [Google Scholar]
- CIBSE. TM54: Evaluating Operational Energy Performance of Buildings at the Design Stage; The Chartered Institution of Building Services Engineers (CIBSE): London, UK, 2013. [Google Scholar]
- Morgenstern, P.; Li, M.; Raslan, R.; Ruyssevelt, P.; Wright, A. Benchmarking acute hospitals: Composite electricity targets based on departmental consumption intensities? Energy Build. 2016, 118, 277–290. [Google Scholar] [CrossRef]
- Kimpian, J.; Chisholm, S. Tracking Design and Actual Energy Use: CarbonBuzz, an RIBA CIBSE platform. In Proceedings of the PLEA 2011, Louvain-la-Neuve, Belgium, 13–15 July 2011. [Google Scholar]
- Burman, E.; Rigamonti, D.; Kimpain, J.; Mumovic, D. Performance gap and thermal modelling: A comparison of simulation results and actual energy performance for an academy in North-West England. In Proceedings of the First Building Simulation and Optimization Conference, Loughborough, UK, 10–11 September 2012. [Google Scholar]
- BCC. 2020 Air Quality Annual Status Report (ASR); Bristol City Council: Bristol, UK, 2020.
- BCC. Air Quality Dashboard. Open Data Bristol; 2020. Available online: https://opendata.bristol.gov.uk/pages/air-quality-dashboard-new/air-quality-now#map. (accessed on 20 November 2020).
- Chamseddine, A.; Alameddine, I.; Hatzopoulou, M.; El-Fadel, M. Seasonal variation of air quality in hospitals with indoor-outdoor correlations. Build. Environ. 2019, 148, 689–700. [Google Scholar] [CrossRef]
- CIBSE. CIBSE Guide A: Environmental Design; The Chartered Institution of Building Services Engineers: London, UK, 2015. [Google Scholar]
- ISO/TS 12913-2:2018. Acoustics—Soundscape—Part 2: Data Collection and Reporting Requirements; International Organization for Standardization: Geneva, Switzerland, 2018. [Google Scholar]
- BSI. BS 667: Illuminance Meters. Requirements and Test Methods; British Standards Institution: London, UK, 2005. [Google Scholar]
- Chen, C.; Zhao, B. Review of relationship between indoor and outdoor particles: I/O ratio, infiltration factor and penetration factor. Atmospheric Environ. 2011, 45, 275–288. [Google Scholar] [CrossRef]
- DECC. Energy Consumption in the UK (2018) Chapter 5: Service Sector Energy Consumption in the UK between 1970 and 2017; Department of Energy & Climate Change: London, UK, 2018.
- Kukadia, V.; Upton, S. Ensuring Good Indoor Air Quality in Buildings; BRE Trust: Watford, UK, 2019. [Google Scholar]
- Fang, L.; Clausen, G.; Fanger, P.O. Impact of temperature and humidity on perception of indoor air quality. Indoor Air 1998, 8, 80–90. [Google Scholar] [CrossRef]
- Nathanson, T. Indoor Air Quality in Office Buildings: A Technical Guide; Minister of Supply and Services Canada: Ottawa, ON, Canada, 1995. [Google Scholar]
- Taylor, S. Using the Indoor Environment to Contain the Coronavirus; Engineered Systems: Troy, MI, USA, 2020. [Google Scholar]
- Thomas, P.; Aletta, F.; Filipan, K.; Mynsbrugge, T.V.; De Geetere, L.; Dijckmans, A.; Botteldooren, D.; Petrovic, M.; Van De Velde, D.; De Vriendt, P.; et al. Noise environments in nursing homes: An overview of the literature and a case study in Flanders with quantitative and qualitative methods. Appl. Acoust. 2020, 159, 107103. [Google Scholar] [CrossRef]
