
Understanding Vernal Keratoconjunctivitis: Beyond Allergic Mechanisms



{kind=link}
{kind=link}
{kind=link}
Abstract
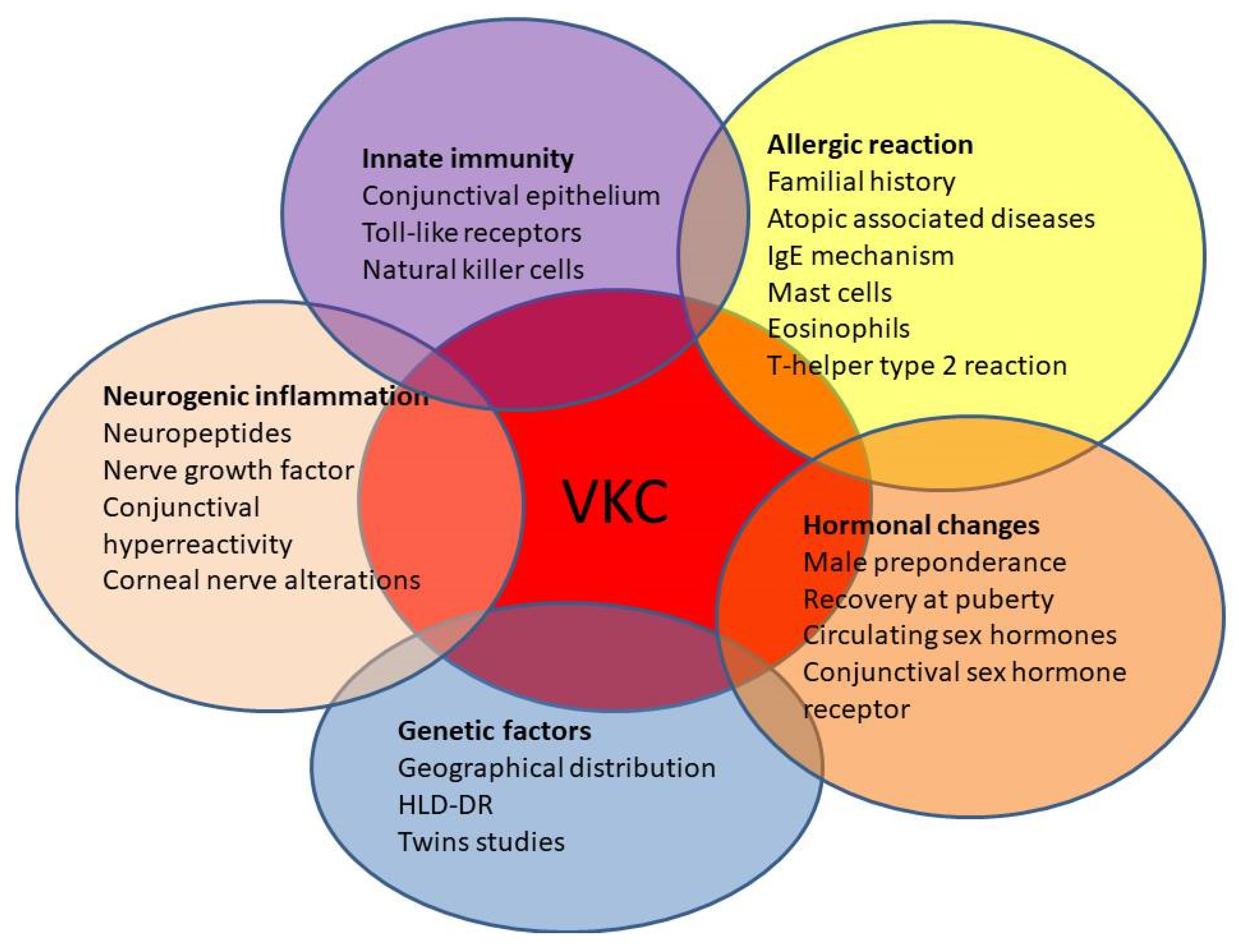
1. Introduction
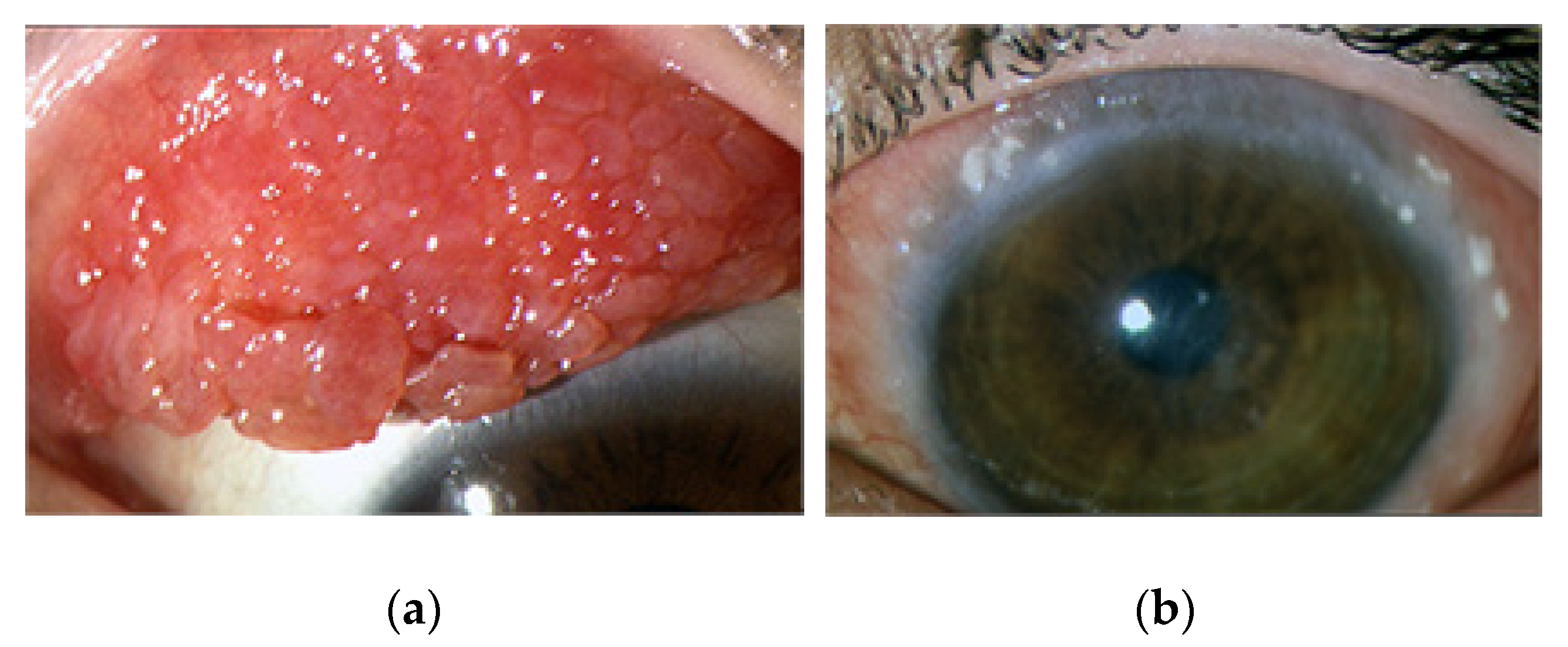
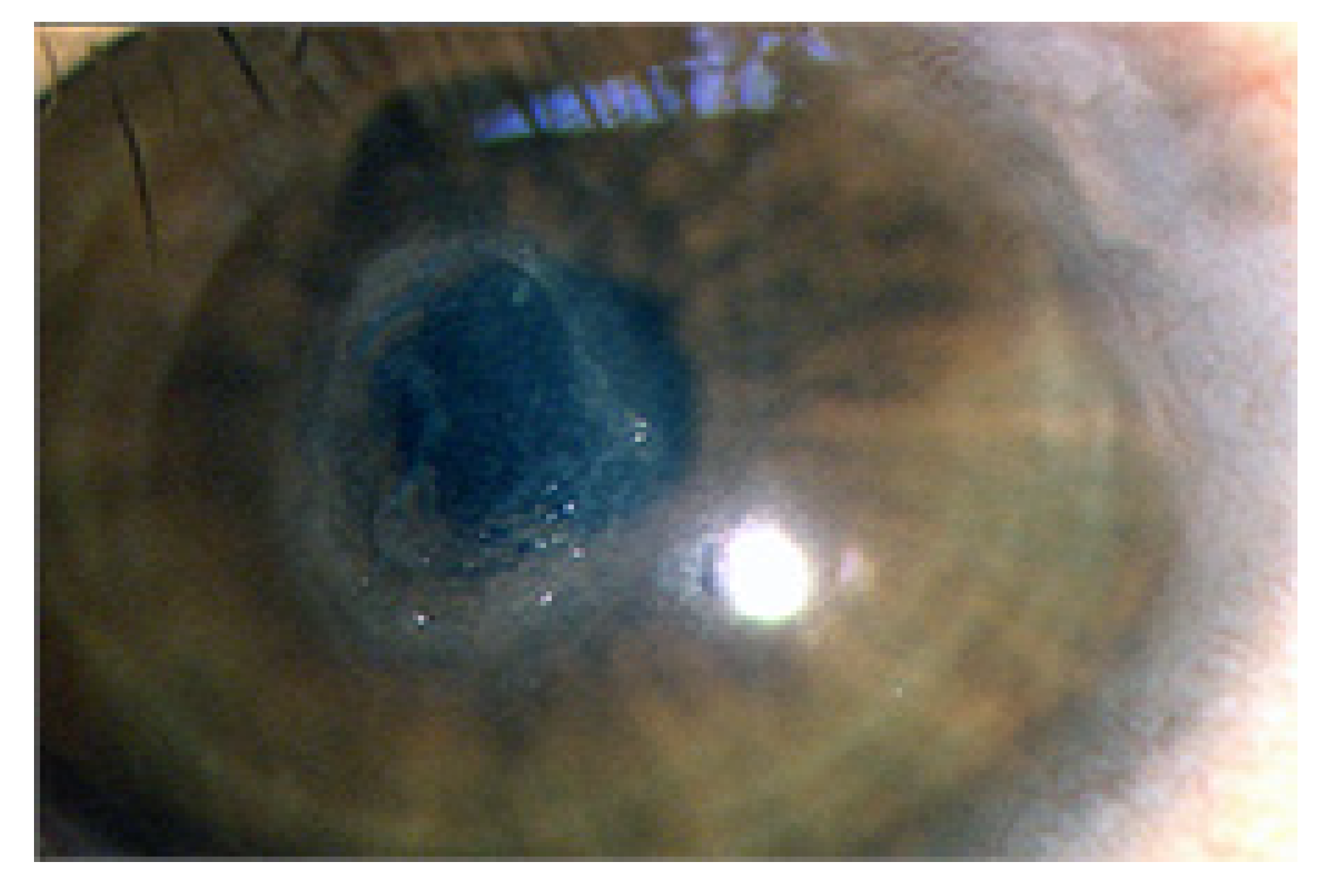
2. Clinical Characteristics of VKC
3. IgE-Mediated Hypersensitivity Reaction in VKC
4. Cellular Allergic Reaction in VKC
5. Role of Innate Immunity in VKC
6. Genetic Factors
7. Neuroinflammatory Reaction in VKC
8. Hormonal Influence in VKC
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Bonini, S.; Coassin, M.; Aronni, S.; Lambiase, A. Vernal keratoconjunctivitis. Eye 2004, 18, 345–351. [Google Scholar] [CrossRef]
- Bonini, S.; Bonini, S.; Lambiase, A.; Marchi, S.; Pasqualetti, P.; Zuccaro, O.; Rama, P.; Magrini, L.; Juhas, T.; Bucci, M.G. Vernal keratoconjunctivitis revisited: A case series of 195 patients with long-term followup. Ophthalmology 2000, 107, 1157–1163. [Google Scholar] [CrossRef]
- Leonardi, A.; Busca, F.; Motterle, L.; Cavarzeran, F.; Fregona, I.A.; Plebani, M.; Secchi, A.G. Case series of 406 vernal keratoconjunctivitis patients: A demographic and epidemiological study. Acta Ophthalmol. Scand. 2006, 84, 406–410. [Google Scholar] [CrossRef]
- Sacchetti, M.; Abicca, I.; Bruscolini, A.; Cavaliere, C.; Nebbioso, M.; Lambiase, A. Allergic conjunctivitis: Current concepts on pathogenesis and management. J. Biol. Regul. Homeost. Agents 2018, 32, 49–60. [Google Scholar]
- De Smedt, S.; Wildner, G.; Kestelyn, P. Vernal keratoconjunctivitis: An update. Br. J. Ophthalmol. 2013, 97, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Lambiase, A.; Normando, E.M.; Vitiello, L.; Micera, A.; Sacchetti, M.; Perrella, E.; Racioppi, L.; Bonini, S.; Bonini, S. Natural killer cells in vernal keratoconjunctivitis. Mol. Vis. 2007, 13, 1562–1567. [Google Scholar] [PubMed]
- Lambiase, A.; Micera, A.; Sacchetti, M.; Mantelli, F.; Bonini, S. Toll-like receptors in ocular surface diseases: Overview and new findings. Clin. Sci. 2011, 120, 441–450. [Google Scholar] [CrossRef] [PubMed]
- Micera, A.; Stampachiacchiere, B.; Normando, E.M.; Lambiase, A.; Bonini, S.; Bonini, S. Nerve growth factor modulates toll-like receptor (TLR) 4 and 9 expression in cultured primary VKC conjunctival epithelial cells. Mol. Vis. 2009, 15, 2037–2044. [Google Scholar] [PubMed]
- Bonini, S.; Micera, A.; Iovieno, A.; Lambiase, A.; Bonini, S. Expression of Toll-like receptors in healthy and allergic conjunctiva. Ophthalmology 2005, 112, 1528; discussion 1529–1548. [Google Scholar] [CrossRef]
- Leonardi, A.; Lazzarini, D.; Motterle, L.; Bortolotti, M.; Deligianni, V.; Curnow, S.J.; Bonini, S.; Fregona, I.A. Vernal keratoconjunctivitis-like disease in adults. Am. J. Ophthalmol. 2013, 155, 796–803. [Google Scholar] [CrossRef] [PubMed]
- Di Zazzo, A.; Bonini, S.; Fernandes, M. Adult vernal keratoconjunctivitis. Curr. Opin. Allergy Clin. Immunol. 2020, 20, 501–506. [Google Scholar] [CrossRef]
- Kosrirukvongs, P.; Vichyanond, P.; Wongsawad, W. Vernal keratoconjunctivitis in Thailand. Asian Pac. J. Allergy Immunol. 2003, 21, 25–30. [Google Scholar]
