1. Introduction
Opportunistic premise plumbing pathogens (OPPPs) such as
Pseudomonas aeruginosa (
P. aeruginosa),
Legionella pneumophila (
L. pneumophila),
Mycobacterium avium (
M. avium), and
Naegleria fowleri (
N. fowleri) can pose a serious risk to human health, and even death in some cases, when contacted through contaminated water [
1,
2,
3]. OPPPs are responsible for a large number of infections and the risk of infections is increasing significantly day by day [
2,
3]. For example, the crude national incidence rate of
Legionella spp. infections increased by about 350% in the United States, from 0.42 cases per 100,000 persons to 1.89 between 2000 to 2015 [
4]. Nearly 40,000 hospitalizations per year have been reported in the United States and the cost of treatment for the relevant diseases (i.e., Legionnaires’ disease, cryptosporidiosis, giardiasis, non-tuberculous mycobacterial infection, and otitis externa) exceeds
$900 million [
5]. Previous studies have been conducted to provide risk-based boundary concentrations for
L. pneumophila [
6], but no such studies have been conducted for
P. aeruginosa and
N. fowleri to protect human health.
P. aeruginosa, a common opportunistic pathogen, has been reported to be responsible for about 17% of nosocomial pneumonia cases and 11% cases of urinary tract infection (UTI) as well as surgical site infections in the US between 1992 and 1997 [
7]. Most of the
P. aeruginosa infections occur among hospital patients and immunocompromised peoples through exposure to the eyes and ears [
1]. Most of these infections can cause severe illness such as meningitis, UTI, community-acquired pneumonia (CAP) [
8,
9], and even death in extreme cases [
10]. Over the years, antimicrobial drug resistance in
Pseudomonas has led to serious restrictions in treatment options for such infections [
1] which cause about 51,000 healthcare-related infections every year in the US [
11]. The most common routes of
P. aeruginosa infection are exposure to contaminated water through ingestion and skin contact; and even greater risk of infection may occur due to lung exposure through inhalation [
12]. The potential scenarios of
P. aeruginosa exposure include swimming in contaminated water, using contaminated hot tubs, cleaning contact lenses with contaminated tap water, and through medical equipment and medical workers in a hospital setting [
12,
13]. Serious
P. aeruginosa infections are usually found in hospitals and/or immunocompromised people [
14]. However, healthy people may also develop mild illness after exposure to contaminated water [
15]. Eye infection is one of the commonly reported infections due to
P. aeruginosa; particularly through the use of contaminated contact lenses [
16].
Naegleria fowleri, the only species that has been known to cause primary amoebic meningoencephalitis (PAM), is a free-living amoeba that occurs naturally in soil and water and thrives at temperatures between 25 °C and 42 °C [
17].
N. fowleri infections can only occur when contaminated water enters a person’s body through the nose [
18]. PAM has an high fatality rate, up to 98% [
19,
20]. Infection occurs when
N. fowleri travels through the nose into the brain through the cribriform plate and begins consuming brain cells (i.e., astrocytes and neurons) [
21,
22]. Only four people survived out of 143 PAM infections cases reported in the United States during the period of 1962–2017 [
23,
24]. Most PAM cases are reported in children and young adults with a history of swimming in naturally warm waters; however, it has also been suggested that infection can be caused by inhaling and ingesting contaminated water during bathing and neti pot™ usage [
25].
