
A Mirror Bilateral Neuro-Rehabilitation Robot System with the sEMG-Based Real-Time Patient Active Participant Assessment

Abstract
:1. Introduction
2. Mirror Bilateral Neuro-Rehabilitation System Overall
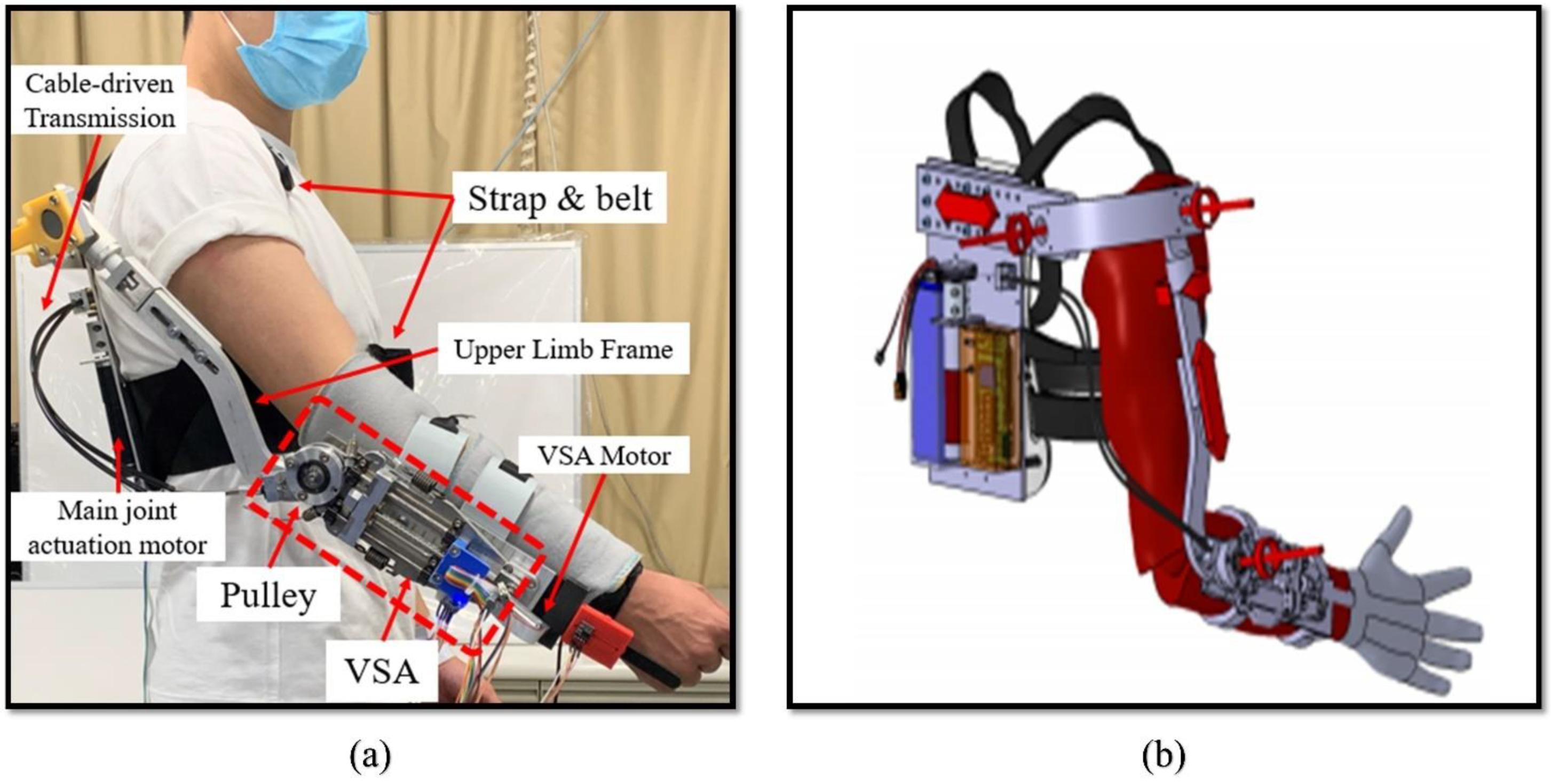
2.1. PVSED Hardware
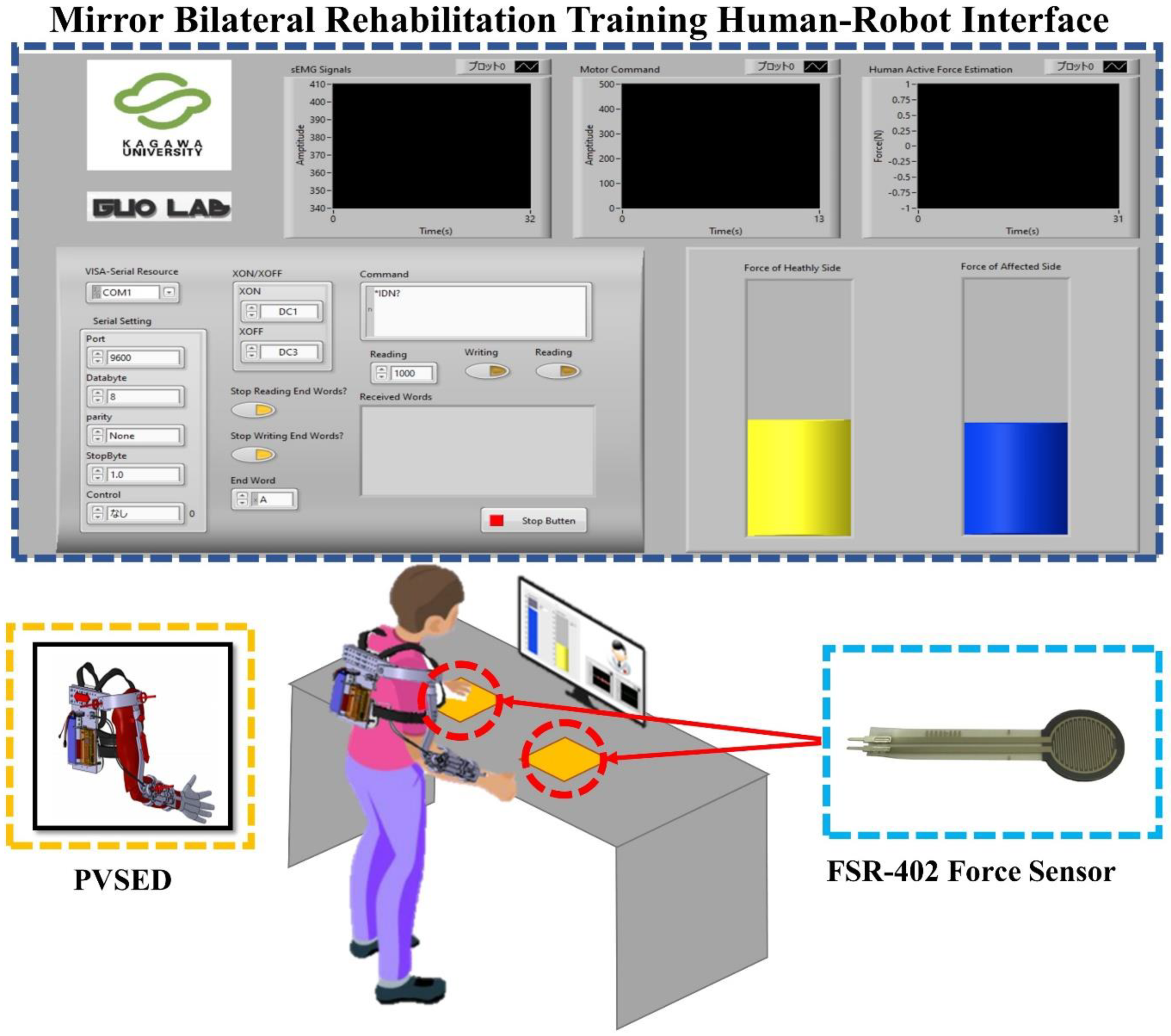
2.2. Mirror Visual Feedback-Based Human-Robot Interface
2.3. The Mirror Bilateral Training Protocol of Upper Limb Elbow Joint
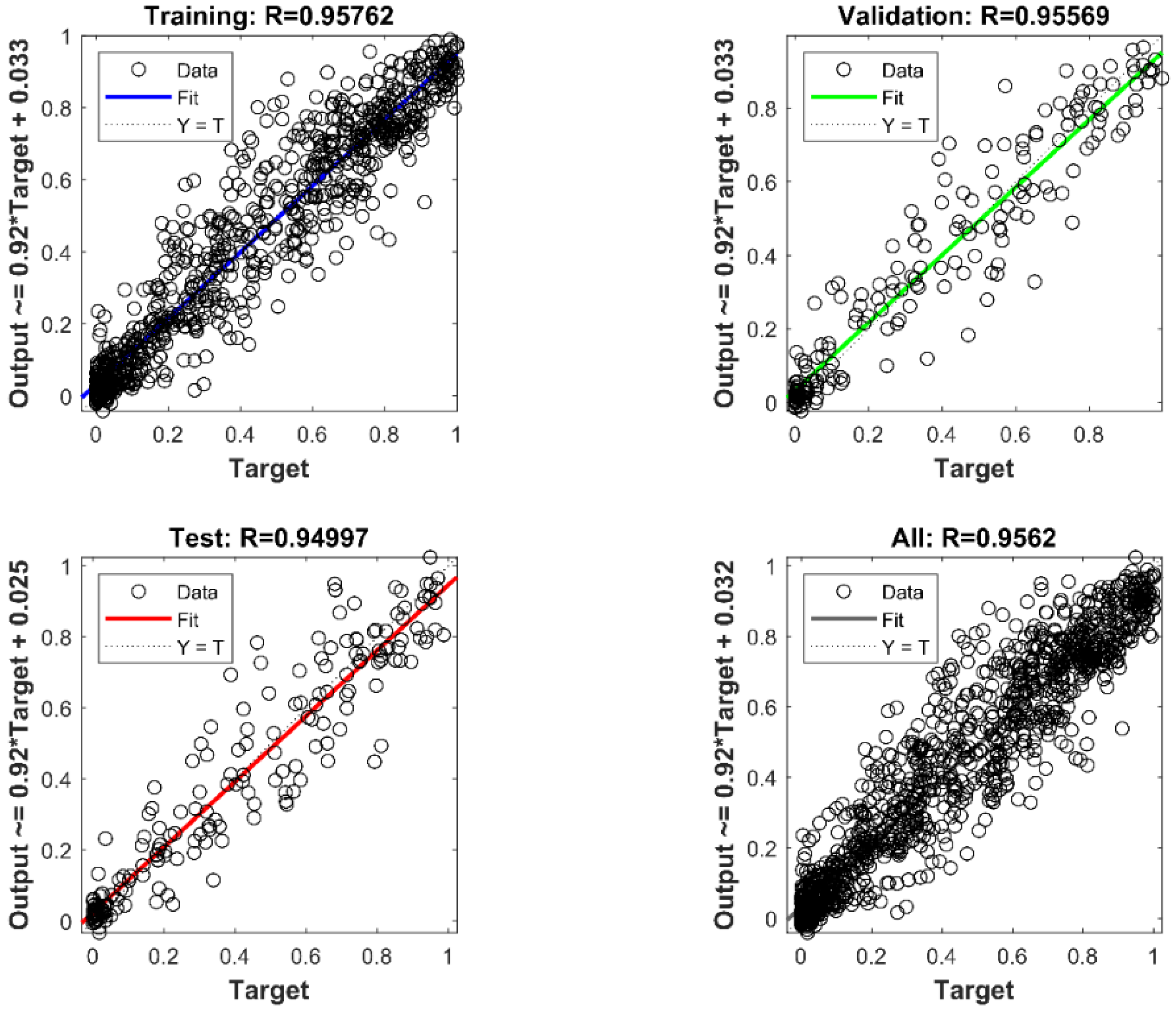
3. sEMG-Based Isometric Active Force Estimation
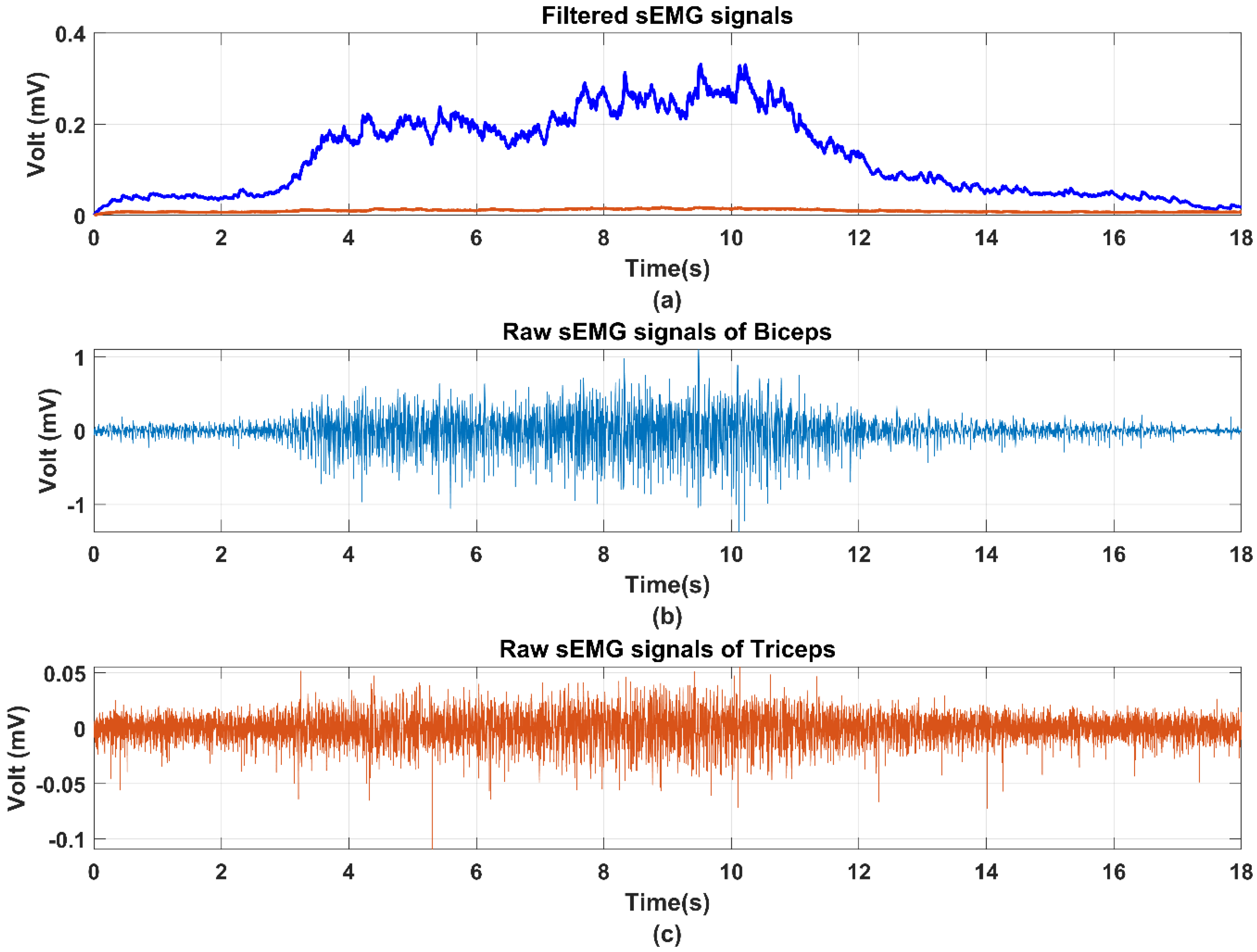
3.1. sEMG Signal Processing
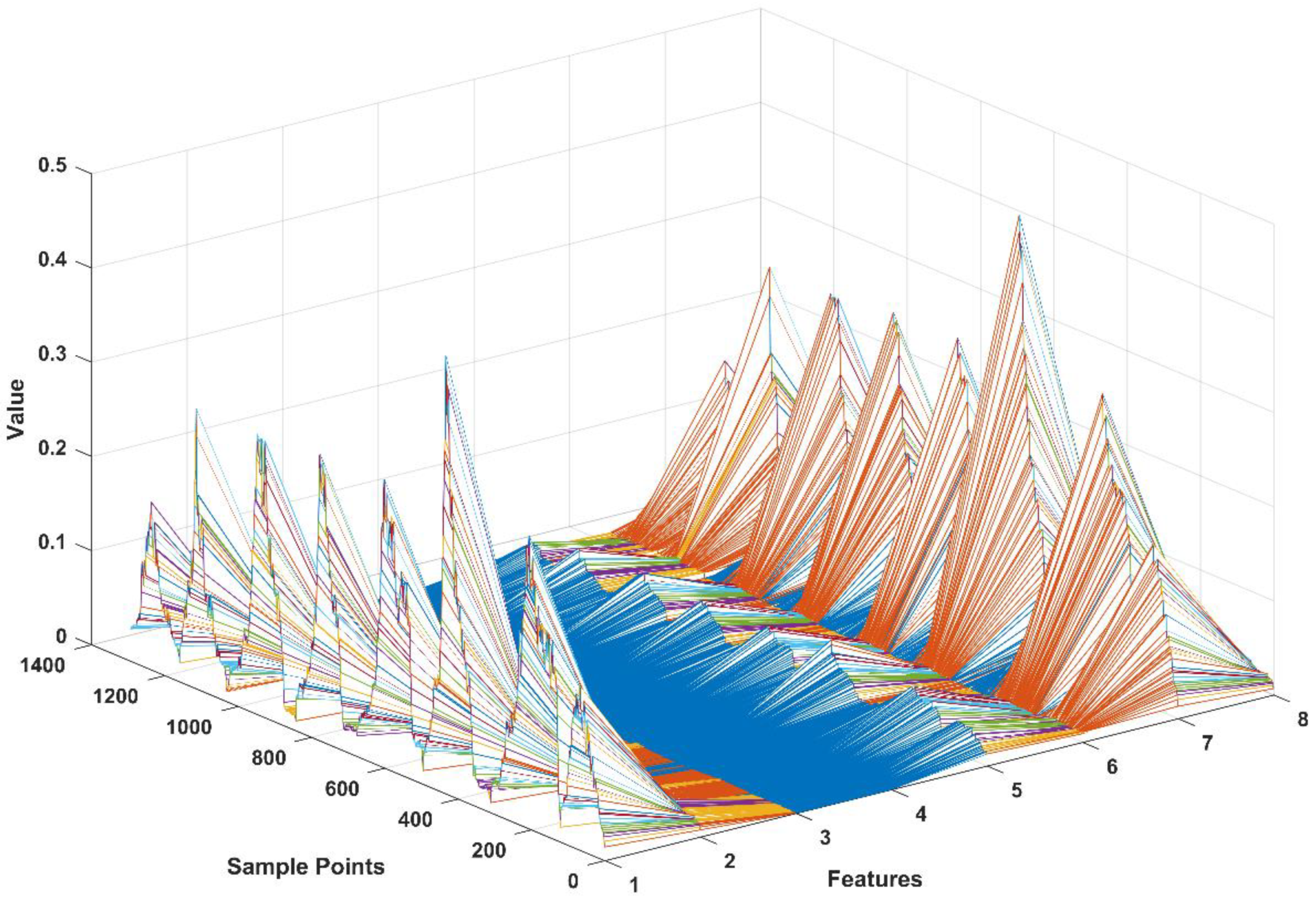
3.2. Feature Extraction
3.3. BPNN
4. Mirror Bilateral Control for Bilateral Limb Coordination
5. Experimental Setup and Results
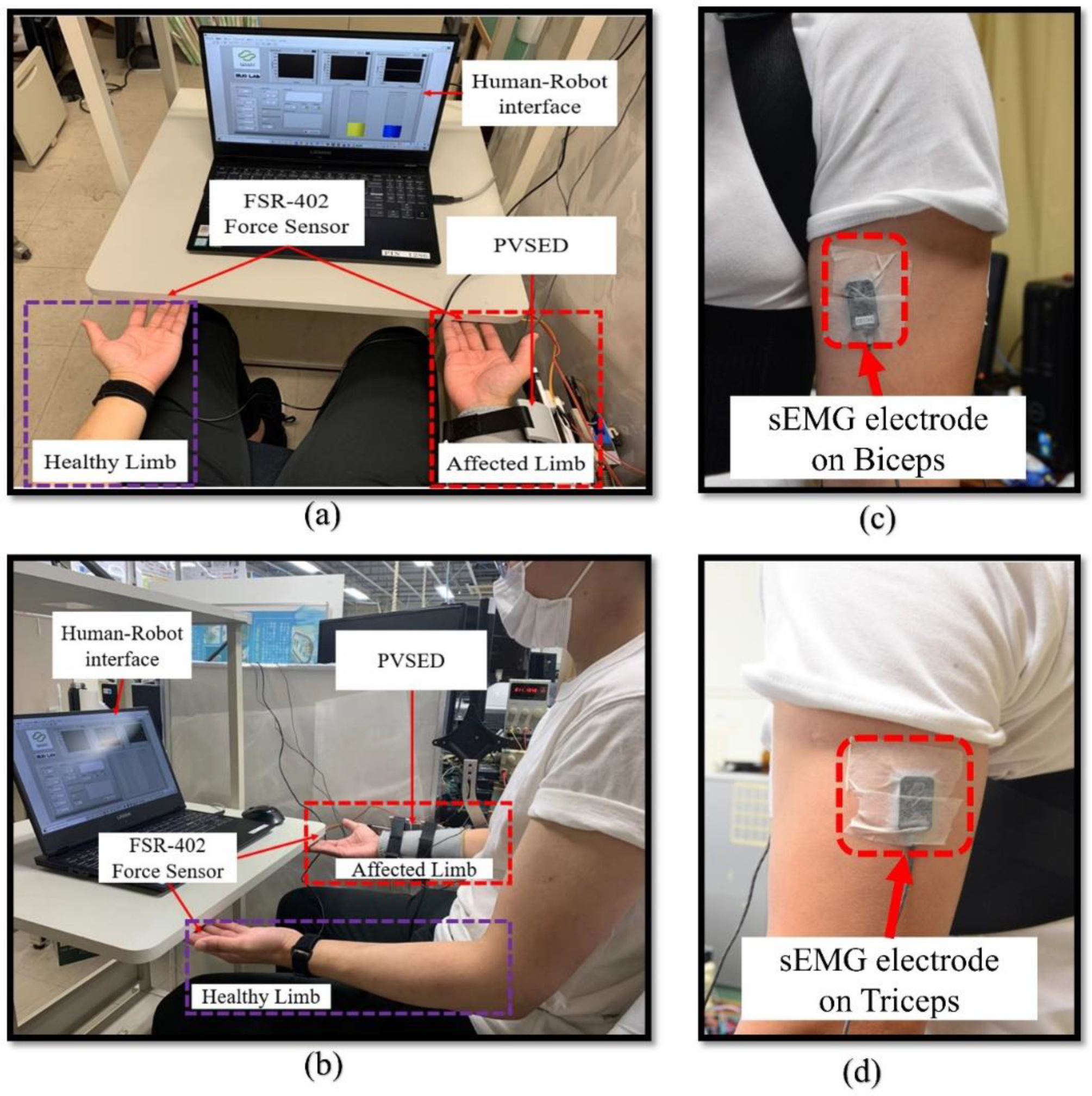
5.1. Experimental Setup
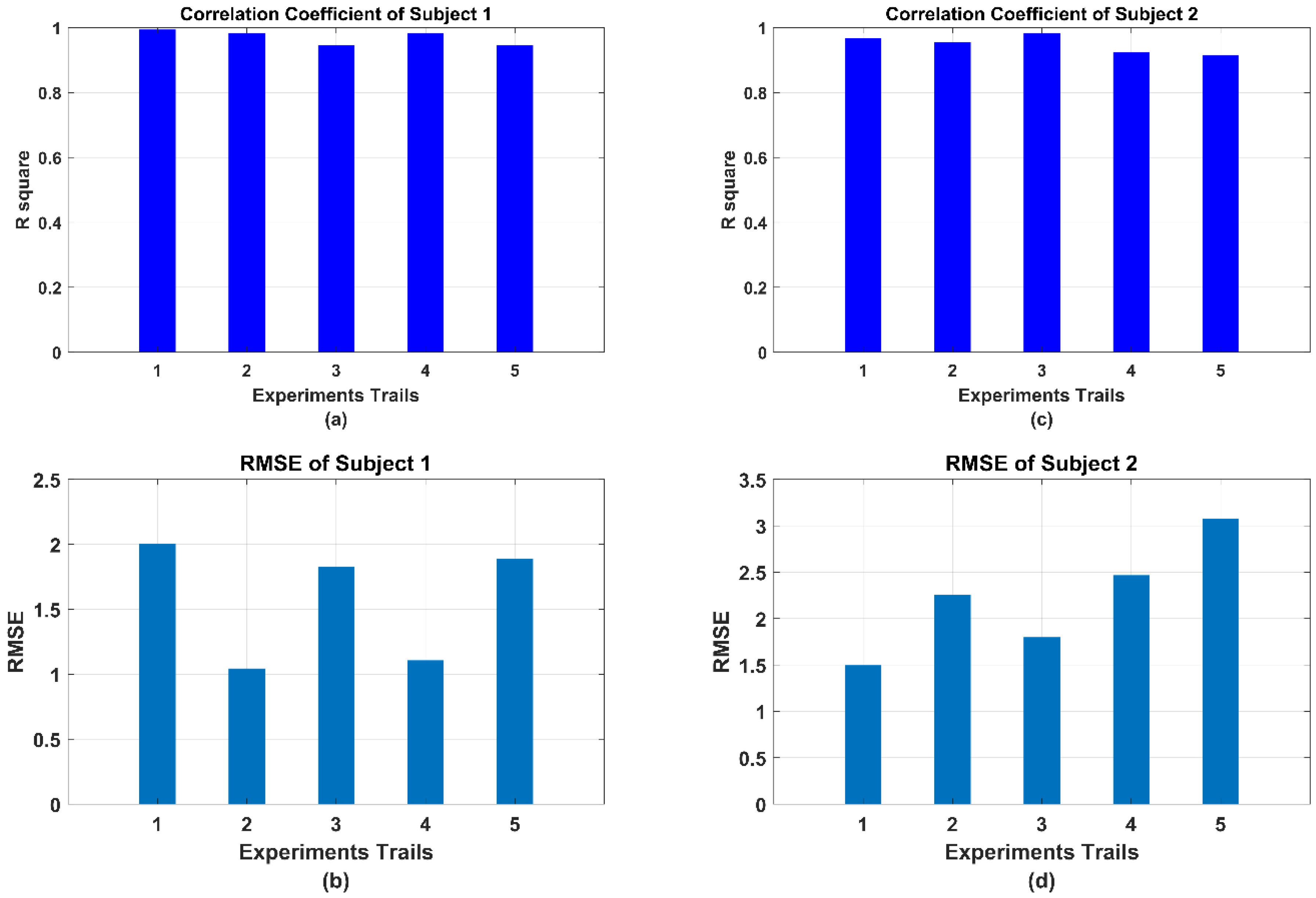
5.2. Experimental Results
6. Discussion
6.1. Comparison of the sEMG-Based Active Force Estimation with the State-of-Art
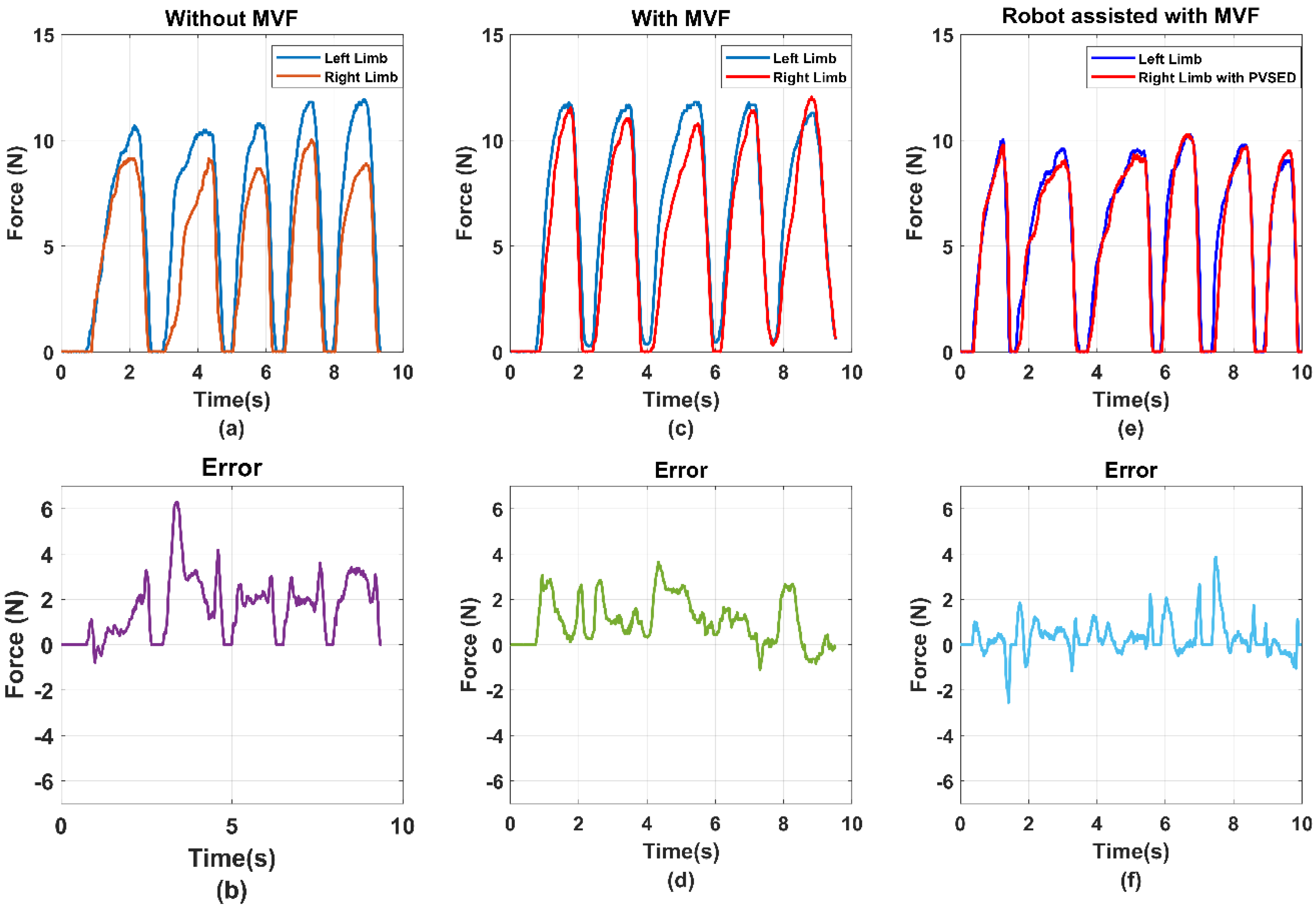
6.2. Analysis of the Efficiency of the MVF to the Bilateral Rehabilitation
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Piscitelli, D.; Turpin, N.A.; Subramanian, S.; Feldman, A.G.; Levin, M.F. Deficits in corticospinal control of stretch reflex thresholds in stroke: Implications for motor impairment. Clin. Neurophysiol. 2020, 131, 2067–2078. [Google Scholar] [CrossRef]
