
Vertebral Slip Morphology in Dysplastic Spondylolisthesis as a Criterion for the Choice of the L5/S1 Support (ALIF, PLIF, Fibular Graft) in Surgical Treatment

 , , , , , ,
, , , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection
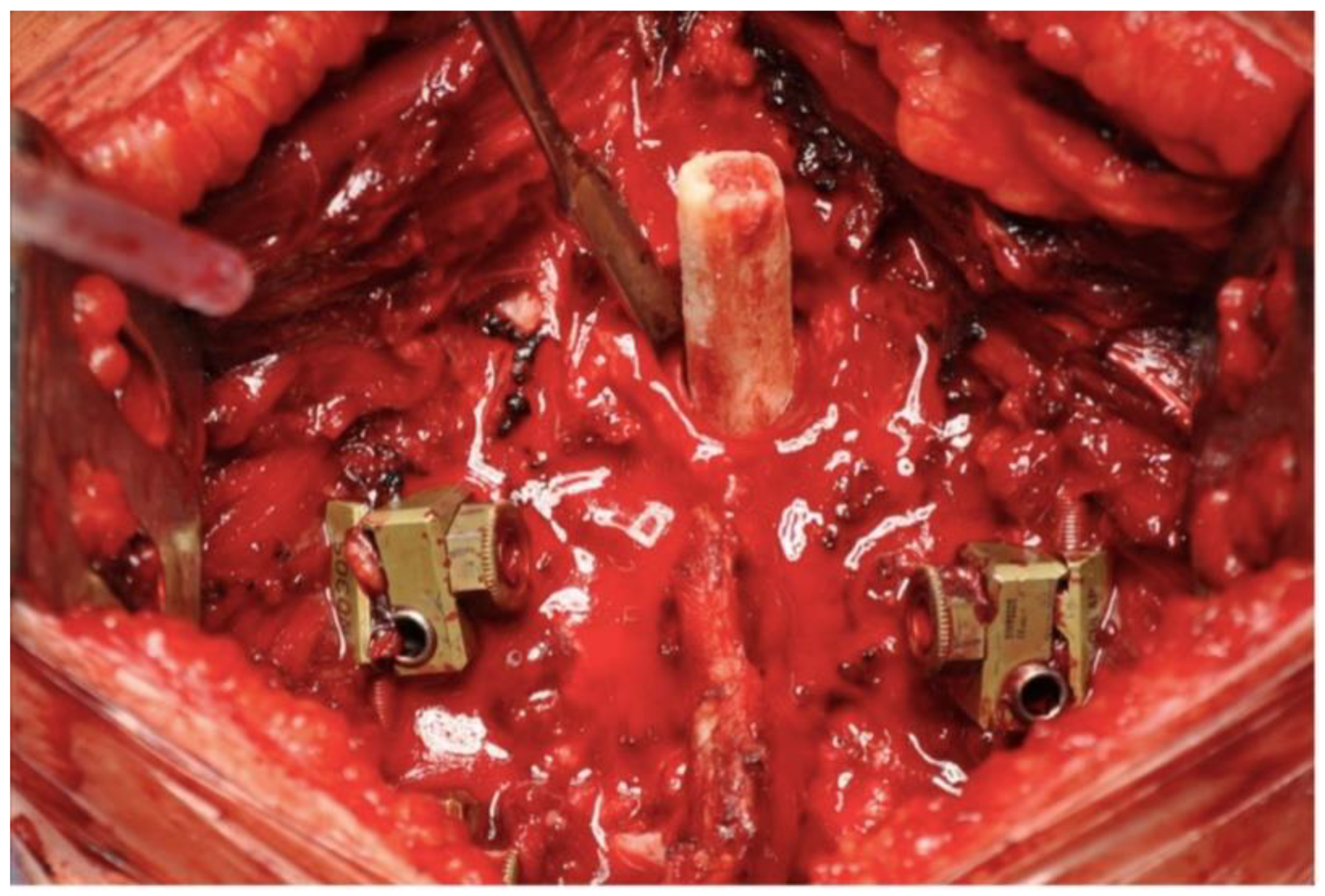
2.2. Surgical Technique
2.2.1. Posterior Approach Only
2.2.2. Combination of Posterior and Anterior Approaches
2.3. Evaluation
3. Results
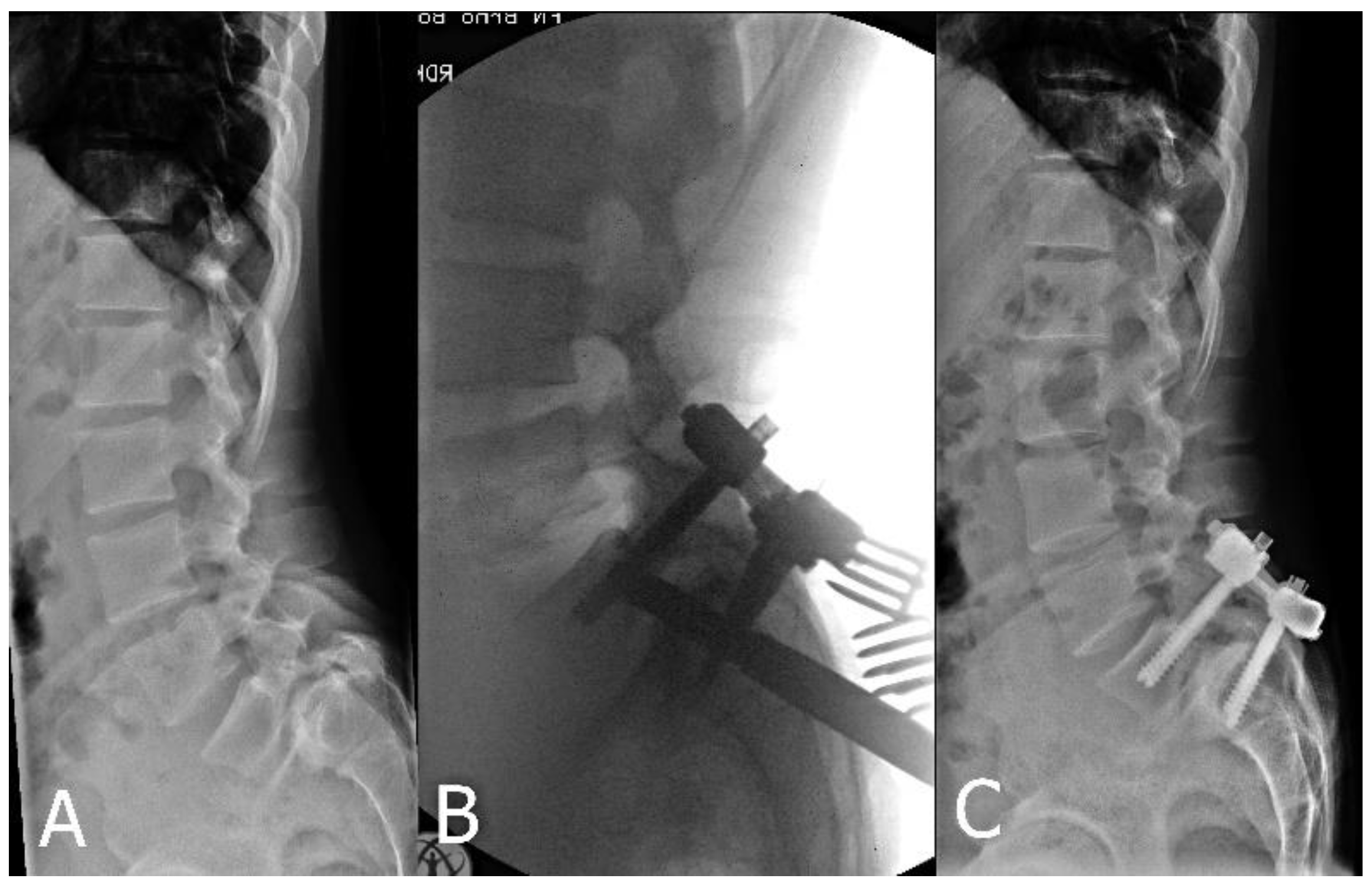
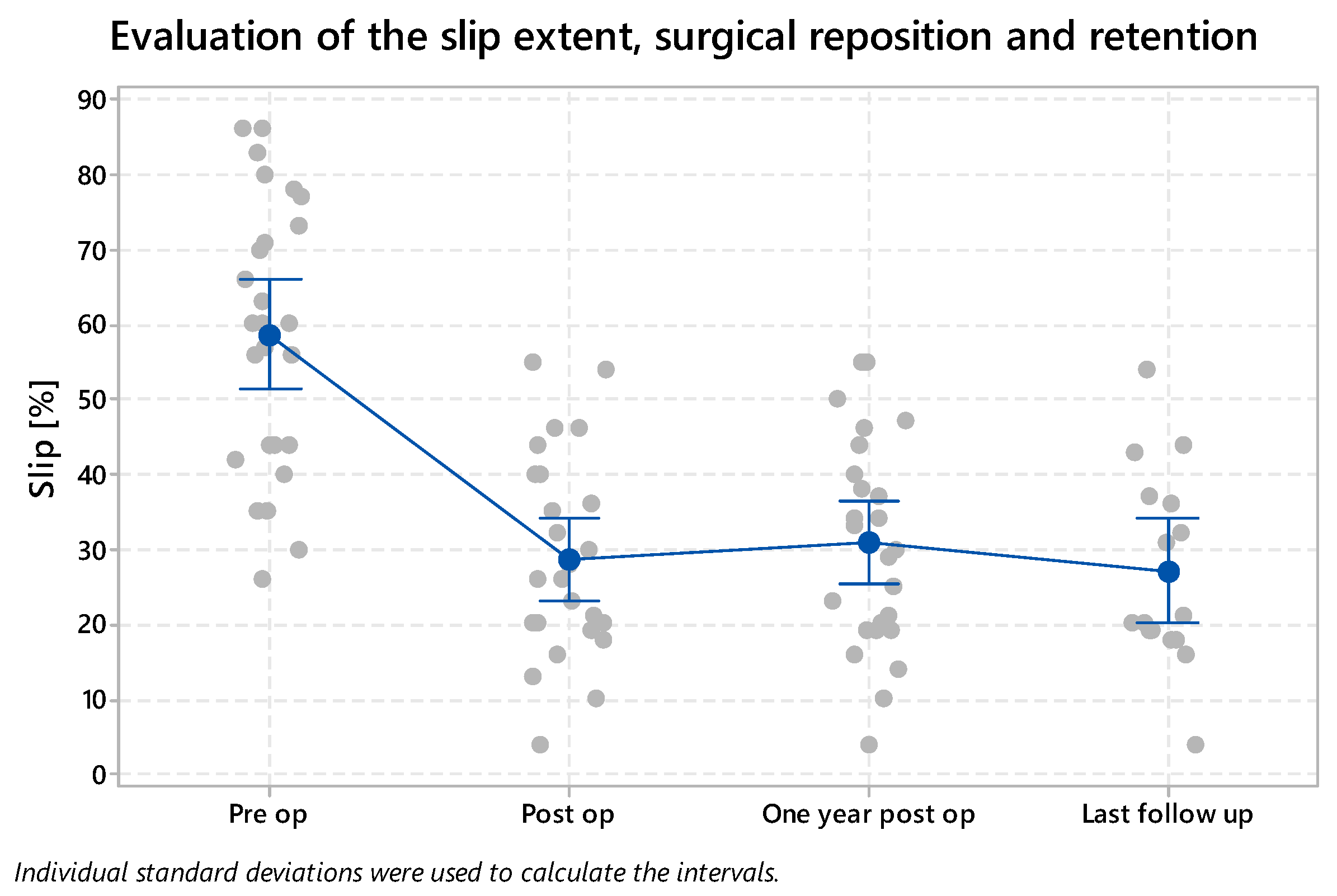
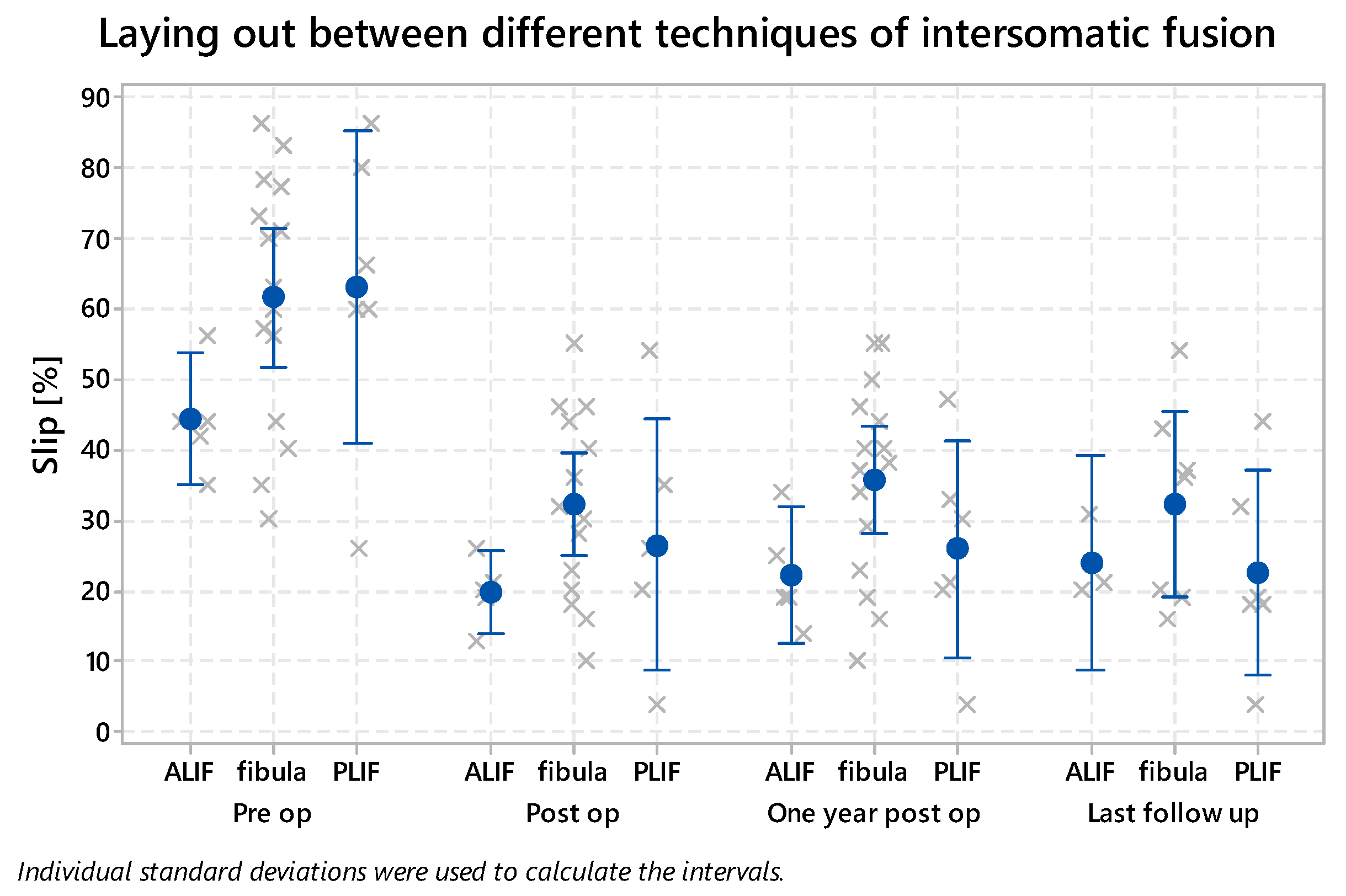
3.1. Slip Reduction and Retention
3.2. Surgical Time and Complications
3.3. Sagittal Balance
3.4. Satisfaction Questionnaires
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lamartina, C.; Zavatsky, J.M.; Petruzzi, M.; Specchia, N. Novel concepts in the evaluation and treatment of high-dysplastic spondylolisthesis. Eur. Spine J. 2009, 18, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Wiltse, L.L.; Newman, P.H.; Macnab, I. Classification of spondylolysis and spondylolisthesis. Clin. Orthop. 1976, 117, 23–29. [Google Scholar]
- Marchetti, P.C.; Bartolozzi, P. Classification of spondylolisthesis as a guideline for treatment. In The Textbook of Spinal Surgery, 2nd ed.; Bridwell, K.H., DeWald, R.L., Hammerberg, K.W., Eds.; Lippincott-Raven: Philadelphia, PA, USA, 1997; pp. 1211–1254. [Google Scholar]