Quantitative microbial risk assessment (QMRA) is the process of estimating the risk, (i.e., the probability of an adverse effect such as infection, illness, and/or death) from exposure to microorganisms, usually waterborne, foodborne, or airborne [
26]. A typical QMRA approach starts with an environmental concentration of microorganisms as input and then calculates the associated risk as an output. QMRA studies are typically conducted to calculate the risk of infection and/or illness due to exposures from different concentrations/doses of waterborne pathogens [
26,
27,
28,
29,
30,
31,
32,
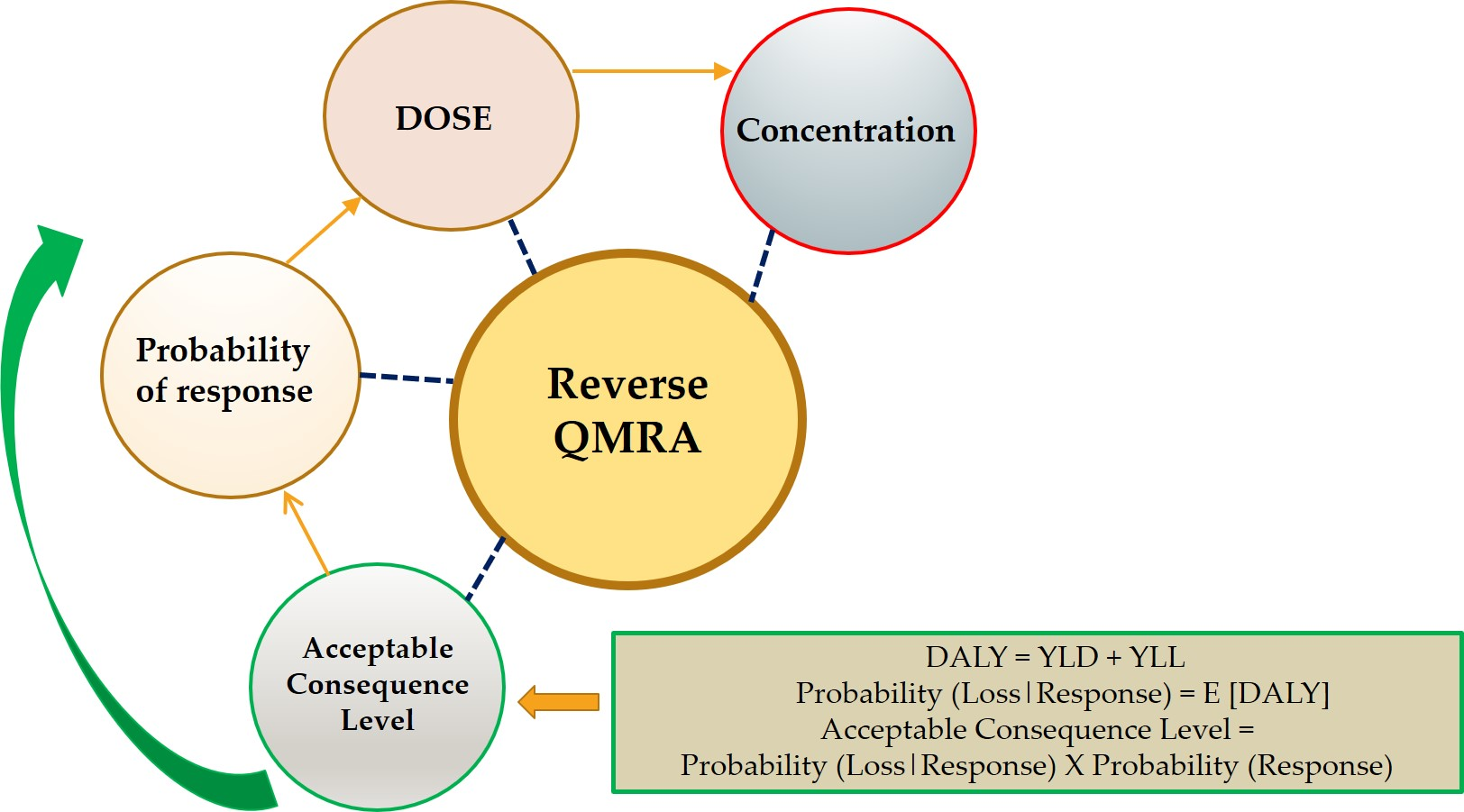
33]. At the same time, the QMRA approach can also be useful in quality control and setting microbial water quality standards where a critical level of risk (i.e., the boundary between actionable and non-actionable risk) can be used to differentiate between acceptable and unacceptable concentrations of microorganisms. The concentrations of
P. aeruginosa and
N. fowleri in water samples can be determined using microbiological analyses, and then the QMRA-based critical concentrations can be used in interpreting the results of microbial analyses and provide guidance on what concentrations may be considered tolerable (i.e., acceptable risks) and what action levels are required. This process of calculating the critical microbial concentration based on the critical level of risk is referred to as the “reverse QMRA” approach [
6,
34,
35]. While potentially useful in setting up guidelines and monitoring waterborne and airborne microbial risk, reverse QMRA-based studies are rare in the literature, except Hamilton et al., (2019) [
6] have recently used this approach to calculate the critical concentration of
Legionella pneumophila for indoor residential water usage. To the best of our knowledge, this approach has not been applied to other waterborne opportunistic pathogens.