- Kim, R.K.; Kang, N. Bimanual Coordination Functions between Paretic and Nonparetic Arms: A Systematic Review and Meta-analysis. J. Stroke Cerebrovasc. Dis. 2020, 29, 104544. [Google Scholar] [CrossRef]
- Wu, J.; Cheng, H.; Zhang, J.; Bai, Z.; Cai, S. The modulatory effects of bilateral arm training (BAT) on the brain in stroke patients: A systematic review. Neurol. Sci. 2021, 42, 501–511. [Google Scholar] [CrossRef]
- Deconinck, F.J.A.; Smorenburg, A.R.P.; Benham, A.; Ledebt, A.; Feltham, M.G.; Savelsbergh, G.J.P. Reflections on mirror therapy: A systematic review of the effect of mirror visual feedback on the brain. Neurorehabilit. Neural Repair 2015, 29, 349–361. [Google Scholar] [CrossRef] [Green Version]
- Nojima, I.; Mima, T.; Koganemaru, S.; Thabit, M.N.; Fukuyama, H.; Kawamata, T. Human motor plasticity induced by mirror visual feedback. J. Neurosci. 2012, 32, 1293–1300. [Google Scholar] [CrossRef] [Green Version]
- Krebs, H.I. Twenty + years of robotics for upper-extremity rehabilitation following a stroke. Rehabil. Robot. 2018, 175–192. [Google Scholar]
- Bao, G.; Pan, L.; Fang, H.; Wu, X.; Yu, H. Academic Review and Perspectives on Robotic Exoskeletons. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 2294–2304. [Google Scholar] [CrossRef]
- Leonardis, D.; Chisari, C.; Bergamasco, M.; Frisoli, A.; Barsotti, M.; Loconsole, C.; Solazzi, M.; Troncossi, M.; Mazzotti, C.; Castelli, V.P.; et al. An EMG-controlled robotic hand exoskeleton for bilateral rehabilitation. IEEE Trans. Haptics 2015, 8, 140–151. [Google Scholar] [CrossRef] [PubMed]
