

Intravenous Immunoglobulins as Immunomodulators in Autoimmune Diseases and Reproductive Medicine

 ,
,  ,
,  , , and
, , and
Abstract
:1. Introduction
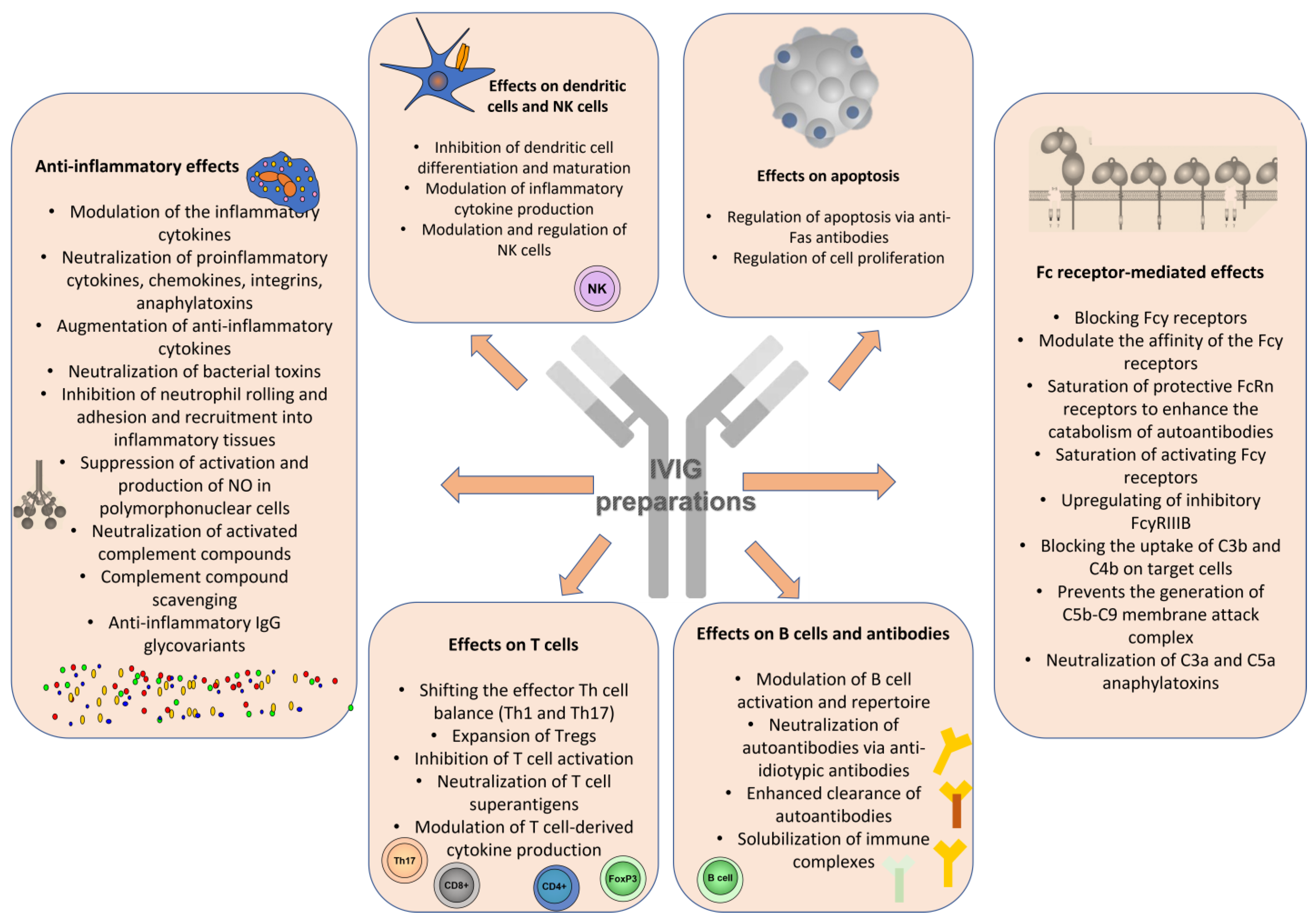
2. Immune Mechanisms of IVIGs as Immunomodulators
2.1. IVIG Effects on Antigen-Presenting Cells and Proinflammatory Cytokine Production
2.2. IVIG Effect on NK and NKT Cells
2.3. IVIG Effects on Adaptive Immune Cells
2.4. Dose-Dependent Effects of IVIGs and Relevant Immunoglobulin Receptors
3. IVIG Treatment for Autoimmune Diseases
3.1. Idiopathic Autoimmune Inflammatory Myositis
3.2. Systemic Lupus Erythematosus
3.3. Anti-Phospholipid Syndrome
3.4. Systemic Sclerosis
3.5. Kawasaki Disease
3.6. ANCA-Associated Vasculitides
3.7. Gastrointestinal Autoimmune Diseases
3.8. Autoimmune Neurological Disorders
3.9. Other Autoimmune Diseases
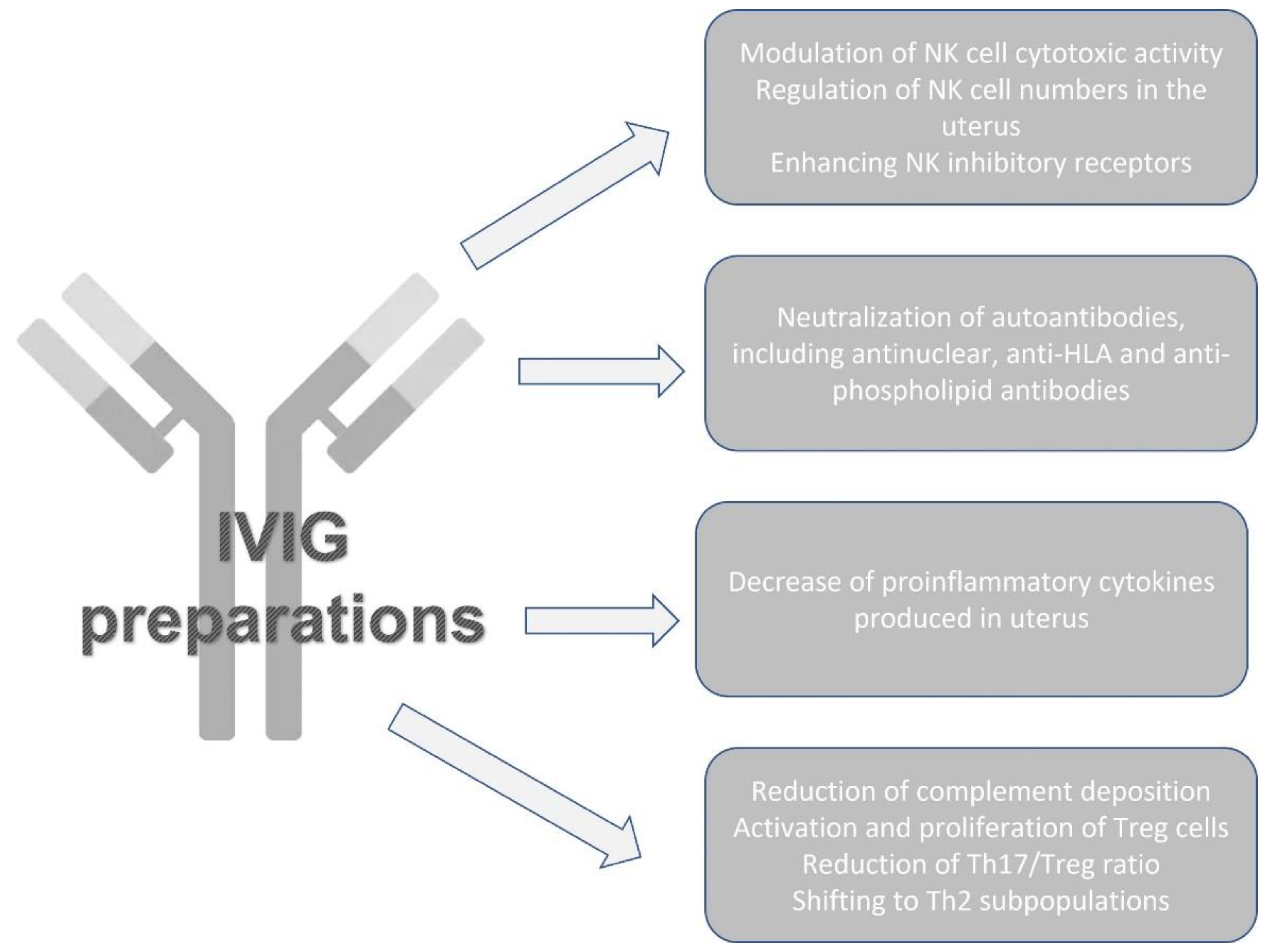
4. IVIGs as Immunomodulators in Patients with Reproduction Failures
4.1. IVIGs for Immune Cells Modulation
4.2. Obstetric APS
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Navarro, R.P.; Ballow, M.; Fenrick, B.; Pezalla, E.J. Considerations for the optimal use of immunoglobulin. Am. J. Manag. Care 2012, 18, S67–S78. [Google Scholar]
- Koblet, H.; Barandun, S.; Diggelmann, H. Turnover of standard-gammaglobulin, pH-4-gammaglobulin and pepsin desaggregated gammaglobulin and clinical implications. Vox Sang. 1967, 13, 93–102. [Google Scholar]
- Kazatchkine, M.D.; Kaveri, S.V. Immunomodulation of Autoimmune and Inflammatory Diseases with Intravenous Immune Globulin. N. Engl. J. Med. 2001, 345, 747–755. [Google Scholar] [CrossRef]
- Sakthiswary, R.; D’Cruz, D. Intravenous immunoglobulin in the therapeutic armamentarium of systemic lupus erythematosus: A systematic review and meta-analysis. Medicine 2014, 93, e86. [Google Scholar] [CrossRef]
- Pyne, D.; Ehrenstein, M.; Morris, V. The therapeutic uses of intravenous immunoglobulins in autoimmune rheumatic diseases. Rheumatology 2002, 41, 367–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Novaretti, M.C.Z.; Dinardo, C.L. Clinical applications of immunoglobulin. Rev. Bras. Hematol. Hemoter. 2011, 33, 221–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gelfand, E.W. Intravenous Immune Globulin in Autoimmune and Inflammatory Diseases. N. Engl. J. Med. 2012, 367, 2015–2025. [Google Scholar] [CrossRef] [PubMed]
- Bayry, J.; Misra, N.; Latry, V.; Prost, F.; Delignat, S.; Lacroix-Desmazes, S.; Kazatchkine, M.; Kaveri, S. Mechanisms of action of intravenous immunoglobulin in autoimmune and inflammatory diseases. Transfus. Clin. Biol. 2003, 10, 165–169. [Google Scholar] [CrossRef]
- Negi, V.-S.; Elluru, S.R.; Siberil, S.; Graff-Dubois, S.; Mouthon, L.; Kazatchkine, M.D.; Lacroix-Desmazes, S.; Bayry, J.; Kaveri, S.V. Intravenous Immunoglobulin: An Update on the Clinical Use and Mechanisms of Action. J. Clin. Immunol. 2007, 27, 233–245. [Google Scholar] [CrossRef]
- Patil, V.; Kaveri, S.V. The mechanisms of action of IVIG in autoimmune and inflammatory diseases. ISBT Sci. Ser. 2013, 8, 185–188. [Google Scholar] [CrossRef]
- Rigal, D.; Vermot-Desroches, C.; Heitz, S.; Bernaud, J.; Alfonsi, F.; Monier, J. Effects of Intravenous Immunoglobulins (IVIG) on Peripheral Blood B, NK, and T Cell Subpopulations in Women with Recurrent Spontaneous Abortions: Specific Effects on LFA-1 and CD56 Molecules. Clin. Immunol. Immunopathol. 1994, 71, 309–314. [Google Scholar] [CrossRef]
- Kwak, J.; Kwak, F.; Ainbinder, S.; Ruiz, A.; Beer, A. Elevated Peripheral Blood Natural Killer Cells Are Effectively Downregulated by Immunoglobulin G Infusion in Women with Recurrent Spontaneous Abortions. Am. J. Reprod. Immunol. 1996, 35, 363–369. [Google Scholar] [CrossRef]
- Finberg, R.W.; Newburger, J.W.; Mikati, M.A.; Heller, A.H.; Burns, J.C. Effect of high doses of intravenously administered immune globulin on natural killer cell activity in peripheral blood. J. Pediatr. 1992, 120, 376–380. [Google Scholar] [CrossRef]
