Factors Affecting Consumption of Water from a Newly Introduced Safe Drinking Water System: The Case of Managed Aquifer Recharge (MAR) Systems in Bangladesh


 ,
,  and
and
Abstract
:1. Introduction
2. Explaining Variation in the Use of New Drinking Water Systems
3. Materials and Methods
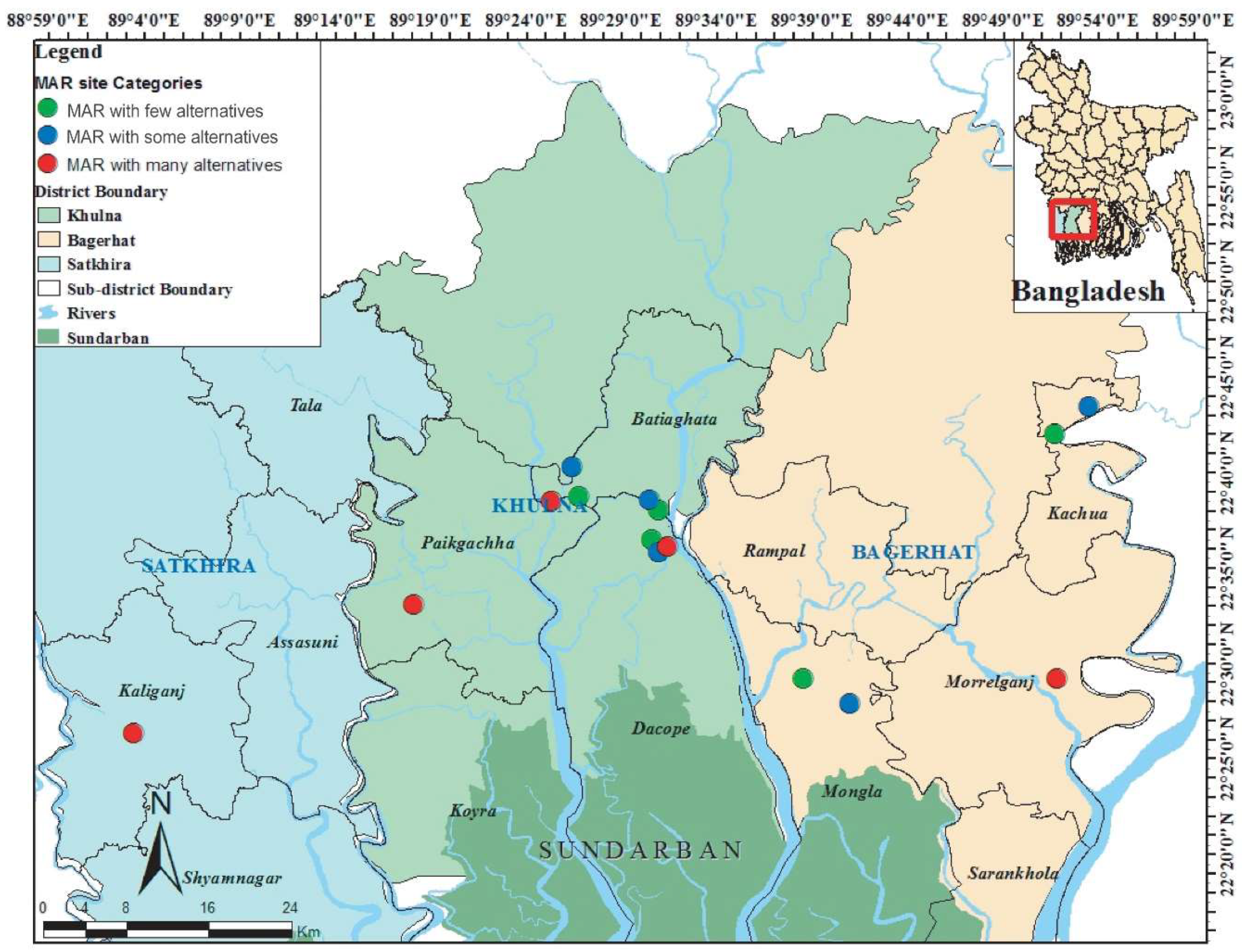
3.1. Sample Selection
3.2. Operationalization
3.3. Data Collection
3.4. Data Analysis
4. Results
5. Discussion and Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Moretto, L.; Faldi, G.; Ranzato, M.; Rosati, F.N.; Ilito Boozi, J.P.; Teller, J. Challenges of water and sanitation service co-production in the global South. Environ. Urban. 2018, 30, 425–443. [Google Scholar] [CrossRef]
- Peters, C.N.; Baroud, H.; Hornberger, G.M. Multicriteria decision analysis of drinking water source selection in southwestern Bangladesh. J. Water Resour. Plan. Manag. 2019, 145, 05019004. [Google Scholar] [CrossRef]
- Van Houtven, G.L.; Pattanayak, S.K.; Usmani, F.; Yang, J.C. What are households willing to pay for improved water access? Results from a meta-analysis. Ecol. Econ. 2017, 136, 126–135. [Google Scholar] [CrossRef]
- WHO/UNICEF, JMP. 2017 Annual Report WHO/UNICEF Joint Monitoring Programme for Water Supply, Sanitation and Hygiene (JMP). Available online: https://washdata.org/sites/default/files/documents/reports/2018-07/JMP-2017-annual-report.pdf (accessed on 22 November 2019).
- Veldkamp, T.I.E.; Wada, Y.; de Moel, H.; Kummu, M.; Eisner, S.; Aerts, J.C.J.H.; Ward, P.J. Changing mechanism of global water scarcity events: Impacts of socioeconomic changes and inter-annual hydro-climatic variability. Glob. Environ. Chang. 2015, 32, 18–29. [Google Scholar] [CrossRef]
- Prüss-Üstün, A.; Bos, R.; Gore, F.; Bartram, J. Safer Water. Better Health: Costs, Benefits and Sustainability of Interventions to Protect and Promote Health; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Kiguchi, M.; Shen, Y.; Kanae, S.; Oki, T. Re-evaluation of future water stress due to socio-economic and climate factors under a warming climate. Hydrol. Sci. J. 2014, 60, 14–29. [Google Scholar] [CrossRef]
- Schewe, J.; Heinke, J.; Gerten, D.; Haddeland, I.; Arnell, N.W.; Clark, D.B.; Dankers, R.; Eisner, S.; Fekete, B.M.; Colón-González, F.J.; et al. Multimodel assessment of water scarcity under climate change. Proc. Natl. Acad. Sci. USA 2014, 111, 3245–3250. [Google Scholar] [CrossRef]
- Murshed, S.B.; Kaluarachchi, J.J. Scarcity of fresh water resources in the Ganges Delta of Bangladesh. Water Secur. 2018, 4–5, 8–18. [Google Scholar] [CrossRef]
- WHO/UNICEF. WHO/UNICEF Joint Monitoring Programme (JMP) for Water Supply and Sanitation, Bangladesh; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Piechulek, H.; Al-Sabbir, A.; Mendoza-Aldana, J. Diarrhea and ARI in rural areas of Bangladesh. Southeast. Asian J. Trop. Med. Public Health 2003, 34, 337–342. [Google Scholar]