In this study, our goal was to use a reverse QMRA approach to calculate critical concentrations of
P. aeruginosa and
N. fowleri based on acceptable risk values in potable and recreational water at point of use systems. Two different health-based target risk values (i.e., 10
−4 annual probability of illness [
36] and 10
−6 disability-adjusted life years per person per year [
37]) were considered for this study. Disability-adjusted life years (DALYs) is a commonly used metric used for quantifying the burden of disease from mortality and morbidity [
37]. Heating of water is used worldwide to treat and provide safe water [
38]. Previous studies recommended heating of water as a sufficient measure to inactivate microbial pathogens [
39]. Considering the lack of guidance on the critical concentrations of
P. aeruginosa and
N. fowleri, the objectives of this study were to (a) calculate the boundary concentrations of
P. aeruginosa for contact lens exposure scenarios and of
N. fowleri for neti pot™ use and swimming exposure scenarios based on the established target risk values using the reverse QMRA approach and (b) compare the values considering hot water vs. room temperature water usage scenario for contact lens exposure of
P. aeruginosa and neti pot™ exposure of
N. fowleri. 4. Discussion
The risks of hospital-acquired and cystic fibrosis infections and even deaths caused by
P. aeruginosa are increasing every year in the United States [
14]. Infections caused by
P. aeruginosa are also becoming very difficult to treat due to the multiple antibiotic resistance of this microorganism [
14,
15]. Infection scenarios discussed in this study for
P. aeruginosa become even more relevant because studies have found that
P. aeruginosa survives for up to 4 h in the standard lens cleaning solution [
55], indicating that contaminated cleaning solution could conceivably be a source of exposure. Therefore, the concentration values identified in this study could also be applicable to appropriate cleaning solutions. Even though the risk of infection caused by the
N. fowleri is very low, the extremely high fatality rate makes it a matter of great concern. Standards for monitoring critical concentrations, that delineate acceptable risks, of
P. aeruginosa and
N. fowleri in premise plumbing and other recreational waters are rare in the literature. Only a few critical concentration values for
P. aeruginosa are available [
12,
15,
56,
57], and the reported values lack a documented scientific basis for how they were obtained. For
N. fowleri the critical concentration values are not available at all. Therefore, risk-based boundary concentration values corresponding to acceptable risks for these microorganisms are highly sought by regulatory agencies to enforce standards to ensure public safety against infections/deaths caused by these pathogens.
To calculate the boundary concentrations of
P. aeruginosa and
N. fowleri, several assumptions were made in setting health-based risk values, exposure routes, and contact scenarios. Commonly accepted target values of 10
−4 annual risk of illness (see footnote to
Table 6) and 10
−6 DALYs per person per year were selected as health-based risk metrics [
6,
36,
37]. In general, the DALY based metric will generate lower values of critical concentrations for both microorganisms compared to the annual risk-based metric. The DALY metric and the annual risk metric used in this study were more closely aligned for less severe illnesses such as gastrointestinal (GI) illness [
58]. When the annual risk metric will be considered, the DALY/case would yield a value of 10
−2 for such illnesses, but for exposure to even low levels of OPPPs such as
Naegleria fowleri would produce a much higher DALY/case which makes the DALY approach more restrictive. The risk interpretation and implementation of the critical concentration values calculated in this study are also dependent on other factors such as contact scenarios under consideration and the dose–response models used.
