T2-high Asthma, Classified by Sputum mRNA Expression of IL4, IL5, and IL13, is Characterized by Eosinophilia and Severe Phenotype



Abstract
:1. Introduction
2. Results
2.1. Higher IL4, IL5, and IL13 mRNA Expression in Induced Sputum Cells of Asthmatic Patients
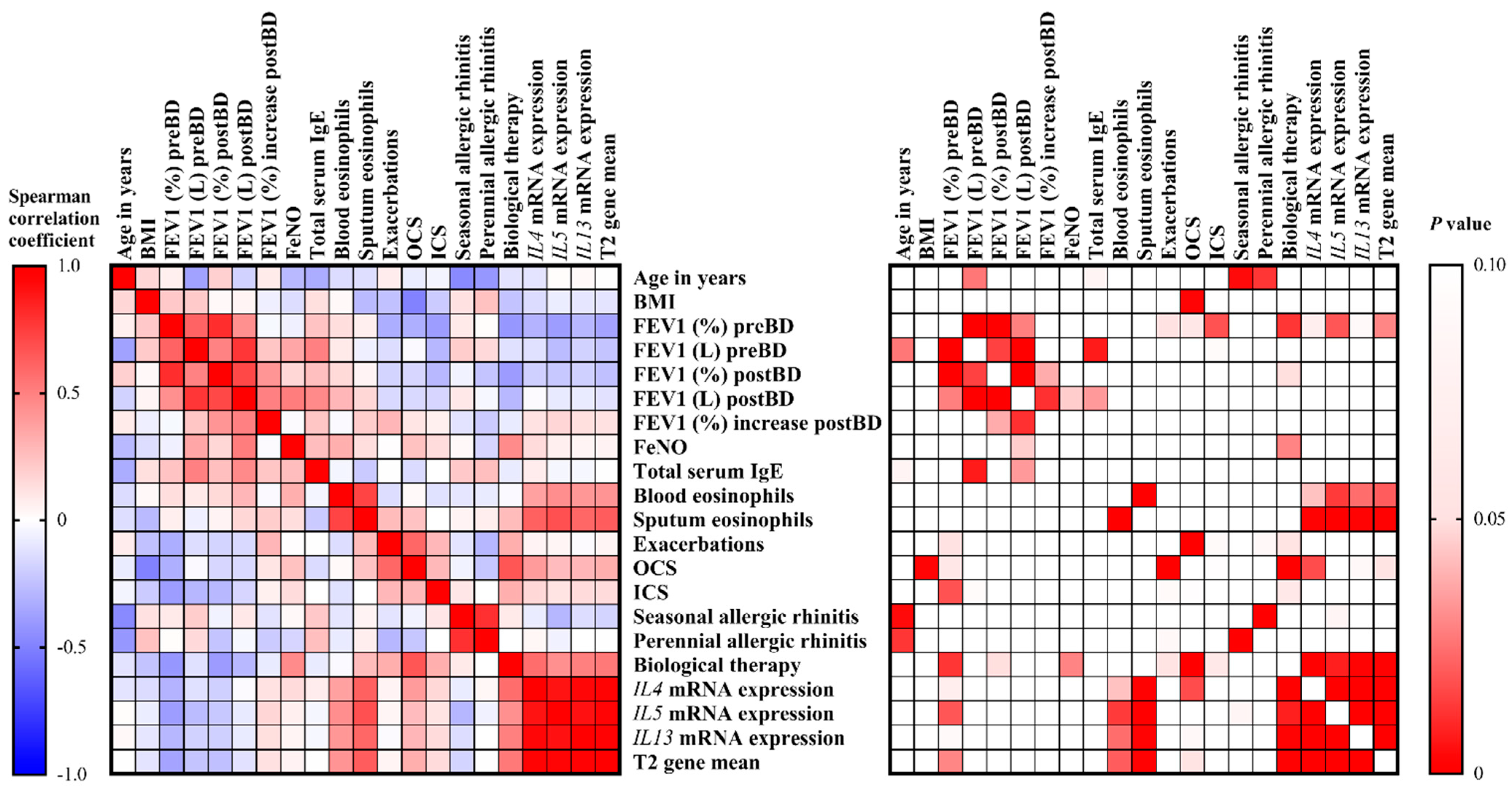
2.2. T2-High Asthma is Characterized by Eosinophilia and Severe, Difficult-to-Treat Asthma
3. Discussion
4. Materials and Methods
4.1. Study Subjects
4.2. Sputum Collection and Processing
4.3. RNA Isolation and Gene Expression
4.4. Statistical Analyses
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BMI | Body mass index |
| FEV1 | Forced expiratory volume in 1 s |
| FeNO | Exhaled nitric oxide |
| ICS | Inhaled corticosteroids |
| LABA | Long-acting beta-agonists |
| preBD | Pre-bronchodilation |
| postBD | Post-bronchodilation |
| OCS | Oral corticosteroids |
| RT-qPCR | Quantitative reverse transcription PCR |
References
- Global Initiative for Asthma: Global Strategy for Asthma Management and Prevention. Updated 2020. Available online: www.ginasthma.org (accessed on 2 November 2020).