- Afroz, S.; Cramb, R.; Grunbuhel, C. Collective management of water resources in coastal Bangladesh: Formal and substantive approaches. Hum. Ecol. 2016, 44, 17–31. [Google Scholar] [CrossRef]
- Hoque, B.A.; Hoque, M.M.; Ahmed, T.; Islam, S.; Azad, A.K.; Ali, N.; Hossain, M.; Hossain, M.S. Demand-based water options for arsenic mitigation: An experience from rural Bangladesh. Public Health 2004, 118, 70–77. [Google Scholar] [CrossRef]
- Shafiquzzaman, M.; Azam, M.S.; Moshima, I.; Nakajima, J. Technical and social evaluation of arsenic mitigation in rural bangladesh. J. Health Popul. Nutr. 2009, 27, 674–683. [Google Scholar] [CrossRef] [PubMed]
- Hossain, M.; Rahman, S.N.; Bhattacharya, P.; Jacks, G.; Saha, R.; Rahman, M. Sustainability of arsenic mitigation interventions: An evaluation of different alternative safe drinking water options provided in Matlab, an arsenic hot spot in Bangladesh. Front. Environ. Sci. 2015, 3, 1–15. [Google Scholar] [CrossRef]
- Obergfell, C.; Bakker, M.; Maas, K. Estimation of average diffuse aquifer recharge using time series modeling of groundwater heads. Water Resour. Res. 2019, 55, 2194–2210. [Google Scholar] [CrossRef]
- Antoniou, E.A.; Stuyfzand, P.J.; van Breukelen, B.M. Reactive transport modeling of an aquifer storage and recovery (ASR) pilot to assess long-term water quality improvements and potential solutions. Appl. Geochem. 2013, 35, 173–186. [Google Scholar] [CrossRef]
- Fielding, K.S.; Gardner, J.; Leviston, Z.; Price, J. Comparing public perceptions of alternative water sources for potable use: The case of rainwater, stormwater, desalinated water, and recycled water. Water Resour. Manag. 2015, 29, 4501–4518. [Google Scholar] [CrossRef]
- Leviston, Z.; Nancarrow, B.E.; Tucker, D.I.; Porter, N.B. Predicting Community Behaviour: Indirect Potable Reuse of Wastewater Through Managed Aquifer Recharge; Land and Water Science Report 2906; CSIRO: Canberra, Australia, 2006. [Google Scholar]
- Wu, Z.; McKay, J.; Keremane, G. Issues affecting community attitudes and intended behaviours in stormwater reuse: A case study of Salisbury, South Australia. Water 2012, 4, 835–847. [Google Scholar] [CrossRef]
- Mosler, H.J. A systematic approach to behavior change interventions for the water and sanitation sector in developing countries: A conceptual model, a review, and a guideline. Int. J. Environ. Health Res. 2012, 22, 431–449. [Google Scholar] [CrossRef]
- Inauen, J.; Hossain, M.M.; Johnston, R.B.; Mosler, H.J. Acceptance and use of eight arsenic-safe drinking water options in Bangladesh. PLoS ONE 2013, 8. [Google Scholar] [CrossRef]