- Gasser, B.W.; Martinez, A.; Sasso-Lance, E.; Kandilakis, C.; Durrough, C.M.; Goldfarb, M. Preliminary Assessment of a Hand and Arm Exoskeleton for Enabling Bimanual Tasks for Individuals with Hemiparesis. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 2214–2223. [Google Scholar] [CrossRef] [PubMed]
- Miao, Q.; Peng, Y.; Liu, L.; McDaid, A.; Zhang, M. Subject-specific compliance control of an upper-limb bilateral robotic system. Robot. Auton. Syst. 2020, 126, 103478. [Google Scholar] [CrossRef]
- Song, Z.; Guo, S.; Xiao, N.; Gao, B.; Shi, L. Implementation of human-machine synchronization control for active rehabilitation using an inertia sensor. Sensors 2012, 12, 16046–16059. [Google Scholar] [CrossRef]
- Song, Z.; Guo, S.; Pang, M.; Zhang, S.; Xiao, N.; Gao, B.; Shi, L. Implementation of resistance training using an upper-limb exoskeleton rehabilitation device for elbow joint. J. Med. Biol. Eng. 2014, 34, 188–196. [Google Scholar] [CrossRef]
- Zhang, S.; Guo, S.; Pang, M.; Gao, B.; Guo, P. Mechanical Design and Control Method for SEA and VSA-based Exoskeleton Devices for Elbow Joint Rehabilitation. Neurosci. Biomed. Eng. 2015, 2, 142–147. [Google Scholar] [CrossRef] [Green Version]
- Zhang, S.; Guo, S.; Fu, Y.; Boulardou, L.; Huang, Q.; Hirata, H.; Ishihara, H. Integrating Compliant Actuator and Torque Limiter Mechanism for Safe Home-Based Upper-Limb Rehabilitation Device Design. J. Med. Biol. Eng. 2017, 37, 357–364. [Google Scholar] [CrossRef]