- Kang, J.; Xie, H. The acoustic environment of intensive care wards based on long period nocturnal measurements. Noise Heal. 2012, 14, 230–236. [Google Scholar] [CrossRef] [PubMed]
- SLL. The SLL Code for Lighting; Society of Light and Lighting: London, UK, 2012. [Google Scholar]
- Nazarian, M.; Price, A.; Demian, P. A Review of Different Approaches to Access and People Circulation within Health-Care Facilities and the Application of Modelling, Simulation and Visualisation; Architectural Management in the Digital Arena (CIB-W096): Vienna, Austria, 2011. [Google Scholar]
- Jain, N.; Burman, E.; Stamp, S.; Mumovic, D.; Davies, M. Cross-sectoral assessment of the performance gap using calibrated building energy performance simulation. Energy Build. 2020, 224, 110271. [Google Scholar] [CrossRef]
- Bawaneh, K.; Nezami, F.G.; Rasheduzzaman, M.; Deken, B. Energy Consumption Analysis and Characterization of Healthcare Facilities in the United States. Energies 2019, 12, 3775. [Google Scholar] [CrossRef]
- CIBSE. TM63: Operational Performance: Building Performance Modelling; The Chartered Institution of Building Services Engineers (CIBSE): London, UK, 2020. [Google Scholar]
- CIBSE. TM61: Operational Performance of Building; The Chartered Institution of Building Services Engineers (CIBSE): London, UK, 2020. [Google Scholar]
- Way, M.; Bordass, B.; Leaman, A.; Bunn, R. The Soft Landings Framework; Building Services Research & Information Association and Usable Build Trust: London, UK, 2009. [Google Scholar]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Season | CO2 | NO2 | PM2.5 | PM10 | |
|---|---|---|---|---|---|
| Non -Heating Season | 3F Ward | 1.05 | 0.66 | 0.04 | 0.20 |
| 4F Ward | 1.10 | 1.12 | 0.12 | 0.35 | |
| 7F Ward | 1.00 | 0.49 | 0.17 | 0.36 | |
| Heating Season | 3F Ward | 1.05 | 0.61 | 0.05 | 0.18 |
| 4F Ward | 1.03 | 1.04 | 0.12 | 0.28 | |
| 7F Ward | 1.07 | 0.51 | 0.19 | 0.30 |
| Pollutant | 3rd Floor (μg/m3) | 4th Floor (μg/m3) | 7th Floor (μg/m3) | Outside (μg/m3) | IEA EBC Annex 68 ELV (μg/m3) | PHE guideline, long-term ELV/Approved Document Part F (μg/m3) |
|---|---|---|---|---|---|---|
| Benzene | <1.9 | <1.9 | <1.9 | 3.4 | 0.2 * | No safe level recommended |
| Toluene | 2.5 ± 0.4 | 2.5 ± 0.4 | <1.6 | 2.30 ± 0.4 | 250.0 | 2300.0 |
| Trichloroethylene | <0.9 | <0.9 | <0.9 | <0.9 | 2.0 | No safe level recommended |
| Tetrachloroethylene | <1.1 | <1.1 | <1.1 | <1.1 | 100.0 | 40.0 |
| Styrene | <1.0 | <1.0 | <1.0 | <1.0 | 30.0 | 850.0 |
| Naphthalene | <0.8 | <0.8 | <0.8 | <0.8 | 2.0 | 3.0 |
| Formaldehyde | 6.3 ± 0.9 | 4.2 ± 0.6 | 4.8 ± 0.7 | 3.6 ± 0.5 | 9.0 | 10.00 |
| NO2 | 28.4 ± 2.2 | 30.2 ± 2.3 | 30.2 ± 2.3 | 37.6 ± 2.9 | 20.0 | 40.0 |
| O3 | 9.5 ± 0.0 | 12.0 ± 0.3 | 11.2 ± 0.2 | 39.9 ± 3.1 | N/A | 100.0 |
| Pollutant | 3rd Floor (μg/m3) | 4th Floor (μg/m3) | 7th Floor (μg/m3) | Outside (μg/m3) | IEA EBC Annex 68 ELV (μg/m3) | PHE guideline, long-term ELV/Approved Document Part F (μg/m3) |
|---|---|---|---|---|---|---|