- Araujo, L.M.; Chauvineau, A.; Zhu, R.; Diem, S.; Bourgeois, E.A.; Levescot, A.; Huerre, M.; Gombert, J.-M.; Bayry, J.; Daëron, M.; et al. Cutting edge: Intravenous Ig inhibits invariant NKT cell-mediated allergic airway inflammation through FcγRIIIA-dependent mechanisms. J. Immunol. 2011, 186, 3289–3293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Séïté, J.-F.; Cornec, D.; Renaudineau, Y.; Youinou, P.; Mageed, R.A.; Hillion, S. IVIg modulates BCR signaling through CD22 and promotes apoptosis in mature human B lymphocytes. Blood 2010, 116, 1698–1704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bayry, J.; Fournier, E.M.; Maddur, M.S.; Vani, J.; Wootla, B.; Sibéril, S.; Dimitrov, J.D.; Lacroix-Desmazes, S.; Berdah, M.; Crabol, Y.; et al. Intravenous immunoglobulin induces proliferation and immunoglobulin synthesis from B cells of patients with common variable immunodeficiency: A mechanism underlying the beneficial effect of IVIg in primary immunodeficiencies. J. Autoimmun. 2011, 36, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Kessel, A.; Ammuri, H.; Peri, R.; Pavlotzky, E.R.; Blank, M.; Shoenfeld, Y.; Toubi, E. Intravenous immunoglobulin therapy affects T regulatory cells by increasing their suppressive function. J. Immunol. 2007, 179, 5571–5575. [Google Scholar] [CrossRef] [Green Version]
- Ephrem, A.; Chamat, S.; Miquel, C.; Fisson, S.; Mouthon, L.; Caligiuri, G.; Delignat, S.; Elluru, S.R.; Bayry, J.; Lacroix-Desmazes, S.; et al. Expansion of CD4+ CD25+ regulatory T cells by intravenous immunoglobulin: A critical factor in controlling experimental autoimmune encephalomyelitis. Blood 2008, 111, 715–722. [Google Scholar] [CrossRef] [PubMed]
- Maddur, M.S.; Kaveri, S.V.; Bayry, J. Comparison of different IVIg preparations on IL-17 production by human Th17 cells. Autoimmun. Rev. 2011, 10, 809–810. [Google Scholar] [CrossRef]
- Hulett, M.D.; Hogarth, P.M. Molecular Basis of Fc Receptor Function. Adv. Immunol. 1994, 57, 1–127. [Google Scholar]
- Rossi, F.; Kazatchkine, M.D. Antiidiotypes against autoantibodies in pooled normal human polyspecific Ig. J. Immunol. 1989, 143, 4104–4109. [Google Scholar] [CrossRef] [PubMed]
- Basta, M. Ambivalent effect of immunoglobulins on the complement system: Activation versus inhibition. Mol. Immunol. 2008, 45, 4073–4079. [Google Scholar] [CrossRef]
- Spahn, J.D.; Leung, D.Y.; Chan, M.T.; Szefler, S.J.; Gelfand, E.W. Mechanisms of glucocorticoid reduction in asthmatic subjects treated with intravenous immunoglobulin. J. Allergy Clin. Immunol. 1999, 103, 421–426. [Google Scholar] [CrossRef] [PubMed]
- Schwab, I.; Nimmerjahn, F. Intravenous immunoglobulin therapy: How does IgG modulate the immune system? Nat. Rev. Immunol. 2013, 13, 176–189. [Google Scholar] [CrossRef] [PubMed]
- Yates, M.; A Watts, R.; Bajema, I.M.; Cid, M.C.; Crestani, B.; Hauser, T.; Hellmich, B.; Holle, J.U.; Laudien, M.; A Little, M.; et al. EULAR/ERA-EDTA recommendations for the management of ANCA-associated vasculitis. Ann. Rheum. Dis. 2016, 75, 1583–1594, Erratum in: Ann. Rheum Dis. 2017, 76, 1480; Erratum in: Ann. Rheum Dis. 2022, 81, e109. [Google Scholar] [CrossRef] [Green Version]
- Katz-Agranov, N.; Khattri, S.; Zandman-Goddard, G. The role of intravenous immunoglobulins in the treatment of rheumatoid arthritis. Autoimmun. Rev. 2015, 14, 651–658. [Google Scholar] [CrossRef]
- Mulhearn, B.; Bruce, I.N. Indications for IVIG in rheumatic diseases. Rheumatology 2014, 54, 383–391. [Google Scholar] [CrossRef] [Green Version]
- Shoenfeld, Y.; Katz, U. IVIg therapy in autoimmunity and related disorders: Our experience with a large cohort of patients. Autoimmunity 2005, 38, 123–137. [Google Scholar] [CrossRef]
- Dalakas, M.C. Inflammatory Myopathies. In Handbook of Clinical Neurology; Rowland, L.P., DiMauro, S., Eds.; Elsevier Science: Amsterdam, The Netherlands, 1992; Volume 18, pp. 369–390. [Google Scholar]
- Dalakas, M.C. Inflammatory myopathies. Curr. Opin. Neurol. Neurosurg 1990, 3, 689–696. [Google Scholar]
- Emslie-Smith, A.M.; Arahata, K.; Engel, A.G. Major histocompatibility complex class I antigen expression, immunolocalization of interferon subtypes, and T cell-mediated cytotoxicity in myopathies. Hum. Pathol. 1989, 20, 224–231. [Google Scholar] [CrossRef]
- Engel, A.G.; Arahata, K. Mononuclear cells in myopathies: Quantitation of functionally distinct subsets, recognition of antigen-specific cell-mediated cytotoxicity in some diseases, and implications for the pathogenesis of the different inflammatory myopathies. Hum. Pathol. 1986, 17, 704–721. [Google Scholar] [CrossRef] [PubMed]
- Kissel, J.T.; Mendell, J.R.; Rammohan, K.W. Microvascular deposition of complement membrane attack complex in dermatomyositis. N. Engl. J. Med. 1986, 314, 329–334. [Google Scholar] [CrossRef] [PubMed]
- Oxford Centre for Evidence-Based Medicine: Levels of Evidence (March 2009). Available online: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/oxford-centre-for-evidence-based-medicine-levels-of-evidence-march-2009 (accessed on 15 February 2023).