- Lambiase, A.; Minchiotti, S.; Leonardi, A.; Secchi, A.G.; Rolando, M.; Calabria, G.; Orsoni, J.; Zola, E.; Ferreri, G.; Aragona, P.; et al. Prospective, multicenter demographic and epidemiological study on vernal keratoconjunctivitis: A glimpse of ocular surface in Italian population. Ophthalmic Epidemiol. 2009, 16, 38–41. [Google Scholar] [CrossRef] [PubMed]
- Vichyanond, P.; Pacharn, P.; Pleyer, U.; Leonardi, A. Vernal keratoconjunctivitis: A severe allergic eye disease with remodeling changes. Pediatr. Allergy Immunol. 2014, 25, 314–322. [Google Scholar] [CrossRef] [PubMed]
- Leonardi, A. Vernal keratoconjunctivitis: Pathogenesis and treatment. Prog. Retin. Eye Res. 2002, 21, 319–339. [Google Scholar] [CrossRef]
- Bonini, S.; Sacchetti, M.; Mantelli, F.; Lambiase, A. Clinical grading of vernal keratoconjunctivitis. Curr. Opin. Allergy Clin. Immunol. 2007, 7, 436–441. [Google Scholar] [CrossRef]
- Feizi, S.; Javadi, M.A.; Alemzadeh-Ansari, M.; Arabi, A.; Shahraki, T.; Kheirkhah, A. Management of corneal complications in vernal keratoconjunctivitis: A review. Ocul. Surf. 2021, 19, 282–289. [Google Scholar] [CrossRef]
- Liendo, V.L.; Vola, M.E.; Barreiro, T.P.; Wakamatsu, T.H.; Gomes, J.A.P.; Santos, M.S.D. Topical tacrolimus for the treatment of severe allergic keratoconjunctivitis in children. Arq. Bras. Oftalmol. 2017, 80, 211–214. [Google Scholar] [CrossRef]
- Arif, A.S.; Aaqil, B.; Siddiqui, A.; Nazneen, Z.; Farooq, U. Corneal Complications and Visual Impairment in Vernal Keratoconjunctivitis Patients. J. Ayub Med. Coll. Abbottabad JAMC 2017, 29, 58–60. [Google Scholar]
- Nebbioso, M.; Zicari, A.M.; Lollobrigida, V.; Marenco, M.; Duse, M. Assessment of corneal alterations by confocal microscopy in vernal keratoconjunctivitis. Semin. Ophthalmol. 2015, 30, 40–43. [Google Scholar] [CrossRef]
- Leonardi, A.; Lazzarini, D.; Bortolotti, M.; Piliego, F.; Midena, E.; Fregona, I. Corneal confocal microscopy in patients with vernal keratoconjunctivitis. Ophthalmology 2012, 119, 509–515. [Google Scholar] [CrossRef] [PubMed]
- Sacchetti, M.; Lambiase, A. Neurotrophic factors and corneal nerve regeneration. Neural Regen. Res. 2017, 12, 1220–1224. [Google Scholar] [CrossRef] [PubMed]
- Artesani, M.C.; Esposito, M.; Sacchetti, M.; Sansone, A.; Romanzo, A.; Buzzonetti, L.; Fiocchi, A.G.; Mennini, M. Health-related quality of life in children at the diagnosis of Vernal Keratoconjunctivitis. Pediatr. Allergy Immunol. 2021, 32, 1271–1277. [Google Scholar] [CrossRef] [PubMed]
- Sacchetti, M.; Baiardini, I.; Lambiase, A.; Aronni, S.; Fassio, O.; Gramiccioni, C.; Bonini, S.; Bonini, S. Development and testing of the quality of life in children with vernal keratoconjunctivitis questionnaire. Am. J. Ophthalmol. 2007, 144, 557–563. [Google Scholar] [CrossRef]
- Zicari, A.M.; Capata, G.; Nebbioso, M.; De Castro, G.; Midulla, F.; Leonardi, L.; Loffredo, L.; Spalice, A.; Perri, L.; Duse, M. Vernal Keratoconjunctivitis: An update focused on clinical grading system. Ital. J. Pediatr. 2019, 45, 64. [Google Scholar] [CrossRef]
- Sacchetti, M.; Bruscolini, A.; Abicca, I.; Nebbioso, M.; La Cava, M.; Bonini, S.; Lambiase, A. Current and emerging treatment options for vernal keratoconjunctivitis. Expert Opin. Orphan Drugs 2017, 5, 343–353. [Google Scholar] [CrossRef]