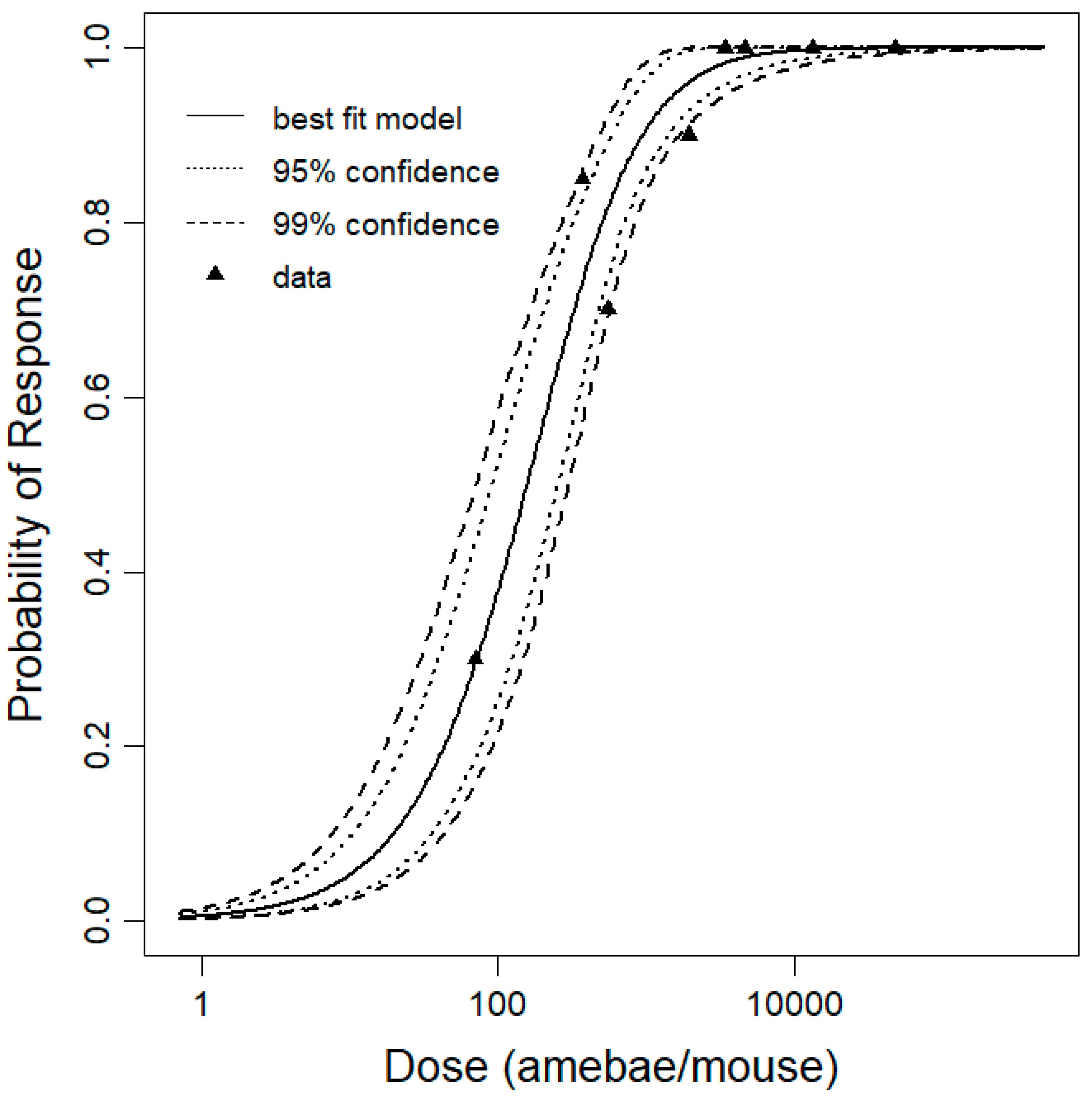
Previously the dose–response model for
N. fowleri was developed using intranasal and swimming exposure to CD1 mice [
51], but for our study only intranasal exposure to Swiss OF1 female mice were considered. In the Dean et al., (2019) [
51] study, the intranasal exposure experiment data was based on 10 mice per dose but for our study 10 to 20 mice per dose were used to develop the dose–response model. The beta-Poisson model was reported as the best fit dose–response model for
N. fowleri [
51] which was consistent with our results as the pooled data for our dose–response model were also best fit with the beta-Poisson model. The beta-Poisson curve for our best fit data was much steeper than the curves of previous studies (
Figure 2) which indicates a higher probability of death at low doses [
51].
The choice of target risk values of illness per event caused by
P. aeruginosa and
N. fowleri for both the risk metrics used in this study fell within the acceptable limit of 10
−4 to 10
−6 set forth by Environmental Protection Agency (EPA) [
59]. The two methods of contact rate measurements in the contact lens scenarios (Scenarios 1a and 1b) predicted similar critical concentrations of
P. aeruginosa, for the DALY risk metric (mean concentration 0.30 to 0.33 CFU/L) and annual risk metric (mean concentration range from 30 to 33 CFU/L); the critical concentrations based on experimental measurements may be a more reliable method to choose. There are no specific regulations available to control
P. aeruginosa in municipal drinking water at domestic and healthcare facilities in the United States. However, regulations to control
P. aeruginosa both in domestic premise plumbing, as well as immune-compromised patients in hospitals are available, though contradictory, in other countries. For example, the Department of Health in the United Kingdom suggests that
P. aeruginosa should be undetected in healthcare facilities [
56] and the European Union [
57] suggest a standard of non-detectable
P. aeruginosa in 250 mL volumes of water in bottled water [
12]. For health care facilities that are relatively more prone to infections the French Ministry of Social Affairs and Health guidelines recommend 10 CFU/L
P. aeruginosa in water as safety standard [
15]. These contradictory guidelines may have been the result of the differences in the recommended microbial measurement approaches. The acceptable risk critical concentrations of
P. aeruginosa calculated for the contact lens risk scenarios simulated in this study roughly agree with the UK and European Union guidelines when DALY metric was used (mean concentration 0.30 CFU/L) and with French guidelines when the annual risk-based metric was used (mean concentration 29.95 CFU/L). Even though the predicted critical concentrations in this study are more or less in agreement with the available guidelines values, previous studies have reported more than two fold higher mean concentrations (i.e., 70 CFU/L) of
P. aeruginosa in tap water samples in Southern Greece [
60]. This may have been because of various other factors, including different
P. aeruginosa isolates used for the dose–response model in this study, and warrants further investigation. The detection limit of
P. aeruginosa was found to be 330 CFU·PCR
−1 [
61]. Considering 330 cells of
P. aeruginosa and 10 L as a volume of water sample to be filtered, the detection limit of
P. aeruginosa would be 33 CFU/L. This detection limit of concentration is aligned with our calculated boundary concentration which might be costly and difficult to filter but filtering greater sample volumes would produce more precise measurements. Also, the relationship between boundary concentration and number of exposure events was found to be linear. In cases where exposures are less frequent (i.e., smaller
N), the boundary concentration would be higher and hence easier to detect.