- Oddis, C.V. Update on the pharmacological treatment of adult myositis. J. Intern. Med. 2016, 280, 63–74. [Google Scholar] [CrossRef] [Green Version]
- Dalakas, M.C. Mechanistic Effects of IVIg in Neuroinflammatory Diseases: Conclusions Based on Clinicopathologic Correlations. J. Clin. Immunol. 2014, 34, S120–S126. [Google Scholar] [CrossRef] [PubMed]
- Dalakas, M.C.; Illa, I.; Dambrosia, J.M.; Soueidan, S.A.; Stein, D.P.; Otero, C.; Dinsmore, S.T.; McCrosky, S. A Controlled Trial of High-Dose Intravenous Immune Globulin Infusions as Treatment for Dermatomyositis. N. Engl. J. Med. 1993, 329, 1993–2000. [Google Scholar] [CrossRef]
- Marie, I.; Menard, J.-F.; Hatron, P.Y.; Hachulla, E.; Mouthon, L.; Tiev, K.; Ducrotte, P.; Cherin, P. Intravenous immunoglobulins for steroid-refractory esophageal involvement related to polymyositis and dermatomyositis: A series of 73 patients. Arthritis Care Res. 2010, 62, 1748–1755. [Google Scholar] [CrossRef]
- Suzuki, Y.; Hayakawa, H.; Miwa, S.; Shirai, M.; Fujii, M.; Gemma, H.; Suda, T.; Chida, K. Intravenous Immunoglobulin Therapy for Refractory Interstitial Lung Disease Associated with Polymyositis/Dermatomyositis. Lung 2009, 187, 201–206. [Google Scholar] [CrossRef]
- Cherin, P.; Pelletier, S.; Teixeira, A.; Laforet, P.; Genereau, T.; Simon, A.; Maisonobe, T.; Eymard, B.; Herson, S. Results and long-term follow-up of intravenous immunoglobulin infusions in chronic, refractory polymyositis: An open study with thirty-five adult patients. Arthritis Rheum. 2002, 46, 467–474. [Google Scholar] [CrossRef]
- Soueidan, S.A.; Dalakas, M.C. Treatment of inclusion-body myositis with high-dose intravenous immunoglobulin. Neurology 1993, 43, 876. [Google Scholar] [CrossRef]
- Danieli, M.G.; Gambini, S.; Pettinari, L.; Logullo, F.; Veronesi, G.; Gabrielli, A. Impact of treatment on survival in polymyositis and dermatomyositis. A single-centre long-term follow-up study. Autoimmun. Rev. 2014, 13, 1048–1054. [Google Scholar] [CrossRef]
- Aggarwal, R.; Charles-Schoeman, C.; Schessl, J.; Bata-Csorgo, Z.; Dimachkie, M.; Zoltan, G.; Sergey, M.; Chester, O.; Elena, S.; Jiri, V.; et al. The ProDERM study: Safety and Tolerability Results from randomized, double-blind, placebo-controlled Phase-III-Trial in Patients with Dermatomyositis (P3-1.004). Neurology 2022, 98 (Suppl. S18), 2564. [Google Scholar]
- Aggarwal, R.; Charles-Schoeman, C.; Schessl, J.; Dimachkie, M.M.; Beckmann, I.; Levine, T. Prospective, double-blind, randomized, placebo-controlled phase III study evaluating efficacy and safety of octagam 10% in patients with dermatomyositis (“ProDERM Study”). Medicine 2021, 100, e23677. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, R.; Charles-Schoeman, C.; Schessl, J.; Bata-Csörgő, Z.; Dimachkie, M.M.; Griger, Z.; Moiseev, S.; Oddis, C.; Schiopu, E.; Vencovský, J.; et al. Trial of Intravenous Immune Globulin in Dermatomyositis. N. Engl. J. Med. 2022, 387, 1264–1278. [Google Scholar] [CrossRef]
- Kocoloski, A.D.; Martinez, S.; Moghadam-Kia, S.M.; Lacomis, D.; Oddis, C.V.; Ascherman, D.P.; Aggarwal, R.M. Role of Intravenous Immunoglobulin in Necrotizing Autoimmune Myopathy. Am. J. Clin. Oncol. 2021, 28, e517–e520. [Google Scholar] [CrossRef] [PubMed]
- Corvetta, A.; Della Bitta, R.; Gabrielli, A.; Spaeth, P.J.; Danieli, G. Use of high-dose intravenous immunoglobulin in systemic lupus erythematosus: Report of three cases. Ann. Rheum. Dis. 1989, 7, 295–299. [Google Scholar]
- Basta, M. Modulation of complement-mediated immune damage by intravenous immune globulin. Clin. Exp. Immunol. 1996, 104, 21–25. [Google Scholar] [CrossRef]
- Ballow, M. Mechanisms of action of intravenous immunoglobulin therapy and potential use in autoimmune connective tissue diseases. Cancer 1991, 68 (Suppl. S6), 1430–1436. [Google Scholar] [CrossRef]
- HYamada; Morikawa, M.; Furuta, I.; Kato, E.; Shimada, S.; Iwabuchi, K.; Minakami, H. Intravenous immunoglobulin treatment in women with recurrent abortions: Increased cytokine levels and reduced Th1/Th2 lymphocyte ratio in peripheral blood. Am. J. Reprod. Immunol. 2003, 49, 84. [Google Scholar]
- Toubi, E.; Kessel, A.; Shoenfeld, Y. High-Dose Intravenous Immunoglobulins: An Option in the Treatment of Systemic Lupus Erythematosus. Hum. Immunol. 2005, 66, 395–402. [Google Scholar] [CrossRef]
- Akilesh, S.; Petkova, S.; Sproule, T.; Shaffer, D.; Christianson, G.; Roopenian, D. The MHC class I-like Fc receptor promotes humorally mediated autoimmune disease. J. Clin. Investig. 2004, 113, 1328. [Google Scholar]
- Boletis, J.N.; Ioannidis, J.P.; A Boki, K.; Moutsopoulos, H.M. Intravenous immunoglobulin compared with cyclophosphamide for proliferative lupus nephritis. Lancet 1999, 354, 569–570. [Google Scholar] [CrossRef]
- Wenderfer, S.E.; Thacker, T. Intravenous Immunoglobulin in the Management of Lupus Nephritis. Autoimmune Dis. 2012, 2012, 589359. [Google Scholar] [CrossRef] [Green Version]
- Ruiz-Irastorza, G.; Espinosa, G.; Frutos, M.; Jiménez-Alonso, J.; Praga, M.; Pallarés, L.; Riverag, F.; Marhuendah, Á.R.; Segarrai, A.; Queredaj, C. Diagnosis and treatment of lupus nephritis: Consensus document from the systemic autoimmune disease group (GEAS) of the Spanish Society of Internal Medicine (SEMI) and the Spanish Society of Nephrology (S.E.N.). Nefrologia 2012, 32 (Suppl. S1), 1–45. [Google Scholar]
- Bayry, S.; Lacroix-Desmazes, S.; Deligant, L.; Mouthon, B.; Weill, M.D. Kazatchkine IVIG abrogates dendritic cell differentiation induced by interferon-α present in serum from patients with SLE. Arthritis Rheum. 2003, 48, 3497. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, J.; A Zeuner, R.; Euler, H.H.; Löffler, H. High dose intravenous immunoglobulins in systemic lupus erythematosus: Clinical and serological results of a pilot study. J. Rheumatol. 1996, 23, 71–75. [Google Scholar] [PubMed]
- Karin, N. Induction of protective therapy for autoimmune diseases by targeted DNA vaccines encoding proinflammatory cytokines and chemokine. Curr. Opin. Mol. Ther. 2004, 6, 27. [Google Scholar] [PubMed]
- Molica, S.; Musto, P.; Chiurazzi, F.; Specchia, G.; Brugiatelli, M.; Cicoira, L.; Levato, D.; Nobile, F.; Carotenuto, M.; Liso, V.; et al. Prophylaxis against infections with low-dose intravenous immunoglobulins (IVIG) in chronic lymphocytic leukemia. Results of a crossover study. Haematologica 1996, 81, 121–126. [Google Scholar] [PubMed]
