Origin, Fate and Control of Pharmaceuticals in the Urban Water Cycle: A Case Study



Abstract
1. Introduction
2. Materials and Methods
2.1. General Approach and Data Used in This Study
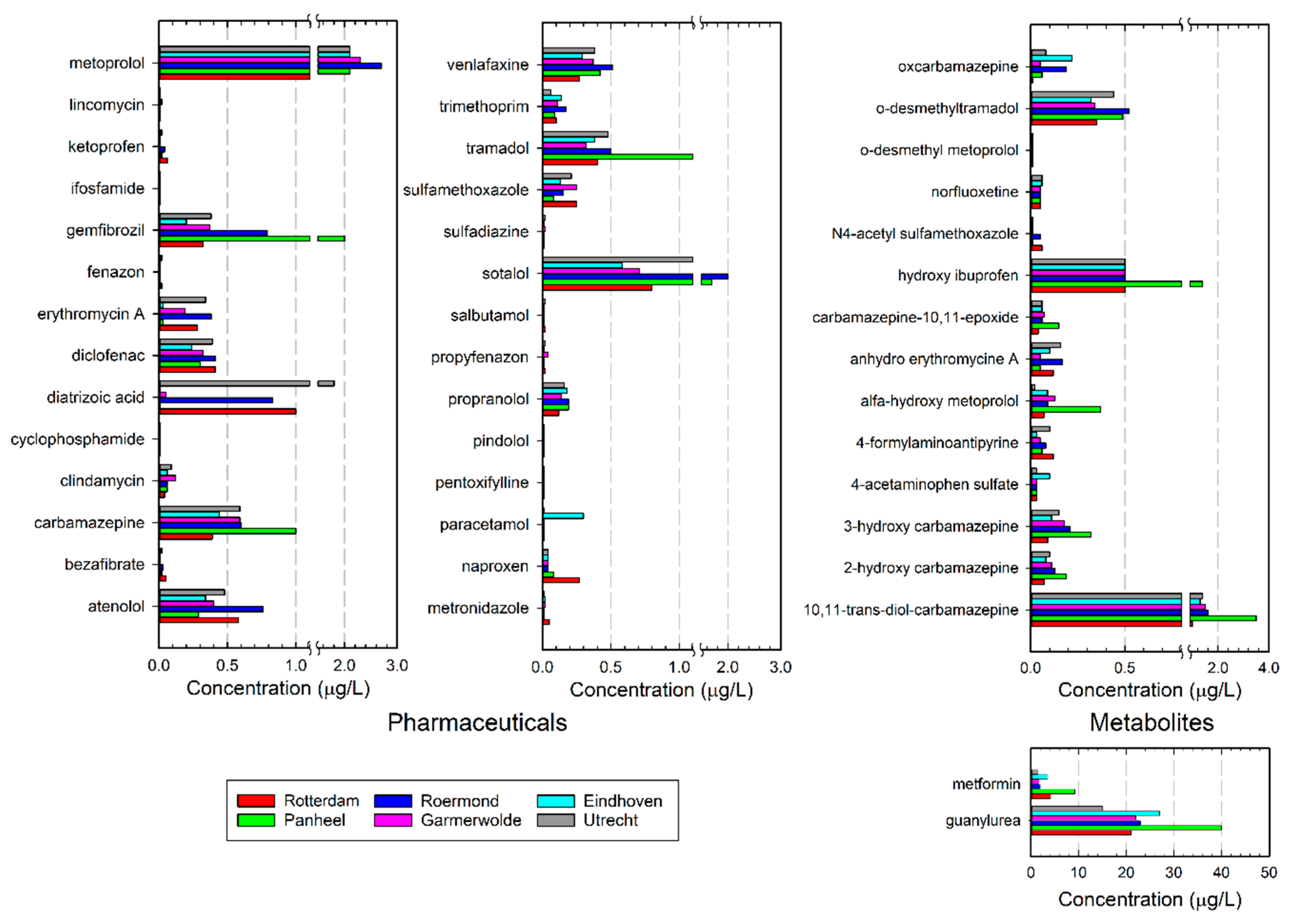
- Assessment of concentrations of pharmaceuticals and metabolites in several wastewater treatment effluents throughout The Netherlands to provide contextual or reference data for comparison with the effluents in the study area.
