
Vitamin D Status in Patients with Primary Antiphospholipid Syndrome (PAPS): A Systematic Review and Meta-Analysis

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Guidelines and Protocol
2.2. Eligibility Criteria and Search Strategies
2.3. Study Screening and Selection
2.4. Quality Assessment
2.5. Data Extraction
2.6. Data Analyses
3. Results
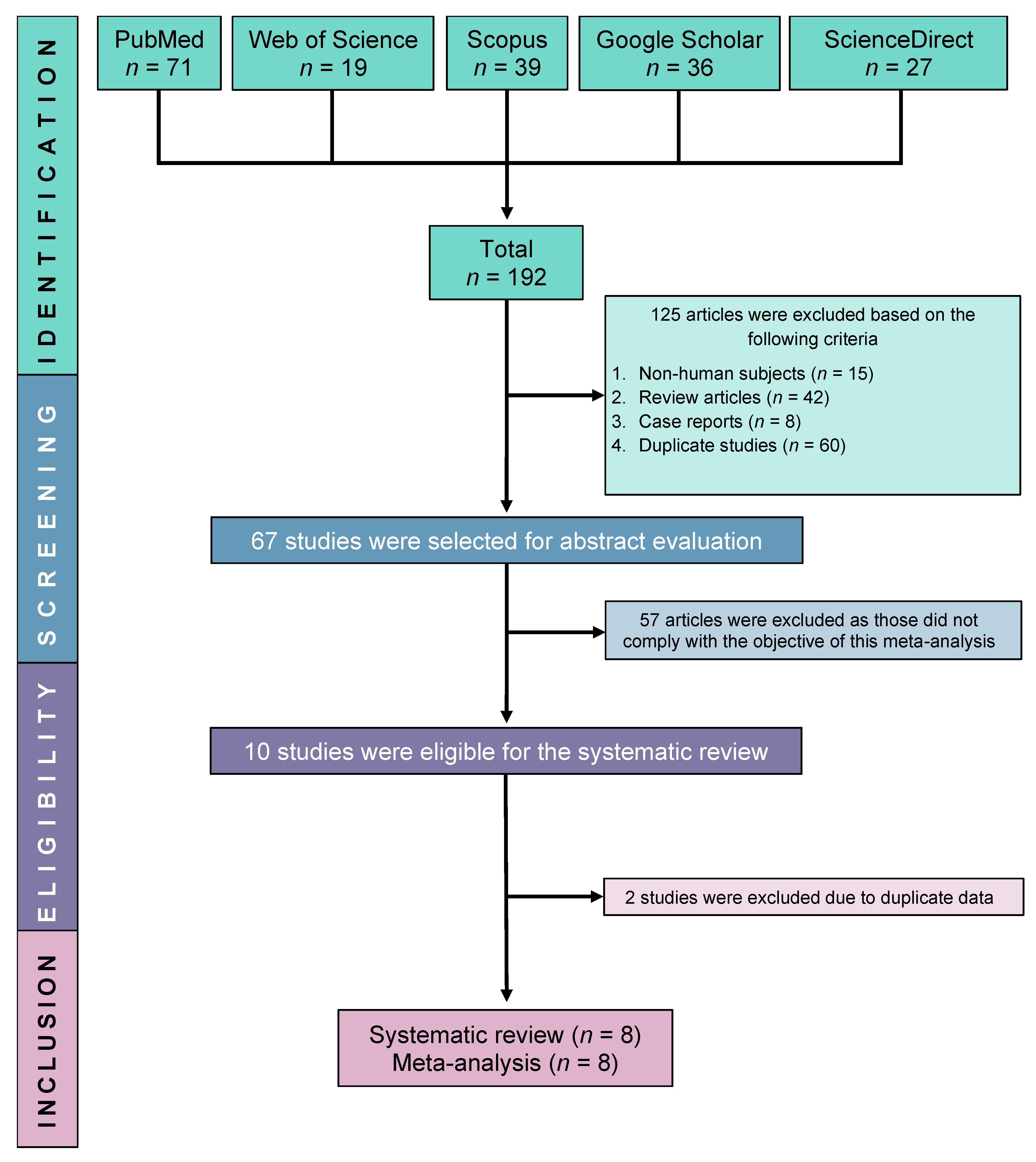
3.1. Study Selection
3.2. Characteristics of Included Studies
3.3. Meta-Analyses
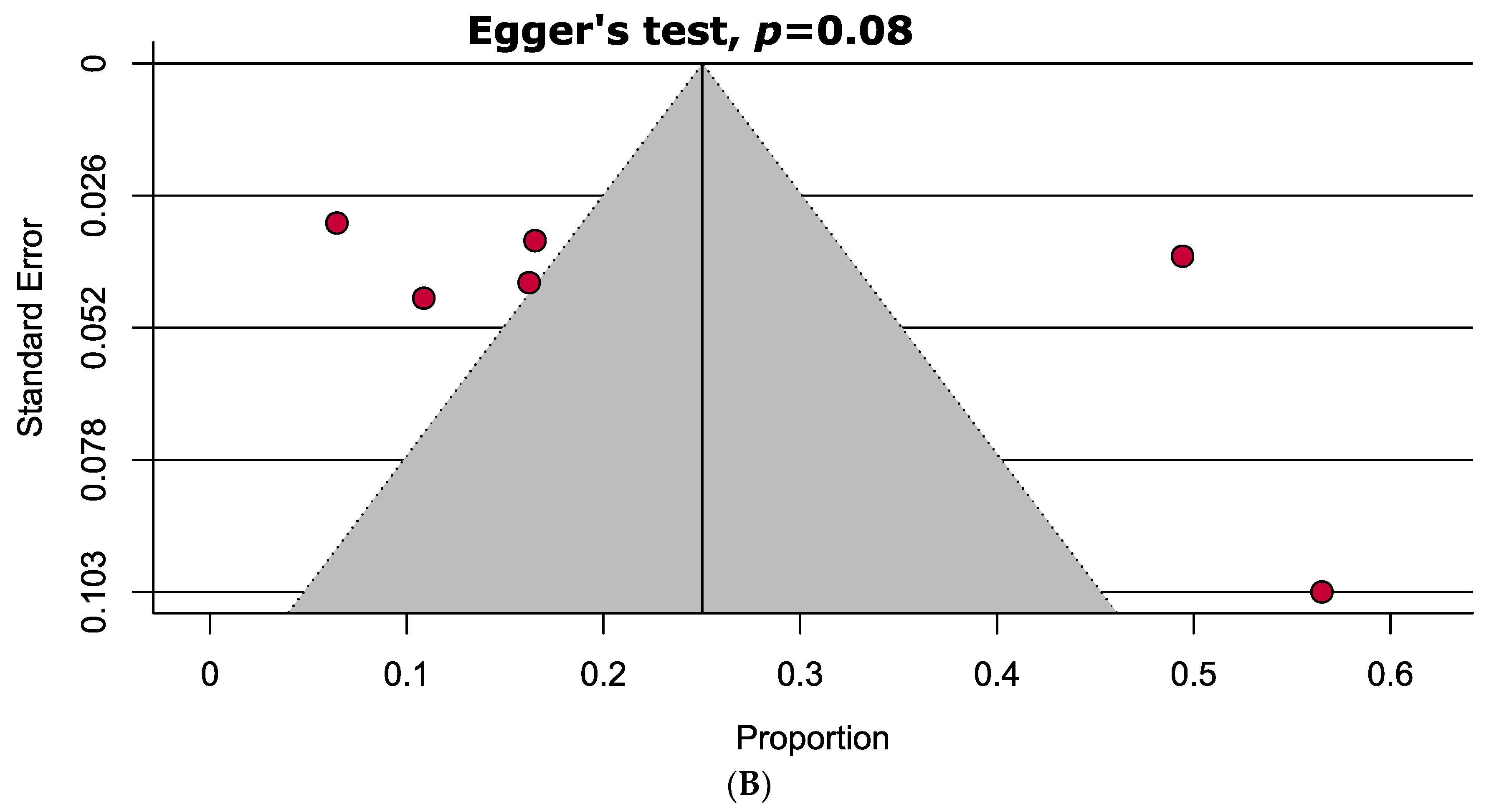
3.4. Quality Assessment and Publication Bias
3.5. Sensitivity Analyses
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barbhaiya, M.; Zuily, S.; Naden, R.; Hendry, A.; Manneville, F.; Amigo, M.C.; Amoura, Z.; Andrade, D.; Andreoli, L.; Artim-Esen, B.; et al. 2023 ACR/EULAR antiphospholipid syndrome classification criteria. Ann. Rheum. Dis. 2023, 82, 1258–1270. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.A.; Alam, F.; Sasongko, T.H.; Gan, S.H. Antiphospholipid Antibody-Mediated Thrombotic Mechanisms in Antiphospholipid Syndrome: Towards Pathophysiology-Based Treatment. Curr. Pharm. Des. 2016, 22, 4451–4469. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.A.; Khandker, S.S.; Alam, F.; Kamal, M.A.; Gan, S.H. Genetic risk factors in thrombotic primary antiphospholipid syndrome: A systematic review with bioinformatic analyses. Autoimmun. Rev. 2018, 17, 226–243. [Google Scholar] [CrossRef] [PubMed]
- Salman-Monte, T.C.; Torrente-Segarra, V.; Vega-Vidal, A.L.; Corzo, P.; Castro-Dominguez, F.; Ojeda, F.; Carbonell-Abelló, J. Bone mineral density and vitamin D status in systemic lupus erythematosus (SLE): A systematic review. Autoimmun. Rev. 2017, 16, 1155–1159. [Google Scholar] [CrossRef] [PubMed]
- Shoenfeld, Y.; Giacomelli, R.; Azrielant, S.; Berardicurti, O.; Reynolds, J.A.; Bruce, I.N. Vitamin D and systemic lupus erythematosus-The hype and the hope. Autoimmun. Rev. 2018, 17, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.A.; Khandker, S.S.; Kotyla, P.J.; Hassan, R. Immunomodulatory Effects of Diet and Nutrients in Systemic Lupus Erythematosus (SLE): A Systematic Review. Front. Immunol. 2020, 11, 1477. [Google Scholar] [CrossRef] [PubMed]
- Brunton, N.E.; Casanegra, A.I.; Houghton, D.E. “No Shoes. No Shirt. No Thrombus.” Could Vitamin D Levels Change the Tune for Patients with Antiphospholipid Syndrome? Hematologist 2023, 20. [Google Scholar] [CrossRef]
- Mohammad, S.; Mishra, A.; Ashraf, M.Z. Emerging Role of Vitamin D and its Associated Molecules in Pathways Related to Pathogenesis of Thrombosis. Biomolecules 2019, 9, 649. [Google Scholar] [CrossRef]
