An Effective Surrogate Tracer Technique for S. aureus Bioaerosols in a Mechanically Ventilated Hospital Room Replica Using Dilute Aqueous Lithium Chloride

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Biological Surrogates
3. Methodology
3.1. Empty Chamber
3.2. Hospital Single Room Replica
3.3. Aerosol Generation
3.4. Sample Collection and Processing
3.5. Statistical Analyis
4. Results
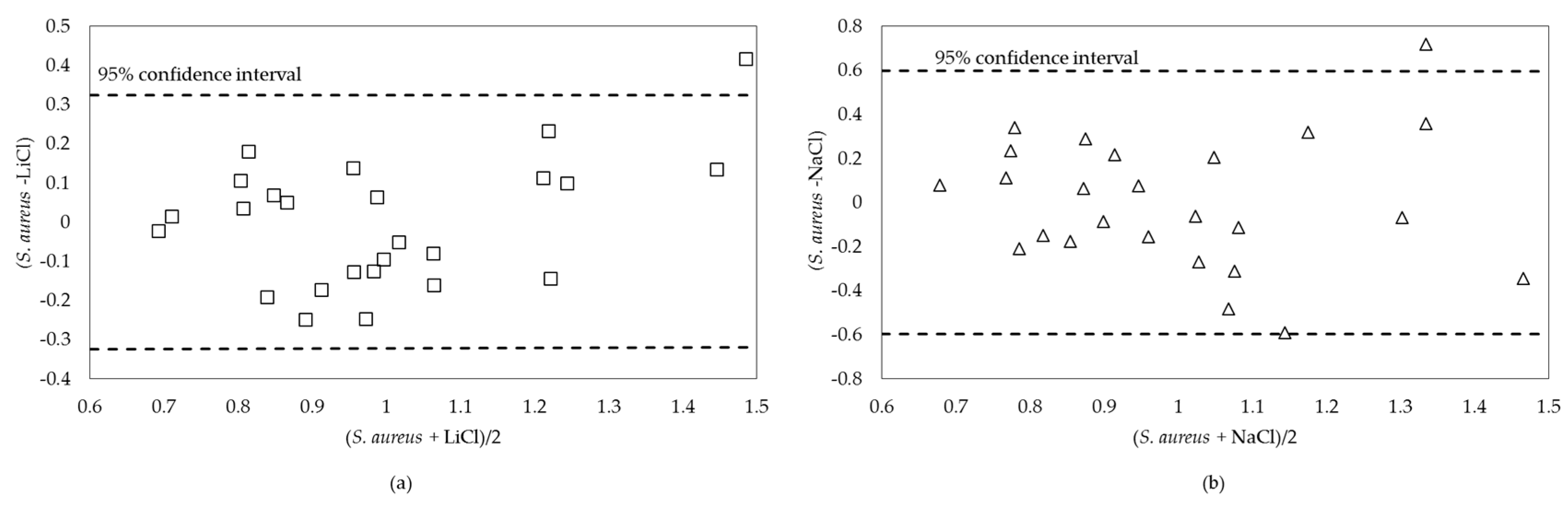
4.1. Precision of Methodology
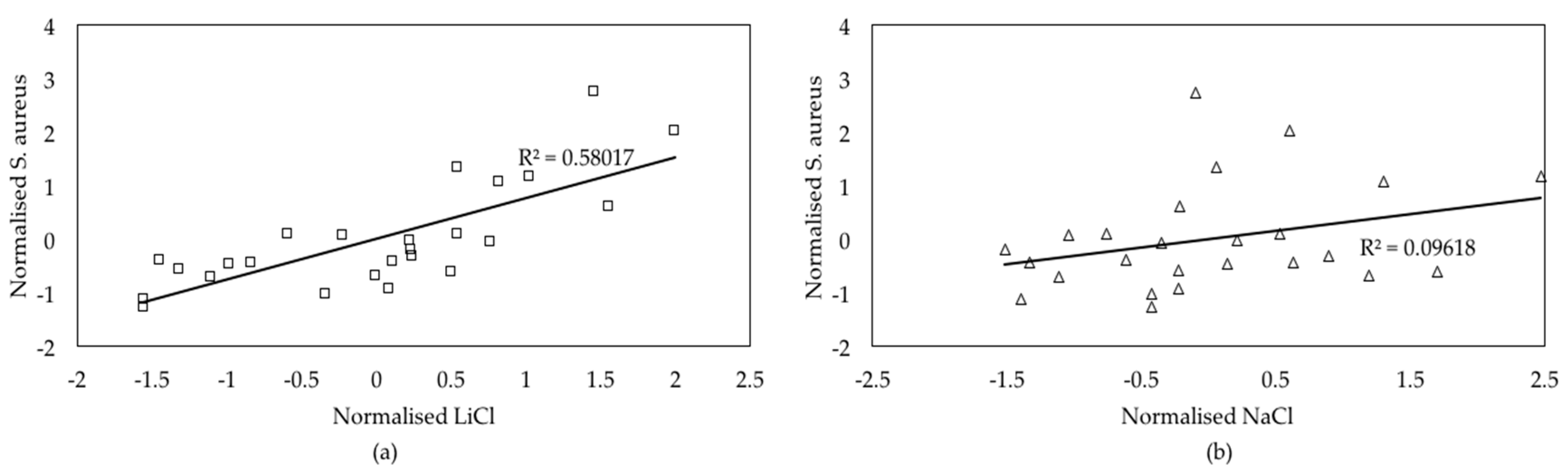
4.2. Replicability and Sensitivity of Experiments
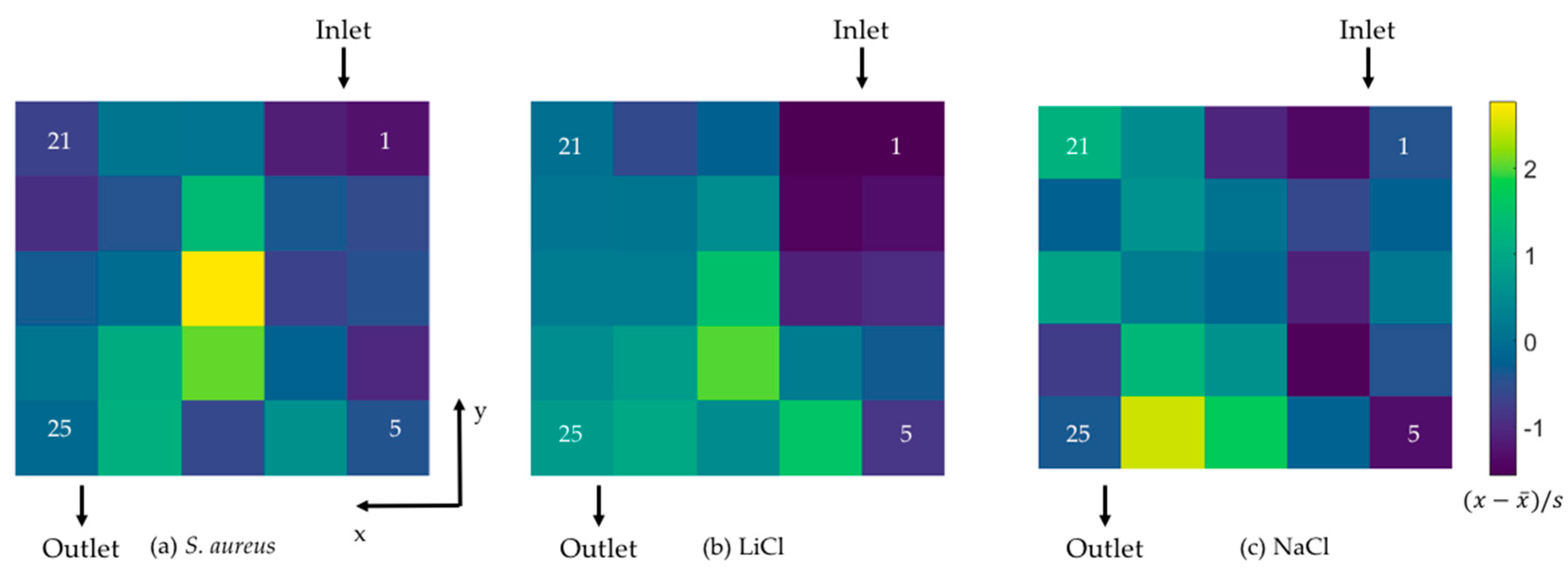
4.3. Single Patient Room Experiment
5. Discussion
5.1. Empty Room
5.2. Single-Bed Room
5.3. General Observations
5.4. Implications
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Graves, N. Economics and preventing hospital-acquired infection. Emerg. Infect. Dis. 2004, 10, 561–566. [Google Scholar] [CrossRef] [PubMed]
- McBryde, E.S.; Bradley, L.C.; Whitby, M.; McElwain, D.L.S. An investigation of contact transmission of methicillin-resistant Staphylococcus aureus. J. Hosp. Infect. 2004, 58, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.J.; Young, V.; Robertson, C.; Dancer, S.J. Where do hands go? An audit of sequential hand-touch events on a hospital ward. J. Hosp. Infect. 2012, 80, 206–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allegranzi, B.; Pittet, D. Role of hand hygiene in healthcare-associated infection prevention. J. Hosp. Infect. 2009, 73, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.W.; Li, Y.; Eames, I.; Chan, P.K.S.; Ridgway, G.L. Factors involved in the aerosol transmission of infection and control of ventilation in healthcare premises. J. Hosp. Infect. 2006, 64, 100–114. [Google Scholar] [CrossRef] [PubMed]
- Eames, I.; Shoaib, D.; Klettner, C.A.; Taban, V. Movement of airborne contaminants in a hospital isolation room. J. R. Soc. Interface 2009, 6, S757–S766. [Google Scholar] [CrossRef] [PubMed]
- Bacaër, N.; Ouifki, R.; Pretorius, C.; Wood, R.; Williams, B. Modeling the joint epidemics of TB and HIV in a South African township. J. Math. Biol. 2008, 57, 557–593. [Google Scholar] [CrossRef] [PubMed]
- Escombe, A.R.; Huaroto, L.; Ticona, E.; Burgos, M.; Sanchez, I.; Carrasco, L.; Farfán, E.; Flores, F.; Moore, D.A.J. Tuberculosis transmission risk and infection control in a hospital emergency department in Lima, Peru. Int. J. Tuberc. Lung Dis. 2010, 14, 1120–1126. [Google Scholar] [PubMed]