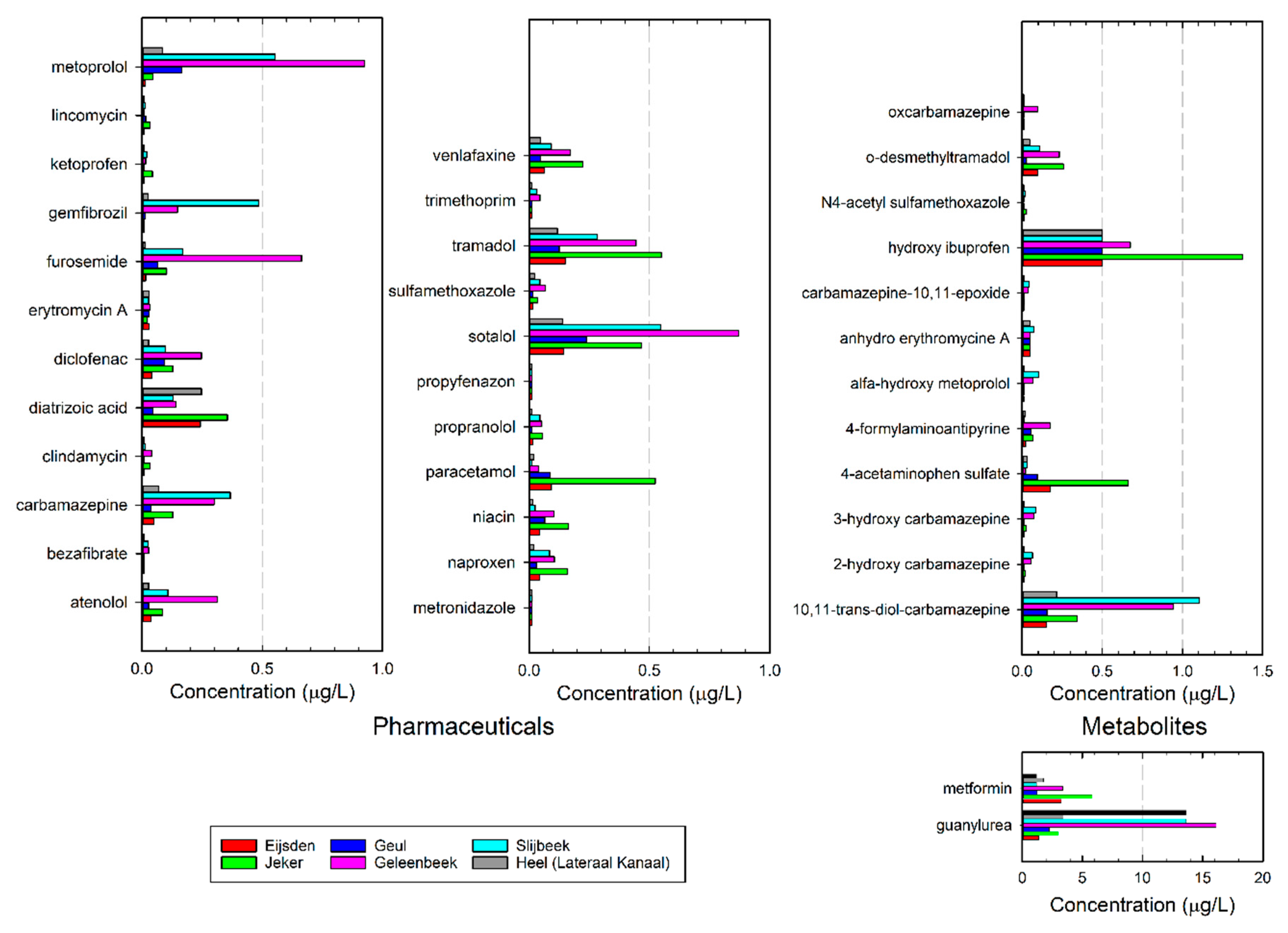
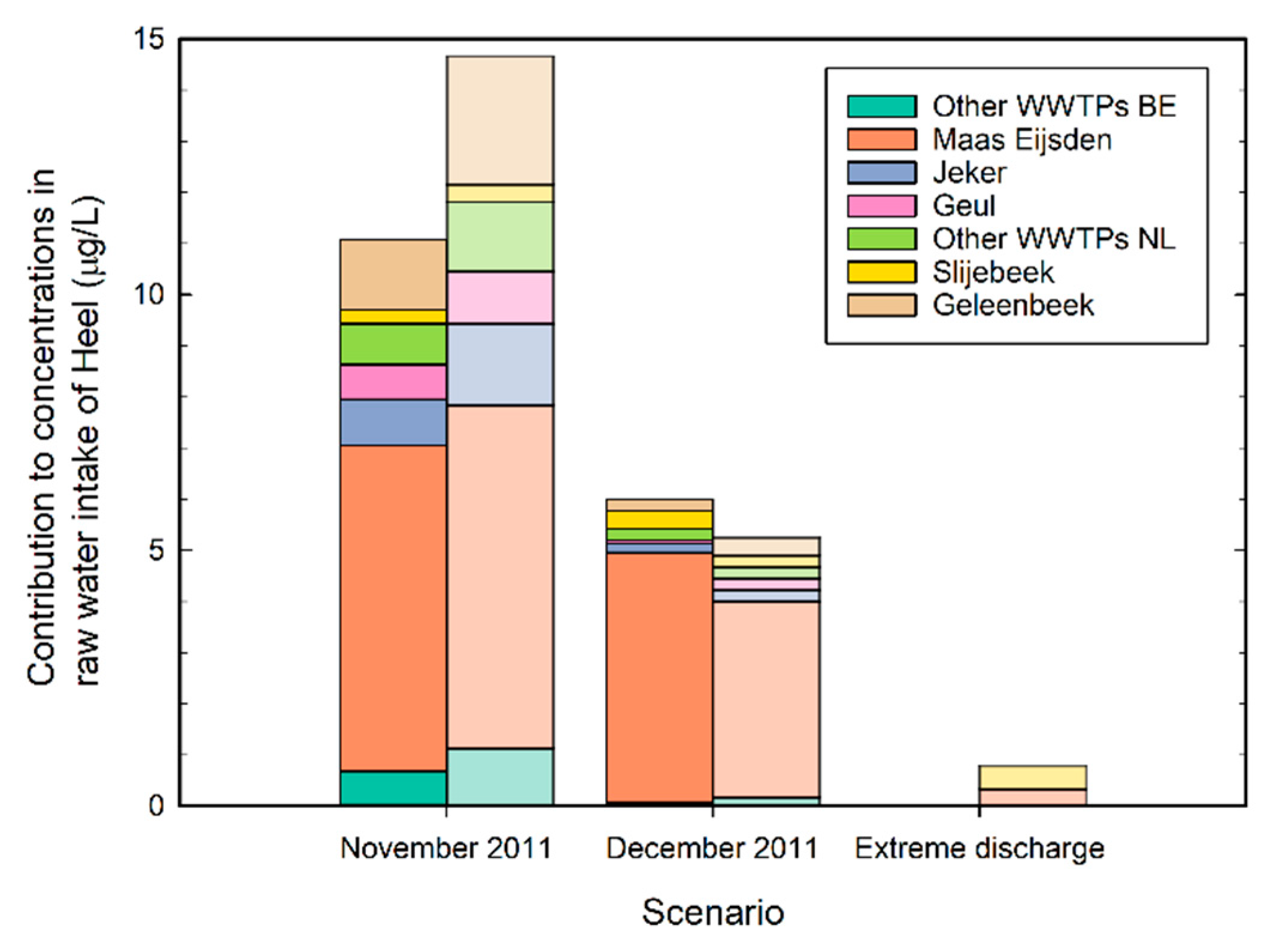
- Assessment of loads and concentrations of pharmaceuticals in the river Meuse and tributaries upstream of the drinking water intake of treatment plant Heel. This includes the apportionment of the contribution of pharmaceuticals of the different wastewater treatment plants in the study area to the drinking water intake.