- Vidal, J.; Marnay, T. Morphology and anteroposterior body equilibrium in spondylolisthesis L5-S1. Rev. Chir. Orthop. Reparatrice Appar. Mot. 1983, 69, 17–28. [Google Scholar] [PubMed]
- Osterman, K.; Schlenzka, D.; Poussa, M.; Seitsalo, S.; Virta, L. Isthmic spondylolisthesis in symptomatic and asymptomatic subjects, epidemiology, and natural history with special reference to disk abnormality and mode of treatment. Clin. Orthop. 1993, 297, 65–70. [Google Scholar] [CrossRef]
- Kunze, K.N.; Lilly, D.T.; Khan, J.M.; Louie, P.K.; Ferguson, J.; Basques, B.A.; Nolte, M.T.; Dewald, C.J. High-Grade Spondylolisthesis in Adults: Current Concepts in Evaluation and Management. Int. J. Spine Surg. 2020, 14, 327–340. [Google Scholar] [CrossRef]
- Wright, I.P. Who Was Meyerding? Spine 2003, 28, 733–735. [Google Scholar] [CrossRef]
- Taillard, W.F. Etiology of spondylolisthesis. Clin. Orthop. 1976, 117, 30–39. [Google Scholar] [CrossRef]
- Rivollier, M.; Marlier, B.; Kleiber, J.-C.; Eap, C.; Litre, C.-F. Surgical treatment of high-grade spondylolisthesis: Technique and results. J. Orthop. 2020, 22, 383–389. [Google Scholar] [CrossRef]
- Mac-Thiong, J.-M.; Labelle, H. A proposal for a surgical classification of pediatric lumbosacral spondylolisthesis based on current literature. Eur. Spine J. 2006, 15, 1425–1435. [Google Scholar] [CrossRef]