- Andersen, M.K.; Rudiger, I.H.; Vestergaard, A.L.; Palarasah, Y.; Bor, P.; Larsen, A.; Bor, M.V. Vitamin D Deficiency is Associated with Increased Plasminogen Activator Inhibitor 1/Plasminogen Activator Inhibitor 2 Ratio in Pregnancy. Clin. Appl. Thromb. Hemost. 2023, 29, 10760296231201855. [Google Scholar] [CrossRef]
- Aihara, K.; Azuma, H.; Akaike, M.; Ikeda, Y.; Yamashita, M.; Sudo, T.; Hayashi, H.; Yamada, Y.; Endoh, F.; Fujimura, M.; et al. Disruption of nuclear vitamin D receptor gene causes enhanced thrombogenicity in mice. J. Biol. Chem. 2004, 279, 35798–35802. [Google Scholar] [CrossRef]
- Agmon-Levin, N.; Blank, M.; Zandman-Goddard, G.; Orbach, H.; Meroni, P.L.; Tincani, A.; Doria, A.; Cervera, R.; Miesbach, W.; Stojanovich, L.; et al. Vitamin D: An instrumental factor in the anti-phospholipid syndrome by inhibition of tissue factor expression. Ann. Rheum. Dis. 2011, 70, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Jorde, R.; Haug, E.; Figenschau, Y.; Hansen, J.B. Serum levels of vitamin D and haemostatic factors in healthy subjects: The Tromso study. Acta Haematol. 2007, 117, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Mohd, S.; Sharma, S.; Mishra, A.; Ashraf, M.Z. Vitamin D and its relationship with the pathways related to thrombosis and various diseases. In Vitamin D; BoD—Books on Demand: Norderstedt, Germany, 2021. [Google Scholar]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M.; Endocrine, S. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Cutolo, M.; Pizzorni, C.; Sulli, A. Vitamin D endocrine system involvement in autoimmune rheumatic diseases. Autoimmun. Rev. 2011, 11, 84–87. [Google Scholar] [CrossRef] [PubMed]
- Orbach, H.; Zandman-Goddard, G.; Amital, H.; Barak, V.; Szekanecz, Z.; Szucs, G.; Danko, K.; Nagy, E.; Csepany, T.; Carvalho, J.F.; et al. Novel biomarkers in autoimmune diseases: Prolactin, ferritin, vitamin D, and TPA levels in autoimmune diseases. Ann. N. Y. Acad. Sci. 2007, 1109, 385–400. [Google Scholar] [CrossRef] [PubMed]
- Piantoni, S.; Andreoli, L.; Allegri, F.; Meroni, P.; Tincani, A. Low levels of vitamin D are common in primary antiphospholipid syndrome with thrombotic disease. Reumatismo 2012, 65, 307–313. [Google Scholar] [CrossRef]
- Riancho-Zarrabeitia, L.; Cubería, M.; García-Canale, S.; Daroca, G.; García-Unzueta, M.; Hernández, J.; Lόpez-Hoyos, M.; Muñoz, P.; Agudo, M.; Martínez-Taboada, V. Vitamin D: Potential role in antiphospholipid syndrome. Ann. Rheum. Dis. 2017, 76, 1229–1230. [Google Scholar]