- Senthil, S.; Thakur, M.; Rao, H.L.; Mohamed, A.; Jonnadula, G.B.; Sangwan, V.; Garudadri, C.S. Steroid-induced glaucoma and blindness in vernal keratoconjunctivitis. Br. J. Ophthalmol. 2020, 104, 265–269. [Google Scholar] [CrossRef]
- Lambiase, A.; Leonardi, A.; Sacchetti, M.; Deligianni, V.; Sposato, S.; Bonini, S. Topical cyclosporine prevents seasonal recurrences of vernal keratoconjunctivitis in a randomized, double-masked, controlled 2-year study. J. Allergy Clin. Immunol. 2011, 128, 896–897.e899. [Google Scholar] [CrossRef]
- Roumeau, I.; Coutu, A.; Navel, V.; Pereira, B.; Baker, J.S.; Chiambaretta, F.; Bremond-Gignac, D.; Dutheil, F. Efficacy of medical treatments for vernal keratoconjunctivitis: A systematic review and meta-analysis. J. Allergy Clin. Immunol. 2021, 148, 822–834. [Google Scholar] [CrossRef]
- Yucel, O.E.; Ulus, N.D. Efficacy and safety of topical cyclosporine A 0.05% in vernal keratoconjunctivitis. Singap. Med. J. 2016, 57, 507–510. [Google Scholar] [CrossRef]
- Sacchetti, M.; Lambiase, A.; Mantelli, F.; Deligianni, V.; Leonardi, A.; Bonini, S. Tailored approach to the treatment of vernal keratoconjunctivitis. Ophthalmology 2010, 117, 1294–1299. [Google Scholar] [CrossRef]
- Leonardi, A.; Lazzarini, D.; La Gloria Valerio, A.; Scalora, T.; Fregona, I. Corneal staining patterns in vernal keratoconjunctivitis: The new VKC-CLEK scoring scale. Br. J. Ophthalmol. 2018, 102, 1448–1453. [Google Scholar] [CrossRef]
- Bonini, S.; Bonini, S. IgE and non-IgE mechanisms in ocular allergy. Ann. Allergy 1993, 71, 296–299. [Google Scholar]
- Abelson, M.B.; Baird, R.S.; Allansmith, M.R. Tear histamine levels in vernal conjunctivitis and other ocular inflammations. Ophthalmology 1980, 87, 812–814. [Google Scholar] [CrossRef]
- Fukagawa, K.; Saito, H.; Azuma, N.; Tsubota, K.; Iikura, Y.; Oguchi, Y. Histamine and tryptase levels in allergic conjunctivitis and vernal keratoconjunctivitis. Cornea 1994, 13, 345–348. [Google Scholar] [CrossRef] [PubMed]
- Leonardi, A.; Di Stefano, A.; Vicari, C.; Motterle, L.; Brun, P. Histamine H4 receptors in normal conjunctiva and in vernal keratoconjunctivitis. Allergy 2011, 66, 1360–1366. [Google Scholar] [CrossRef]
- Bonini, S.; Bonini, S.; Schiavone, M.; Centofanti, M.; Allansmith, M.R.; Bucci, M.G. Conjunctival hyperresponsiveness to ocular histamine challenge in patients with vernal conjunctivitis. J. Allergy Clin. Immunol. 1992, 89, 103–107. [Google Scholar] [CrossRef]
- Allansmith, M.R.; Hahn, G.S.; Simon, M.A. Tissue, tear, and serum IgE concentrations in vernal conjunctivitis. Am. J. Ophthalmol. 1976, 81, 506–511. [Google Scholar] [CrossRef]
- Leonardi, A.; Borghesan, F.; Faggian, D.; Plebani, M. Microarray-based IgE detection in tears of patients with vernal keratoconjunctivitis. Pediatr. Allergy Immunol. 2015, 26, 641–645. [Google Scholar] [CrossRef] [PubMed]
- Ballow, M.; Mendelson, L. Specific immunoglobulin E antibodies in tear secretions of patients with vernal conjunctivitis. J. Allergy Clin. Immunol. 1980, 66, 112–118. [Google Scholar] [CrossRef]