- Peters, S.P.; Busse, W.W. New and Anticipated Therapies for Severe Asthma. J. Allergy Clin. Immunol. Pract. 2017, 5, S15–S24. [Google Scholar] [CrossRef] [PubMed]
- Custovic, A.; Henderson, J.; Simpson, A. Does Understanding Endotypes Translate to Better Asthma Management Options for All? J. Allergy Clin. Immunol. 2019, 144, 25–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fricker, M.; Gibson, P.G.; Powell, H.; Simpson, J.L.; Yang, I.A.; Upham, J.W.; Reynolds, P.N.; Hodge, S.; James, A.L.; Jenkins, C.; et al. A Sputum 6-Gene Signature Predicts Future Exacerbations of Poorly Controlled Asthma. J. Allergy Clin. Immunol. 2019, 144, 51–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, M.C.; Mekonnen, Z.K.; Yuan, S.; Bhakta, N.R.; Woodruff, P.G.; Fahy, J.V. Measures of gene expression in sputum cells can identify TH2-high and TH2-low subtypes of asthma. J. Allergy Clin. Immunol. 2014, 133, 388–394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nanzer, A.M.; Menzies-Gow, A. Defining severe asthma—An approach to find new therapies. Eur. Clin. Respir. J. 2014, 1, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chambers, E.S.; Nanzer, A.M.; Pfeffer, P.E.; Richards, D.F.; Timms, P.M.; Martineau, A.R.; Griffiths, C.J.; Corrigan, C.J.; Hawrylowicz, C.M. Distinct Endotypes of Steroid-Resistant Asthma Characterized by IL-17Ahigh and IFN-Γhigh Immunophenotypes: Potential Benefits of Calcitriol. J. Allergy Clin. Immunol. 2015, 136, 628–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, J.; Kuo, H.; Hsu, T.; Ou, C.; Liu, C.; Chuang, H.; Liang, M.; Huang, H.; Yang, K.D. Different Genetic Associations of the IgE Production among Fetus, Infancy and Childhood. PLoS ONE 2013, 8, e70362. [Google Scholar] [CrossRef] [PubMed]
- Breiteneder, H.; Peng, Y.Q.; Agache, I.; Diamant, Z.; Eiwegger, T.; Fokkens, W.J.; Traidl-Hoffmann, C.; Nadeau, K.; O’Hehir, R.E.; O’Mahony, L.; et al. Biomarkers for diagnosis and prediction of therapy responses in allergic diseases and asthma. Allergy 2020. [Google Scholar] [CrossRef] [PubMed]
- Kuo, C.H.S.; Pavlidis, S.; Loza, M.; Baribaud, F.; Rowe, A.; Pandis, I.; Sousa, A.; Corfield, J.; Djukanovic, R.; Lutter, R.; et al. T-Helper Cell Type 2 (Th2) and Non-Th2 Molecular Phenotypes of Asthma Using Sputum Transcriptomics in U-BIOPRED. Eur. Respir. J. 2017, 49, 1602135. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.C.; Kerr, S.; Dunican, E.M.; Woodruff, P.G.; Fajt, M.L.; Levy, B.D.; Israel, E.; Phillips, B.R.; Mauger, D.T.; Comhair, S.A.; et al. Refractory Airway Type 2 Inflammation in a Large Subgroup of Asthmatic Patients Treated with Inhaled Corticosteroids. J. Allergy Clin. Immunol. 2019, 143, 104–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pavlidis, S.; Takahashi, K.; Kwong, F.N.K.; Xie, J.; Hoda, U.; Sun, K.; Elyasigomari, V.; Agapow, P.; Loza, M.; Baribaud, F.; et al. “T2-High” in Severe Asthma Related to Blood Eosinophil, Exhaled Nitric Oxide and Serum Periostin. Eur. Respir. J. 2019, 53, 1800938. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, D.; Lehman, H. Asthma Phenotypes as a Guide for Current and Future Biologic Therapies. Clin. Rev. Allergy Immunol. 2020, 59, 160–174. [Google Scholar] [CrossRef] [PubMed]