- Kundu, D.K.; Gupta, A.; Mol, A.P.J.; Nasreen, M. Understanding social acceptability of arsenic-safe technologies in rural Bangladesh: A user-oriented analysis. Water Policy 2016, 18, 318–334. [Google Scholar] [CrossRef]
- Peal, A.J.; Evans, B.E.; van der Voorden, C. Hygiene and Sanitation Software: An Overview of Approaches; Water Supply and Sanitation Collaborative Council: Geneva, Switzerland, 2010. [Google Scholar]
- Komives, K.; Akanbang, B.; Thorsten, R.; Tuffuor, B.; Wakeman, W.; Larbi, E.; Bakalian, A.; Whittington, D. Post-construction support and the sustainability of rural water projects in Ghana. In Proceedings of the 33rd WEDC International Conference, Accra, Ghana, 7–11 April 2008; pp. 1–294. [Google Scholar]
- Floyd, D.L.; Prentice-Dunn, S.; Rogers, R.W. A meta-analysis of research on protection motivation theory. J. Appl. Soc. Psychol. 2000, 30, 407–429. [Google Scholar] [CrossRef]
- Schwarzer, R. Modeling health behavior change: How to predict and modify the adoption and maintenance of health behaviors. Appl. Psychol. 2008, 57, 1–29. [Google Scholar] [CrossRef]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Ajzen, I.; Driver, B.L. Application of the theory of planned behavior to leisure choice. J. Leis. Res. 1992, 24, 207–224. [Google Scholar] [CrossRef]
- Whittington, D.; Davis, J.; Prokopy, L.; Komives, K.; Thorsten, R.; Lukacs, H.; Bakalian, A.; Wakeman, W. How well is the demand-driven, community management model for rural water supply systems doing? Evidence from Bolivia, Peru and Ghana. Water Policy 2009, 11, 696–718. [Google Scholar] [CrossRef]
- Islam, M.; Ali Akber, M.; Atikul Islam, M. Willingness to pay for improved drinking water in Southwest coastal Bangladesh. Water Sci. Technol. Water Supply 2019, 19, 1–10. [Google Scholar] [CrossRef]
- Mahmuduzzaman, M.; Ahmed, Z.U.; Nuruzzaman, A.K.M.; Ahmed, F.R.S. Causes of salinity intrusion in coastal belt of Bangladesh. Int. J. Plant Res. 2014, 4, 8–13. [Google Scholar] [CrossRef]
- Hoque, M.R. Access to Safe Drinking Water in Rural Bangladesh: Water Governance by DPHE; BRAC University: Dhaka, Bangladesh, 2009. [Google Scholar]
- Hoffmeyer-Zlotnik, J.H.P. New sampling designs and the quality of data. Dev. Appl. Stat. 2003, 19, 205–217. Available online: http://mrvar.fdv.uni-lj.si/pub/mz/mz19/abst/hoff.htm (accessed on 22 November 2019).
- Bartram, D. Increasing validity with forced-choice criterion measurement formats. Int. J. Sel. Assess. 2007, 15, 263–272. [Google Scholar] [CrossRef]
- Huber, A.C.; Mosler, H.J. Determining behavioral factors for interventions to increase safe water consumption: A cross-sectional field study in rural Ethiopia. Int. J. Environ. Health Res. 2013, 23, 96–107. [Google Scholar] [CrossRef]
- Heri, S.; Mosler, H.J. Factors affecting the diffusion of solar water disinfection: A field study in Bolivia. Health Educ. Behav. 2008, 35, 541–560. [Google Scholar] [CrossRef]
