Glomerular Diseases Associated with Malignancies: Histopathological Pattern and Association with Circulating Autoantibodies

 ,
, 


Abstract
1. Introduction
2. Materials and Methods
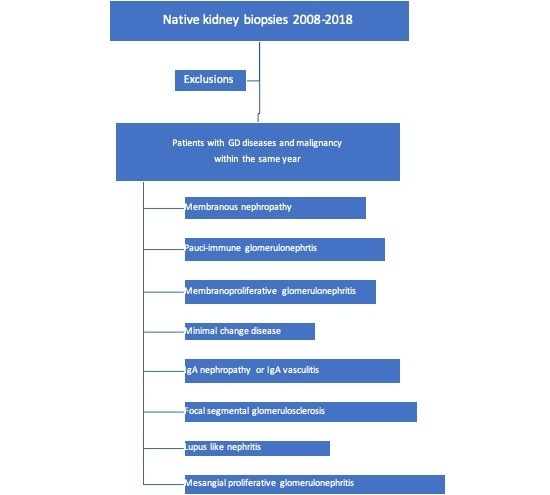
2.1. Participants and Inclusion Criteria
2.2. Renal Histopathology Methods
3. Results
3.1. Description of Patient Population
3.2. Characteristics Related to GD
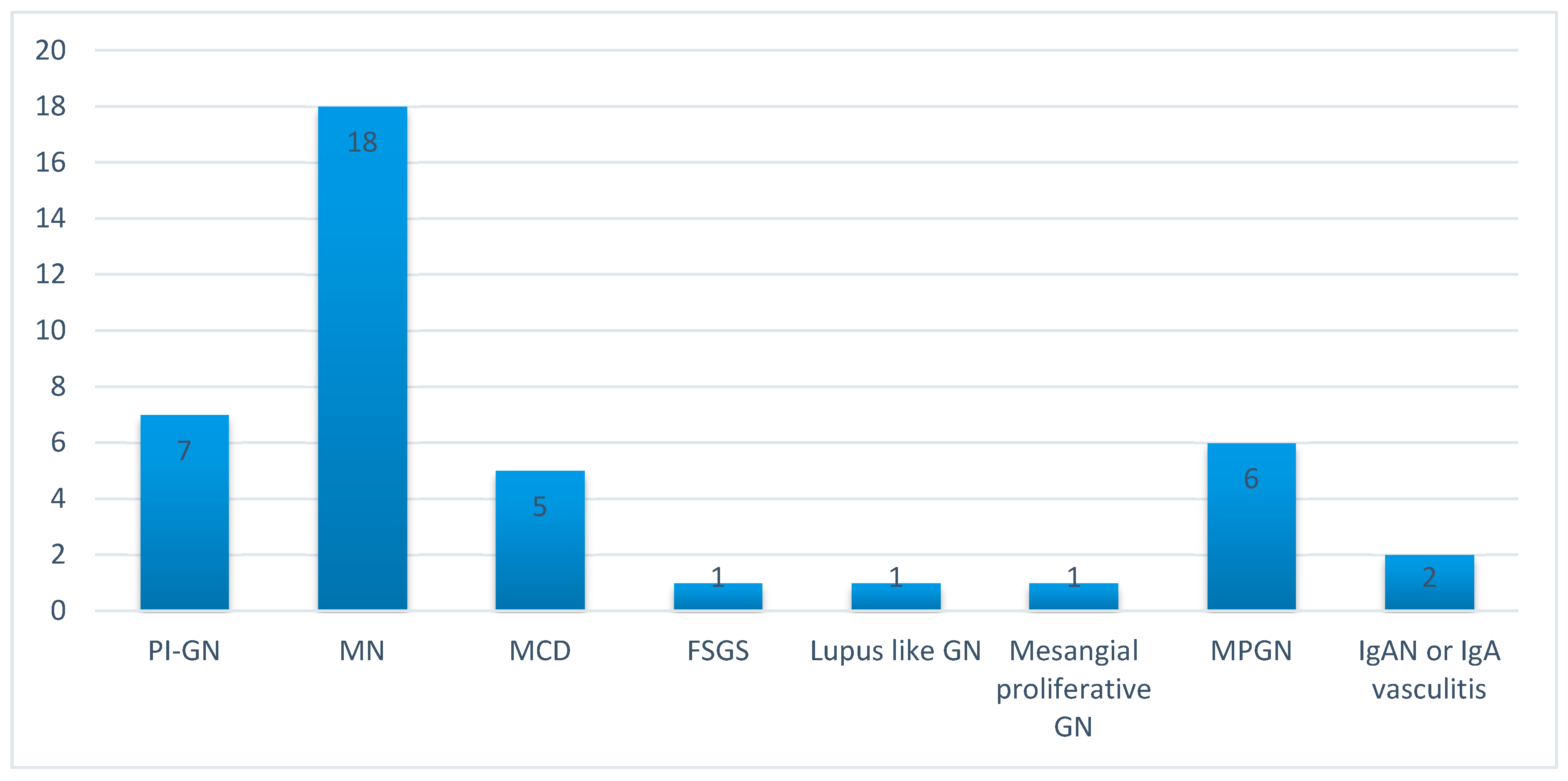
3.3. Histopathology Findings
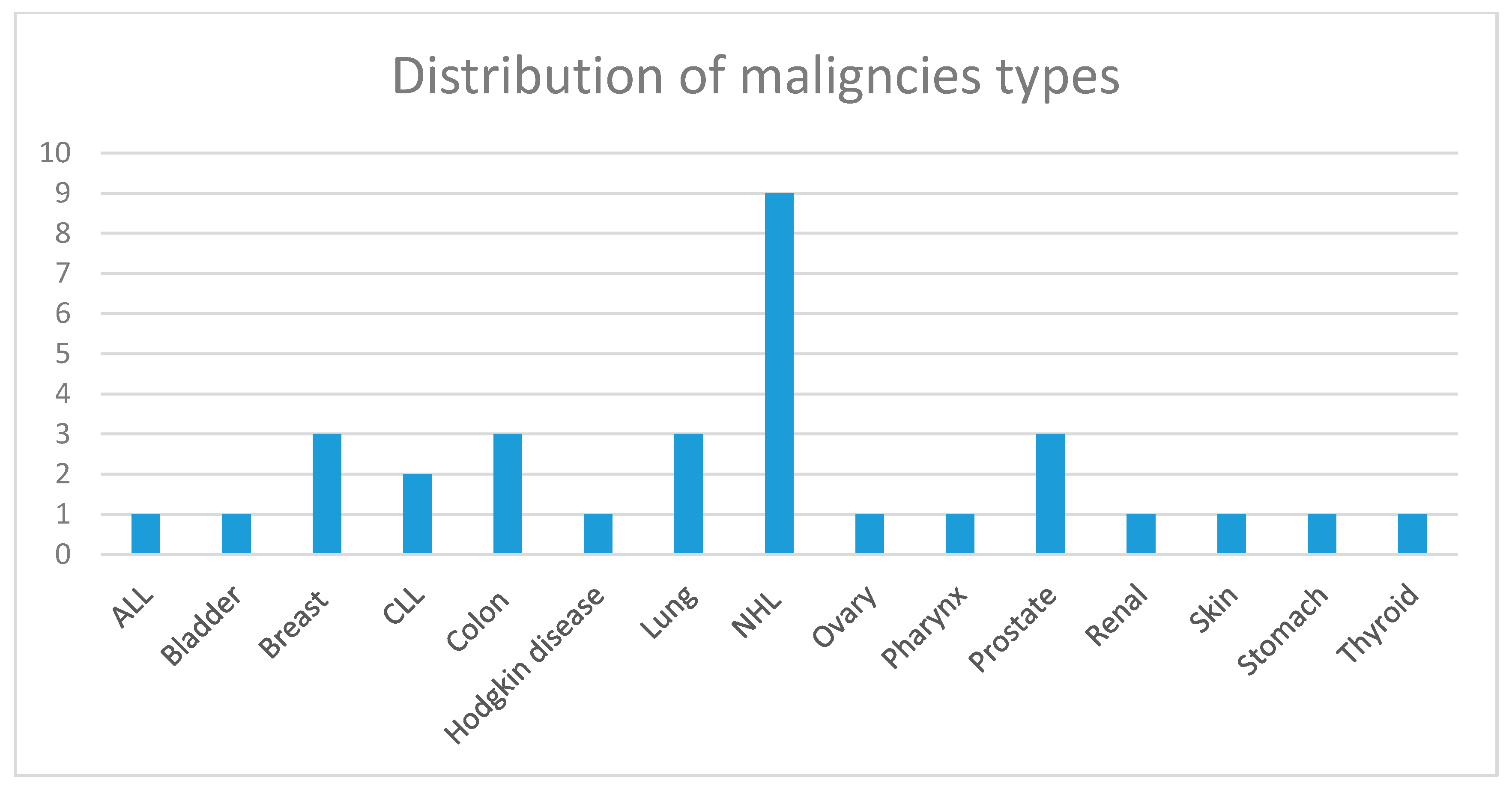
3.4. Characteristics Related to the Malignancy
3.5. Patient and Renal Survival
4. Discussion
5. Statement of Ethics
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| GD | glomerular disease |
| GDAM | glomerular disease associated with malignancy |
| PLA2R | phospholipase A2 receptor |
| ANCA | antineutrophil cytoplasmic autoantibodies |
| MPO | myeloperoxidase |
| PR3 | proteinase 3 |
| ESKD | end stage kidney disease |
| ANA | anti-nuclear autoantibodies |
| PI-GN | pauci-immune glomerulonephritis |
| RPGN | rapidly progressive glomerulonephritis |
| GFR | glomerular filtration rate |
| MPGN | membranoproliferative glomerulonephritis |
| MN | membranous nephropathy |
| IgAN | IgA nephropathy |
| MCD | minimal change disease |
| GN | glomerulonephritis |
| FSGS | focal segmental glomerulosclerosis |
References
- Abudayyeh, A.; Lahoti, A.; Salahudeen, A.K. Onconephrology: The need and the emergence of a subspecialty in nephrology. Kidney Int. 2014, 85, 1002–1004. [Google Scholar] [CrossRef] [PubMed]
- Lien, Y.-H.H.; Lai, L.-W. Pathogenesis, diagnosis and management of paraneoplastic glomerulonephritis. Nat. Rev. Nephrol. 2010, 7, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Beck, L.H. Membranous Nephropathy and Malignancy. Semin. Nephrol. 2010, 30, 635–644. [Google Scholar] [CrossRef] [PubMed]
- Lefaucheur, C.; Stengel, B.; Nochy, D.; Martel, P.; Hill, G.; Jacquot, C.; Rossert, J. for the GN-PROGRESS Study Group Membranous nephropathy and cancer: Epidemiologic evidence and determinants of high-risk cancer association. Kidney Int. 2006, 70, 1510–1517. [Google Scholar] [CrossRef] [PubMed]