- Sasso, R.C.; Shively, K.D.; Reilly, T.M. Transvertebral Transsacral Strut Grafting for High-grade Isthmic Spondylolisthesis L5-S1 With Fibular Allograft. J. Spinal Disord. Technol. 2008, 21, 328–333. [Google Scholar] [CrossRef]
- Suk, K.S.; Jeon, C.H.; Park, M.S.; Moon, S.H.; Kim, N.H.; Lee, H.M. Comparison between posterolateral fusion with pedicle screw fixation and anterior interbody fusion with pedicle screw fixation in adult spondylolytic spondylolisthesis. Yonsei Med. J. 2001, 42, 316–323. [Google Scholar] [CrossRef] [PubMed]
- Ishihara, H.; Osada, R.; Kanamori, M.; Kawaguchi, Y.; Ohmori, K.; Kimura, T.; Matsui, H.; Tsuji, H. Minimum 10-year follow-up study of anterior lumbar interbody fusion for isthmic spondylolisthesis. J. Spinal Disord. 2001, 14, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Fairbank, J.C.T.; Pynsent, P.B. The Oswestry Disability Index. Spine 2000, 25, 2940–2953. [Google Scholar] [CrossRef] [PubMed]
- Jaeschke, R.; Singer, J.; Guyatt, G.H. Measurement of health status: Ascertaining the minimal clinically important difference. Control. Clin. Trials 1989, 10, 407–415. [Google Scholar] [CrossRef]
- Suchomel, P.; Krbec, M. Spondylolisthesis—Diagnostics and Therapy; Galen: Prague, Czech Republic, 2007; pp. 109–111. [Google Scholar]
- Dewald, C.J.; Vartabedian, J.E.; Rodts, M.F.; Hammerberg, K.W. Evaluation and Management of High-Grade Spondylolisthesis in Adults. Spine 2005, 30, S49–S59. [Google Scholar] [CrossRef]