- Zhang, S.; Guo, S.; Gao, B.; Huang, Q.; Pang, M.; Hirata, H.; Ishihara, H. Muscle strength assessment system using sEMG-based force prediction method for wrist joint. J. Med. Biol. Eng. 2016, 36, 121–131. [Google Scholar] [CrossRef]
- Bi, L.; Feleke, A.; Guan, C. A review on EMG-based motor intention prediction of continuous human upper limb motion for human-robot collaboration. Biomed. Signal Process. Control. 2019, 51, 113–127. [Google Scholar] [CrossRef]
- Guo, S.; Yang, Z.; Liu, Y. EMG-based Continuous Prediction of the Upper Limb Elbow Joint Angle Using GRNN. In Proceedings of the 2019 IEEE International Conference on Mechatronics and Automation (ICMA), Tianjin, China, 4–7 August 2019; pp. 2168–2173. [Google Scholar]
- Yang, Z.; Guo, S.; Liu, Y.; Hirata, H.; Tamiya, T. An intention-based online bilateral training system for upper limb motor rehabilitation. Microsyst. Technol. 2021, 27, 211–222. [Google Scholar] [CrossRef]
- Toledo-Perez, D.C.; Rodriguez-Resendiz, J.; Gomez-Loenzo, R.A. A Study of Computing Zero Crossing Methods and an Improved Proposal for EMG Signals. IEEE Access 2020, 8, 8783–8790. [Google Scholar] [CrossRef]
- Toledo-Pérez, D.C.; Martínez-Prado, M.A.; Gómez-Loenzo, R.A.; Paredes-García, W.J.; Rodríguez-Reséndiz, J. A Study of Movement Classification of the Lower Limb Based on up to 4-EMG Channels. Electronics 2019, 8, 259. [Google Scholar] [CrossRef] [Green Version]