- Anderson, R.E.; Young, V.; Stewart, M.; Robertson, C.; Dancer, S.J. Cleanliness audit of clinical surfaces and equipment: Who cleans what? J. Hosp. Infect. 2011, 78, 178–181. [Google Scholar] [CrossRef] [PubMed]
- Dancer, S.J.; White, L.F.; Lamb, J.; Girvan, E.K.; Robertson, C. Measuring the effect of enhanced cleaning in a UK hospital: A prospective cross-over study. BMC Med. 2009, 7, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, A.S.; Dancer, S.J.; Humphreys, H. Priorities in the prevention and control of multidrug-resistant Enterobacteriaceae in hospitals. J. Hosp. Infect. 2012, 82, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Zarpellon, M.N.; Gales, A.C.; Sasaki, A.L.; Selhorst, G.J.; Menegucci, T.C.; Cardoso, C.L.; Garcia, L.B.; Tognim, M.C.B. Survival of vancomycin-intermediate Staphylococcus aureus on hospital surfaces. J. Hosp. Infect. 2015, 90, 347–350. [Google Scholar] [CrossRef] [PubMed]
- Boyce, J.M.; Havill, N.L.; Otter, J.A.; McDonald, L.C.; Adams, N.M.T.; Cooper, T.; Thompson, A.; Wiggs, L.; Killgore, G.; Tauman, A.; et al. Impact of hydrogen peroxide vapor room decontamination on Clostridium difficile environmental contamination and transmission in a healthcare setting. Infect. Control Hosp. Epidemiol. 2008, 29, 723–729. [Google Scholar] [CrossRef] [PubMed]
- Noakes, C.J.; Sleigh, P.A. Mathematical models for assessing the role of airflow on the risk of airborne infection in hospital wards. J. R. Soc. Interface 2009, 6, S791–S800. [Google Scholar] [CrossRef] [PubMed]
- Dancer, S.J. Mopping up hospital infection. J. Hosp. Infect. 1999, 43, 85–100. [Google Scholar] [CrossRef] [PubMed]
- Kiss, I.Z.; Green, D.M.; Kao, R.R. The effect of contact heterogeneity and multiple routes of transmission on final epidemic size. Math. Biosci. 2006, 203, 124–136. [Google Scholar] [CrossRef] [PubMed]
- Pittet, D.; Allegranzi, B.; Sax, H.; Dharan, S.; Pessoa-Silva, C.L.; Donaldson, L.; Boyce, J.M. Evidence-based model for hand transmission during patient care and the role of improved practices. Lancet Infect. Dis. 2006, 6, 641–652. [Google Scholar] [CrossRef]
- King, M.F.; Noakes, C.J.; Sleigh, P.A.; Bale, S.; Waters, L. Relationship between healthcare worker surface contacts, care type and hand hygiene: An observational study in a single-bed hospital ward. J. Hosp. Infect. 2016, 94, 48–51. [Google Scholar] [CrossRef] [PubMed]
