
Mortality Sensitivity of Cardiovascular, Cerebrovascular, and Respiratory Diseases to Warm Season Climate in Japanese Cities


Abstract
:1. Introduction
2. Materials and Methods
2.1. Epidemiological Data
2.2. Age-Adjusted Mortality
2.3. Climate Data
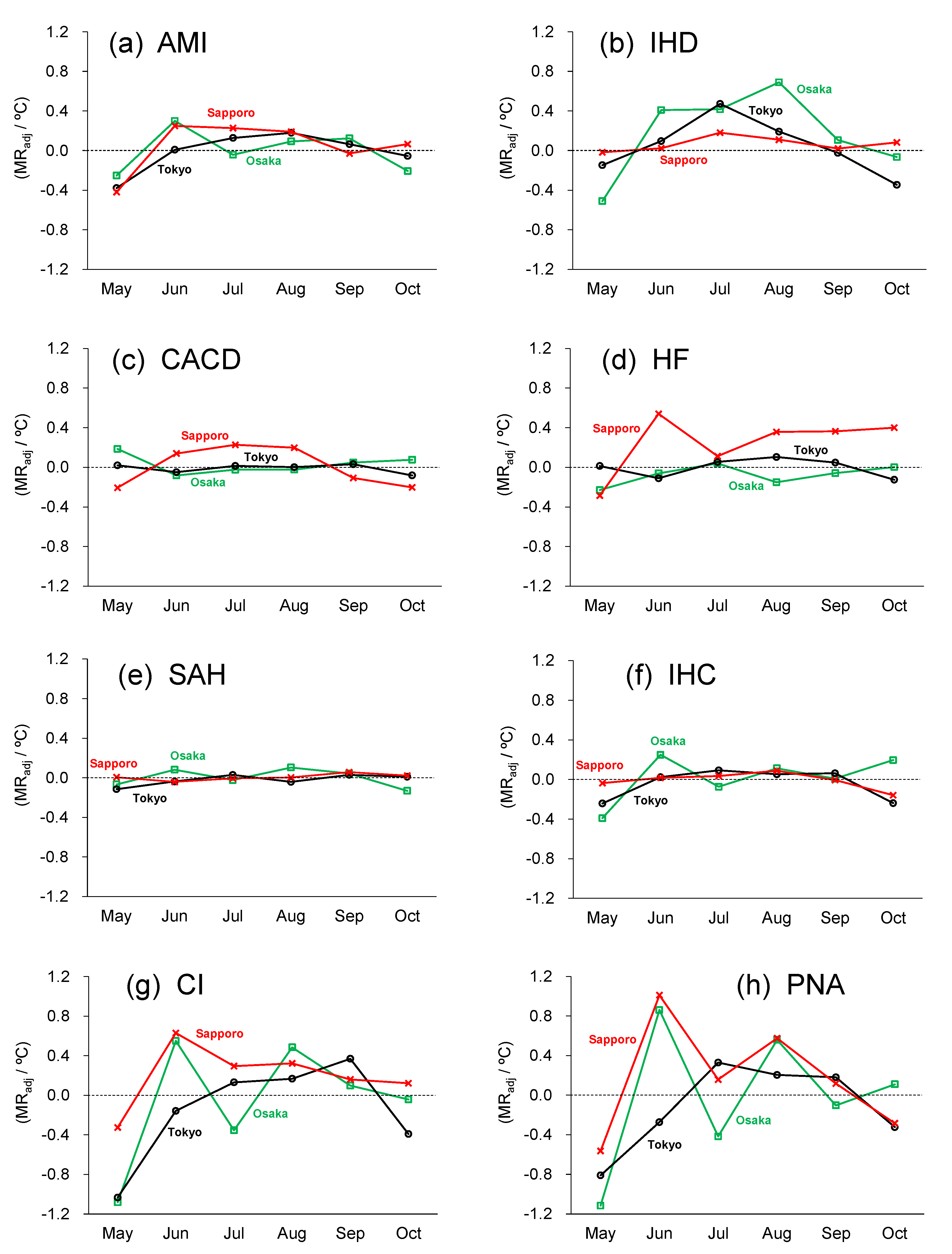
3. Results and Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ostro, B.; Barrera-Gómez, J.; Ballester, J.; Basagaña, X.; Sunyer, J. The impact of future summer temperature on public health in Barcelona and Catalonia, Spain. Int. J. Biometeorol. 2012, 56, 1135–1144. [Google Scholar] [CrossRef] [PubMed]
- Modarres, R.; Ghadami, M.; Naderi, S.; Naderi, M. Future heat stress arising from climate change on Iran’s population health. Int. J. Biometeorol. 2018, 62, 1275–1281. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Yuan, J.; Kopp, R.E. Escalating global exposure to compound heat-humidity extremes with warming. Environ. Res. Lett. 2020, 15, 064003. [Google Scholar] [CrossRef]
- Varquez, A.C.G.; Darmanto, N.S.; Honda, Y.; Ihara, T.; Kanda, M. Future increase in elderly heat-related mortality of a rapidly growing Asian megacity. Sci. Rep. 2020, 10, 9304. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.; Guo, Y.; Ye, T.; Gasparrini, A.; Tong, S.; Overcenco, A.; Urban, A.; Schneider, A.; Entezari, A.; Vicedo-Cabrera, A.M.; et al. Global, regional, and national burden of mortality associated with non-optimal ambient temperatures from 2000 to 2019: A three-stage modelling study. Lancet Planet. Health 2021, 5, e415–e425. [Google Scholar] [CrossRef]
- Liu, L.; Breitner, S.; Pan, X.; Franck, U.; Leitte, A.M.; Wiedensohler, A.; von Klot, S.; Wichmann, H.E.; Peters, A.; Schneider, A. Associations between air temperature and cardio-respiratory mortality in the urban area of Beijing, China: A time-series analysis. Environ. Health 2011, 10, 51. [Google Scholar] [CrossRef] [Green Version]
- de Blois, J.; Kjellstrom, T.; Agewall, S.; Ezekowitz, J.A.; Armstrong, P.W.; Atar, D. The Effects of Climate Change on Cardiac Health. Cardiology 2015, 131, 209–217. [Google Scholar] [CrossRef]
- Achebak, H.; Devolder, D.; Ingole, V.; Ballester, J. Reversal of the seasonality of temperature-attributable mortality from respiratory diseases in Spain. Nat. Commun. 2020, 11, 2457. [Google Scholar] [CrossRef]
- Huang, H.; Deng, X.; Yang, H.; Zhou, X.; Jia, Q. Spatio-temporal mechanism underlying the effect of urban heat island on cardiovascular diseases. Iran. J. Pub. Health 2020, 49, 1455–1466. [Google Scholar] [CrossRef]
- Li, T.; Ban, J.; Horton, R.M.; Bader, D.A.; Huang, G.; Sun, Q.; Kinney, P.L. Heat-related mortality projections for cardiovascular and respiratory disease under the changing climate in Beijing, China. Sci. Rep. 2015, 5, 11441. [Google Scholar] [CrossRef] [Green Version]