- Paupitz, J.; Freire, D.C.J.; Caparbo, V.; Klack, K.; Pereira, R. Primary antiphospholipid syndrome in premenopausal women: Low vitamin D, high fat mass and maintained bone mineral mass. Lupus 2010, 19, 1302–1306. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097-269. [Google Scholar] [CrossRef]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.; Chowdhury, M.I.H.; Sultana, S.; Alam, S.S.; Marzan, M.; Islam, M.A. Prevalence of Antibiotic-Resistant Shigella spp. in Bangladesh: A Systematic Review and Meta-Analysis of 44,519 Samples. Antibiotics 2023, 12, 817. [Google Scholar] [CrossRef] [PubMed]
- Al-Khreisat, M.J.; Ismail, N.H.; Tabnjh, A.; Hussain, F.A.; Mohamed Yusoff, A.A.; Johan, M.F.; Islam, M.A. Worldwide Prevalence of Epstein-Barr Virus in Patients with Burkitt Lymphoma: A Systematic Review and Meta-Analysis. Diagnostics 2023, 13, 2068. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.-T.; Ang, J.-Y.; Islam, M.A.; Chan, H.-K.; Cheah, W.-K.; Gan, S.H. Prevalence of Drug-Related Problems and Complementary and Alternative Medicine Use in Malaysia: A Systematic Review and Meta-Analysis of 37,249 Older Adults. Pharmaceuticals 2021, 14, 187. [Google Scholar] [CrossRef] [PubMed]
- von Hippel, P.T. The heterogeneity statistic I(2) can be biased in small meta-analyses. BMC Med. Res. Methodol. 2015, 15, 35. [Google Scholar] [CrossRef] [PubMed]
- Viechtbauer, W. Conducting meta-analyses in R with the metafor package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef]
- Review Manager (RevMan). [Computer Program]. Version 5.3. Copenhagen: The Nordic Cochrane Centre; The Cochrane Collaboration: London, UK, 2014. [Google Scholar]
- Andreoli, L.; Piantoni, S.; Dall’Ara, F.; Allegri, F.; Meroni, P.; Tincani, A. Vitamin D and antiphospholipid syndrome. Lupus 2012, 21, 736–740. [Google Scholar] [CrossRef]
- Riancho-Zarrabeitia, L.; Cuberia, M.; Munoz, P.; Lopez-Hoyos, M.; Garcia-Canale, S.; Garcia-Unzueta, M.; Hernandez, J.L.; Martinez-Taboada, V.M. Vitamin D and antiphospholipid syndrome: A retrospective cohort study and meta-analysis. Semin. Arthritis Rheum. 2018, 47, 877–882. [Google Scholar] [CrossRef]
- Bećarević, M.; Sarić, M.; Stojanovich, L.; Mirković, D.; Dopsaj, V.; Ignjatović, S. Anti-annexin A5 antibodies and 25-hydroxy-cholecalciferol in female patients with primary antiphospholipid syndrome. Clin. Rheumatol. 2018, 37, 3359–3364. [Google Scholar] [CrossRef]
- Klack, K.; de Carvalho, J.F. High frequency of vitamin D insufficiency in primary antiphospolipid syndrome. Jt. Bone Spine 2010, 5, 489–490. [Google Scholar] [CrossRef]