- Labelle, H.; Roussouly, P.; Berthonnaud, E.; Transfeldt, E.; O’Brien, M.; Chopin, D.; Hresko, T.; Dimnet, J. Spondylolisthesis, Pelvic Incidence, and Spinopelvic Balance. Spine 2004, 29, 2049–2054. [Google Scholar] [CrossRef]
- Hanson, D.S.; Bridwell, K.H.; Rhee, J.M.; Lenke, L.G. Correlation of Pelvic Incidence with Low- and High-Grade Isthmic Spondylolisthesis. Spine 2002, 27, 2026–2029. [Google Scholar] [CrossRef]
- Hresko, M.T.; Labelle, H.; Roussouly, P.; Berthonnaud, E. Classification of High-Grade Spondylolistheses Based on Pelvic Version and Spine Balance. Spine 2007, 32, 2208–2213. [Google Scholar] [CrossRef]
- Boxall, D.; Bradford, D.S.; Winter, R.B.; Moe, J.H. Management of severe spondylolisthesis in children and adolescents. J. Bone Jt. Surg. Am. 1979, 61, 479–495. [Google Scholar] [CrossRef]
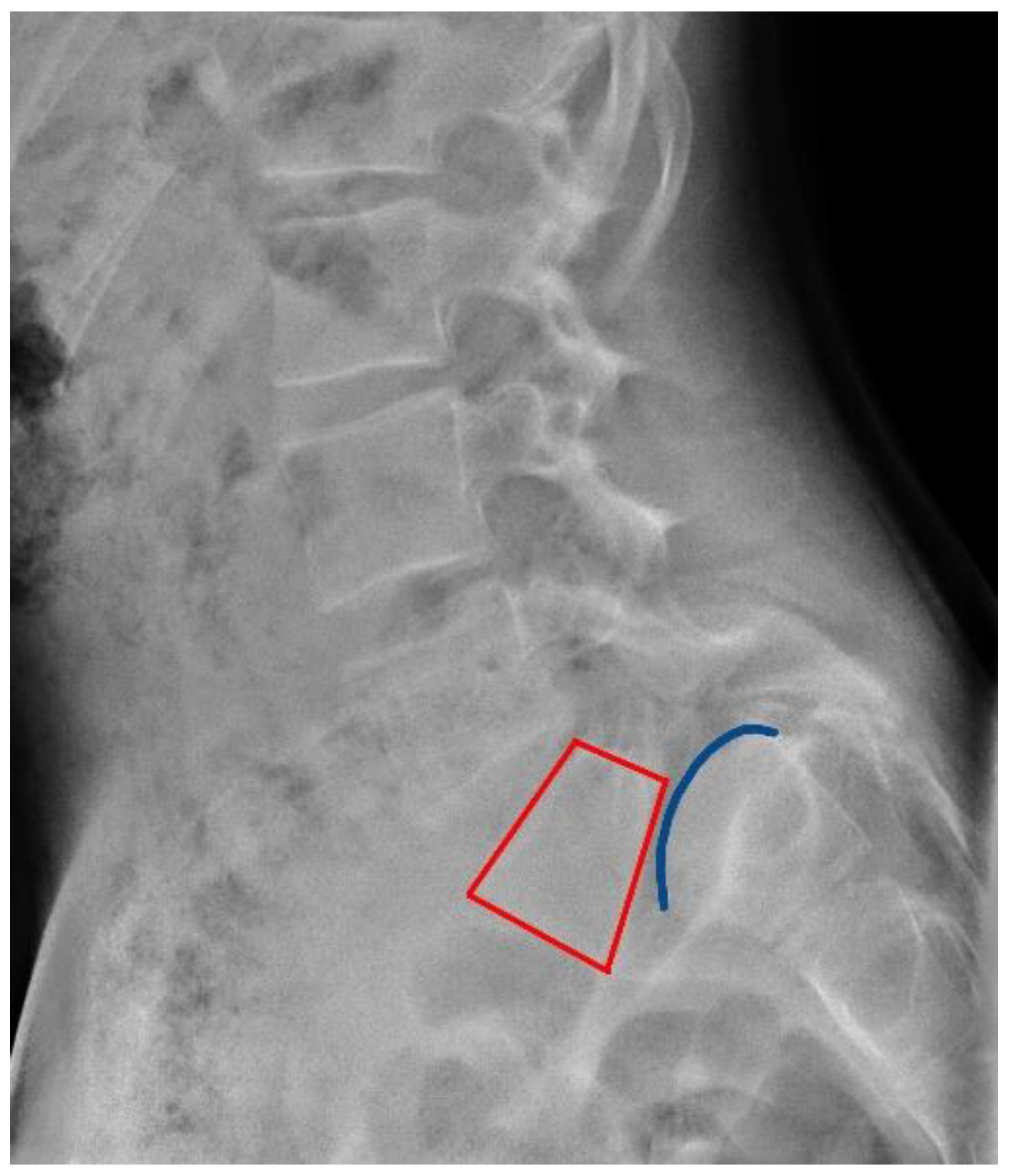
- Lamartina, C. A square to indicate the unstable zone in severe spondylolisthesis. Eur. Spine J. 2001, 10, 444–448. [Google Scholar] [CrossRef]
- Newman, P.H. Spondylolisthesis, its cause and effect. Ann. R. Coll. Surg. Engl. 1955, 16, 305–323. [Google Scholar] [PubMed]
- Scaglietti, O.; Frontino, G. Technique of anatomical reduction of lumbar spondylolisthesis and its surgical stabilization. Clin. Orthop. 1976, 117, 165–175. [Google Scholar] [CrossRef]