- Sompolinsky, D.; Samra, Z.; Zavaro, A.; Barishak, Y. Allergen-specific immunoglobulin E antibodies in tears and serum of vernal conjunctivitis patients. Int. Arch. Allergy Appl. Immunol. 1984, 75, 317–321. [Google Scholar] [CrossRef]
- Abu El-Asrar, A.M.; Fatani, R.A.; Missotten, L.; Geboes, K. Expression of CD23/CD21 and CD40/CD40 ligand in vernal keratoconjunctivitis. Eye 2001, 15, 217–224. [Google Scholar] [CrossRef][Green Version]
- Leonardi, A.; Fregona, I.A.; Gismondi, M.; Daniotti, E.; Carniel, G.; Secchi, A.G. Correlation between conjunctival provocation test (CPT) and systemic allergometric tests in allergic conjunctivitis. Eye 1990, 4, 760–764. [Google Scholar] [CrossRef][Green Version]
- Leonardi, A.; DeFranchis, G.; Zancanaro, F.; Crivellari, G.; De Paoli, M.; Plebani, M.; Secchi, A.G. Identification of local Th2 and Th0 lymphocytes in vernal conjunctivitis by cytokine flow cytometry. Investig. Ophthalmol. Vis. Sci. 1999, 40, 3036–3040. [Google Scholar]
- Metz, D.P.; Hingorani, M.; Calder, V.L.; Buckley, R.J.; Lightman, S.L. T-cell cytokines in chronic allergic eye disease. J. Allergy Clin. Immunol. 1997, 100, 817–824. [Google Scholar] [CrossRef]
- Calder, V.L.; Jolly, G.; Hingorani, M.; Adamson, P.; Leonardi, A.; Secchi, A.G.; Buckley, R.J.; Lightman, S. Cytokine production and mRNA expression by conjunctival T-cell lines in chronic allergic eye disease. Clin. Exp. Allergy 1999, 29, 1214–1222. [Google Scholar] [CrossRef] [PubMed]
- Leonardi, A.; Fregona, I.A.; Plebani, M.; Secchi, A.G.; Calder, V.L. Th1- and Th2-type cytokines in chronic ocular allergy. Graefe’s Arch. Clin. Exp. Ophthalmol. 2006, 244, 1240–1245. [Google Scholar] [CrossRef] [PubMed]
- Bonini, S.; Ghinelli, E. The early and late phase of the ocular allergic reaction. Acta Ophthalmol. Scand. 2000, 230, 41. [Google Scholar] [CrossRef] [PubMed]
- Ebihara, N.; Matsuda, A.; Seto, T.; Ohtomo, K.; Funaki, T.; Takai, T.; Murakami, A. The epithelium takes center stage in allergic keratoconjunctivitis. Cornea 2010, 29 (Suppl. 1), S41–S47. [Google Scholar] [CrossRef]
- Zhang, Z.D.; Deng, Y.X.; Ma, H.X.; Chen, X.G.; Chen, L.H.; Qu, J. Thymic Stromal Lymphopoietin-Related Allergic Pathway in Patients with Vernal Keratoconjunctivitis. Cornea 2019, 38, 344–351. [Google Scholar] [CrossRef]
- Iype, J.; Fux, M. Basophils Orchestrating Eosinophils’ Chemotaxis and Function in Allergic Inflammation. Cells 2021, 10, 895. [Google Scholar] [CrossRef]
- Bonini, S.; Magrini, L.; Rotiroti, G.; Lambiase, A.; Tomassini, M.; Rumi, C.; Bonini, S. The eosinophil and the eye. Allergy 1997, 52, 44–47. [Google Scholar] [CrossRef]
- Leonardi, A.; Borghesan, F.; Faggian, D.; Secchi, A.; Plebani, M. Eosinophil cationic protein in tears of normal subjects and patients affected by vernal keratoconjunctivitis. Allergy 1995, 50, 610–613. [Google Scholar] [CrossRef] [PubMed]
- Bruschi, G.; Ghiglioni, D.G.; Osnaghi, S.; Rosazza, C.; Pires Marafon, D.; Landi, M.; Marchisio, P.G. Role of ocular cytology in vernal keratoconjunctivitis. Immun. Inflamm. Dis. 2020, 8, 3–7. [Google Scholar] [CrossRef]
- Bonini, S.; Schiavone, M.; Bonini, S.; Magrini, L.; Lischetti, P.; Lambiase, A.; Bucci, M.G. Efficacy of lodoxamide eye drops on mast cells and eosinophils after allergen challenge in allergic conjunctivitis. Ophthalmology 1997, 104, 849–853. [Google Scholar] [CrossRef]