- Levy, Y.; Sherer, Y.; Ahmed, A.; Langevitz, P.; George, J.; Fabbrizzi, F.; Terryberry, J.; Meissner, M.; Lorber, M.; Peter, J.B.; et al. A study of 20 SLE patients with intravenous immunoglobulin clinical and serologic response. Lupus 1999, 8, 705–712. [Google Scholar] [CrossRef]
- Hundt, M.; Manger, K.; Dorner, T.; Grimbacher, B.; Kalden, P.; Rascu, A.; Weber, D.; Burmester, G.; Peter, H.; Kalden, J.; et al. Treatment of acute exacerbation of systemic lupus erythematosus with high-dose intravenous immunoglobulin. Rheumatology 2000, 39, 1301. [Google Scholar] [CrossRef] [Green Version]
- Cohen, M.; Li, E. Limited effects of intravenous IgG in treating systemic lupus erythematosus–associated thrombocytopenia. Arthritis Rheum 1991, 34, 787. [Google Scholar] [CrossRef]
- Goodfield, M.; Davison, K.; Bowden, K. IVIG for therapy-resistant cutaneous lupus erythematosus (LE). J. Dermatol. Treat. 2004, 15, 46. [Google Scholar] [CrossRef]
- Engel, G.; van Vollenhoven, R.F. Treatment of Severe CNS Lupus with Intravenous Immunoglobulin. JCR J. Clin. Rheumatol. 1999, 5, 228–232. [Google Scholar] [CrossRef] [PubMed]
- de Jesús Batún Garrido, J.A.; García, U.G.A.; Núñez, É.H. Neurolupus and pregnancy: An ethical and therapeutic dilemma in a second level hospital. Rev. Colomb. Reumatol. 2016, 23, 223–226. [Google Scholar]
- Elsone, L.; Panicker, J.; Mutch, K.; Boggild, M.; Appleton, R.; Jacob, A. Role of intravenous immunoglobulin in the treatment of acute relapses of neuromyelitis optica: Experience in 10 patients. Mult. Scler. J. 2013, 20, 501–504. [Google Scholar] [CrossRef] [PubMed]
- Pranzatelli, M.R.; McGee, N.R.; Wang, Z.Y.; Brajesh, K. Characteristics and pharmacodynamics of severe neuroinflammation in a child with neurolupus. Agrawal. Neurol. Neuroimmunol. Neuroinflamm. 2017, 4, e316. [Google Scholar] [CrossRef] [Green Version]
- Tattevin, P.; Tchamgoué, S.; Belem, A.; Bénézit, F.; Pronier, C.; Revest, M. Aseptic meningitis. Rev. Neurol. 2019, 175, 475–480. [Google Scholar] [CrossRef] [PubMed]
- Orbach, H.; Tishler, M.; Shoenfeld, Y. Intravenous immunoglobulin and the kidney—A two-edged sword. Semin. Arthritis Rheum. 2004, 34, 593–601. [Google Scholar] [CrossRef]
- Tenti, S.; Cheleschi, S.; Guidelli, G.M.; Galeazzi, M.; Fioravanti, A. Intravenous immunoglobulins and antiphospholipid syndrome: How, when and why? A review of the literature. Autoimmun. Rev. 2016, 15, 226–235. [Google Scholar] [CrossRef]
- Sciascia, S.; Giachino, O.; Roccatello, D. Prevention of thrombosis relapse in anti-phospholipid syndrome patients refractory to conventional therapy using intravenous immunoglobulin. Clin. Exp. Rheumatol. 2012, 30, 409–413. [Google Scholar]
- Erkan, D.; Aguiar, C.L.; Andrade, D.; Cohen, H.; Cuadrado, M.J.; Danowski, A.; Levy, R.A.; Ortel, T.L.; Rahman, A.; Salmon, J.E.; et al. 14th International Congress on Anti-phospholipid Antibodies: Task force report on anti-phospholipid syndrome treatment trends. Autoimmun. Rev. 2014, 13, 685–696. [Google Scholar] [CrossRef]
- Rymarz, A.; Niemczyk, S. The complex treatment including rituximab in the Management of Catastrophic Antiphospholid Syndrome with renal involvement. BMC Nephrol. 2018, 19, 132. [Google Scholar] [CrossRef] [Green Version]
- James, T.E.; Martin, L.J.; Warkentin, T.E.; Crowther, M.A. Catastrophic antiphospholipid syndrome refractory to high-dose intravenous immunoglobulin responsive to therapeutic plasma exchange. Platelets 2020, 32, 828–831. [Google Scholar] [CrossRef] [PubMed]
- Gomes, J.P.F.; Santos, L.; Shoenfeld, Y. Intravenous immunoglobulin (IVIG) in the vanguard therapy of Systemic Sclerosis. Clin. Immunol. 2018, 199, 25–28. [Google Scholar] [CrossRef]
- Cantarini, L.; Rigante, D.; Vitale, A.; Napodano, S.; Sakkas, L.I.; Bogdanos, D.P.; Shoenfeld, Y. Intravenous immunoglobulins (IVIG) in systemic sclerosis: A challenging yet promising future. Immunol. Res. 2014, 61, 326–337. [Google Scholar] [CrossRef] [PubMed]
- Levy, Y.; Sherer, Y.; Langevitz, P.; Lorber, M.; Rotman, P.; Fabrizzi, F.; Shoenfeld, Y. Skin score decrease in systemic sclerosis patients treated with intravenous immunoglobulin—A preliminary report. Clin. Rheumatol. 2000, 19, 207–211. [Google Scholar] [CrossRef] [PubMed]
- Nacci, F.; Righi, A.; Conforti, M.L.; Miniati, I.; Fiori, G.; Martinovic, D.; Melchiorre, D.; Sapir, T.; Blank, M.; Shoenfeld, Y.; et al. Intravenous immunoglobulins improve the function and ameliorate joint involvement in systemic sclerosis: A pilot study. Ann. Rheum. Dis. 2007, 66, 977–979. [Google Scholar] [CrossRef] [Green Version]
- Poelman, C.L.; Hummers, L.K.; Wigley, F.M.; Anderson, C.; Boin, F.; Shah, A.A. Intravenous Immunoglobulin May Be an Effective Therapy for Refractory, Active Diffuse Cutaneous Systemic Sclerosis. J. Rheumatol. 2014, 42, 236–242. [Google Scholar] [CrossRef] [Green Version]
- Takehara, K.; Ihn, H.; Sato, S. A randomized, double-blind, placebo-controlled trial: Intravenous immunoglobulin treatment in patients with diffuse cutaneous systemic sclerosis. Ann. Rheum. Dis. 2013, 31 (Suppl. S76), 151–156. [Google Scholar]
- Blank, M.; Levy, Y.; Amital, H.; Shoenfeld, Y.; Pines, M.; Genina, O. The role of intravenous immunoglobulin therapy in mediating skin fibrosis in high skin mice. Arthritis Rheum. 2002, 46, 1689–1690. [Google Scholar] [CrossRef]
- Sanges, S.; Rivière, S.; Mekinian, A.; Martin, T.; Le Quellec, A.; Chatelus, E.; Lescoat, A.; Jego, P.; Cazalets, C.; Quéméneur, T.; et al. Launay Intravenous immunoglobulins in systemic sclerosis: Data from a French nationwide cohort of 46 patients and review of the literature. Autoimmun. Rev. 2017, 16, 377–384. [Google Scholar] [CrossRef]
- Kumar, S.; Singh, J.; Kedika, R.; Mendoza, F.; Jimenez, S.; Blomain, E.S.; Dimarino, A.J.; Cohen, S.; Rattan, S. Role of muscarinic-3 receptor antibody in systemic sclerosis: Correlation with disease duration and effects of IVIG. Am. J. Physiol. Liver Physiol. 2016, 310, G1052–G1060. [Google Scholar] [CrossRef] [PubMed]
- Sherer, Y.; Levy, Y.; Langevitz, P.; Rauova, L.; Fabrizzi, F.; Shoenfeld, Y. Adverse effects of intravenous immunoglobulin therapy in 56 patients with autoimmune diseases. Pharmacology 2001, 62, 133–137. [Google Scholar] [CrossRef] [PubMed]