- Toledo-Pérez, D.C.; Rodríguez-Reséndiz, J.; Gómez-Loenzo, R.A.; Jauregui-Correa, J.C. Support Vector Machine-Based EMG Signal Classification Techniques: A Review. Appl. Sci. 2019, 9, 4402. [Google Scholar] [CrossRef] [Green Version]
- Jiang, N.; Dosen, S.; Mueller, K.-R.; Farina, D. Myoelectric control of artificial limbs—Is there a need to change focus? [In the Spotlight]. IEEE Signal Process. Mag. 2012, 29, 150–152. [Google Scholar] [CrossRef]
- Paskett, D.; Olsen, R.; George, A.; Kluger, T.; Brinton, R.; Davis, S.; Duncan, C.; Clark, A. A Modular Transradial Bypass Socket for Surface Myoelectric Prosthetic Control in Non-Amputees. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 2070–2076. [Google Scholar] [CrossRef] [Green Version]
- Krasoulis, A.; Vijayakumar, S.; Nazarpour, K. Multi-grip classification-based prosthesis control with two sensors. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 508–518. [Google Scholar] [CrossRef] [PubMed]
- McDonald, C.G.; Sullivan, J.L.; Dennis, T.A.; O’Malley, M.K. A Myoelectric Control Interface for Upper-Limb Robotic Rehabilitation Following Spinal Cord Injury. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 978–987. [Google Scholar] [CrossRef]
- Robertson, J.W.; Englehart, K.B.; Member, S.; Erik, J. Effects of Confidence-Based Rejection on Usability and Error in Pattern Recognition- Based Myoelectric Control. IEEE J. Biomed. Health Inform. 2019, 23, 2002–2008. [Google Scholar] [CrossRef] [PubMed]
- Teramae, T.; Noda, T.; Morimoto, J. EMG-Based Model Predictive Control for Physical Human–Robot Interaction: Application for Assist-As-Needed Control. IEEE Robot. Autom. Lett. 2018, 3, 210–217. [Google Scholar] [CrossRef]