- Soroka, N.; Talako, T. The Effect of Vitamin D Supplementation on Antiphospholipid Antibodies Level in Patients with Antiphospholipid Syndrome. Ann. Rheum. Dis. 2016, 75, 1048. [Google Scholar] [CrossRef]
- Gualtierotti, R.; Di Giacomo, A.; Raschi, E.; Borghi, M.O.; Meroni, P.L. Vitamin D and anti-phospholipid antibody syndrome: A comprehensive review. Open Rheumatol. J. 2018, 12, 248–260. [Google Scholar] [CrossRef]
- Lin, J.; Liu, J.; Davies, M.L.; Chen, W. Serum vitamin D level and rheumatoid arthritis disease activity: Review and meta-analysis. PLoS ONE 2016, 11, e0146351. [Google Scholar] [CrossRef] [PubMed]
- Cai, G.; Wang, L.; Fan, D.; Xin, L.; Liu, L.; Hu, Y.; Ding, N.; Xu, S.; Xia, G.; Jin, X. Vitamin D in ankylosing spondylitis: Review and meta-analysis. Clin. Chim. Acta 2015, 438, 316–322. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.A.; Khandker, S.S.; Alam, S.S.; Kotyla, P.; Hassan, R. Vitamin D status in patients with systemic lupus erythematosus (SLE): A systematic review and meta-analysis. Autoimmun. Rev. 2019, 18, 102392. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, V.R.L.S.; Domingueti, C.P. Association of vitamin D deficiency and type 1 diabetes mellitus: A systematic review and meta-analysis. Int. J. Diabetes Dev. Ctries. 2018, 38, 280–288. [Google Scholar] [CrossRef]
- Wang, J.; Lv, S.; Chen, G.; Gao, C.; He, J.; Zhong, H.; Xu, Y. Meta-analysis of the association between vitamin D and autoimmune thyroid disease. Nutrients 2015, 7, 2485–2498. [Google Scholar] [CrossRef]
- Martínez-Lapiscina, E.H.; Mahatanan, R.; Lee, C.-H.; Charoenpong, P.; Hong, J.-P. Associations of serum 25 (OH) vitamin D levels with clinical and radiological outcomes in multiple sclerosis, a systematic review and meta-analysis. J. Neurol. Sci. 2020, 411, 116668. [Google Scholar] [CrossRef]
- An, L.; Sun, M.-h.; Chen, F.; Li, J.-r. Vitamin D levels in systemic sclerosis patients: A meta-analysis. Drug Des. Dev. Ther. 2017, 11, 3119–3125. [Google Scholar] [CrossRef]
- Del Pinto, R.; Pietropaoli, D.; Chandar, A.K.; Ferri, C.; Cominelli, F. Association between inflammatory bowel disease and vitamin D deficiency: A systematic review and meta-analysis. Inflamm. Bowel Dis. 2015, 21, 2708–2717. [Google Scholar] [CrossRef]
- Webb, A.R.; Kline, L.; Holick, M.F. Influence of season and latitude on the cutaneous synthesis of vitamin D3: Exposure to winter sunlight in Boston and Edmonton will not promote vitamin D3 synthesis in human skin. J. Clin. Endocrinol. Metab. 1988, 67, 373–378. [Google Scholar] [CrossRef] [PubMed]