- Leonardi, A.; Jose, P.J.; Zhan, H.; Calder, V.L. Tear and mucus eotaxin-1 and eotaxin-2 in allergic keratoconjunctivitis. Ophthalmology 2003, 110, 487–492. [Google Scholar] [CrossRef]
- Abu El-Asrar, A.M.; Struyf, S.; Al-Kharashi, S.A.; Missotten, L.; Van Damme, J.; Geboes, K. Chemokines in the limbal form of vernal keratoconjunctivitis. Br. J. Ophthalmol. 2000, 84, 1360–1366. [Google Scholar] [CrossRef] [PubMed]
- Secchi, A.; Leonardi, A.; Abelson, M. The role of eosinophil cationic protein (ECP) and histamine in vernal keratoconjunctivitis. Ocul. Immunol. Inflamm. 1995, 3, 23–28. [Google Scholar] [CrossRef]
- Trocme, S.D.; Leiferman, K.M.; George, T.; Bonini, S.; Foster, C.S.; Smit, E.E.; Sra, S.K.; Grabowski, L.R.; Dohlman, C.H. Neutrophil and eosinophil participation in atopic and vernal keratoconjunctivitis. Curr. Eye Res. 2003, 26, 319–325. [Google Scholar] [CrossRef]
- Tomassini, M.; Magrini, L.; De Petrillo, G.; Adriani, E.; Bonini, S.; Balsano, F.; Bonini, S. Serum levels of eosinophil cationic protein in allergic diseases and natural allergen exposure. J. Allergy Clin. Immunol. 1996, 97, 1350–1355. [Google Scholar] [CrossRef]
- Ueta, M.; Kinoshita, S. Ocular surface inflammation mediated by innate immunity. Eye Contact Lens 2010, 36, 269–281. [Google Scholar] [CrossRef] [PubMed]
- Abu El-Asrar, A.M.; Struyf, S.; Van Damme, J.; Geboes, K. Role of chemokines in vernal keratoconjunctivitis. Int. Ophthalmol. Clin. 2003, 43, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Abu el-Asrar, A.M.; Geboes, K.; Tabbara, K.F.; van den Oord, J.J.; Missotten, L. Immunopathogenesis of vernal keratoconjunctivitis. Bull. Soc. Belg. D’ophtalmol. 1996, 261, 15–24. [Google Scholar]
- Leonardi, A.; Tarricone, E.; Corrao, S.; Alaibac, M.; Corso, A.J.; Zavan, B.; Venier, P.; Conway de Macario, E.; Macario, A.J.; Di Stefano, A.; et al. Chaperone patterns in vernal keratoconjunctivitis are distinctive of cell and Hsp type and are modified by inflammatory stimuli. Allergy 2016, 71, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Akira, S.; Takeda, K.; Kaisho, T. Toll-like receptors: Critical proteins linking innate and acquired immunity. Nat. Immunol. 2001, 2, 675–680. [Google Scholar] [CrossRef] [PubMed]
- Baumann, C.L.; Aspalter, I.M.; Sharif, O.; Pichlmair, A.; Bluml, S.; Grebien, F.; Bruckner, M.; Pasierbek, P.; Aumayr, K.; Planyavsky, M.; et al. CD14 is a coreceptor of Toll-like receptors 7 and 9. J. Exp. Med. 2010, 207, 2689–2701. [Google Scholar] [CrossRef] [PubMed]
- Vercelli, D.; Baldini, M.; Stern, D.; Lohman, I.C.; Halonen, M.; Martinez, F. CD14: A bridge between innate immunity and adaptive IgE responses. J. Endotoxin Res. 2001, 7, 45–48. [Google Scholar] [CrossRef]
- Baldini, M.; Vercelli, D.; Martinez, F.D. CD14: An example of gene by environment interaction in allergic disease. Allergy 2002, 57, 188–192. [Google Scholar] [CrossRef]
- Leung, T.F.; Tang, N.L.; Wong, G.W.; Fok, T.F. CD14 and toll-like receptors: Potential contribution of genetic factors and mechanisms to inflammation and allergy. Curr. Drug Targets Inflamm. Allergy 2005, 4, 169–175. [Google Scholar] [CrossRef]