- Warraich, Z.; Kleim, J.A. Neural plasticity: The biological substrate for neurorehabilitation. PM&R 2010, 2, S208–S219. [Google Scholar]
- Sun, W.; Zhu, J.; Jiang, Y.; Yokoi, H.; Huang, Q. One-Channel Surface Electromyography Decomposition for Muscle Force Estimation. Front. Neurorobotics 2018, 12, 20. [Google Scholar] [CrossRef] [PubMed]
- Zonnino, A.; Sergi, F. Model-based estimation of individual muscle force based on measurements of muscle activity in forearm muscles during isometric tasks. IEEE Trans. Biomed. Eng. 2020, 67, 134–145. [Google Scholar] [CrossRef]
- Building, B.; Member, S.; Campus, S.K. Deep Learning for Musculoskeletal Force Prediction. Ann. Biomed. Eng. 2018, 47, 778–789. [Google Scholar]
- Ai, Q.; Liu, Z.; Meng, W.; Liu, Q.; Xie, S.Q. Machine Learning in Robot Assisted Upper Limb Rehabilitation: A Focused Review. IEEE Trans. Cogn. Dev. Syst. 2021. [Google Scholar] [CrossRef]
- Yang, Z.; Guo, S.; Liu, Y. Comparison of Isometric Force Estimation Methods for Upper Limb Elbow Joints. In Proceedings of the 2020 IEEE International Conference on Mechatronics and Automation (ICMA), Beijing, China, 13–16 October 2020; pp. 1558–1563. [Google Scholar]
- Liu, Y.; Guo, S.; Hirata, H.; Ishihara, H.; Tamiya, T. Development of a powered variable-stiffness exoskeleton device for elbow rehabilitation. Biomed. Microdevices 2018, 20, 64. [Google Scholar] [CrossRef] [PubMed]