- Ramos, T.; Dedesko, S.; Siegel, J.A.; Gilbert, J.A.; Stephens, B. Spatial and temporal variations in indoor environmental conditions, human occupancy, and operational characteristics in a new hospital building. PLoS ONE 2015, 10, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Beggs, C.B.; Noakes, C.J.; Sleigh, P.A.; Fletcher, L.A.; Siddiqi, K. The transmission of tuberculosis in confined spaces: An analytical review of alternative epidemiological models. Int. J. Tuberc. Lung Dis. 2003, 7, 1015–1026. [Google Scholar] [PubMed]
- Escombe, A.R.; Moore, D.A.J.; Gilman, R.H.; Navincopa, M.; Ticona, E.; Mitchell, B.; Noakes, C.; Martínez, C.; Sheen, P.; Ramirez, R.; et al. Upper-room ultraviolet light and negative air ionization to prevent tuberculosis transmission. PLoS Med. 2009, 6, e1000043. [Google Scholar] [CrossRef] [PubMed]
- Xie, X. Evaporation and Movement of Respiratory Droplets in Indoor Environments. Ph.D. Thesis, The University of Hong Kong, Hong Kong, China, 2008. [Google Scholar]
- Liu, L.; Wei, J.; Li, Y.; Ooi, A. Evaporation and dispersion of respiratory droplets from coughing. Indoor Air 2017, 27, 179–190. [Google Scholar] [CrossRef] [PubMed]
- Hathway, E.A.; Noakes, C.J.; Sleigh, P.A.; Fletcher, L.A. CFD simulation of airborne pathogen transport due to human activities. Build. Environ. 2011, 46, 2500–2511. [Google Scholar] [CrossRef]
- King, M.F.; Noakes, C.J.; Sleigh, P.A.; Camargo-Valero, M.A. Bioaerosol deposition in single and two-bed hospital rooms: A numerical and experimental study. Build. Environ. 2013, 59, 436–447. [Google Scholar] [CrossRef]
- Wong, L.T.; Chan, W.Y.; Mui, K.W.; Lai, A.C.K. An Experimental and Numerical Study on Deposition of Bioaerosols in a Scaled Chamber. Aerosol Sci. Technol. 2010, 44, 117–128. [Google Scholar] [CrossRef]
- Sinclair, R.G.; Rose, J.B.; Hashsham, S.A.; Gerba, C.P.; Haase, C.N. Criteria for selection of surrogates used to study the sate and control of pathogens in the environment. Appl. Environ. Microbiol. 2012, 78, 1969–1977. [Google Scholar] [CrossRef] [PubMed]
- Hunter, M.; Westgate, M.; Barton, P.; Calhoun, A.; Pierson, J.; Tulloch, A.; Beger, M.; Branquinho, C.; Caro, T.; Gross, J.; et al. Two roles for ecological surrogacy: Indicator surrogates and management surrogates. Ecol. Indic. 2016, 63, 121–125. [Google Scholar] [CrossRef]