- Pani, A.; Porta, C.; Cosmai, L.; Melis, P.; Floris, M.; Piras, D.; Gallieni, M.; Rosner, M.; Ponticelli, C. Glomerular diseases and cancer: Evaluation of underlying malignancy. J. Nephrol. 2015, 29, 143–152. [Google Scholar] [CrossRef]
- Levey, A.; Coresh, J.; Greene, T.; Marsh, J.; Stevens, L.A.; Kusek, J.W.; Van Lente, F.; for Chronic Kidney Disease Epidemiology Collaboration. Expressing the Modification of Diet in Renal Disease Study Equation for Estimating Glomerular Filtration Rate with Standardized Serum Creatinine Values. Clin. Chem. 2007, 53, 766–772. [Google Scholar] [CrossRef]
- Zech, P.; Colon, S.; Pointet, P.; Deteix, P.; Labeeuw, M.; Leitienne, P. The nephrotic syndrome in adults aged over 60: Etiology, evolution and treatment of 76 cases. Clin. Nephrol. 1982, 17, 232–236. [Google Scholar]
- O’Callaghan, C.; Hicks, J.; Doll, H.; Sacks, S.H.; Cameron, J. Characteristics and outcome of membranous nephropathy in older patients. Int. Urol. Nephrol. 2002, 33, 157–165. [Google Scholar] [CrossRef]
- Glassock, R.J. Secondary membranous glomerulonephritis. Nephrol. Dial. Transplant. 1992, 7, 64–71. [Google Scholar]
- Ronco, P.M. Paraneoplastic glomerulopathies: New insights into an old entity. Kidney Int. 1999, 56, 355–377. [Google Scholar] [CrossRef]
- Leeaphorn, N.; Kue-A-Pai, P.; Thamcharoen, N.; Ungprasert, P.; Stokes, M.B.; Knight, E.L. Prevalence of Cancer in Membranous Nephropathy: A Systematic Review and Meta-Analysis of Observational Studies. Am. J. Nephrol. 2014, 40, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Beck, L.H.; Bonegio, R.; Lambeau, G.; Beck, D.M.; Powell, D.W.; Cummins, T.D.; Klein, J.B.; Salant, D.J. M-type phospholipase A2 receptor as target antigen in idiopathic membranous nephropathy. N. Engl. J. Med. 2009, 361, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Biava, C.G.; Gonwa, T.A.; Naughton, J.L.; Hopper, J.J.; Hopper, J. Crescentic Glomerulonephritis Associated with Nonrenal Malignancies. Am. J. Nephrol. 1984, 4, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Tatsis, E.; Reinhold-Keller, E.; Steindorf, K.; Feller, A.C.; Gross, W.L. Wegener’s granulomatosis associated with renal cell carcinoma. Arthritis Rheum. 1999, 4, 751–756. [Google Scholar] [CrossRef]