- Iovieno, A.; Lambiase, A.; Sacchetti, M.; Stampachiacchiere, B.; Micera, A.; Bonini, S. Preliminary evidence of the efficacy of probiotic eye-drop treatment in patients with vernal keratoconjunctivitis. Graefe’s Arch. Clin. Exp. Ophthalmol. 2008, 246, 435–441. [Google Scholar] [CrossRef]
- Leonardi, A.; Daull, P.; Garrigue, J.S.; Cavarzeran, F.; Docquier, M.; Di Stefano, A.; Tarricone, E.; Brun, P. Conjunctival transcriptome analysis reveals the overexpression of multiple pattern recognition receptors in vernal keratoconjunctivitis. Ocul. Surf. 2021, 19, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Zicari, A.M.; Zicari, A.; Nebbioso, M.; Mari, E.; Celani, C.; Lollobrigida, V.; Cesoni Marcelli, A.; Occasi, F.; Duse, M. High-mobility group box-1 (HMGB-1) and serum soluble receptor for advanced glycation end products (sRAGE) in children affected by vernal keratoconjunctivitis. Pediatr. Allergy Immunol. 2014, 25, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Caputo, R.; Pasti, M.; de Libero, C.; Mori, F.; Barni, S.; Danti, G.; Buonvicino, D.; Urru, M.; Chiarugi, A.; Pucci, N. Increased Lacrimal Fluid Level of HMGB1 in Vernal Keratoconjunctivitis. Ocul. Immunol. Inflamm. 2019, 27, 808–812. [Google Scholar] [CrossRef] [PubMed]
- Feijen, M.; Gerritsen, J.; Postma, D.S. Genetics of allergic disease. Br. Med Bull. 2000, 56, 894–907. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, A.; Campbell-Meltzer, R.S.; Chute, K.; Orrell, J.; Ono, S.J. Genetics of allergic disease: Evidence for organ-specific susceptibility genes. Int. Arch. Allergy Immunol. 2001, 124, 197–200. [Google Scholar] [CrossRef]
- Tesse, R.; Spadavecchia, L.; Fanelli, P.; Paglialunga, C.; Capozza, M.; Favoino, B.; Armenio, L.; Cavallo, L. New insights into childhood Vernal keratoconjunctivitis-associated factors. Pediatr. Allergy Immunol. 2012, 23, 682–685. [Google Scholar] [CrossRef]
- Bonini, S.; Bonini, S.; Lambiase, A.; Magrini, L.; Rumi, C.; Del Prete, G.; Schiavone, M.; Rotiroti, G.; Onorati, P.; Rutella, S. Vernal keratoconjunctivitis: A model of 5q cytokine gene cluster disease. Int. Arch. Allergy Immunol. 1995, 107, 95–98. [Google Scholar] [CrossRef]
- Zicari, A.M.; Mora, B.; Lollobrigida, V.; Occasi, F.; Cesoni Marcelli, A.; Megiorni, F.; Pizzuti, A.; Nebbioso, M.; Duse, M. Immunogenetic investigation in vernal keratoconjunctivitis. Pediatr. Allergy Immunol. 2014, 25, 508–510. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, W.N.; Insler, M.S. Vernal keratoconjunctivitis: New corneal findings in fraternal twins. Cornea 1984, 3, 288–290. [Google Scholar] [CrossRef]
- Artesani, M.C.; Esposito, M.; Mennini, M.; Andreani, M.; Locatelli, F.; Buzzonetti, L.; Fiocchi, A. Vernal keratoconjunctivitis in twins: Case report and literature review. Ital. J. Pediatr. 2021, 47, 136. [Google Scholar] [CrossRef]
- Motterle, L.; Diebold, Y.; Enriquez de Salamanca, A.; Saez, V.; Garcia-Vazquez, C.; Stern, M.E.; Calonge, M.; Leonardi, A. Altered expression of neurotransmitter receptors and neuromediators in vernal keratoconjunctivitis. Arch. Ophthalmol. 2006, 124, 462–468. [Google Scholar] [CrossRef]