- Bourassa-Moreau, É.; Mac-Thiong, J.-M.; Joncas, J.; Parent, S.; Labelle, H. Quality of life of patients with high-grade spondylolisthesis: Minimum 2-year follow-up after surgical and nonsurgical treatments. Spine J. 2013, 13, 770–774. [Google Scholar] [CrossRef] [PubMed]
- Poussa, M.; Schlenzka, D.; Seitsalo, S.; Ylikoski, M.; Hurri, H.; Osterman, K. Surgical Treatment of Severe Isthmic Spondylolisthesis in Adolescents: Reduction or Fusion: In Situ. Spine 1993, 18, 894–901. [Google Scholar] [CrossRef]
- Agabegi, S.S.; Fischgrund, J.S. Contemporary management of isthmic spondylolisthesis: Pediatric and adult. Spine J. 2010, 10, 530–543. [Google Scholar] [CrossRef]
- Bradford, D.S.; Boachie-Adjei, O. Treatment of severe spondylolisthesis by anterior and posterior reduction and stabilization. A long-term follow-up study. J. Bone Jt. Surg. Am. 1990, 72, 1060–1066. [Google Scholar] [CrossRef]
- Longo, U.G.; Loppini, M.; Romeo, G.; Maffulli, N.; Denaro, V. Evidence-Based Surgical Management of Spondylolisthesis: Reduction or Arthrodesis in Situ. J. Bone Jt. Surg. 2014, 96, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Boos, N.; Marchesi, D.; Zuber, K.; Aebi, M. Treatment of Severe Spondylolisthesis by Reduction and Pedicular Fixation: A 4–6-Year Follow-Up Study. Spine 1993, 18, 1655–1661. [Google Scholar] [CrossRef]
- Spruit, M.; Pavlov, P.; Leitao, J.; De Kleuver, M.; Anderson, P.; Den Boer, F. Posterior reduction and anterior lumbar interbody fusion in symptomatic low-grade adult isthmic spondylolisthesis: Short-term radiological and functional outcome. Eur. Spine J. 2002, 11, 428–433. [Google Scholar] [CrossRef][Green Version]