- Evaluating different abatement options for pharmaceuticals and metabolites in the study area, including options for drinking water treatment and wastewater treatment. The focus is on the application of advanced oxidation processes.
- Finally, a vision for short term and longer-term solutions is presented.
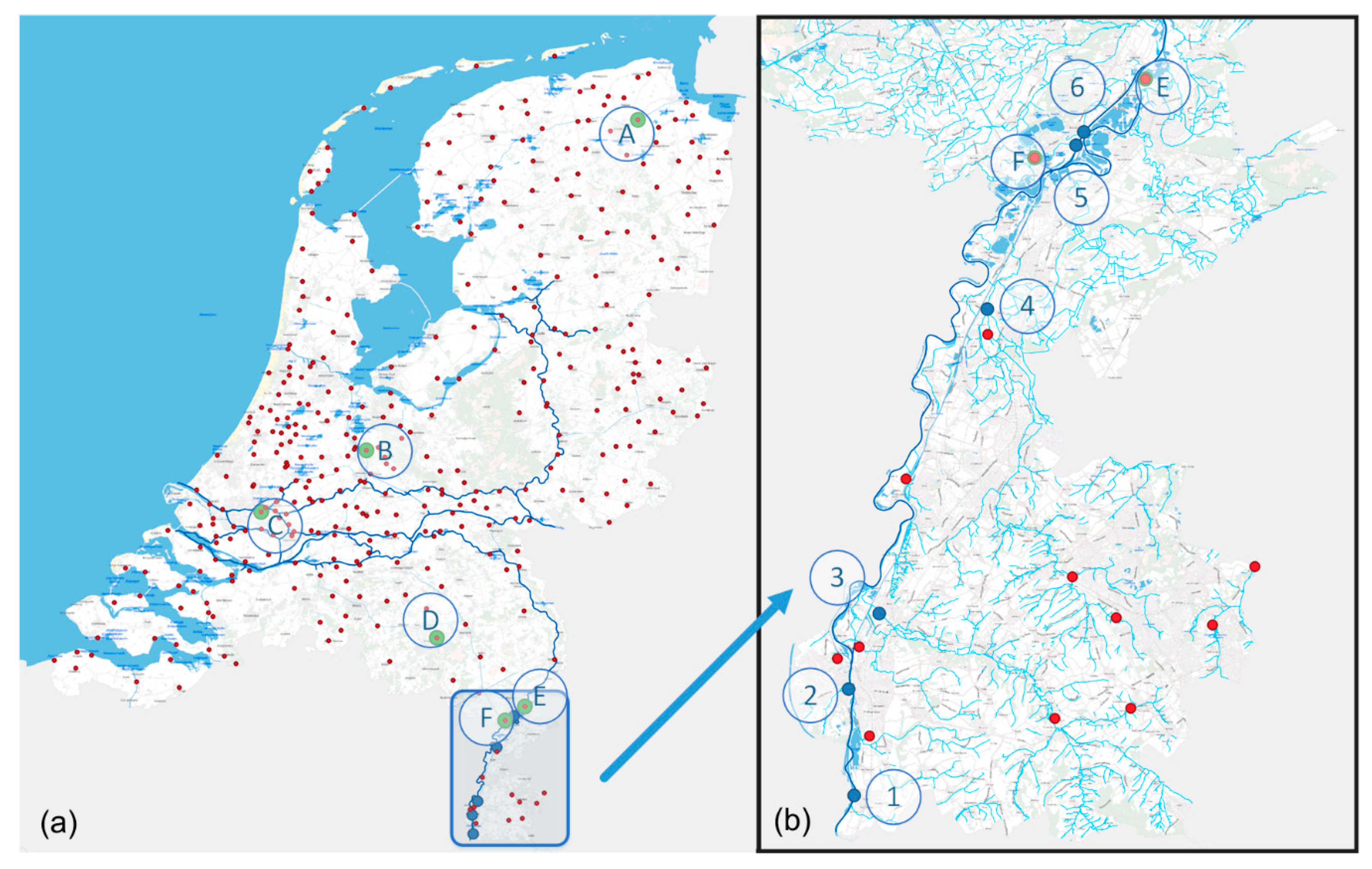
2.2. Study Area and Sampling Points
2.3. National Sampling Campaign
2.4. Wastewater Treatment Pilot Plant Panheel
2.5. Drinking Water Treatment Pilot Plant Heel
3. Results
3.1. Analysis of Wastewater Treatment Plant (WWTP) Effluents
3.2. Pharmaceutical Loads in Surface Waters
3.3. Abatement Options to Protect Surface Water Quality and Drinking Water Production
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Barbosa, M.O.; Moreira, N.F.F.; Ribeiro, A.R.; Pereira, M.F.R.; Silva, A.M.T. Occurrence and removal of organic micropollutants: An overview of the watch list of EU Decision 2015/495. Water Res. 2016, 94, 257–279. [Google Scholar] [CrossRef]
- Richardson, M.L.; Bowron, J.M. The fate of pharmaceutical chemicals in the aquatic environment. J. Pharm. Pharmacol. 1985, 37, 1–12. [Google Scholar] [CrossRef]
- Daughton, C.G.; Ternes, T.A. Pharmaceuticals and personal care products in the environment: Agents of subtle change? Environ. Health Perspect. 1999, 107, 907–938. [Google Scholar] [CrossRef] [PubMed]
- Sui, Q.; Cao, X.; Lu, S.; Zhao, W.; Qiu, Z.; Yu, G. Occurrence, sources and fate of pharmaceuticals and personal care products in the groundwater: A review. Emerg. Contam. 2015, 1, 14–24. [Google Scholar] [CrossRef]
- Van Der Aa, N.G.F.M.; Kommer, G.J.; Van Montfoort, J.E.; Versteegh, J.F.M. Demographic projections of future pharmaceutical consumption in the Netherlands. Water Sci. Technol. 2011, 63, 825–831. [Google Scholar] [CrossRef]