- Sacchetti, M.; Bruscolini, A.; Lambiase, A. Neurotrophic factors and nerve growth factor in ocular allergy. Curr. Opin. Allergy Clin. Immunol. 2019, 19, 510–516. [Google Scholar] [CrossRef]
- Nassenstein, C.; Braun, A.; Erpenbeck, V.J.; Lommatzsch, M.; Schmidt, S.; Krug, N.; Luttmann, W.; Renz, H.; Virchow, J.C., Jr. The neurotrophins nerve growth factor, brain-derived neurotrophic factor, neurotrophin-3, and neurotrophin-4 are survival and activation factors for eosinophils in patients with allergic bronchial asthma. J. Exp. Med. 2003, 198, 455–467. [Google Scholar] [CrossRef]
- Mantelli, F.; Micera, A.; Sacchetti, M.; Bonini, S. Neurogenic inflammation of the ocular surface. Curr. Opin. Allergy Clin. Immunol. 2010, 10, 498–504. [Google Scholar] [CrossRef]
- Bonini, S.; Rasi, G.; Brusasco, V.; Carlsen, K.H.; Crimi, E.; Popov, T.; Schultze-Werninghaus, G.; Gramiccioni, C.; Bonini, M.; Passali, D.; et al. Nonspecific provocation of target organs in allergic diseases: EAACI-GA(2)LEN consensus report. Allergy 2007, 62, 683–694. [Google Scholar] [CrossRef] [PubMed]
- Sacchetti, M.; Micera, A.; Lambiase, A.; Speranza, S.; Mantelli, F.; Petrachi, G.; Bonini, S.; Bonini, S. Tear levels of neuropeptides increase after specific allergen challenge in allergic conjunctivitis. Mol. Vis. 2011, 17, 47–52. [Google Scholar]
- Fujishima, H.; Takeyama, M.; Takeuchi, T.; Saito, I.; Tsubota, K. Elevated levels of substance P in tears of patients with allergic conjunctivitis and vernal keratoconjunctivitis. Clin. Exp. Allergy J. Br. Soc. Allergy Clin. Immunol. 1997, 27, 372–378. [Google Scholar] [CrossRef]
- Lambiase, A.; Bonini, S.; Micera, A.; Tirassa, P.; Magrini, L.; Bonini, S.; Aloe, L. Increased plasma levels of substance P in vernal keratoconjunctivitis. Investig. Ophthalmol. Vis. Sci. 1997, 38, 2161–2164. [Google Scholar]
- Sacchetti, M.; Segatto, M.; Bruscolini, A.; Abicca, I.; Cavaliere, C.; Lambiase, A. Changes of NGF pathway in allergic rhinoconjunctivitis: A conjunctival allergen challenge study. Allergy 2019, 74, 605–607. [Google Scholar] [CrossRef]
- Bonini, S.; Lambiase, A.; Bonini, S.; Angelucci, F.; Magrini, L.; Manni, L.; Aloe, L. Circulating nerve growth factor levels are increased in humans with allergic diseases and asthma. Proc. Natl. Acad. Sci. USA 1996, 93, 10955–10960. [Google Scholar] [CrossRef] [PubMed]
- Lambiase, A.; Bonini, S.; Micera, A.; Rama, P.; Bonini, S.; Aloe, L. Expression of nerve growth factor receptors on the ocular surface in healthy subjects and during manifestation of inflammatory diseases. Investig. Ophthalmol. Vis. Sci. 1998, 39, 1272–1275. [Google Scholar]
- Lambiase, A.; Bonini, S.; Bonini, S.; Micera, A.; Magrini, L.; Bracci-Laudiero, L.; Aloe, L. Increased plasma levels of nerve growth factor in vernal keratoconjunctivitis and relationship to conjunctival mast cells. Investig. Ophthalmol. Vis. Sci. 1995, 36, 2127–2132. [Google Scholar]
- Sanico, A.M.; Koliatsos, V.E.; Stanisz, A.M.; Bienenstock, J.; Togias, A. Neural hyperresponsiveness and nerve growth factor in allergic rhinitis. Int. Arch. Allergy Immunol. 1999, 118, 154–158. [Google Scholar] [CrossRef]