- Mulvey, D.; Redding, P.; Robertson, C.; Woodall, C.; Kingsmore, P.; Bedwell, D.; Dancer, S.J. Finding a benchmark for monitoring hospital cleanliness. J. Hosp. Infect. 2011, 77, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Roberts, K.A. The Use of UV to Disinfect Airborne Pathogens. Ph.D. Thesis, University of Leeds, Leeds, UK, 2008. [Google Scholar]
- Bishop, A.H.; Stapleton, H.L. Aerosol and surface deposition characteristics of two surrogates for Bacillus anthracis spores. Appl. Environ. Microbiol. 2016, 82, 6682–6690. [Google Scholar] [CrossRef] [PubMed]
- Ramos, T.; Stephens, B. Tools to improve built environment data collection for indoor microbial ecology investigations. Build. Environ. 2014, 81, 243–257. [Google Scholar] [CrossRef]
- Jung, J.H.; Lee, J.E. Variation in the fluorescence intensity of thermally-exposed bacterial bioaerosols. J. Aerosol Sci. 2013, 65, 101–110. [Google Scholar] [CrossRef]
- Hathway, E.A.; Noakes, C.J.; Fletcher, L.A.; Sleigh, P.A.; Clifton, I.; Elliott, M.W. The Role of Nursing Activities on the Bioaerosol Production in Hospital Wards. Indoor Built Environ. 2013, 22, 410–421. [Google Scholar] [CrossRef]
- Lewis, T.; Griffith, C.; Gallo, M.; Weinbren, M. A modified ATP benchmark for evaluating the cleaning of some hospital environmental surfaces. J. Hosp. Infect. 2008, 69, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Sze To, G.N.; Wan, M.P.; Chao, C.Y.H.; Wei, F.; Yu, S.C.T.; Kwan, J.K.C. A methodology for estimating airborne virus exposures in indoor environments using the spatial distribution of expiratory aerosols and virus viability characteristics. Indoor Air 2008, 18, 425–438. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.L.; Lynch, R.A. An efficient analytical method for particle counting in evaluating airborne infectious isolation containment using fluorescent microspheres. J. Occup. Environ. Hyg. 2008, 5, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Rydock, J.P. A Simple Method for Tracer Containment Testing of Hospital Isolation Rooms. Appl. Occup. Environ. Hyg. 2002, 17, 486–490. [Google Scholar] [CrossRef] [PubMed]
- Cheong, K.W.D.; Phua, S.Y. Development of ventilation design strategy for effective removal of pollutant in the isolation room of a hospital. Build. Environ. 2006, 41, 1161–1170. [Google Scholar] [CrossRef]