- Bunker, A.; Wildenhain, J.; Vandenbergh, A.; Henschke, N.; Rocklöv, J.; Hajat, S.; Sauerborn, R. Effects of air temperature on climate-sensitive mortality and morbidity outcomes in the elderly; a systematic review and meta-analysis of epidemiological evidence. EBioMedicine 2016, 6, 258–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamanaka, S.; Nakamura, Y. Regional differences in the number of patients for circulatory and respiratory diseases and climatical condition. Jpn. J. Biometeor. 1996, 33, 137–145. (In Japanese) [Google Scholar]
- Xu, J.; Inaba, Y. Seasonal and weather influences on cerebrovascular disorder. Chikyu Kankyo 2003, 8, 201–209. (In Japanese) [Google Scholar]
- Hayama, H.; Kamazawa, Y.; Matsumura, R.; Kikuta, K. Influence of meteorological condition and death location on cause of death. Kousei Shihyo 2011, 58, 1–6. (In Japanese) [Google Scholar]
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems 10th Revision. Available online: https://icd.who.int/browse10/2019/en (accessed on 7 November 2021).
- Beck, H.E.; Zimmermann, N.E.; McVicar, T.R.; Vergopolan, N.; Berg, A.; Wood, E.F. Present and future Koppen-Geiger climate classification maps at 1-km resolution. Sci. Data 2018, 5, 180214. [Google Scholar] [CrossRef] [Green Version]
- Honda, Y.; Kabuto, M.; Ono, M.; Uchiyama, I. Determination of optimum daily maximum temperature using climate data. Environ. Health Prev. Med. 2007, 12, 209–216. [Google Scholar] [CrossRef] [Green Version]
- Honda, Y.; Kondo, M.; McGregor, G.; Kim, H.; Guo, Y.-L.; Hijioka, Y.; Yoshikawa, M.; Oka, K.; Takano, S.; Hales, S.; et al. Heat-related mortality risk model for climate change impact projection. Environ. Health Prev. Med. 2014, 19, 56–63. [Google Scholar] [CrossRef]
- Moghadamnia, M.T.; Ardalan, A.; Mesdaghinia, A.; Keshtkar, A.; Naddafi, K.; Yekaninejad, M.S. Ambient temperature and cardiovascular mortality: A systematic review and meta-analysis. PeerJ 2017, 5, e3574. [Google Scholar] [CrossRef]
- Alahmad, B.; Khraishah, H.; Shakarchi, A.F.; Albaghdadi, M.; Rajagopalan, S.; Koutrakis, P.; Jaffer, F.A. Cardiovascular mortality and exposure to heat an inherently hot region: Implications for climate change. Circulation 2020, 141, 1271–1273. [Google Scholar] [CrossRef]
- Lavados, P.M.; Olavarría, V.V.; Hoffmeister, L. Ambient temperature and stroke risk. Stroke 2018, 49, 255–261. [Google Scholar] [CrossRef]
- Lim, Y.-H.; Park, M.-S.; Kim, Y.; Kim, H.; Hong, T.-C. Effects of cold and hot temperature on dehydration: A mechanism of cardiovascular burden. Int. J. Biometeorol. 2015, 59, 1035–1043. [Google Scholar] [CrossRef] [PubMed]
- Keatinge, W.R.; Donaldson, G.C.; Cordioli, E.; Martinelli, M.; Kunst, A.E.; Mackenbach, J.P.; Nayha, S.; Vuori, I. Heat related mortality in warm and cold regions of Europe: Observational study. BMJ 2000, 321, 670. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ICD-10 Code | Disease Name | Abbreviation | |