- Klein Tank, A.; Beersma, J.; Bessembinder, J.; van den Hurk, B.; Lenderink, G. KNMI ‘14; Klimaatscenario’s Voor Nederland, Leidraad Voor Professionals in Klimaatadaptatie; 2015 Revised Version; Royal Netherlands Meteorological Institute KNMI: De Bilt, The Netherlands, 2015. (In Dutch)
- Sjerps, R.M.A.; Ter Laak, T.L.; Zwolsman, G.J.J.G. Projected impact of climate change and chemical emissions on water quality of the European rivers Rhine and Meuse: A drinking water perspective. Sci. Total Environ. 2017, 601, 1682–1694. [Google Scholar] [CrossRef]
- Heberer, T. Occurrence, fate, and removal of pharmaceutical residues in the aquatic environment: A review of recent research data. Toxicol. Lett. 2002, 131, 5–17. [Google Scholar] [CrossRef]
- Kidd, K.A.; Blanchfield, P.J.; Mills, K.H.; Palace, V.P.; Evans, R.E.; Lazorchak, J.M.; Flick, R.W. Collapse of a fish population after exposure to a synthetic estrogen. Proc. Natl. Acad. Sci. USA 2007, 104, 8897–8901. [Google Scholar] [CrossRef]
- Crane, M.; Watts, C.; Boucard, T. Chronic aquatic environmental risks from exposure to human pharmaceuticals. Sci. Total Environ. 2006, 367, 23–41. [Google Scholar] [CrossRef]
- Santos, L.H.; Araújo, A.N.; Fachini, A.; Pena, A.; Delerue-Matos, C.; Montenegro, M.C.B.S.M. Ecotoxicological aspects related to the presence of pharmaceuticals in the aquatic environment. J. Hazard. Mater. 2010, 175, 45–95. [Google Scholar] [CrossRef]
- Brodin, T.; Piovano, S.; Fick, J.; Klaminder, J.; Heynen, M.; Jonsson, M. Ecological effects of pharmaceuticals in aquatic systems—Impacts through behavioural alterations. Philos. Trans. R. Soc. B Biol. Sci. 2014, 369. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Commission Implementing Decision (EU) 2015/495 of 20 March 2015 Establishing a Watch List of Substances for Union-Wide Monitoring in the Field of Water Policy Pursuant to Directive 2008/105/EC of the European Parliament and of the Council. Available online: http://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32015D0495&from=EN (accessed on 22 October 2018).