- Tang, J.W.; Noakes, C.J.; Nielsen, P.V.; Eames, I.; Nicolle, A.; Li, Y.; Settles, G.S. Observing and quantifying airflows in the infection control of aerosol- and airborne-transmitted diseases: An overview of approaches. J. Hosp. Infect. 2011, 77, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Qian, H.; Li, Y.; Nielsen, P.V.; Huang, X. Spatial distribution of infection risk of SARS transmission in a hospital ward. Build. Environ. 2009, 44, 1651–1658. [Google Scholar] [CrossRef]
- Fabian, P.; McDevitt, J.J.; DeHaan, W.H.; Fung, R.O.P.; Cowling, B.J.; Chan, K.H.; Leung, G.M.; Milton, D.K. Influenza virus in human exhaled breath: An observational study. PLoS ONE 2008, 3, e2691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olmedo, I.; Nielsen, P.V.; Ruiz de Adana, M.; Jensen, R.L.; Grzelecki, P. Distribution of exhaled contaminants and personal exposure in a room using three different air distribution strategies. Indoor Air 2012, 22, 64–76. [Google Scholar] [CrossRef] [PubMed]
- Bjørn, E.; Nielsen, P.V. Dispersal of exhaled air and personal exposure in displacement ventilated rooms. Indoor Air 2002, 12, 147–164. [Google Scholar] [CrossRef] [PubMed]
- Gilkeson, C.A.; Camargo-Valero, M.A.; Pickin, L.E.; Noakes, C.J. Measurement of ventilation and airborne infection risk in large naturally ventilated hospital wards. Build. Environ. 2013, 65, 35–48. [Google Scholar] [CrossRef]
- Sze To, G.N.; Chao, C.Y.H. Review and comparison between the Wells-Riley and dose-response approaches to risk assessment of infectious respiratory diseases. Indoor Air 2010, 20, 2–16. [Google Scholar] [CrossRef] [PubMed]
- Zoon, W.A.C.; Loomans, M.G.L.C.; Hensen, J.L.M. Testing the effectiveness of operating room ventilation with regard to removal of airborne bacteria. Build. Environ. 2011, 46, 2570–2577. [Google Scholar] [CrossRef]
- Zhu, S.; Kato, S.; Yang, J.H. Study on transport characteristics of saliva droplets produced by coughing in a calm indoor environment. Build. Environ. 2006, 41, 1691–1702. [Google Scholar] [CrossRef]
- Best, E.L.; Parnell, P.; Wilcox, M.H. Microbiological comparison of hand-drying methods: The potential for contamination of the environment, user, and bystander. J. Hosp. Infect. 2014, 88, 199–206. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, A.; Sextro, R.G.; Byrne, M.A. Mass transport of deposited particles by surface-to-surface contact. J. Hazard. Mater. 2012, 227, 370–377. [Google Scholar] [CrossRef] [PubMed]