- Slater, N.A.; Rager, M.L.; Havrda, D.E.; Harralson, A.F. Genetic Variation in CYP2R1 and GC Genes Associated with Vitamin D Deficiency Status. J. Pharm. Pract. 2017, 30, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Brouwer-Brolsma, E.M.; Vaes, A.M.M.; van der Zwaluw, N.L.; van Wijngaarden, J.P.; Swart, K.M.A.; Ham, A.C.; van Dijk, S.C.; Enneman, A.W.; Sohl, E.; van Schoor, N.M.; et al. Relative importance of summer sun exposure, vitamin D intake, and genes to vitamin D status in Dutch older adults: The B-PROOF study. J. Steroid Biochem. Mol. Biol. 2016, 164, 168–176. [Google Scholar] [CrossRef]
- Thongthai, P.; Chailurkit, L.O.; Chanprasertyothin, S.; Nimitphong, H.; Sritara, P.; Aekplakorn, W.; Ongphiphadhanakul, B. Vitamin D binding protein gene polymorphism as a risk factor for vitamin D deficiency in Thais. Endocr. Pract. 2015, 21, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.J.; Zhang, F.; Richards, J.B.; Kestenbaum, B.; van Meurs, J.B.; Berry, D.; Kiel, D.P.; Streeten, E.A.; Ohlsson, C.; Koller, D.L.; et al. Common genetic determinants of vitamin D insufficiency: A genome-wide association study. Lancet 2010, 376, 180–188. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Carrio, J.; Alperi-Lopez, M.; Naves-Diaz, M.; Dusso, A.; Lopez, P.; Ballina-Garcia, F.J.; Cannata-Andia, J.B.; Suarez, A. Vitamin D Receptor Polymorphism and DHCR7 Contribute to the Abnormal Interplay between Vitamin D and Lipid Profile in Rheumatoid Arthritis. Sci. Rep. 2019, 9, 2546. [Google Scholar] [CrossRef] [PubMed]
- Alathari, B.E.; Cruvinel, N.T.; da Silva, N.R.; Chandrabose, M.; Lovegrove, J.A.; Horst, M.A.; Vimaleswaran, K.S. Impact of Genetic Risk Score and Dietary Protein Intake on Vitamin D Status in Young Adults from Brazil. Nutrients 2022, 14, 1015. [Google Scholar] [CrossRef] [PubMed]
- Arnson, Y.; Amital, H.; Shoenfeld, Y. Vitamin D and autoimmunity: New aetiological and therapeutic considerations. Ann. Rheum. Dis. 2007, 66, 1137–1142. [Google Scholar] [CrossRef]
- Crescioli, C.; Minisola, S. Vitamin D: Autoimmunity and gender. Curr. Med. Chem. 2017, 24, 2671–2686. [Google Scholar] [CrossRef]
- Yamamoto, E.; Jørgensen, T.N. Immunological effects of vitamin D and their relations to autoimmunity. J. Autoimmun. 2019, 100, 7–16. [Google Scholar] [CrossRef]
- Korkmaz, U.T.K.; Ersoy, S.; Yuksel, A.; Celik, H.; Ucaroglu, E.R.; Velioglu, Y.; Cetinkaya, A.; Demir, D.; Esen, U.; Erdem, K. Association between vitamin D levels and lower-extremity deep vein thrombosis: A case-control study. Sao Paulo Med. J. 2021, 139, 279–284. [Google Scholar] [CrossRef]