- Orbach, H.; Katz, U.; Sherer, Y.; Shoenfeld, Y. Intravenous immunoglobulin: Adverse effects and safe administration. Clin. Rev. Allergy Immunol. 2005, 29, 173–184. [Google Scholar] [CrossRef] [PubMed]
- Katz, U.; Achiron, A.; Sherer, Y.; Shoenfeld, Y. Safety of intravenous immunoglobulin (IVIG) therapy. Autoimmun. Rev. 2007, 6, 257–259. [Google Scholar] [CrossRef]
- Sharma, D.; Singh, S. Kawasaki disease—A common childhood vasculitis. Indian J. Rheumatol. 2015, 10, S78–S83. [Google Scholar] [CrossRef]
- Taubert, K.A.; Rowley, A.H.; Shulman, S.T. Nationwide survey of Kawasaki disease and acute rheumatic fever. J. Pediatr. 1991, 119, 279–282. [Google Scholar] [CrossRef]
- Newburger, J.W.; Takahashi, M.; Gerber, M.A.; Gewitz, M.H.; Tani, Y.; Burns, J.C.; Shulman, S.T.; Bolger, F.; Ferrieri, P.; Baltimore, R.S.; et al. Diagnosis, treatment, and long-term management of Kawasaki disease: A statement for health professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Pediatrics 2004, 114, 1708–1733. [Google Scholar] [CrossRef] [Green Version]
- Yan, F.; Zhang, H.; Xiong, R.; Cheng, X.; Chen, Y.; Zhang, F. Effect of Early Intravenous Immunoglobulin Therapy in Kawasaki Disease: A Systematic Review and Meta-Analysis. Front. Pediatr. 2020, 8, 593435. [Google Scholar] [CrossRef]
- McCrindle, B.W.; Rowley, A.H.; Newburger, J.W.; Burns, J.C.; Bolger, A.F.; Gewitz, M.; Baker, A.L.; Jackson, M.A.; Takahashi, M.; Shah, P.B.; et al. Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease: A Scientific Statement for Health Professionals from the American Heart Association. Circulation 2017, 135, e927–e999. [Google Scholar] [CrossRef]
- Suzuki, T.; Michihata, N.; Yoshikawa, T.; Hata, T.; Matsui, H.; Fushimi, K.; Yasunaga, H. High-dose versus low-dose intravenous immunoglobulin for treatment of children with Kawasaki disease weighing 25 kg or more. Eur. J. Pediatr. 2020, 179, 1901–1907. [Google Scholar] [CrossRef]
- Jayne, D.; Chapel, H.; Adu, D.; Misbah, S.; O’Donoghue, D.; Scott, D.; Lockwood, C. Intravenous immunoglobulin for ANCA-associated systemic vasculitis with persistent disease activity. Qjm: Int. J. Med. 2000, 93, 433–439. [Google Scholar] [CrossRef] [Green Version]
- Fortin, P.M.; Tejani, A.M.; Bassett, K.; Musini, V. Intravenous immunoglobulin as adjuvant therapy for Wegener’s granulomatosis. Cochrane Database Syst. Rev. 2013, 31, CD007057. [Google Scholar] [CrossRef] [PubMed]
- Muso, E.; Ito-Ihara, T.; Ono, T.; Imai, E.; Yamagata, K.; Akamatsu, A.; Suzuki, K. Intravenous immunoglobulin (IVIg) therapy in MPO-ANCA related polyangiitis with rapidly progressive glomerulonephritis in Japan. Jpn. J. Infect. Dis. 2004, 57, S17–S18. [Google Scholar]
- Chung, S.A.; Langford, C.A.; Maz, M.; Abril, A.; Gorelik, M.; Guyatt, G.; Archer, A.M.; Conn, D.L.; Full, K.A.; Grayson, P.C.; et al. 2021 American College of Rheumatology/Vasculitis Foundation Guideline for the Management of Antineutrophil Cytoplasmic Antibody–Associated Vasculitis. Arthritis Rheumatol. 2021, 73, 1366–1383. [Google Scholar] [CrossRef] [PubMed]
- Crickx, E.; Machelart, I.; Lazaro, E.; Kahn, J.E.; Cohen-Aubart, F.; Martin, T.; Mania, A.; Hatron, P.-Y.; Hayem, G.; Blanchard-Delaunay, C.; et al. Intravenous immunoglobulin as an immunomodulating agent in antineutrophil cytoplasmic antibody–associated vasculitides: A French nationwide study of ninety-two patients. Arthritis Rheumatol. 2016, 68, 702–712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pasha, S.F.; Lunsford, T.N.; Lennon, V.A. Autoimmune Gastrointestinal Dysmotility Treated Successfully With Pyridostigmine. Gastroenterology 2006, 131, 1592–1596. [Google Scholar] [CrossRef] [PubMed]
- Dhamija, R.; Tan, K.M.; Pittock, S.J.; Foxx–Orenstein, A.; Benarroch, E.; Lennon, V.A. Serologic Profiles Aiding the Diagnosis of Autoimmune Gastrointestinal Dysmotility. Clin. Gastroenterol. Hepatol. 2008, 6, 988–992. [Google Scholar] [CrossRef] [Green Version]
- Flanagan, E.P.; Saito, Y.A.; Lennon, V.A.; McKeon, A.; Fealey, R.D.; Szarka, L.A.; Murray, J.A.; Foxx-Orenstein, A.E.; Fox, J.C.; Pittock, S.J. Immunotherapy trial as diagnostic test in evaluating patients with presumed autoimmune gastrointestinal dysmotility. Neurogastroenterol. Motil. 2014, 26, 1285–1297. [Google Scholar] [CrossRef] [Green Version]
- Schofield, J.R.; Chemali, K.R. Intravenous Immunoglobulin Therapy in Refractory Autoimmune Dysautonomias: A Retrospective Analysis of 38 Patients. Am. J. Ther. 2019, 26, e570–e582. [Google Scholar] [CrossRef]
- Kawanishi, K.; Moribata, K.; Kato, J.; Murata, K.; Fukatsu, K.; Tamaki, H.; Itou, D.; Wada, Y.; Ichinose, M. [A case report of chronic intestinal pseudo-obstruction with autoimmune autonomic ganglionopathy suspected from seropositive results for anti-ganglionic acetylcholine receptor antibody]. Nihon Shokakibyo Gakkai Zasshi 2015, 112, 62–69. [Google Scholar]
- Montalvo, M.; Nallapaneni, P.; Hassan, S.; Nurko, S.; Pittock, S.J.; Khlevner, J. Autoimmune gastrointestinal dysmotility following SARS-CoV-2 infection successfully treated with intravenous immunoglobulin. Neurogastroenterol. Motil. 2022, 34, e14314. [Google Scholar] [CrossRef] [PubMed]
- Morales-Ruiz, V.; Juárez-Vaquera, V.H.; Rosetti-Sciutto, M.; Sánchez-Muñoz, F.; Adalid-Peralta, L. Efficacy of intravenous immunoglobulin in autoimmune neurological diseases. Literature systematic review and meta-analysis. Autoimmun. Rev. 2021, 21, 103019. [Google Scholar] [CrossRef]
- Leonhard, S.E.; Mandarakas, M.R.; Gondim, F.A.A.; Bateman, K.; Ferreira, M.L.B.; Cornblath, D.R.; Van Doorn, P.A.; Dourado, M.E.; Hughes, R.A.C.; Islam, B.; et al. Diagnosis and management of Guillain–Barré syndrome in ten steps. Nat. Rev. Neurol. 2019, 15, 671–683. [Google Scholar] [CrossRef] [PubMed]
- Dalakas, M.C. Intravenous Immunoglobulin in Autoimmune Neuromuscular Diseases. JAMA 2004, 291, 2367–2375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hughes, R.A.C.; Hadden, R.D.M.; Gregson, N.A.; Smith, K.J. Pathogenesis of Guillain–Barré syndrome. J. Neuroimmunol. 1999, 100, 74–97. [Google Scholar] [CrossRef] [PubMed]
- van der Meché, F.; Schmitz, P. A Randomized Trial Comparing Intravenous Immune Globulin and Plasma Exchange in Guillain–Barré Syndrome. N. Engl. J. Med. 1992, 326, 1123–1129. [Google Scholar] [CrossRef]