- Aliasgharpour, M.; Hagani, H. Evaluation of lithium determination in three analyzers: Flame emission, flame atomic absorption spectroscopy and ion selective electrode. N. Am. J. Med. Sci. 2009, 1, 244–246. [Google Scholar] [PubMed]
- Julian, T.R.; Canales, R.A.; Leckie, J.O.; Boehm, A.B. A model of exposure to rotavirus from nondietary ingestion iterated by simulated intermittent contacts. Risk Anal. 2009, 29, 617–632. [Google Scholar] [CrossRef] [PubMed]
- Sickbert-Bennett, E.E.; Weber, D.J.; Gergen-Teague, M.F.; Sobsey, M.D.; Samsa, G.P.; Rutala, W.A. Comparative efficacy of hand hygiene agents in the reduction of bacteria and viruses. Am. J. Infect. Control 2005, 33, 67–77. [Google Scholar] [CrossRef] [PubMed]
- Tung-Thompson, G.; Libera, D.A.; Koch, K.L.; De Los Reyes, F.L.; Jaykus, L.A. Aerosolization of a human norovirus surrogate, bacteriophage MS2, during simulated vomiting. PLoS ONE 2015, 10, e0134277. [Google Scholar] [CrossRef] [PubMed]
- Seo, E.Y.; Ahn, T.S.; Zo, Y.G. Agreement, precision, and accuracy of epifluorescence microscopy methods for enumeration of total bacterial numbers. Appl. Environ. Microbiol. 2010, 76, 1981–1991. [Google Scholar] [CrossRef] [PubMed]
- Sattar, S.A.; Springthorpe, S.; Mani, S.; Gallant, M.; Nair, R.C.; Scott, E.; Kain, J. Transfer of bacteria from fabrics to hands and other fabrics: Development and application of a quantitative method using Staphylococcus aureus as a model. J. Appl. Microbiol. 2001, 90, 962–970. [Google Scholar] [CrossRef] [PubMed]
- Qian, H.; Li, Y.; Nielsen, P.V.; Hyldgaard, C.E. Dispersion of exhalation pollutants in a two-bed hospital ward with a downward ventilation system. Build. Environ. 2008, 43, 344–354. [Google Scholar] [CrossRef]
- Gilkeson, C.A.; Noakes, C.J.; Sleigh, P.A.; Khan, M.A.I. Simulating Pathogen Transport within a Naturally Ventilated Hospital Ward. In Proceedings of the International Conference on Computational Fluid Dynamics, Paris, France, 27–29 September 2011. [Google Scholar]
- Tang, J.W.; Liebner, T.J.; Craven, B.A.; Settles, G.S. A schlieren optical study of the human cough with and without wearing masks for aerosol infection control. J. R. Soc. Interface 2009, 6, S727–S736. [Google Scholar] [CrossRef] [PubMed]
- Heating and Ventilation of Health Sector Buildings (HTM 03-01); Department of Health: London, UK, 2007.