- George, C.M.; Inauen, J.; Perin, J.; Tighe, J.; Hasan, K.; Zheng, Y. Behavioral determinants of switching to arsenic-safe water wells: An Analysis of a randomized controlled trial of health education interventions coupled with water arsenic testing. Health Educ. Behav. 2017, 44, 92–102. [Google Scholar] [CrossRef] [PubMed]
- Mosler, H.J.; Blöchliger, O.R.; Inauen, J. Personal, social, and situational factors influencing the consumption of drinking water from arsenic-safe deep tubewells in Bangladesh. J. Environ. Manag. 2010, 91, 1316–1323. [Google Scholar] [CrossRef] [PubMed]
- Inauen, J.; Mosler, H.J. Developing and testing theory-based and evidence-based interventions to promote switching to arsenic-safe wells in Bangladesh. J. Health Psychol. 2014, 19, 1483–1498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anthonj, C.; Fleming, L.; Cronk, R.; Godfrey, S.; Ambelu, A.; Bevan, J.; Sozzi, E.; Bartram, J. Improving monitoring and water point functionality in rural Ethiopia. Water 2018, 10, 1591. [Google Scholar] [CrossRef] [Green Version]
- Jiménez, A.; LeDeunff, H.; Giné, R.; Sjödin, J.; Cronk, R.; Murad, S.; Takane, M.; Bartram, J. The enabling environment for participation in water and sanitation: A conceptual framework. Water 2019, 11, 308. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Sub-Samples | Community Name | Sub-Sistrict | District | MAR Sites (#) | Respondents (Survey) | Interviewees (Experts) | Households (per Community) * | Average Income ($/Month) ** | Average Education (years) ** | Average Household Size ** | Travel Time to Nearest Urban Center (min) *** |
|---|---|---|---|---|---|---|---|---|---|---|---|
| MAR with a few alternatives (1–2 options) | Barunpara | Batiaghata | Khulna | 1 | 35 | 2 | 486 | 144 | 7 | 4.23 | 40 |
| Bhogobotipur | Batiaghata | Khulna | 1 | 57 | 2 | 276 | 131 | 6 | 4.40 | 45 | |
| Chalna | Dacope | Khulna | 1 | 55 | 2 | 326 | 176 | 9 | 4.98 | 20 | |
| South Chadpai | Mongla | Bagerhat | 1 | 62 | 2 | 426 | 141 | 6 | 4.82 | 30 | |
| Boyer singa guccho gram | Kochua | Bagerhat | 1 | 49 | 2 | 72 | 129 | 4 | 4.94 | 40 | |
| MAR with some alternatives (3 options) | Kayemkhula | Botiaghata | Khulna | 1 | 57 | 2 | 170 | 138 | 6 | 4.42 | 45 |
| Kollansree | Botiaghata | Khulna | 1 | 55 | 2 | 360 | 136 | 4 | 4.84 | 60 | |
| Duariara | Mongla | Bagerhat | 1 | 56 | 2 | 152 | 190 | 8 | 4.54 | 50 | |
| Achbua | Dacop | Khulna | 1 | 51 | 2 | 667 | 206 | 9 | 4.45 | 60 | |
| Gazalia | Kachua | Bagerhat | 1 | 48 | 2 | 365 | 158 | 6 | 4.81 | 40 | |
| MAR with many alternatives (>3 options) | Laxmikhula | Paikgacha | Khulna | 1 | 48 | 2 | 220 | 142 | 7 | 5.21 | 60 |
| Kalikabari | Morrelgonj | Bagerhat | 1 | 49 | 2 | 407 | 144 | 7 | 4.69 | 30 | |
| Chalna bazar | Dacop | Khulna | 1 | 48 | 2 | 278 | 120 | 6 | 4.46 | 15 | |