- Khademvatani, K.; Seyyed-Mohammadzad, M.H.; Akbari, M.; Rezaei, Y.; Eskandari, R.; Rostamzadeh, A. The relationship between vitamin D status and idiopathic lower-extremity deep vein thrombosis. Int. J. Gen. Med. 2014, 7, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Koyama, T.; Hirosawa, S. Anticoagulant effects of synthetic retinoids and activated vitamin D3. Semin. Thromb. Hemost. 1998, 24, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Ohsawa, M.; Koyama, T.; Yamamoto, K.; Hirosawa, S.; Kamei, S.; Kamiyama, R. 1α, 25-dihydroxyvitamin D3 and its potent synthetic analogs downregulate tissue factor and upregulate thrombomodulin expression in monocytic cells, counteracting the effects of tumor necrosis factor and oxidized LDL. Circulation 2000, 102, 2867–2872. [Google Scholar] [CrossRef] [PubMed]
- Wu-Wong, J.R.; Nakane, M.; Ma, J. Vitamin D analogs modulate the expression of plasminogen activator inhibitor-1, thrombospondin-1 and thrombomodulin in human aortic smooth muscle cells. J. Vasc. Res. 2007, 44, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Stach, K.; Kälsch, A.-I.; Nguyen, X.D.; Elmas, E.; Kralev, S.; Lang, S.; Weiss, C.; Borggrefe, M.; Kälsch, T. 1α, 25-dihydroxyvitamin D3 attenuates platelet activation and the expression of VCAM-1 and MT1-MMP in human endothelial cells. Cardiology 2011, 118, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Norman, P.; Powell, J. Vitamin D and cardiovascular disease. Circ. Res. 2014, 114, 379–393. [Google Scholar] [CrossRef]
- Al Anouti, F.; Thomas, J.; Abdel-Wareth, L.; Rajah, J.; Grant, W.B.; Haq, A. Vitamin D deficiency and sun avoidance among university students at Abu Dhabi, United Arab Emirates. Dermatoendocrinology 2011, 3, 235–239. [Google Scholar] [CrossRef]
- Kashi, Z.; sima Saeedian, F.; Akha, O.; fatemeh Emadi, S.; Zakeri, H. Vitamin D deficiency prevalence in summer compared to winter in a city with high humidity and a sultry climate. Endokrynol. Pol. 2011, 62, 249–251. [Google Scholar]
- Singh, S.K.; Prakash, V.; Tiwari, S.; Daliparthy, D.P.; Singh, S.; Jain, P. Summer and winter prevalence of vitamin D deficiency of young resident doctors in North India. Nutr. Diet. 2011, 68, 280–284. [Google Scholar] [CrossRef]
- Chaiamnuay, S.; Chailurkit, L.-o.; Narongroeknawin, P.; Asavatanabodee, P.; Laohajaroensombat, S.; Chaiamnuay, P. Current daily glucocorticoid use and serum creatinine levels are associated with lower 25 (OH) vitamin D levels in Thai patients with systemic lupus erythematosus. J. Clin. Rheumatol. 2013, 19, 121–125. [Google Scholar] [CrossRef]