|---|---|---|---|
| Cardiovascular diseases (CVD) | I21–I22 | Acute myocardial infarction | AMI |
| I20, I23–I25 | Other ischemic heart disease | IHD | |
| I44–I49 | Cardiac arrhythmia and conduction disorder | CACD | |
| I50 | Heart failure | HF | |
| Cerebrovascular diseases (CBD) | I60, I69.0 | Subarachnoid hemorrhage | SAH |
| I61, I69.1 | Intracerebral hemorrhage | ICH | |
| I63, I69.3 | Cerebral infarction | CI | |
| Respiratory diseases (RD) | J12–J18 | Pneumonia | PNA |
| May | Jun | Jul | Aug | Sep | Oct | |
|---|---|---|---|---|---|---|
| max/mean/min | max/mean/min | max/mean/min | max/mean/min | max/mean/min | max/mean/min | |
| Osaka | 24.5/19.7/15.6 | 27.8/23.5/20.0 | 31.6/27.4/24.3 | 33.4/28.8/25.4 | 29.3/25.0/21.7 | 23.3/19.0/15.5 |
| Tokyo (23 wards) | 22.9/18.2/14.0 | 25.5/21.4/18.0 | 29.2/25.0/21.8 | 30.8/26.4/23.0 | 26.9/22.8/19.7 | 21.5/17.5/14.2 |
| Sapporo | 17.3/12.4/8.3 | 21.5/16.7/12.9 | 24.9/20.5/17.3 | 26.4/22.3/19.1 | 22.4/18.1/14.2 | 16.2/11.8/7.5 |
| Osaka | Tokyo (23 Wards) | Sapporo | ||
|---|---|---|---|---|
| Cardiovascular diseases (CVD) | AMI | Sen: +0.12–0.30 Risk: 1.35–1.39 | Sen: +0.13–0.18 Risk: 1.31–1.42 | Sen: +0.19–0.25 Risk: 1.37–1.65 |
| IHD | Sen: +0.41–0.69 Risk: 1.25–1.65 | Sen: +0.19–0.47 Risk: 1.10–1.54 | Sen: +0.11–0.18 Risk: 1.28–1.32 | |
| CACD | -- | -- | Sen: +0.14–0.23 Risk: 1.39–1.63 | |
| HF | -- | -- | Sen: +0.36–0.54 Risk: 1.28–1.41 | |
| Cerebrovascular diseases (CBD) | SAH | -- | -- | -- |
| ICH | -- | -- | -- | |
| CI | Sen: +0.48–0.55 Risk: 1.26–1.41 | Sen: +0.13–0.37 Risk: 1.10–1.34 | Sen: +0.16–0.63 Risk: 1.19–1.76 | |
| Respiratory diseases (RD) | PNA | Sen: +0.56–0.86 Risk: 1.15–1.16 | Sen: +0.33 Risk: 1.21 | Sen: +0.58–1.01 Risk: 1.31–1.54 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ohashi, Y.; Miyata, A.; Ihara, T. Mortality Sensitivity of Cardiovascular, Cerebrovascular, and Respiratory Diseases to Warm Season Climate in Japanese Cities. Atmosphere 2021, 12, 1546. https://doi.org/10.3390/atmos12121546
Ohashi Y, Miyata A, Ihara T. Mortality Sensitivity of Cardiovascular, Cerebrovascular, and Respiratory Diseases to Warm Season Climate in Japanese Cities. Atmosphere. 2021; 12(12):1546. https://doi.org/10.3390/atmos12121546
Chicago/Turabian StyleOhashi, Yukitaka, Akari Miyata, and Tomohiko Ihara. 2021. "Mortality Sensitivity of Cardiovascular, Cerebrovascular, and Respiratory Diseases to Warm Season Climate in Japanese Cities" Atmosphere 12, no. 12: 1546. https://doi.org/10.3390/atmos12121546
APA StyleOhashi, Y., Miyata, A., & Ihara, T. (2021). Mortality Sensitivity of Cardiovascular, Cerebrovascular, and Respiratory Diseases to Warm Season Climate in Japanese Cities. Atmosphere, 12(12), 1546. https://doi.org/10.3390/atmos12121546