- Hruby, Z.; Bronowicz, A.; Rabczyński, J.; Kopeć, W.; Szewczyk, Z. A case of severe anti-neutrophil cytoplasmic antibody (ANCA)-positive crescentic glomerulonephritis and asymptomatic gastric cancer. Int. Urol. Nephrol. 1994, 26, 579–586. [Google Scholar] [CrossRef]
- Baschinsky, D.Y.; Baker, P.B.; Niemann, T.H.; Wilmer, W.A. Pauci-immune ANCA-positive crescentic glomerulonephritis associated with metastatic adenocarcinoma of the lung. Am. J. Kidney Dis. 2000, 36, e24.1–e24.7. [Google Scholar] [CrossRef]
- Diez-Porres, L.; Blanco, J.J.R.; Robles-Marhuenda, A.; Gutiérrez-Molina, M.; Gil-Aguado, A.; Vázquez-Rodríguez, J.J. ANCA-associated vasculitis as paraneoplastic syndrome with colon cancer: A case report. Lupus 2005, 14, 632–634. [Google Scholar] [CrossRef]
- Lionaki, S.; Blyth, E.R.; Hogan, S.L.; Hu, Y.; Senior, B.A.; Jennette, C.E.; Nachman, P.H.; Jennette, J.C.; Falk, R.J.; Senior, J.B.A. Classification of antineutrophil cytoplasmic autoantibody vasculitides: The role of antineutrophil cytoplasmic autoantibody specificity for myeloperoxidase or proteinase 3 in disease recognition and prognosis. Arthritis Rheum. 2012, 64, 3452–3462. [Google Scholar] [CrossRef]
- Holder, S.M.T.; Joy, M.S.; Falk, R.J. Cutaneous and systemic manifestations of drug-induced vasculitis. Ann. Pharmacother. 2002, 36, 130–147. [Google Scholar] [CrossRef]
- Lionaki, S.; Hogan, S.L.; Falk, R.J.; Joy, M.S.; Chin, H.; Jennette, C.E.; Nachman, P.H. Association between thyroid disease and its treatment with ANCA small-vessel vasculitis: A case control study. Nephrol. Dial. Transplant. 2007, 22, 3508–3515. [Google Scholar] [CrossRef]
- Hosoya, Y.; Minota, S.; Lefor, A.; Sakuma, K.; Aoki, Y.; Kamimura, T.; Niwa, Y.; Kajii, E.; Kanai, N.; Yasuda, Y. Resolution of anti-neutrophil cytoplasmic antibody-associated vasculitis after resection of gastric cancer. Mod. Rheumatol. 2010, 20, 102–105. [Google Scholar] [CrossRef] [PubMed]