- Carvalho, R.N.; Ceriani, L.; Ippolito, A.; Lettieri, T. Development of the first Watch List under the Environmental Quality Standards Directive; EC Joint Research Centre: Ispra, Italy, 2015. [Google Scholar]
- European Commission. Proposal for a Directive of the European Parliament and of the Council on the Quality of Water Intended for Human Consumption (Recast). Available online: http://eur-lex.europa.eu/resource.html?uri=cellar:8c5065b2-074f-11e8-b8f5-01aa75ed71a1.0016.02/DOC_1&format=PDF (accessed on 22 October 2018).
- Van der Grinten, E.; van der Maaden, T.; van Vlaardingen, P.L.A.; Venhuis, B.J.; Moermond, C.T.A. Milieuafwegingen in de Geneesmiddelvoorziening; Rijksinstituut voor Volksgezondheid en Milieu; Ministerie van Volksgezondheid, Welzijn en Sport: Bilthoven, The Netherlands, 2017. (In Dutch)
- Waterschap Drents Overijsselse Delta. Evaluatie van het Project Milieubewust Medicijnen Voorschrijven Door Huisartsen in Meppel; Waterschap Drents Overijsselse Delta: Meppel, The Netherlands, 2017. (In Dutch) [Google Scholar]
- Mulder, M.; Antakyali, D.; Ante, S. Verwijdering van Microverontreinigingen uit Effluenten van RWZI’s: Een Vertaling van Kennis en Ervaring uit Duitsland en Zwitserland.; Stichting Toegepast Onderzoek Waterbeheer (STOWA): Amersfoort, The Netherlands, 2015. (In Dutch) [Google Scholar]
- Varanasi, L.; Coscarelli, E.; Khaksari, M.; Mazzoleni, L.R.; Minakata, D. Transformations of dissolved organic matter induced by UV photolysis, Hydroxyl radicals, chlorine radicals, and sulfate radicals in aqueous-phase UV-Based advanced oxidation processes. Water Res. 2018, 135, 22–30. [Google Scholar] [CrossRef]
- Nihemaiti, M.; Miklos, D.B.; Hübner, U.; Linden, K.G.; Drewes, J.E.; Croué, J.P. Removal of trace organic chemicals in wastewater effluent by UV/H2O2 and UV/PDS. Water Res. 2018, 145, 487–497. [Google Scholar] [CrossRef] [PubMed]
- Miklos, D.B.; Hartl, R.; Michel, P.; Linden, K.G.; Drewes, J.E.; Hübner, U. UV/H2O2 process stability and pilot-scale validation for trace organic chemical removal from wastewater treatment plant effluents. Water Res. 2018, 136, 169–179. [Google Scholar] [CrossRef]
- Miklos, D.B.; Remy, C.; Jekel, M.; Linden, K.G.; Drewes, J.E.; Hübner, U. Evaluation of advanced oxidation processes for water and wastewater treatment—A critical review. Water Res. 2018, 139, 118–131. [Google Scholar] [CrossRef]
- Miklos, D.B.; Wang, W.L.; Linden, K.G.; Drewes, J.E.; Hübner, U. Comparison of UV-AOPs (UV/H2O2, UV/PDS and UV/Chlorine) for TOrC removal from municipal wastewater effluent and optical surrogate model evaluation. Chem. Eng. J. 2019, 362, 537–547. [Google Scholar] [CrossRef]
- Guo, K.; Wu, Z.; Yan, S.; Yao, B.; Song, W.; Hua, Z.; Zhang, X.; Kong, X.; Li, X.; Fang, J. Comparison of the UV/chlorine and UV/H2O2 processes in the degradation of PPCPs in simulated drinking water and wastewater: Kinetics, radical mechanism and energy requirements. Water Res. 2018, 147, 184–194. [Google Scholar] [CrossRef]
- Ter Laak, T.; Tolkamp, H.; Hofman, J. Geneesmiddelen in de Watercyclus in Limburg; KWR Watercycle Research Institute: Nieuwegein, The Netherlands, 2013. (In Dutch) [Google Scholar]