- Tu, K.-C.; Shih, C.-M.; Chen, K.-H.; Pan, C.-C.; Jiang, F.-C.; Hsu, C.-E.; Wang, Y.-M.; Lee, C.-H. Direct reduction of high-grade lumbosacral spondylolisthesis with anterior cantilever technique—Surgical technique note and preliminary results. BMC Musculoskelet. Disord. 2021, 22, 1–10. [Google Scholar] [CrossRef]
- Hanson, D.S.; Bridwell, K.H.; Rhee, J.M.; Lenke, L.G. Dowel Fibular Strut Grafts for High-Grade Dysplastic Isthmic Spondylolisthesis. Spine 2002, 27, 1982–1988. [Google Scholar] [CrossRef] [PubMed]
- Shufflebarger, H.L.; Geck, M.J. High-Grade Isthmic Dysplastic Spondylolisthesis. Spine 2005, 30, S42–S48. [Google Scholar] [CrossRef] [PubMed]
- Min, K.; Liebscher, T.; Rothenfluh, D. Sacral dome resection and single-stage posterior reduction in the treatment of high-grade high dysplastic spondylolisthesis in adolescents and young adults. Eur. Spine J. 2011, 21, 785–791. [Google Scholar] [CrossRef] [PubMed]
- Molinari, M.R.W.; Bridwell, K.H.; Lenke, L.G.; Ungacta, F.F.; Riew, K.D. Complications in the Surgical Treatment of Pediatric High-Grade, Isthmic Dysplastic Spondylolisthesis: A Comparison of Three Surgical Approaches. Spine 1999, 24, 1701. [Google Scholar] [CrossRef]