- Küçük, M.; Koklu, H.; Ozkazanc, G.; Erkul, Y.; Koklu, N.O.; Derici, U.; Gonul, I.I. Sixty-Eight-Year-Old Man Presenting with Concurrent Microscopic Polyangiitis and Prostate Cancer. J. Am. Geriatr. Soc. 2015, 63, 1716–1717. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Lim, C.; Mahar, A.; Clark, J.; McGuigan, L.; Felbel, W.; Murali, R. Concurrent involvement of thyroid gland by Wegener’s granulomatosis and papillary thyroid carcinoma. Pathology 2011, 43, 381–383. [Google Scholar] [CrossRef] [PubMed]
- Hommel, C.; Rihova, Z.; Mokaddem, F.; Libotte, B. pANCA-vasculitis associated with rectal adenocarcinoma. Acta Clin. Belg. 2014, 69, 463–466. [Google Scholar] [CrossRef] [PubMed]
- Abe, H.; Momose, S.; Takeuchi, T. Microscopic polyangitis complicating double carcinoma of the stomach and duodenum: Improvement after the resection of these carcinomas. Rheumatol. Int. 2009, 31, 105–108. [Google Scholar] [CrossRef]
- Watz, H.; Hammerl, P.; Matter, C.; Degen, M.; Heimann, F.; Heitmann, H.; Ermert, L.; Wagner, T.O. Bronchioloalveolar carcinoma of the lung associated with a highly positive pANCA-titer and clinical signs of microscopic polyangiitis. Pneumologie 2004, 7, 493–498. [Google Scholar] [CrossRef][Green Version]
- Hamidou, M.; El Kouri, D.; Audrain, M.; Grolleau, J.-Y. Systemic antineutrophil cytoplasmic antibody vasculitis associated with lymphoid neoplasia. Ann. Rheum. Dis. 2001, 60, 293–295. [Google Scholar] [CrossRef]
- Navarro, J.F.; Quereda, C.; Rivera, M.; Navarro, F.J.; Ortuño, J. Anti-neutrophil cytoplasmic antibody-associated paraneoplastic vasculitis. Postgrad. Med. J. 1994, 70, 373–375. [Google Scholar] [CrossRef][Green Version]
- Cambier, J.-F.; Ronco, P. Onco-Nephrology: Glomerular Diseases with Cancer. Clin. J. Am. Soc. Nephrol. 2012, 7, 1701–1712. [Google Scholar] [CrossRef]
- Bear, H.D.; Tang, G.; Rastogi, P.; Geyer, C.E., Jr.; Robidoux, A.; Atkins, J.N.; Baez-Diaz, L.; Brufsky, A.M.; Mehta, R.S.; Fehrenbacher, L.; et al. Bevacizumab added to neoadjuvant chemotherapy for breast cancer. N. Engl. J. Med. 2012, 4, 310–320. [Google Scholar] [CrossRef]