| Bigordana | Paikgacha | Khulna | 1 | 53 | 2 | 203 | 156 | 7 | 4.17 | 45 | |
| Thekra Rahimpur | Kaligonj | Satkhira | 1 | 57 | 2 | 421 | 151 | 7 | 4.72 | 40 | |
| Total | 15 | 7 | 3 | 15 | 780 | 30 | 4829 |
| Dependent Variable | Definition | Assessment | Response Options |
|---|---|---|---|
| Consumption of MAR water (in percentage) | The percentage of total drinking water used during the dry season that comes from MAR | How many pitchers of water from the following water sources do you collect for drinking purposes on a typical day during the peak of the dry season (i.e., April)? | Open (all possible sources—including MAR—are presented to the respondent) |
| Risk | |||
| Perceived vulnerability | A person’s subjective perception of his/her risk of contracting a disease | What do you think is the chance that you will get sick from using MAR water? | Four-point scale from high risk (4) to no risk at all (1). |
| Perceived severity | person’s perception of the seriousness of the consequences of contracting a disease | Imagine you contracted a disease (e.g., like arsenicosis, cholera or diarrhea) from your drinking water source, how severe would the impact be on your daily life? | Four-point scale from very severe (4) to not severe at all (1) |
| Factual knowledge | An understanding of how a person could become affected by a disease transmitted by drinking water | Factual knowledge about (i) actual contamination levels of MAR water, (ii) the actual medical conditions that may occur from drinking MAR water, and (iii) the treatment of MAR water. | Four-point scale from no knowledge (1) to maximum knowledge (4) |
| Attitude | |||
| Instrumental beliefs | Opinion about the distance of the MAR site | How far is the MAR site located from your house? | Four-point scale from very far (4) to not far at all (1) |
| Opinion about the costs of MAR | How expensive do you think it is for you to contribute to the operation and maintenance of MAR? | Four-point scale from very expensive (1) to very cheap (4) | |
| Opinion about the accessibility of the MAR site | How accessible do you think the MAR system is? | Four-point scale from not accessible (1) to very accessible (4) | |
| Affective beliefs | Opinion about the taste of MAR water | Do you like the taste of the water from the MAR system? | Five-point from “I dislike it very much” (1) to “I like it very much” (5) |
| Opinion about the smell of MAR water | Do you like the smell of the water from the MAR system? | Five-point from “I dislike it very much” (1) to “I like it very much” (5) | |
| Opinion about the color of MAR water | Do you like the color of the water from the MAR system? | Five-point from “I dislike it very much” (1) to “I like it very much” (5) | |
| Norms | |||