- Kermani, N.Z.; Saqi, M.; Agapow, P.; Pavlidis, S.; Kuo, C.; Tan, K.S.; Mumby, S.; Sun, K.; Loza, M.; Baribaud, F. Type 2-Low Asthma Phenotypes by Integration of Sputum Transcriptomics and Serum Proteomics. Allergy 2020. [Google Scholar] [CrossRef]
- Silkoff, P.E.; Laviolette, M.; Singh, D.; FitzGerald, J.M.; Kelsen, S.; Backer, V.; Porsbjerg, C.M.; Girodet, P.-O.; Berger, P.; Kline, J.N.; et al. Identification of Airway Mucosal Type 2 Inflammation by Using Clinical Biomarkers in Asthmatic Patients. J. Allergy Clin. Immunol. 2017, 140, 710–719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuruvilla, M.E.; Lee, F.E.; Lee, G.B. Understanding Asthma Phenotypes, Endotypes, and Mechanisms of Disease. Clin. Rev. Allergy Immunol. 2019, 56, 219–233. [Google Scholar] [CrossRef] [PubMed]
- Kaur, R.; Chupp, G. Phenotypes and Endotypes of Adult Asthma: Moving toward Precision Medicine. J. Allergy Clin. Immunol. 2019, 144, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, C.M.; Hessel, E.M. Functions of T Cells in Asthma: More than Just T(H)2 Cells. Nat. Rev. Immunol. 2010, 10, 838–848. [Google Scholar] [CrossRef] [PubMed]
- Schofield, J.P.R.; Burg, D.; Nicholas, B.; Strazzeri, F.; Brandsma, J.; Staykova, D.; Folisi, C.; Bansal, A.T.; Xian, Y.; Guo, Y.; et al. Stratification of Asthma Phenotypes by Airway Proteomic Signatures. J. Allergy Clin. Immunol. 2019, 144, 70–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rossios, C.; Pavlidis, S.; Hoda, U.; Kuo, C.-H.; Wiegman, C.; Russell, K.; Sun, K.; Loza, M.J.; Baribaud, F.; Durham, A.L.; et al. Sputum Transcriptomics Reveal Upregulation of IL-1 Receptor Family Members in Patients with Severe Asthma. J. Allergy Clin. Immunol. 2018, 141, 560–570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marc-Malovrh, M.; Camlek, L.; Škrgat, S.; Kern, I.; Fležar, M.; Dežman, M.; Korošec, P. Elevated Eosinophils, IL5 and IL8 in Induced Sputum in Asthma Patients with Accelerated FEV1 Decline. Respir. Med. 2020, 162, 105875. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| T2-low Asthma | T2-High Asthma | p Value b | |
|---|---|---|---|
| No. | 12 | 24 | |
| Age in years, median (IQR) | 59 (27.0) | 53 (19.3) | 0.779 |
| Female sex, No. (%) | 9 (75) | 17 (71) | 1.000 |
| BMI (kg/m2), median (IQR) | 25.2 (4.9) | 27.5 (5.7) | 0.748 |
| FEV1 (%) preBD, median (IQR) | 92.5 (39.3) | 70 (28.3) | 0.051 |
| FEV1 (L) preBD, median (IQR) | 2.43 (0.92) | 2.20 (1.02) | 0.366 |
| FEV1 (%) postBD, median (IQR) | 97 (38) | 77 (25) | 0.019 |
| FEV1 (L) postBD, median (IQR) | 2.99 (1.41) | 2.21 (1.31) | 0.050 |
| FEV1 (%) increase postBD, median (IQR) | 9 (16) | 7 (15.5) | 0.391 |
| Positive reversibility test, No. (%) | 2 (17) | 4 (17) | 1.000 |
| FeNO (ppb), median (IQR) | 44 (57) | 55 (69) | 0.365 |