Since no specific guideline documents are available for exposure risk from
N. fowleri, the critical concentrations values obtained in this study may help develop standards for swimming (Scenario 2) and neti pot™ use (Scenario 3) exposure scenarios. In general, the tolerable critical concentrations of
N. fowleri are much lower compared to those for
P. aeruginosa except for the swimming scenario with the annual risk metric which is still more than an order of magnitude below the
P. aeruginosa values. The critical concentrations for neti pot™ use are lower than the swimming scenarios for both risk metrics which is still more than an order of magnitude below the
P. aeruginosa values, which can be attributed to the higher contact rate during neti pot™ use compared to swimming. These results seem in agreement with the general perception that one would expect stringent standard requirement for neti pot™ use where water is forced through the nose and therefore the possibility of entering the brain is high. The tolerable mean critical concentration of
N. fowleri for the swimming scenario with the annual risk metric has a mean concentration 1.4 CFU/L, with a range from 0.29 to 4.0 CFU/L. Given that the end response is death with a 100% percent mortality rate, it may be wise to pick a lower range of critical concentration (0.29 CFU/L) for developing standards, and the same can be applied for developing standards for other scenarios related to
N. fowleri. Previous studies found the detection limit of
N. fowleri to be 1–50 cells per reaction using both the nested and real-time PCR assays [
19]. Considering 50 cells of
N. fowleri and 200 L as a volume of water sample to be filtered, the detection limit of
N. fowleri would be 0.25
N. fowleri/L which is also aligned with our calculated boundary concentration of
N. fowleri using the annual risk metric.
Higher tolerable concentration standard can be set for using hot plumbing water for contact lenses exposure scenarios for
P. aeruginosa but not for exposure scenarios for
N. fowleri. Optimum growth temperature for
P. aeruginosa and
N. fowleri are quite different.
P. aeruginosa can grow at temperatures between 10–42 °C, with an optimum growth temperature at 37 °C [
15]. For
N. fowleri, the growth temperatures are between 25–42 °C, and they can continue to survive for a long time at lower temperatures [
19]. Temperatures between 55–65 °C are generally suggested as effective for the elimination of waterborne pathogens, hot water temperatures above 60 °C are considered to present a risk of scalding [
62] and pipe corrosion [
63]. Thus, 55 °C is generally considered as microbial inactivation temperature and is used in premise plumbing. The mean critical concentrations for
P. aeruginosa were increased by approximately two-fold for both scenarios using heat treatment (Scenario 4a,b). Though this increment indicated that temperature control may be used to eradicate
P. aeruginosa from premise plumbing water systems; it may not have an impact on setting standard guidelines since the allowable mean concentrations are still undetectable (0.55 CFU/L, DALY metric) or at the lower end of the detectable range (55 CFU/L, annual rick metric) of most of the culture-based assays. The change in critical concentrations for
N. fowleri after heat treatment was not significant. This might be due to the low heat inactivation constant for
N. fowleri (
Table 7).
There are various limitations of this study. Dose–response data used in this study were subject to uncertainty and variability which eventually influenced the calculated critical concentrations of P. aeruginosa and N. fowleri. More nasal instillation data are required to address this uncertainty and variability for N. fowleri. Uncertainty due to variation of frequencies of activities (i.e., swimming, neti pot™ use) and volume of water entering into the brain should be studied and analyzed to estimate the burden of disease associated with these organisms. The use L. pneumophila associated with Acanthamoeba trophozoites heat activation data for N. fowleri also introduced uncertainty in the heat inactivation estimates for N. fowleri.

 ,
, 





{kind=link}
{kind=link}
{kind=link}