| Descriptive norm | Perceptions of which behaviors are typically performed | How many people in this neighborhood outside your family collect water from the MAR system? | Four-point scale from almost nobody (1) to almost everybody (4) |
| Injunctive norm | Perceptions of which behaviors are typically approved or disapproved of by important others | Do people that are important to you rather approve or disapprove of using water from the MAR system? | Four-point scale from strongly disapprove (1) to strongly approve (4) |
| Ability | |||
| Self-efficacy | The belief in one’s capabilities to organize and execute the course of actions required to manage prospective situations | How certain are you that you can collect as much safe water as you need from this source during the peak of the dry season from the MAR system? | Four-point scale from not at all certain (1) to completely certain (4) |
| Action knowledge | Knowing how to perform the behavior | How capable do you think the user committee responsible for MAR is? | Four-point scale from not capable at all (1) to very capable (4) |
| Self-regulation | |||
| Coping planning | How the person plans to cope with distractions and barriers | Do MAR users have a plan regarding what to do when the MAR system gets broken? | Four-point scale from no detailed plan (1) at all to very detailed plan (4) |
| Commitment | How committed the person is to the new behavior (i.e., using MAR water) | Do you feel committed to collect water from the MAR system? | Four-point scale from not at all committed (1) to completely committed (4) |
| Context | |||
| Alternative options | The level of competition that MAR faces in a community | How many drinking water options alternative to the MAR system do you have in your community? | Three-point scale from many alternatives (3) to few alternatives (1) |
| Factors | Sub-Factors | Descriptive Statistics | |||
|---|---|---|---|---|---|
| n | Range | M | SD | ||
| Risk | Perceived vulnerability | 636 | (1–4) | 2.70 | 1.09 |
| Perceived severity | 636 | (1–4) | 1.84 | 0.78 | |
| Factual knowledge | 636 | (1–4) | 2.40 | 0.68 | |
| Attitude | Perceived distance | 636 | (1–4) | 2.46 | 0.93 |
| Perceived cost | 636 | (1–4) | 2.41 | 0.98 | |
| Accessibility | 636 | (1–4) | 2.47 | 1.06 | |
| Perceived Taste | 636 | (1–5) | 3.48 | 1.37 | |
| Perceived Smell | 636 | (1–5) | 3.08 | 1.44 | |
| Color | 636 | (1–5) | 4.16 | 1.20 | |
| Norms | Descriptive norm | 636 | (1–4) | 2.15 | 0.98 |
| Injunctive norm | 636 | (1–4) | 2.32 | 1.07 | |
| Ability | Self-efficacy | 636 | (1–4) | 3.32 | 0.89 |
| Action knowledge | 636 | (1–4) | 2.77 | 0.96 | |
| Self-regulation | Coping planning | 636 | (1–4) | 2.22 | 0.86 |
| Commitment | 636 | (1–4) | 2.35 | 1.20 | |
| Context | Availability of alternative options | 636 | (1–3) | 2.14 | 0.81 |