- Huber, S.A.; Balz, A.; Abert, M.; Pronk, W. Characterisation of aquatic humic and non-humic matter with size-exclusion chromatography—Organic carbon detection—Organic nitrogen detection (LC-OCD-OND). Water Res. 2011, 45, 879–885. [Google Scholar] [CrossRef] [PubMed]
- Hofman-Caris, C.H.M.; Harmsen, D.J.H.; Van Remmen, A.M.; Knol, A.H.; Van Pol, W.L.C.; Wols, B.A. Optimization of UV/H2O2 processes for the removal of organic micropollutants from drinking water: Effect of reactor geometry and water pretreatment on EEO values. Water Sci. Technol. 2017, 17, 508–518. [Google Scholar] [CrossRef]
- Wols, B.A.; Hofman-Caris, C.H.M.; Harmsen, D.J.H.; Beerendonk, E.F. Degradation of 40 selected pharmaceuticals by UV/H2O2. Water Res. 2013, 47, 5876–5888. [Google Scholar] [CrossRef]
- Hofman-Caris, C.H.M.; Siegers, W.G.; van de Merlen, K.; de Man, A.W.A.; Hofman, J.A.M.H. Removal of pharmaceuticals from WWTP effluent: Removal of EfOM followed by advanced oxidation. Chem. Eng. J. 2017, 327, 514–521. [Google Scholar] [CrossRef]
- Wols, B.A.; Harmsen, D.J.H.; van Remmen, T.; Beerendonk, E.F.; Hofman-Caris, C.H.M. Design aspects of UV/H2O2 reactors. Chem. Eng. Sci. 2015, 137, 712–721. [Google Scholar] [CrossRef]
- Vergouwen, A.A.; Pieters, B.J.; Kools, S. ZORG Inventarisatie van Emissie van Geneesmiddelen uit Zorginstellingen; Part C; Stichting Toegepast Onderzoek Waterbeheer (STOWA): Amersfoort, The Netherlands, 2011. (In Dutch) [Google Scholar]
- Niemuth, N.J.; Jordan, R.; Crago, J.; Blanksma, C.; Johnson, R.; Klaper, R.D. Metformin exposure at environmentally relevant concentrations causes potential endocrine disruption in adult male fish. Environ. Toxicol. Chem. 2015, 34, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Niemuth, N.J.; Klaper, R.D. Emerging wastewater contaminant metformin causes intersex and reduced fecundity in fish. Chemosphere 2015, 135, 38–45. [Google Scholar] [CrossRef]
- Société Publique de Gestion de l’Eau. Plan Dássainissement par Sous-Bassin Hydrographique (PASH); Société Publique de Gestion de l’Eau: Verviers, Belgium, 2005. (In French) [Google Scholar]
- Ter Laak, T.L.; Kooij, P.J.F.; Tolkamp, H.; Hofman, J. Different compositions of pharmaceuticals in Dutch and Belgian rivers explained by consumption patterns and treatment efficiency. Environ. Sci. Pollut. Res. 2014, 21, 12843–12855. [Google Scholar] [CrossRef] [PubMed]
- Bourgin, M.; Beck, B.; Boehler, M.; Borowska, E.; Fleiner, J.; Salhi, E.; Teichler, R.; von Gunten, U.; Siegrist, H.; McArdell, C.S. Evaluation of a full-scale wastewater treatment plant upgraded with ozonation and biological post-treatments: Abatement of micropollutants, formation of transformation products and oxidation by-products. Water Res. 2018, 129, 486–498. [Google Scholar] [CrossRef]
- Coppens, L.J.C.; van Gils, J.A.G.; ter Laak, T.L.; Raterman, B.W.; van Wezel, A.P. Towards spatially smart abatement of human pharmaceuticals in surface waters: Defining impact of sewage treatment plants on susceptible functions. Water Res. 2015, 81, 356–365. [Google Scholar] [CrossRef]
- Kümmerer, K. Chapter 7 Benign by design. In Green and Sustainable Medicinal Chemistry: Methods, Tools and Strategies for the 21st Century Pharmaceutical Industry; Somerton, L., Sneddon, H.F., Jones, L.C., Clark, J.H., Eds.; RSC Green Chemistry: Cambridge, UK, 2016; pp. 73–81. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Meuse | Meuse | Geul | Geleenbeek | Slijbeek | Jeker | |