| Total serum IgE (kU/L), median (IQR) | 338 (871) | 136 (261) | 0.449 |
| Blood eosinophils (cells/μL), median (IQR) | 205 (253) | 535 (855) | 0.035 |
| Sputum eosinophils (%), median (IQR) | 5 (11.5) | 18 (42.0) | 0.017 |
| Active/ex-smokers, No. (%) | 1/3 (8.3/25.0) | 2/4 (8.3/16.7) | 0.700 |
| Exacerbations in the past year, No. (%) | 8 (67) | 15 (63) | 1.000 |
| ICS use, No. (%) | 10 (83) | 22 (92) | 0.588 |
| OCS maintenance use, No. (%) | 2 (17) | 12 (50) | 0.076 |
| Seasonal allergic rhinitis, No. (%) | 6 (50) | 8 (33) | 0.472 |
| Perennial allergic rhinitis, No. (%) | 6 (50) | 12 (50) | 1.000 |
| Biological therapy a, No. (%) | 1 (8) | 15 (63) | 0.004 |
| Control Subjects | Asthmatic Subjects | p Value b | |
|---|---|---|---|
| No. | 8 | 36 | |
| Age in years, median (IQR) | 48.5 (14.3) | 55.5 (19.5) | 0.223 |
| Female sex, No. (%) | 7 (88) | 26 (72) | 0.656 |
| BMI (kg/m2), median (IQR) | 26.9 (7.9) | 26.1 (6.2) | 0.899 |
| FEV1 (%) preBD, median (IQR) | 100.5 (11.8) | 74 (42.1) | 0.017 |
| FEV1 (L) preBD, median (IQR) | 2.88 (0.69) | 2.33 (1.01) | 0.013 |
| FEV1 (%) postBD, median (IQR) | ND | 2.26 (1.31) | |
| FEV1 (L) postBD, median (IQR) | ND | 79 (29) | |
| Positive reversibility test, No. (%) | ND | 6 (17) | |
| FeNO (ppb), median (IQR) | 30 (54) | 55 (57) | 0.313 |
| Total serum IgE (kU/l), median (IQR) | ND | 168 (417) | |
| Blood eosinophils (cells/μL), median (IQR) | 180 (65) | 315 (720) | 0.197 |
| Sputum eosinophils (%), median (IQR) | 0.5 (4.8) | 16 (25.5) | 0.016 |
| Active/ex-smokers, No. (%) | 4/0 (50/0) | 3/7 (8.3/19.4) | 0.242 |
| Exacerbations in the past year, No. (%) | 23 (64) | ||
| ICS c use, No. (%) | 32 (89)c | ||
| OCS maintenance use, No. (%) | 14 (39) | ||
| Seasonal allergic rhinitis, No. (%) | 14 (39) | ||
| Perennial allergic rhinitis, No. (%) | 18 (50) | ||
| Biological therapy a, No. (%) | 16 (44) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rijavec, M.; Krumpestar, T.; Škrgat, S.; Kern, I.; Korošec, P. T2-high Asthma, Classified by Sputum mRNA Expression of IL4, IL5, and IL13, is Characterized by Eosinophilia and Severe Phenotype. Life 2021, 11, 92. https://doi.org/10.3390/life11020092
Rijavec M, Krumpestar T, Škrgat S, Kern I, Korošec P. T2-high Asthma, Classified by Sputum mRNA Expression of IL4, IL5, and IL13, is Characterized by Eosinophilia and Severe Phenotype. Life. 2021; 11(2):92. https://doi.org/10.3390/life11020092
Chicago/Turabian StyleRijavec, Matija, Tomaž Krumpestar, Sabina Škrgat, Izidor Kern, and Peter Korošec. 2021. "T2-high Asthma, Classified by Sputum mRNA Expression of IL4, IL5, and IL13, is Characterized by Eosinophilia and Severe Phenotype" Life 11, no. 2: 92. https://doi.org/10.3390/life11020092
APA StyleRijavec, M., Krumpestar, T., Škrgat, S., Kern, I., & Korošec, P. (2021). T2-high Asthma, Classified by Sputum mRNA Expression of IL4, IL5, and IL13, is Characterized by Eosinophilia and Severe Phenotype. Life, 11(2), 92. https://doi.org/10.3390/life11020092