- Brouwer, E.; Huitema, M.G.; Mulder, A.H.; Heeringa, P.; van Goor, H.; Tervaert, J.W.; Weening, J.J.; Kallenberg, C.G. Neutrophil activation in vitro and in vivo in Wegener’sgranulomatosis. Kidney Int. 1994, 45, 1120–1131. [Google Scholar] [CrossRef] [PubMed]
- Xiao, H.; Hu, P.; Falk, R.J.; Jennette, J.C. Overview of the Pathogenesis of ANCA-Associated Vasculitis. Kidney Dis. 2015, 1, 205–215. [Google Scholar] [CrossRef] [PubMed]
- Ewert, B.H.; Jennette, J.C.; Falk, R.J. The Pathogenic Role of Antineutrophil Cytoplasmic Autoantibodies. Am. J. Kidney Dis. 1991, 18, 188–195. [Google Scholar] [CrossRef]
- Neelapu, S.S.; Locke, F.L.; Bartlett, N.L.; Lekakis, L.J.; Miklos, D.B.; Jacobson, C.A.; Braunschweig, I.; Oluwole, O.O.; Siddiqi, T.; Lin, Y.; et al. Axicabtagene Ciloleucel CAR T-Cell Therapy in Refractory Large B-Cell Lymphoma. N. Engl. J. Med. 2017, 377, 2531–2544. [Google Scholar] [CrossRef] [PubMed]
- Mallouk, A.; Pham, P.T.; Pham, P.C. Concurrent FSGS and Hodgkin’s lymphoma: Case report and literature review on the link between nephrotic glomerulopathies and hematological malignancies. Clin. Exp. Nephrol. 2006, 4, 284–289. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Age (Years) | Renal Histopathology | Type of Malignancy | Clinical Presentation of the Glomerular Disease | Ser. Creat. (mg/dL) | 24 h Protein Excretion (mg) | Positive Serological Findings |
|---|---|---|---|---|---|---|---|
| P. 1 | 61 | MPGN | NHL (Malt) | Acute GN | 1.9 | 9905 | ANA |
| P. 2 | 76 | MPGN | NHL (B cell) | Rapidly progressive GN | 4.7 | 6641 | ANA |
| P. 3 | 46 | MPGN | NHL (T cell) | Nephritic syndrome | 1.1 | 2000 | - |
| P. 4 | 52 | MN | NHL (B cell) | Nephrotic syndrome | 1.2 | 3200 | - |
| P. 5 | 43 | MPGN | NHL (Malt) | Nephritic syndrome | 0.98 | 1100 | ANA |
| P. 6 | 62 | IgAN | CLL | Acute GN | 1.4 | 1020 | - |
| P. 7 | 57 | MPGN | NHL (B cell) | Nephritic syndrome | 0.6 | 850 | ANA |
| P. 8 | 59 | MN | ALL | Nephrotic syndrome-AKI | 7.7 | 12,000 | - |