- Micera, A.; Lambiase, A.; Stampachiacchiere, B.; Sgrulletta, R.; Normando, E.M.; Bonini, S.; Bonini, S. Nerve growth factor has a modulatory role on human primary fibroblast cultures derived from vernal keratoconjunctivitis-affected conjunctiva. Mol. Vis. 2007, 13, 981–987. [Google Scholar]
- Nebbioso, M.; Zicari, A.M.; Celani, C.; Lollobrigida, V.; Grenga, R.; Duse, M. Pathogenesis of Vernal Keratoconjunctivitis and Associated Factors. Semin. Ophthalmol. 2015, 30, 340–344. [Google Scholar] [CrossRef]
- Chen, W.; Mempel, M.; Schober, W.; Behrendt, H.; Ring, J. Gender difference, sex hormones, and immediate type hypersensitivity reactions. Allergy 2008, 63, 1418–1427. [Google Scholar] [CrossRef] [PubMed]
- Sacchetti, M.; Lambiase, A.; Moretti, C.; Mantelli, F.; Bonini, S. Sex hormones in allergic conjunctivitis: Altered levels of circulating androgens and estrogens in children and adolescents with vernal keratoconjunctivitis. J. Immunol. Res. 2015, 2015, 945317. [Google Scholar] [CrossRef] [PubMed]
- Di Zazzo, A.; Micera, A.; De Piano, M.; Coassin, M.; Sharma, S.; Bonini, S.; Fernandes, M. Adult Vernal Keratoconjunctivitis: Clinical and biochemical profile of a rare disease. Ocul. Surf. 2019, 17, 737–742. [Google Scholar] [CrossRef]
- Cutolo, M.; Seriolo, B.; Villaggio, B.; Pizzorni, C.; Craviotto, C.; Sulli, A. Androgens and estrogens modulate the immune and inflammatory responses in rheumatoid arthritis. Ann. N. Y. Acad. Sci. 2002, 966, 131–142. [Google Scholar] [CrossRef] [PubMed]
- Bonini, S.; Lambiase, A.; Schiavone, M.; Centofanti, M.; Palma, L.A.; Bonini, S. Estrogen and progesterone receptors in vernal keratoconjunctivitis. Ophthalmology 1995, 102, 1374–1379. [Google Scholar] [CrossRef]
- Zicari, A.M.; Nebbioso, M.; Lollobrigida, V.; Bardanzellu, F.; Celani, C.; Occasi, F.; Cesoni Marcelli, A.; Duse, M. Vernal keratoconjunctivitis: Atopy and autoimmunity. Eur. Rev. Med. Pharmacol. Sci. 2013, 17, 1419–1423. [Google Scholar] [PubMed]
- Stagi, S.; Pucci, N.; Di Grande, L.; de Libero, C.; Caputo, R.; Pantano, S.; Mattei, I.; Mori, F.; de Martino, M.; Novembre, E. Increased incidence of thyroid dysfunction and autoimmunity in patients with vernal keratoconjunctivitis. Int. J. Endocrinol. 2014, 2014, 804870. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sacchetti, M.; Plateroti, R.; Bruscolini, A.; Giustolisi, R.; Marenco, M. Understanding Vernal Keratoconjunctivitis: Beyond Allergic Mechanisms. Life 2021, 11, 1012. https://doi.org/10.3390/life11101012
Sacchetti M, Plateroti R, Bruscolini A, Giustolisi R, Marenco M. Understanding Vernal Keratoconjunctivitis: Beyond Allergic Mechanisms. Life. 2021; 11(10):1012. https://doi.org/10.3390/life11101012
Chicago/Turabian StyleSacchetti, Marta, Rocco Plateroti, Alice Bruscolini, Rosalia Giustolisi, and Marco Marenco. 2021. "Understanding Vernal Keratoconjunctivitis: Beyond Allergic Mechanisms" Life 11, no. 10: 1012. https://doi.org/10.3390/life11101012
APA StyleSacchetti, M., Plateroti, R., Bruscolini, A., Giustolisi, R., & Marenco, M. (2021). Understanding Vernal Keratoconjunctivitis: Beyond Allergic Mechanisms. Life, 11(10), 1012. https://doi.org/10.3390/life11101012