- Huisman, A.M.; White, K.P.; Algra, A.; Harth, M.; Vieth, R.; Jacobs, J.; Bijlsma, J.; Bell, D.A. Vitamin D levels in women with systemic lupus erythematosus and fibromyalgia. J. Rheumatol. 2001, 28, 2535–2539. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study ID [References] | Country (Latitude) | Study Population | Age of the APS (Mean ± SD/Median [IQR]) (Years) | Disease Duration [Mean ± SD or Median (IQR)] (Months) | APS Classification Criteria | Vitamin D Measurement Method | Cut-Off for Vitamin D Deficiency, Insufficiency (ng/mL) | Summary Outcomes |
|---|---|---|---|---|---|---|---|---|
| Riancho-Zarrabeitia 2018 [30] | Spain (40.46° N) | Case: 74 Control: 215 | 46.1 ± 15.3 | NR | 2006 Sydney | Chemiluminescent immunoassay | <10, 10–30 | Frequency of vitamin D deficiency was found to be higher in APS patients compared to healthy controls. However, no significant difference of vitamin D insufficiency was observed between the healthy control and APS group. |
| Bećarević 2018 [31] | Serbia (44.81° N) | Case: 62 | 46.9 ± 12.2 | 77.9 ± 73.2 | 2006 Sydney | Chemiluminescent immunoassay | <20, 20–30 | Vitamin D levels were significantly lower in female APS patients. |
| Soroka 2016 [33] | Belarus (53.90° N) | Case: 16 | 34 ± 6.4 | NR | 2006 Sydney | ELISA | <15, 20–30 | Significant vitamin D deficiency was observed in APS patients. |
| Andreoli 2012 [29] | Italy (41.87° N) | Case: 115 Control: 128 | 46.0 [18.0-79.0] | NR | 2006 Sydney | Chemiluminescent immunoassay | <10, 10–30 | Significantly reduced levels of vitamin D were found in APS patients and thrombotic APS patients showed significantly lower levels of vitamin D than obstetric APS patients. |
| Agmon-levin 2011 [11] | Italy (41.87° N), Israel (31.04° N), Serbia (44.01° N), Germany (51.16° N), Spain (40.46° N) | Case: 113 Control: 141 | 48.5 ± 15 | NR | 2006 Sydney | Chemiluminescent immunoassay | <15, 15–30 | In comparison to controls, APS patients had considerably reduced serum vitamin D levels, which were linked to thrombosis. |
| Paupitz 2010 [20] | Brazil (23.55° S) | Case: 23 Control: 23 | 33.0 ± 8.2 | 43.3 ± 35.6 | 1999 Sapporo | Chemiluminescent immunoassay | <20, 20–30 | Lower levels of vitamin D were found in APS patients than controls. |
| Klack 2010 [32] | Brazil (23.55° S) | Case: 46 | 40.2 ± 11.9 | 75.0 ± 56.9 | 1999 Sapporo | Radioimmunoassay | <10, 10–30 | Patients with APS had a very high frequency of vitamin D insufficiency. |