| P. 9 | 79 | MPGN | NHL (T cell) | Acute GN | 1.4 | 299 | ANA |
| P. 10 | 79 | MN | NHL (B cell) | Nephrotic syndrome | 0.9 | 7500 | - |
| P. 11 | 66 | MCD | NHL (B cell) | Nephrotic syndrome | 0.9 | 4200 | - |
| P. 12 | 66 | MN | CLL | Nephrotic syndrome-AKI | 2.8 | 9540 | - |
| P. 13 | 56 | MCD | Hodgkin disease | Nephrotic syndrome-AKI | 1.5 | 16,900 | - |
| Patient | Age (Years) | Renal Histopathology | Type of Malignancy | Clinical Presentation of the Glomerular Disease | Ser. Creatinine (mg/dL) | 24 h Protein Excretion (mg) | Positive Serological Findings |
|---|---|---|---|---|---|---|---|
| P. 1 | 59 | PI-GN | Breast cancer | Rapidly progressive GN | 3.3 | 1200 | - |
| P. 2 | 70 | PI-GN | Prostate cancer | Pulmonary-renal syndrome | 9.6 | 120 | MPO-ANCA |
| P. 3 | 59 | MCD | Ovary cancer | Nephrotic syndrome | 0.8 | 6670 | - |
| P. 4 | 59 | MN | Colon cancer | Nephrotic syndrome | 0.8 | 4000 | - |
| P. 5 | 59 | MN | Lung cancer | Nephrotic syndrome | 1.2 | 4900 | - |
| P. 6 | 71 | PI-GN | Pharynx cancer | Rapidly progressive GN | 6.2 | 1435 | MPO-ANCA |
| P. 7 | 54 | MN | Lung cancer | Nephrotic syndrome | 0.7 | 10,300 | - |
| P. 8 | 44 | MN | Thyroid cancer | Nephrotic syndrome | 0.8 | 3700 | - |
| P. 9 | 82 | MCD | Prostate cancer | Nephrotic syndrome-AKI | 2.8 | 6900 | - |
| P. 10 | 65 | MN | Colon cancer | Nephrotic syndrome | 0.6 | 3200 | - |
| P. 11 | 80 | MN | Colon cancer | Nephrotic syndrome | 0.9 | 7600 | - |
| P.12 | 37 | Lupus-like GN | Kidney cancer | Nephritic syndrome | 0.7 | 4300 | ANA |
| P. 13 | 67 | MN | Breast cancer | Subnephrotic proteinuria | 0.9 | 2200 | - |
| P.14 | 49 | Mesangial proliferative GN | Breast cancer | Glomerular hematuria, proteinuria | 0.8 | 625 | - |
| P.15 | 67 | PI-GN | Bladder cancer | Acute GN | 3.3 | 810 | MPO-ANCA |
| P. 16 | 67 | PI-GN | Prostate cancer | Acute GN | 2.7 | 1200 | MPO-ANCA |
| P. 17 | 68 | PI-GN | Skin cancer | Acute GN | 2.6 | 1030 | MPO-ANCA |
| P. 18 | 70 | FSGS-tip lesion | Colon cancer | Nephrotic syndrome | 1.0 | 8300 | - |
| P. 19 | 82 | PI-GN | Stomach (neuroendocrine) | Rapidly progressive GN | 8.5 | 5400 | - |