|---|---|---|---|---|---|---|
| ‘Low’ | ‘High’ | |||||
| Discharge (m3/s) | 14 1 | 253 2 | 2.8 3 | 2.1 3 | 0.1 4 | 1.7 3 |
| Near minimum | Above nominal | Nominal | Nominal | Estimated | Nominal | |
| Proportion of WWTP effluent to discharge (%) | No data available | No data available | 15 | 38 | 51 | Unknow; untreated discharges |
| Total pharmaceuticals load (kg/day) | 10 | 106 | 1.4 | 4.9 | 0.1 | 2.2 |
| guanylurea | 25% | 12% | 40% | 60% | 68% | 20% |
| metformine | 47% | 49% | 22% | 13% | 6% | 39% |
| 10,11-trans-diol-carbamazepine | 2% | 2% | 3% | 4% | 5% | 2% |
| metoprolol | 0% | 0% | 3% | 3% | 3% | 0% |
| sotalol | 2% | 2% | 4% | 3% | 3% | 3% |
| hydroxy ibuprofen | 6% | 10% | 9% | 3% | 2% | 9% |
| furosemide | 0% | 0% | 1% | 2% | 1% | 1% |
| tramadol | 2% | 2% | 2% | 2% | 1% | 4% |
| atenolol | 1% | 1% | 0% | 1% | 1% | 1% |
| carbamazepine | 1% | 1% | 1% | 1% | 2% | 1% |
| diclofenac | 1% | 1% | 2% | 1% | 0% | 1% |
| Other 26 compounds | 13% | 19% | 13% | 7% | 8% | 19% |
| Abatement Option | Effect on Drinking Water | Effect on Surface Water | Total Additional Costs 1 | Advantages | Disadvantages |
|---|---|---|---|---|---|
| Prevent and reduce pharmaceutical emission at source (toilets) | Effective | Effective | unknown | Protects aquatic environment | Difficult to realize; long-term effects |
| Different layout of water system; diverting WWTP effluent downstream of the drinking water intake | Effective | Not effective | low | Quick solution | Emergency measure |
| Extension of individual WWTPs | Not effective unless realized on multiple locations | Effective for small surface waters | 8–15 M€/year | Local improvement of surface water quality | Only effective for drinking water on long-term and at large-scale application |
| Extension of WWTPs on a large, international scale | Effective | Effective | 8–15 M€/year in The Netherlands | Strong improvement of surface water quality | Long-term realization |
| Extension drinking water treatment | Effective | Not effective | 4–8 M€/year | Short-term realization | No improvement of surface water quality |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hofman-Caris, R.; ter Laak, T.; Huiting, H.; Tolkamp, H.; de Man, A.; van Diepenbeek, P.; Hofman, J. Origin, Fate and Control of Pharmaceuticals in the Urban Water Cycle: A Case Study. Water 2019, 11, 1034. https://doi.org/10.3390/w11051034
Hofman-Caris R, ter Laak T, Huiting H, Tolkamp H, de Man A, van Diepenbeek P, Hofman J. Origin, Fate and Control of Pharmaceuticals in the Urban Water Cycle: A Case Study. Water. 2019; 11(5):1034. https://doi.org/10.3390/w11051034
Chicago/Turabian StyleHofman-Caris, Roberta, Thomas ter Laak, Hans Huiting, Harry Tolkamp, Ad de Man, Peter van Diepenbeek, and Jan Hofman. 2019. "Origin, Fate and Control of Pharmaceuticals in the Urban Water Cycle: A Case Study" Water 11, no. 5: 1034. https://doi.org/10.3390/w11051034
APA StyleHofman-Caris, R., ter Laak, T., Huiting, H., Tolkamp, H., de Man, A., van Diepenbeek, P., & Hofman, J. (2019). Origin, Fate and Control of Pharmaceuticals in the Urban Water Cycle: A Case Study. Water, 11(5), 1034. https://doi.org/10.3390/w11051034