- Sekhavat, Y.A.; Namani, M.S. Projection-Based AR: Effective Visual Feedback in Gait Rehabilitation. IEEE Trans. Hum.-Mach. Syst. 2018, 48, 626–636. [Google Scholar] [CrossRef]
- Yang, Z.; Guo, S.; Liu, Y. Preliminary Evaluation of a Performance-based Stiffness Control for Upper Limb Elbow Joints Rehabilitation. In Proceedings of the 2021 IEEE International Conference on Mechatronics and Automation (ICMA), Takamatsu, Japan, 8–11 August 2021; pp. 1280–1285. [Google Scholar]
- Hajian, G.; Etemad, A.; Morin, E. Generalized EMG-based isometric contact force estimation using a deep learning approach. Biomed. Signal Process. Control. 2021, 70, 103012. [Google Scholar] [CrossRef]
- Zhang, C.; Chen, X.; Cao, S.; Zhang, X.; Chen, X. A Novel HD-sEMG Preprocessing Method Integrating Muscle Activation Heterogeneity Analysis and Kurtosis-Guided Filtering for High-Accuracy Joint Force Estimation. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 1920–1930. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Feature | Equation | Description |
|---|---|---|
| Mean absolute value (MAV) | The average of absolute value of the EMG signals amplitude in a segment | |
| Root mean square (RMS) | The measure of power of the EMG signals which can be calculated as the amplitude modulated Gaussian random process | |
| Difference absolute standard deviation value (DASDV) | The standard deviation absolute value of the difference between the adjacent samples of EMG signals | |