- Raphael, J.; Chevret, S.; Harboun, M.; M-Ce Jars-Guincestre for the French Guillain-Barré Syndrome Cooperative Group. Intravenous immune globulins in patients with Guillain-Barré syndrome and contraindications to plasma exchange: 3 days versus 6 days. J. Neurol. Neurosurg. Psychiatry 2001, 71, 235–238. [Google Scholar] [CrossRef] [Green Version]
- Gajdos, P.; Chevret, S.; Clair, B.; Tranchant, C.; Chastang, C. Clinical trial of plasma exchange and high-dose intravenous immunoglobulin in myasthenia gravis. Ann. Neurol. 1997, 41, 789–796. [Google Scholar] [CrossRef]
- Bain, P.G.; Motomura, M.; Newsom-Davis, J.; Misbah, S.A.; Chapel, H.M.; Lee, M.L.; Vincent, A.; Lang, B. Effects of intravenous immunoglobulin on muscle weakness and calcium-channel autoantibodies in the Lambert-Eaton myasthenic syndrome. Neurology 1996, 47, 678–683. [Google Scholar] [CrossRef] [PubMed]
- Seeliger, T.; Prenzler, N.K.; Gingele, S.; Seeliger, B.; Körner, S.; Thiele, T.; Bönig, L.; Sühs, K.-W.; Witte, T.; Stangel, M.; et al. Neuro-Sjögren: Peripheral Neuropathy With Limb Weakness in Sjögren’s Syndrome. Front. Immunol. 2019, 10, 1600. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, J.H.O.; Enk, A.H. High-Dose Intravenous Immunoglobulin in Skin Autoimmune Disease. Front. Immunol. 2019, 10, 1090. [Google Scholar] [CrossRef]
- Gao, Y.; Jin, H. Efficacy and safety of intravenous immunoglobulin for treating refractory livedoid vasculopathy: A systematic review. Ther. Adv. Chronic Dis. 2022, 13, 20406223221097331. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Sung, N.; Gilman-Sachs, A.; Kwak-Kim, J. T Helper (Th) Cell Profiles in Pregnancy and Recurrent Pregnancy Losses: Th1/Th2/Th9/Th17/Th22/Tfh Cells. Front. Immunol. 2020, 11, 2025. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, M.; Ghaebi, M.; Abdolmohammadi-Vahid, S.; Abbaspour-Aghdam, S.; Hamdi, K.; Abdollahi-Fard, S.; Danaii, S.; Mosapour, P.; Koushaeian, L.; Dolati, S.; et al. NK cell frequency and cytotoxicity in correlation to pregnancy outcome and response to IVIG therapy among women with recurrent pregnancy loss. J. Cell. Physiol. 2018, 234, 9428–9437. [Google Scholar] [CrossRef] [PubMed]
- Jafarpour, R.; Pashangzadeh, S.; Mehdizadeh, S.; Bayatipoor, H.; Shojaei, Z.; Motallebnezhad, M. Functional significance of lymphocytes in pregnancy and lymphocyte immunotherapy in infertility: A comprehensive review and update. Int. Immunopharmacol. 2020, 87, 106776. [Google Scholar] [CrossRef]
- Kolanska, K.; Alijotas-Reig, J.; Cohen, J.; Cheloufi, M.; Selleret, L.; D’Argent, E.; Kayem, G.; Valverde, E.E.; Fain, O.; Bornes, M.; et al. Endometriosis with infertility: A comprehensive review on the role of immune deregulation and immunomodulation therapy. Am. J. Reprod. Immunol. 2020, 85, e13384. [Google Scholar] [CrossRef]
- Parhizkar, F.; Motavalli-Khiavi, R.; Aghebati-Maleki, L.; Parhizkar, Z.; Pourakbari, R.; Kafil, H.S.; Danaii, S.; Yousefi, M. The Impact of New Immunological Therapeutic Strategies on Recurrent Miscarriage and Recurrent Implantation Failure. Immunol. Lett. 2021, 236, 20–30. [Google Scholar] [CrossRef]
- Ermakov, E.A.; Nevinsky, G.A.; Buneva, V.N. Immunoglobulins with Non-Canonical Functions in Inflammatory and Autoimmune Disease States. Int. J. Mol. Sci. 2020, 21, 5392. [Google Scholar] [CrossRef]
- Ahmadi, M.; Abdolmohammadi-vahid, S.; Ghaebi, M.; Aghebati-Maleki, L.; Afkham, A.; Danaii, S.; Abdollahi-Fard, S.; Heidari, L.; Jadidi-Niaragh, F.; Younesi, V.; et al. Effect of Intravenous immunoglobulin on Th1 and Th2 lymphocytes and improvement of pregnancy outcome in recurrent pregnancy loss (RPL). Biomed. Pharmacother. 2017, 92, 1095–1102. [Google Scholar] [CrossRef]
- Jerzak, M.G.; Gorski, A.; Rechberger, T. Intravenous Immunoglobulin Therapy Influences T cell Adhesion to Extracellular Matrix in Women with a History of Recurrent Spontaneous Abortions. Am. J. Reprod. Immunol. 2000, 44, 336–341. [Google Scholar] [CrossRef]
- Tha-In, T.; Metselaar, H.J.; Tilanus, H.W.; Groothuismink, Z.M.; Kuipers, E.J.; de Man, R.A.; Kwekkeboom, J. Intravenous immunoglobulins suppress T-cell priming by modulating the bidirectional interaction between dendritic cells and natural killer cells. Blood 2007, 110, 3253–3262. [Google Scholar] [CrossRef] [PubMed]
- Jacobi, C.; Claus, M.; Wildemann, B.; Wingert, S.; Korporal, M.; Römisch, J.; Meuer, S.; Watzl, C.; Giese, T. Exposure of NK cells to intravenous immunoglobulin induces IFN gamma release and degranulation but inhibits their cytotoxic activity. Clin. Immunol. 2009, 133, 393–401. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.J.; Lee, S.K.; Kim, J.Y.; Na, B.J.; Hur, S.E.; Lee, M.; Kwak-Kim, J. Intravenous Immunoglobulin G Modulates Peripheral Blood Th17 and Foxp3+ Regulatory T Cells in Pregnant Women with Recurrent Pregnancy Loss. Am. J. Reprod. Immunol. 2014, 71, 441–450. [Google Scholar] [CrossRef]
- Li, J.; Chen, Y.; Liu, C.; Hu, Y.; Li, L. Intravenous Immunoglobulin Treatment for Repeated IVF/ICSI Failure and Unexplained Infertility: A Systematic Review and a Meta-Analysis. Am. J. Reprod. Immunol. 2013, 70, 434–447. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, M.; Aghdam, S.A.; Nouri, M.; Babaloo, Z.; Farzadi, L.; Ghasemzadeh, A.; Hamdi, K.; Movassaghpour, A.; Jadidi-Niaragh, F.; Afkham, A.; et al. Yousefi, Intravenous immunoglobulin (IVIG) treatment modulates peripheral blood Th17 and regulatory T cells in recurrent miscarriage patients: Non randomized, open-label clinical trial. Immunol. Lett. 2017, 192, 12–19. [Google Scholar] [CrossRef]
- Abdolmohammadi-Vahid, S.; Pashazadeh, F.; Pourmoghaddam, Z.; Aghebati-Maleki, L.; Abdollahi-Fard, S.; Yousefi, M. The effectiveness of IVIG therapy in pregnancy and live birth rate of women with recurrent implantation failure (RIF): A systematic review and meta-analysis. J. Reprod. Immunol. 2019, 134–135, 28–33. [Google Scholar] [CrossRef]
- Heilmann, L.; Schorsch, M.; Hahn, T. SHORT COMMUNICATION: CD3− CD56+ CD16+ Natural Killer Cells and Improvement of Pregnancy Outcome in IVF/ICSI Failure After Additional IVIG-Treatment. Am. J. Reprod. Immunol. 2010, 63, 263–265. [Google Scholar] [CrossRef]
- Moraru, M.; Carbone, J.; Alecsandru, D.; Castillo-Rama, M.; García-Segovia, A.; Gil, J.; Alonso, B.; Aguarón, A.; Ramos-Medina, R.; de María, J.M.; et al. Intravenous Immunoglobulin Treatment Increased Live Birth Rate in a Spanish Cohort of Women with Recurrent Reproductive Failure and Expanded CD56+ Cells. Am. J. Reprod. Immunol. 2012, 68, 75–84. [Google Scholar] [CrossRef]