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Int. J. Nurs. Stud. 2010, 47, 931–936. [Google Scholar] [CrossRef]
- Dancer, S.J.; Anderson, R.; Young, V.; Stewart, M. P11.05 Cleanliness audit of clinical surfaces and equipment: Who cleans what? J. Hosp. Infect. 2010, 76, S34. [Google Scholar] [CrossRef]
- Rountree, P.M. The Effect of Desiccation on the Viability of Staphylococcus Aureus. J. Hyg. 1963, 61, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Beauchêne, C.; Laudinet, N.; Choukri, F.; Rousset, J.L.; Benhamadouche, S.; Larbre, J.; Chaouat, M.; Benbunan, M.; Mimoun, M.; Lajonchère, J.P.; et al. Accumulation and transport of microbial-size particles in a pressure protected model burn unit: CFD simulations and experimental evidence. BMC Infect. Dis. 2011, 11, 58. [Google Scholar] [CrossRef] [PubMed]
- Noakes, C.J.; Fletcher, L.A.; Sleigh, P.A.; Booth, W.B.; Beato-Arribas, B.; Tomlinson, N. Comparison of tracer techniques for evaluating the behaviour of bioaerosols in hospital isolation rooms. In Proceedings of the Healthy Buildings, Kuala Lumpur, Malaysia, 13–17 September 2009. [Google Scholar]
- Dancer, S.J.; Crawford, A. Keeping hospital MRSA out of a district general. J. Hosp. Infect. 1999, 43, 19–27. [Google Scholar] [CrossRef]
- Otter, J.A.; Yezli, S.; French, G.L. The role played by contaminated surfaces in the transmission of nosocomial pathogens. Infect. Control Hosp. Epidemiol. 2011, 32, 687–699. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Surrogate Name | Used for | Advantages | Disadvantages | Reference |
|---|---|---|---|---|
| Staphylococcus aureus | MRSA (Methicillin Resistant Staphylococcus aureus) | Non-pathogenic to healthy individuals and morphologically identical to MRSA. Readily grows on standard nutrient agar. | Requires culturing period and counting colonies by hand or machine. Cannot be used in-vivo locations | [24,25] |
| Bacillus thuringiensis subsp. kurstaki | Bacillus anthracis | Non-pathogenic and morphologically representative of microorganism | Cannot be used in in-vivo locations | [31] |
| MS2 phage | Viruses, e.g., rotavirus | Representative of typical larger viruses | Requires specialist microbiological and microscopy skills. Cannot be used in in-vivo locations. | [52,53,54] |
| Oil droplets | (Bio)aerosols | Specific size droplets can be produced. | Hard to clean surfaces | [47] |
| Fluorescent latex spheres | (Bio)aerosols | Quantitative airborne and surface counts. Consistent size. | Cannot retrieve spheres, latex is an allergen. | [55] |
| Fluorescein | General purpose tracer | Highly soluble. Quantitative airborne and surface contamination. Fluorescence easy to detect | Quantitative correlation to microorganisms unknown. Requires expert preparation and can cause anaphylaxis in up to 6% of exposed. Hard to clean. | [50] |
| Fluorescent bacterial staining | Airborne and surface contamination | Gives total bacterial count. | Requires specialist microbiological and microscopy skills. Does not give total viable count. | [37,56] |
| Smoke sticks | Airflow movement | Easy to use, leaves no trace | Qualitative results only. Use of laser light to track particles requires sealed opaque room. | [24,57] |
| CO2/NO2 | Airborne contaminant transport | CO2 canisters are abundant and sensors are cheap and accurate | Exists in background concentrations so needs high levels. Asphixiant so cannot be used in situ. | [45,58] |
| Ink/food colorant/Rhodamine | Surface contamination | Cheap and visual | Qualitative results | [23,49] |
| Schlieren photography | Airflow movement | Safe for human participants | Small field of view and qualitative results. | [40,59] |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
King, M.-F.; Camargo-Valero, M.A.; Matamoros-Veloza, A.; Sleigh, P.A.; Noakes, C.J. An Effective Surrogate Tracer Technique for S. aureus Bioaerosols in a Mechanically Ventilated Hospital Room Replica Using Dilute Aqueous Lithium Chloride. Atmosphere 2017, 8, 238. https://doi.org/10.3390/atmos8120238
King M-F, Camargo-Valero MA, Matamoros-Veloza A, Sleigh PA, Noakes CJ. An Effective Surrogate Tracer Technique for S. aureus Bioaerosols in a Mechanically Ventilated Hospital Room Replica Using Dilute Aqueous Lithium Chloride. Atmosphere. 2017; 8(12):238. https://doi.org/10.3390/atmos8120238
Chicago/Turabian StyleKing, Marco-Felipe, Miller Alonso Camargo-Valero, Adriana Matamoros-Veloza, P. Andrew Sleigh, and Catherine J. Noakes. 2017. "An Effective Surrogate Tracer Technique for S. aureus Bioaerosols in a Mechanically Ventilated Hospital Room Replica Using Dilute Aqueous Lithium Chloride" Atmosphere 8, no. 12: 238. https://doi.org/10.3390/atmos8120238
APA StyleKing, M.-F., Camargo-Valero, M. A., Matamoros-Veloza, A., Sleigh, P. A., & Noakes, C. J. (2017). An Effective Surrogate Tracer Technique for S. aureus Bioaerosols in a Mechanically Ventilated Hospital Room Replica Using Dilute Aqueous Lithium Chloride. Atmosphere, 8(12), 238. https://doi.org/10.3390/atmos8120238