| Benzene | <1.1 | <1.1 | <1.1 | <1.1 | 0.2 * | No safe level recommended |
| Toluene | 2.0 ± 0.4 | 2.1 ± 0.4 | <0.9 | <0.9 | 250.0 | 2300.0 |
| Trichloroethylene | <0.5 | <0.5 | <0.5 | <0.5 | 2.0 | No safe level recommended |
| Tetrachloroethylene | <0.6 | <0.6 | <0.7 | <0.7 | 100.0 | 40.0 |
| Styrene | <0.6 | <0.6 | <0.6 | <0.6 | 30.0 | 850.0 |
| Naphthalene | 0.6 ± 0.1 | <0.5 | <0.5 | <0.5 | 2.0 | 3.0 |
| Formaldehyde | 3.3 ± 0.5 | 2.7 ± 0.4 | 2.8 ± 0.4 | 1.8 ± 0.3 | 9.0 | 10.0 |
| NO2 | 10.6 ± 0.8 | 11.0 ± 0.9 | 12.2 ± 1.0 | 10.9 ± 0.9 | 20.0 | 40.0 |
| O3 | 16.0 ± 0.3 | 18.2 ± 0.5 | 16.1 ± 0.3 | 44.6 ± 3.2 | N/A | 100.0 |
| Source | Sound Pressure Level (SPL) (dB) | Loudness (soneGF) | Sharpness (acum) | Tonality (tu) | ||||
|---|---|---|---|---|---|---|---|---|
| Left | Right | Left | Right | Left | Right | Left | Right | |
| 3rd floor atrium | 73.5 | 72.9 | 19.7 | 18.7 | 2.22 | 2.08 | 0.0951 | 0.0937 |
| 3rd floor small office | 64.2 | 63.2 | 8.88 | 8.14 | 1.34 | 1.38 | 0.100 | 0.0847 |
| 5th floor large office | 67.2 | 67.9 | 11.2 | 10.8 | 2.08 | 1.99 | 0.0749 | 0.0727 |
| 7th floor treatment room | 62.7 | 62.6 | 7.06 | 7.51 | 1.48 | 1.47 | 0.0558 | 0.0769 |
| 9th floor patient room | 71.1 | 71.3 | 16.7 | 16.0 | 2.13 | 2.00 | 0.0992 | 0.0948 |
| 9th floor quiet room | 63.2 | 63.9 | 6.60 | 6.55 | 1.42 | 1.42 | 0.0541 | 0.0554 |
| Criteria | Energy Use (Gas + Elec) (kWh/m2) | CO2 Emission (kgCO2/m2) * | Diff from Benchmark |
|---|---|---|---|
| Current Performance | 318 (206+112) | 99 | - |
| CIBSE TM46 ** [37] | 510 (420+90) | 130 | 24% Less |
| ECG72 Best Practice [36] | 498 (423+75) | 122 | 19% Less |
| Similar UK hospitals *** [3] | 429 (311+118) | 123 | 19% Less |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jain, N.; Burman, E.; Stamp, S.; Shrubsole, C.; Bunn, R.; Oberman, T.; Barrett, E.; Aletta, F.; Kang, J.; Raynham, P.; et al. Building Performance Evaluation of a New Hospital Building in the UK: Balancing Indoor Environmental Quality and Energy Performance. Atmosphere 2021, 12, 115. https://doi.org/10.3390/atmos12010115
Jain N, Burman E, Stamp S, Shrubsole C, Bunn R, Oberman T, Barrett E, Aletta F, Kang J, Raynham P, et al. Building Performance Evaluation of a New Hospital Building in the UK: Balancing Indoor Environmental Quality and Energy Performance. Atmosphere. 2021; 12(1):115. https://doi.org/10.3390/atmos12010115
Chicago/Turabian StyleJain, Nishesh, Esfand Burman, Samuel Stamp, Clive Shrubsole, Roderic Bunn, Tin Oberman, Edward Barrett, Francesco Aletta, Jian Kang, Peter Raynham, and et al. 2021. "Building Performance Evaluation of a New Hospital Building in the UK: Balancing Indoor Environmental Quality and Energy Performance" Atmosphere 12, no. 1: 115. https://doi.org/10.3390/atmos12010115
APA StyleJain, N., Burman, E., Stamp, S., Shrubsole, C., Bunn, R., Oberman, T., Barrett, E., Aletta, F., Kang, J., Raynham, P., Mumovic, D., & Davies, M. (2021). Building Performance Evaluation of a New Hospital Building in the UK: Balancing Indoor Environmental Quality and Energy Performance. Atmosphere, 12(1), 115. https://doi.org/10.3390/atmos12010115