- Nyborg, K.M.; Kolte, A.M.; Larsen, E.C.; Christiansen, O.B. Immunomodulatory treatment with intravenous immunoglobulin and prednisone in patients with recurrent miscarriage and implantation failure after in vitro fertilization/intracytoplasmic sperm injection. Fertil. Steril. 2014, 102, 1650–1655.e1. [Google Scholar] [CrossRef]
- Winger, E.E.; Reed, J.L.; Ashoush, S.; Ahuja, S.; El-Toukhy, T.; Taranissi, M. ORIGINAL ARTICLE: Treatment with Adalimumab (Humira®) and Intravenous Immunoglobulin Improves Pregnancy Rates in Women Undergoing IVF*. Am. J. Reprod. Immunol. 2008, 61, 113–120. [Google Scholar] [CrossRef]
- Winger, E.E.; Reed, J.L. ORIGINAL ARTICLE: Treatment with Tumor Necrosis Factor Inhibitors and Intravenous Immunoglobulin Improves Live Birth Rates in Women with Recurrent Spontaneous Abortion. Am. J. Reprod. Immunol. 2008, 60, 8–16. [Google Scholar] [CrossRef]
- Chambers, C.D.; Johnson, D.L. Emerging data on the use of anti-tumor necrosis factor-alpha medications in pregnancy. Birth Defects Res. Part A Clin. Mol. Teratol. 2012, 94, 607–611. [Google Scholar] [CrossRef]
- Hyde, K.J.; Schust, D.J. Genetic Considerations in Recurrent Pregnancy Loss. Cold Spring Harb. Perspect. Med. 2015, 5, a023119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carp, H.J.; Asherson, R.A.; Shoenfeld, Y. Intravenous immunoglobulin in pregnancies complicated by the anti-phospholipid syndrome: What is its role? J. Clin. Rheumatol. 2001, 7, 291–294. [Google Scholar] [CrossRef] [PubMed]
- Alijotas-Reig, J. Treatment of refractory obstetric anti-phospholipid syndrome: The state of the art and new trends in the therapeutic management. Lupus 2013, 22, 6–17. [Google Scholar] [CrossRef]
- Valensise, H.; Vaquero, E.; De Carolis, C.; Stipa, E.; Perricone, R.; Arduini, D.; Romanini, C. Normal fetal growth in women with anti-phospholipid syndrome treated with high-dose intravenous immunoglobulin (IVIG). Prenat. Diagn. 1995, 15, 509–517. [Google Scholar] [CrossRef] [PubMed]
- Clark, A.L.; Branch, D.W.; Silver, R.M.; Harris, E.N.; Pierangeli, S.; Spinnato, J.A. Pregnancy complicated by the anti-phospholipid syndrome: Outcomes with intravenous immunoglobulin therapy. Obstet. Gynecol. 1999, 93, 437–441. [Google Scholar]
- Watanabe, N.; Yamaguchi, K.; Motomura, K.; Hisano, M.; Sago, H.; Murashima, A. Combination therapy with anticoagulants, corticosteroids and intravenous immunoglobulin for women with severe obstetric anti-phospholipid syndrome. Clin. Exp. Rheumatol. 2014, 32, 299–300. [Google Scholar]
- Marzusch, K.; Dietl, J.; Klein, R.; Hornung, D.; Neuer, A.; Berg, P.A. Recurrent first trimester spontaneous abortion associated with anti-phospholipid antibodies: A pilot study of treatment with intravenous immunoglobulin. Acta Obstet. Gynecol. Scand 1996, 75, 922–926. [Google Scholar] [CrossRef]
- Sher, G.; Matzner, W.; Feinman, M.; Maassarani, G.; Zouves, C.; Chong, P.; Ching, W. The selective use of heparin/aspirin therapy, alone or in combination with intravenous immunoglobulin G, in the management of anti-phospholipid antibody-positive women undergoing in vitro fertilization. Am. J. Reprod. Immunol. 1998, 40, 74–82. [Google Scholar] [CrossRef]
- Branch, D.W.; Peaceman, A.M.; Druzin, M.; Silver, R.K.; El-Sayed, Y.; Silver, R.M.; Peaceman, A.M.; Spinnato, J.; Harger, J. A multicenter, placebo-controlled pilot study of intravenous immune globulin treatment of anti-phospholipid syndrome during pregnancy. Am. J. Obstet. Gynecol. 2000, 182, 122–127. [Google Scholar] [CrossRef]
- Vaquero, E.; Valensise, H.; Menghini, S.; Di Pierro, G.; Romanini, C.; Lazzarin, N.; Cesa, F. Pregnancy outcome in recurrent spontaneous abortion associated with anti-phospholipid antibodies: A comparative study of intravenous immunoglobulin versus prednisone plus low-dose aspirin. Am. J. Reprod. Immunol. 2001, 45, 174–179. [Google Scholar] [CrossRef]
- Diejomaoh, M.F.; Al-Azemi, M.M.; Bandar, A.; Egbase, P.E.; Jirous, J.; Al-Othman, S.; Bukhadour, N.; Al-Sweih, N. A favorable outcome of pregnancies in women with primary and secondary recurrent pregnancy loss associated with anti-phospholipid syndrome. Arch. Gynecol. Obstet. 2002, 266, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Triolo, G.; Ferrante, A.; Ciccia, F.; Accardo-Palumbo, A.; Perino, A.; Castelli, A.; Giarratano, A.; Licata, G. Randomized study of subcutaneous low molecular weight heparin plus aspirin versus intravenous immunoglobulin in the treatment of recurrent fetal loss associated with anti-phospholipid antibodies. Arthritis Rheum. 2003, 48, 728–731. [Google Scholar] [CrossRef]
- Jeremić, K.; Pervulov, M.; Gojnić, M.; Dukanac, J.; Ljubić, A.; Stojnić, J. Comparison of two therapeutic protocols in patients with anti-phospholipid antibodies and recurrent miscarriages. Vojnosanit. Pregl. 2005, 62, 435–439. [Google Scholar] [CrossRef] [PubMed]
- Dendrinos, S.; Sakkas, E.; Makrakis, E. Low-molecular-weight heparin versus intravenous immunoglobulin for recurrent abortion associated with anti-phospholipid antibody syndrome. Int. J. Gynaecol. Obstet. 2009, 104, 223–225. [Google Scholar] [CrossRef]
- Heilmann, L.; Schorch, M.; Hahn, T.; Adasz, G.; Schilberz, K.; Adiguzel, C.; Fareed, J. Pregnancy outcome in women with anti-phospholipid antibodies: Report on a retrospective study. Semin. Thromb. Hemost. 2008, 34, 794–802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, J.; Xiong, J.; Zhu, F.; He, L. Effect of prednisone, aspirin, low molecular weight heparin and intravenous immunoglobulin on the outcome of pregnancy in women with anti-phospholipid syndrome. Exp. Ther. Med. 2013, 5, 287–291. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Autoimmune Condition | Type of Study | Patients | Dosage Regimen | Results | Ref. |
|---|---|---|---|---|---|
| Idiopathic inflammatory myopathies | Double-blind, placebo-controlled | 15 biopsy-proved, treatment-resistant dermatomyositis | 2 g per kilogram of body weight or placebo per month for 3 months | Significant improvement in scores of muscle strength and neuromuscular symptoms | [37] |
| Retrospective | Steroid-refractory esophageal involvement related to polymyositis and dermatomyositis | 2 mg/kg monthly | 82.6% of patients exhibited resolution of esophageal impairment | [38] | |