| Total household water consumption | 780 | open | 23.27 | 8.56 | |
| % MAR water in total household water consumption | 636 | open | 29.39 | 40.72 | |
| Factors | Sub-Factors | Correlation | Regression Analysis | ||||
|---|---|---|---|---|---|---|---|
| R | B | SE B | β | t | p-Value | ||
| Risk | Perceived vulnerability | 0.422 | 4.016 | 1.237 | 0.108 | 3.246 | 0.001 *** |
| Perceived severity | 0.078 | 0.390 | 1.416 | −0.008 | −0.275 | 0.783 | |
| Factual knowledge | 0.253 | 7.239 | 1.682 | 0.122 | 4.304 | 0.000 *** | |
| Attitude | Perceived distance | 0.178 | 2.322 | 1.505 | 0.053 | 1.542 | 0.123 |
| Perceived cost | 0.154 | 2.029 | 1.187 | 0.049 | 1.709 | 0.088 * | |
| Accessibility | 0.250 | 1.453 | 1.329 | 0.038 | 1.094 | 0.274 | |
| Perceived Taste | 0.348 | 2.841 | 1.044 | 0.096 | 2.721 | 0.007 *** | |
| Perceived Smell | 0.250 | −1.027 | 0.937 | −0.036 | −1.096 | 0.273 | |
| Color | 0.145 | −0.848 | 1.002 | −0.025 | −0.846 | 0.398 | |
| Norms | Descriptive norm | 0.583 | 11.201 | 1.409 | 0.270 | 7.950 | 0.000 *** |
| Injunctive norm | 0.678 | 16.109 | 1.432 | 0.424 | 11.246 | 0.000 *** | |
| Ability | Self-efficacy | 0.294 | 2.251 | 1.350 | 0.049 | 1.667 | 0.096 * |
| Action knowledge | 0.182 | −2.714 | 1.238 | −0.064 | −2.193 | 0.029 ** | |
| Self-regulation | Coping planning | −0.089 | −3.057 | 1.545 | −0.065 | −1.979 | 0.048 ** |
| Commitment | 0.293 | 0.375 | 0.978 | 0.011 | 0.384 | 0.701 | |
| Context | Availability of alternative options | 0.236 | −2.937 | 1.670 | −0.058 | −1.759 | 0.079 * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hasan, M.B.; Driessen, P.P.J.; Majumder, S.; Zoomers, A.; van Laerhoven, F. Factors Affecting Consumption of Water from a Newly Introduced Safe Drinking Water System: The Case of Managed Aquifer Recharge (MAR) Systems in Bangladesh. Water 2019, 11, 2459. https://doi.org/10.3390/w11122459
Hasan MB, Driessen PPJ, Majumder S, Zoomers A, van Laerhoven F. Factors Affecting Consumption of Water from a Newly Introduced Safe Drinking Water System: The Case of Managed Aquifer Recharge (MAR) Systems in Bangladesh. Water. 2019; 11(12):2459. https://doi.org/10.3390/w11122459
Chicago/Turabian StyleHasan, Muhammad Badrul, Peter P. J. Driessen, Shantanu Majumder, Annelies Zoomers, and Frank van Laerhoven. 2019. "Factors Affecting Consumption of Water from a Newly Introduced Safe Drinking Water System: The Case of Managed Aquifer Recharge (MAR) Systems in Bangladesh" Water 11, no. 12: 2459. https://doi.org/10.3390/w11122459
APA StyleHasan, M. B., Driessen, P. P. J., Majumder, S., Zoomers, A., & van Laerhoven, F. (2019). Factors Affecting Consumption of Water from a Newly Introduced Safe Drinking Water System: The Case of Managed Aquifer Recharge (MAR) Systems in Bangladesh. Water, 11(12), 2459. https://doi.org/10.3390/w11122459