| Wavelength (WL) | The measure of complexity of the EMG signals which defined s cumulative length of the EMG waveform over the time segment |
| Research | Joints | EMG Channels | Features | Model | Other Sensors | Results |
|---|---|---|---|---|---|---|
| Zhang [15] | Wrist | 4 | Muscle activation | ANN and Prediction Function | MTx sensor | : 0.9085 |
| Hajian [37] | Elbow | 21 | Temporal and Spectral information (16 in total) | Deep convolutional neural networks | no | NMSE: 1.60 ± 3.69 |
| Zhang [38] | Elbow | 128 | Principal component analysis (PCA) and Heterogeneity information | Optimal Principal Component Selection and kurtosis-guided filter | no | 0.877~0.955 |
| This work | Elbow | 2 | MAV, RMS, DADSV, WL | BPNN | no | 0.9562 RMSE: 1.8935 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, Z.; Guo, S.; Hirata, H.; Kawanishi, M. A Mirror Bilateral Neuro-Rehabilitation Robot System with the sEMG-Based Real-Time Patient Active Participant Assessment. Life 2021, 11, 1290. https://doi.org/10.3390/life11121290
Yang Z, Guo S, Hirata H, Kawanishi M. A Mirror Bilateral Neuro-Rehabilitation Robot System with the sEMG-Based Real-Time Patient Active Participant Assessment. Life. 2021; 11(12):1290. https://doi.org/10.3390/life11121290
Chicago/Turabian StyleYang, Ziyi, Shuxiang Guo, Hideyuki Hirata, and Masahiko Kawanishi. 2021. "A Mirror Bilateral Neuro-Rehabilitation Robot System with the sEMG-Based Real-Time Patient Active Participant Assessment" Life 11, no. 12: 1290. https://doi.org/10.3390/life11121290