| Orbach 2007 [17] | Italy (41.87° N), Israel (31.04° N), Hungary (47.16° N) | Case: 160 Control: 141 | NR | NR | 1999 Sapporo | Radioimmunoassay | <20, 20–30 | 25-Hydroxy vitamin D levels were relatively lower in APS patients than controls. |
| Strategies of Sensitivity Analyses | Results | Difference of Pooled Results Compared to the Main Result | Number of Studies Analysed | Total Number of Subjects | Heterogeneity | |
|---|---|---|---|---|---|---|
| I2 | p-Value | |||||
| Estimating prevalence of vitamin D deficiency | ||||||
| Excluding small studies (<100) | 32.9 [0.7, 65.2] | 2.2% higher | 2 | 291 | 98% | <0.01 |
| Excluding low- and medium-quality studies | 24.9 [10.0, 39.7] | 22.7% lower | 6 | 496 | 95% | <0.01 |
| Using a fixed-effects model | 21.9 [18.8, 25.1] | 32.0% lower | 7 | 512 | 96% | <0.01 |
| Estimating odds ratio of vitamin D deficiency | ||||||
| Excluding small studies (<100) | 3.08 [1.89, 5.02] | 0.23 lower | 3 | Case: 365 Control: 484 | 25% | <0.00001 |
| Excluding low- and medium-quality studies | 3.31 [2.09, 5.24] | No change | 4 | Case: 388 Control: 507 | 21% | <0.00001 |
| Using a fixed-effects model | 3.03 [2.10, 4.37] | 0.28 lower | 4 | Case: 388 Control: 507 | 60% | <0.00001 |
| Estimating mean difference of vitamin D level | ||||||
| Excluding small studies (<100) | −5.47 [−10.13, −0.82] | 0.28 lower | 3 | Case: 347 Control: 497 | 91% | <0.00001 |
| Excluding low- and medium-quality studies | −3.62 [−5.43, −1.81] | 2.13 lower | 3 | Case: 210 Control: 379 | 0% | <0.00001 |
| Using a fixed-effects model | −6.59 [−7.88, −5.30] | 0.84 higher | 4 | Case: 370 Control: 520 | 87% | <0.00001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Islam, M.A.; Ahmed, S.; Sultana, S.; Alam, S.S.; Hossan, T.; Gouda, W.; Alsaqabi, F.; Hassan, R.; Kotyla, P.J. Vitamin D Status in Patients with Primary Antiphospholipid Syndrome (PAPS): A Systematic Review and Meta-Analysis. Antibodies 2024, 13, 22. https://doi.org/10.3390/antib13010022
Islam MA, Ahmed S, Sultana S, Alam SS, Hossan T, Gouda W, Alsaqabi F, Hassan R, Kotyla PJ. Vitamin D Status in Patients with Primary Antiphospholipid Syndrome (PAPS): A Systematic Review and Meta-Analysis. Antibodies. 2024; 13(1):22. https://doi.org/10.3390/antib13010022
Chicago/Turabian StyleIslam, Md Asiful, Saleh Ahmed, Shabiha Sultana, Sayeda Sadia Alam, Tareq Hossan, Wesam Gouda, Faisal Alsaqabi, Rosline Hassan, and Przemysław J. Kotyla. 2024. "Vitamin D Status in Patients with Primary Antiphospholipid Syndrome (PAPS): A Systematic Review and Meta-Analysis" Antibodies 13, no. 1: 22. https://doi.org/10.3390/antib13010022