| Open | 35 patients with chronic, refractory polymyositis | 1 mg/kg/day for 2 consecutive days per month | Significant clinical improvement in 71.4% and biochemical response | [40] | |
| Single-center long-term follow-up | 91 patients with polymyositis and dermatomyositis | 1 g/kg (5 g/h) on two consecutive days each month for six months | Better survival in IVIG/subcutaneous Ig treated patients | [42] | |
| Prospective, double-blind, randomized, placebo-controlled phase III study-ProDERM Study | Patients with dermatomiositis | 2 g/kg of IVIg or placebo, every 4 weeks until week 16 | Improvement in total improvement score, time to improvement, proportions of patients with deteriorations | [44] | |
| randomized, placebo-controlled, ProDERM | 95 patients with dermatomiositis | 2 g/kg of IVIg or placebo, every 4 weeks until week 16 | 79% had a total improvement score of at least 20; at least moderate improvement and major improvement | [45] | |
| Systemic lupus eryhtmeatodes | Systematic review and meta-analysis (3 controlled and 10 observational studies) | Heterogenous group of SLE patients, subjects with lupus nephritis, hematological and cutaneous involvement | 400 mg/kg/d over 5 days | Response rate of 30.9%; reduction of SLE disease score | [4] |
| Pilot | 12 patients with mildly to moderately active SLE | 30 g of sulfonated IVIG preparation on each of Days 1–4 and 21–24 | Systemic Lupus Activity Measure dropped significantly, lasted 5–12 months, decline in anti-dsDNA antibodies | [57] | |
| Observational | 20 SLE patients | 2 g/kg IVIg monthly, in a 5-d schedule | Beneficial clinical response, more responsive to treatment-arthritis, fever, thrombocytopenia, and neuropsychiatric lupus | [60] | |
| Anti-phospholipid syndrome | Review of the literature | Patients with obstetric APS | 0.4–1 g/kg/month | Prevent recurrent thrombosis in APS patients refractory to conventional anticoagulant treatment | [70] |
| Systemic sclerosis | Preliminary report | 3 patients with systemic sclerosis | 2 g/kg at six courses | large decrease in the skin score, no changes in anti-PM-Scl antibodies | [77] |
| Pilot | 7 women with systemic sclerosis | 2 g/kg body weight during 4 days/month for six consecutive courses | Decrease in joint pain and tenderness, hand function improved together with quality of life, the skin score reduced | [78] | |
| Retrospective | 46 patients with systemic sclerosis | at least 1 IVIG infusion at a dosage > 1 g/kg/cycle | Significant improvement of muscle pain, muscle weakness, joint pain, CK and CRP levels | [82] | |
| Kawasaki disease | Systematic review and meta-analysis | 14 studies with 70,396 patients | High dose | Reduced risk of coronary artery lesions; Early treatment with IVIG can lead to an increased risk of IVIG unresponsiveness | [90] |
| ANCA-associated vasculitides | Randomized, controlled | 34 patients with Wegener granulomatosis | 2 g/kg | Fall in disease activity score | [94] |
| French Nationwide | 92 patients with granulomatosis with polyangiitis (Wegener’s), eosinophilic granulomatosis with polyangiitis (Churg–Strauss), or microscopic polyangiitis | 1 mg/kg/d for 2 days, 0.5 mg/kg/d for 4 days, other | Remission in 56% of patients at 6th month | [97] | |
| Autoimmune dysautonomias | Retrospective | 38 patients with disabling, refractory autoimmune dysautonomias, incl. postural tachycardia syndrome and gastrointestinal dysmotility | 1 mg/kg monthly for 3 months | Improved composite autonomic symptom scale and functional/ability score in 83.5% of patients | [101] |
| Autoimmune neurological diseases | Meta-analysis | 23 reports with 344 patients with Guillain–Barre, autoimmune encephalitis, etc. | 1–2 g/kg at an average | Beneficial effect of IVIG administration on patient improvement over placebo and identical effects to plasmapheresis | [104] |
| Guillain–Barré syndrome | Multi-center, randomized | 150 patients with Guillain–Barré syndrome | 5 doses of 0.4 g per kilogram per day | Improved strength, significantly fewer complications and less need for artificial ventilation | [108] |
| Single-center trial | 36 patients with Guillain–Barré syndrome with severe hemostasis, unstable hemodynamics, or uncontrolled sepsis | 0.4 g/kg/day IVIg for 3 or 6 days | Improvement in walking without assistance and needed for ventilation | [109] | |
| Myasthenia gravis | Randomized clinical trial | 87 patients with myasthenia gravis | 0.4 mg/kg daily | Improvement of myasthenic muscular score | [110] |
| Livedoid vasculopathy | Systematic review | 17 articles-80 patients with livedoid vasculopathy | 1–2.1 g/kg body weight every 4 weeks | Resolution of pain, skin ulcerations, and neurological symptoms, and reducing the dependence on glucocorticoids and immunosuppressive agents | [114] |
| Sjögren syndrome with severe neuropathy and limb weakness | Cross-sectional | 184 patients with Neuro-Sjögren | N/A | Improvement in motor function or stabilization of status quo; temporary improvement of all symptoms, but long-term clinical benefit could not be achieved as symptoms relapsed | [112] |
| Dermatological autoimmune diseases | Retrospective | Pemphigus vulgaris, pemphigus foliaceous, bullous pemphigoid, mucous membrane pemphigoid, epidermolysis bullosa acquisita, and cutaneous lupus erythematosus | 2 g per kg body weight distributed over 2–5 days every 4 weeks | Achieved diseases control, reduction of immunosuppressive therapy | [113] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Velikova, T.; Sekulovski, M.; Bogdanova, S.; Vasilev, G.; Peshevska-Sekulovska, M.; Miteva, D.; Georgiev, T. Intravenous Immunoglobulins as Immunomodulators in Autoimmune Diseases and Reproductive Medicine. Antibodies 2023, 12, 20. https://doi.org/10.3390/antib12010020
Velikova T, Sekulovski M, Bogdanova S, Vasilev G, Peshevska-Sekulovska M, Miteva D, Georgiev T. Intravenous Immunoglobulins as Immunomodulators in Autoimmune Diseases and Reproductive Medicine. Antibodies. 2023; 12(1):20. https://doi.org/10.3390/antib12010020
Chicago/Turabian StyleVelikova, Tsvetelina, Metodija Sekulovski, Simona Bogdanova, Georgi Vasilev, Monika Peshevska-Sekulovska, Dimitrina Miteva, and Tsvetoslav Georgiev. 2023. "Intravenous Immunoglobulins as Immunomodulators in Autoimmune Diseases and Reproductive Medicine" Antibodies 12, no. 1: 20. https://doi.org/10.3390/antib12010020