| P. 20 | 73 | MN | Lung cancer | Nephrotic syndrome-AKI | 7.5 | 8341 | - |
| P.21 | 64 | IgA vasculitis | Lung cancer | RPGN | 8.1 | 2831 | - |
| P.22 | 50 | MN | Thyroid cancer | Nephrotic syndrome | 0.76 | 7700 | - |
| P.23 | 67 | MN | Lung cancer | Nephrotic syndrome | 0.79 | 10,500 | - |
| P.24 | 68 | MN | Kidney cancer | Nephrotic syndrome | 2.05 | 8100 | - |
| P.25 | 73 | MN | Breast cancer | Nephrotic syndrome | 0.66 | 4500 | - |
| P.26 | 59 | MN | Mesothelioma | Nephrotic syndrome | 0.6 | 10,314 | - |
| P.27 | 60 | MN | Colon (neuroendocrine) | Nephrotic syndrome | 0.6 | 6350 | - |
| P.28 | 72 | MCD | Ovary cancer | Nephrotic syndrome | 0.6 | 15,100 | ANA |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lionaki, S.; Marinaki, S.; Panagiotellis, K.; Tsoumbou, I.; Liapis, G.; Vlahadami, I.; Tzioufas, A.; Sfikakis, P.; Boletis, I. Glomerular Diseases Associated with Malignancies: Histopathological Pattern and Association with Circulating Autoantibodies. Antibodies 2020, 9, 18. https://doi.org/10.3390/antib9020018
Lionaki S, Marinaki S, Panagiotellis K, Tsoumbou I, Liapis G, Vlahadami I, Tzioufas A, Sfikakis P, Boletis I. Glomerular Diseases Associated with Malignancies: Histopathological Pattern and Association with Circulating Autoantibodies. Antibodies. 2020; 9(2):18. https://doi.org/10.3390/antib9020018
Chicago/Turabian StyleLionaki, Sophia, Smaragdi Marinaki, Konstantinos Panagiotellis, Ioanna Tsoumbou, George Liapis, Ioanna Vlahadami, Athanasios Tzioufas, Petros Sfikakis, and Ioannis Boletis. 2020. "Glomerular Diseases Associated with Malignancies: Histopathological Pattern and Association with Circulating Autoantibodies" Antibodies 9, no. 2: 18. https://doi.org/10.3390/antib9020018
APA StyleLionaki, S., Marinaki, S., Panagiotellis, K., Tsoumbou, I., Liapis, G., Vlahadami, I., Tzioufas, A., Sfikakis, P., & Boletis, I. (2020). Glomerular Diseases Associated with Malignancies: Histopathological Pattern and Association with Circulating Autoantibodies. Antibodies, 9(2), 18. https://doi.org/10.3390/antib9020018