- Lombardi, F.; Custodi, V.M.; Pugliese, R.; Risso, A.; Gaetani, P.; Butti, G. Treatment of high-grade spondylolisthesis with Schanz recoil screws: Our experience. Eur. Spine J. 2013, 22, 914–918. [Google Scholar] [CrossRef]
- Martiniani, M.; Lamartina, C.; Specchia, N. “In situ” fusion or reduction in high-grade high dysplastic developmental spondylolisthesis (HDSS). Eur. Spine J. 2012, 21, 134–140. [Google Scholar] [CrossRef]
- Štulík, J.; Nesnidal, P.; Kozelnicka, K.; Barna, M. Surgical Treatment of High-Grade High-Dysplastic Spondylolistheses in Young Patients—Prospective Monocentric Study of 29 Patients. Acta Chir. Orthop. Traumatol. Cech 2018, 85, 305–318. [Google Scholar]
- Schär, R.T.; Sutter, M.; Mannion, A.F.; Eggspühler, A.; Jeszenszky, D.; Fekete, T.F.; Kleinstück, F.; Haschtmann, D. Outcome of L5 radiculopathy after reduction and instrumented transforaminal lumbar interbody fusion of high-grade L5–S1 isthmic spondylolisthesis and the role of intraoperative neurophysiological monitoring. Eur. Spine J. 2017, 26, 679–690. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Spinopelvic Parameters | Preoperative | Postoperative | ||
|---|---|---|---|---|
| Mean | Min–Max | Mean | Min–Max | |
| Slip angle (SA) | 16° | 0–53° | 9° | 0–28° |
| Pelvic Incidence, PI | 70° | 55–84° | 70° | 46–84° |
| Pelvic Tilt, PT | 31° | 5–54° | 24° | 5–48° |
| Sacral slope, SS | 39° | 20–67° | 43° | 22–75° |
| Incidence L5, IL5 | 55° | 20–111° | 43° | 21–74° |
| Lumbar Lordosis, LL | 56° | 20–82° | 51° | 24–82° |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vyskocil, R.; Prymek, M.; Ryba, L.; Sklensky, J.; Kocanda, J.; Lujc, M.; Vosynek, P.; Repko, M. Vertebral Slip Morphology in Dysplastic Spondylolisthesis as a Criterion for the Choice of the L5/S1 Support (ALIF, PLIF, Fibular Graft) in Surgical Treatment. Symmetry 2022, 14, 1466. https://doi.org/10.3390/sym14071466
Vyskocil R, Prymek M, Ryba L, Sklensky J, Kocanda J, Lujc M, Vosynek P, Repko M. Vertebral Slip Morphology in Dysplastic Spondylolisthesis as a Criterion for the Choice of the L5/S1 Support (ALIF, PLIF, Fibular Graft) in Surgical Treatment. Symmetry. 2022; 14(7):1466. https://doi.org/10.3390/sym14071466
Chicago/Turabian StyleVyskocil, Robert, Martin Prymek, Ludek Ryba, Jan Sklensky, Jan Kocanda, Michael Lujc, Petr Vosynek, and Martin Repko. 2022. "Vertebral Slip Morphology in Dysplastic Spondylolisthesis as a Criterion for the Choice of the L5/S1 Support (ALIF, PLIF, Fibular Graft) in Surgical Treatment" Symmetry 14, no. 7: 1466. https://doi.org/10.3390/sym14071466
APA StyleVyskocil, R., Prymek, M., Ryba, L., Sklensky, J., Kocanda, J., Lujc, M., Vosynek, P., & Repko, M. (2022). Vertebral Slip Morphology in Dysplastic Spondylolisthesis as a Criterion for the Choice of the L5/S1 Support (ALIF, PLIF, Fibular Graft) in Surgical Treatment. Symmetry, 14(7), 1466. https://doi.org/10.3390/sym14071466