
Isolated Arthroscopic Lateral Retinacular Release for Lateral Patellar Compression Syndrome

 ,
, 
 , ,
, , 
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design
2.2. Eligibility Criteria
2.3. Surgical Technique
2.4. Outcomes of Interest
3. Results
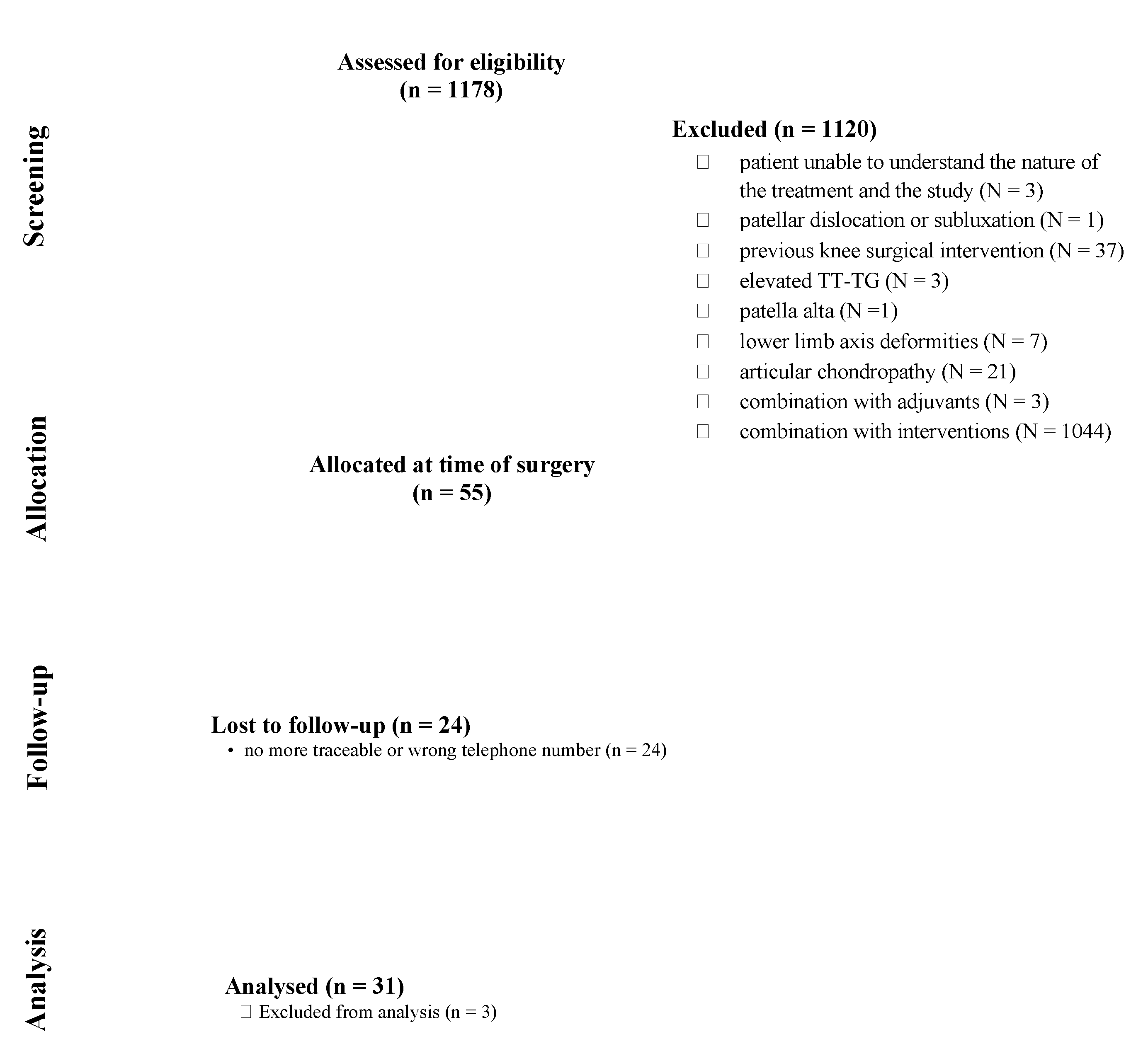
3.1. Search Results
3.2. Patient Demographics
3.3. Clinical Assessment
3.4. Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Saper, M.G.; Shneider, D.A. Diagnosis and treatment of lateral patellar compression syndrome. Arthrosc. Tech. 2014, 3, e633–e638. [Google Scholar] [CrossRef]
- Chen, J.B.; Chen, D.; Xiao, Y.P.; Chang, J.Z.; Li, T. Efficacy and experience of arthroscopic lateral patella retinaculum releasing through/outside synovial membrane for the treatment of lateral patellar compression syndrome. BMC Musculoskelet. Disord. 2020, 21, 108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dzioba, R.B. Diagnostic arthroscopy and longitudinal open lateral release. A four year follow-up study to determine predictors of surgical outcome. Am. J. Sports Med. 1990, 18, 343–348. [Google Scholar] [CrossRef]
- Ostermeier, S.; Holst, M.; Hurschler, C.; Windhagen, H.; Stukenborg-Colsman, C. Dynamic measurement of patellofemoral kinematics and contact pressure after lateral retinacular release: An in vitro study. Knee Surg. Sports Traumatol. Arthrosc. 2007, 15, 547–554. [Google Scholar] [CrossRef] [PubMed]
- Bentley, G.; Dowd, G. Current concepts of etiology and treatment of chondromalacia patellae. Clin. Orthop. Relat. Res. 1984, 189, 209–228. [Google Scholar]
- Wu, T.; Tang, S.; Wang, F. Treatment for lateral patellar impingement syndrome with arthroscopic lateral patelloplasty: A bidirectional cohort study. J. Orthop. Surg. Res. 2017, 12, 173. [Google Scholar] [CrossRef]
- Smith, B.E.; Selfe, J.; Thacker, D.; Hendrick, P.; Bateman, M.; Moffatt, F.; Rathleff, M.S.; Smith, T.O.; Logan, P. Incidence and prevalence of patellofemoral pain: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0190892. [Google Scholar] [CrossRef] [Green Version]
- Merchant, A.C.; Mercer, R.L. Lateral release of the patella. A preliminary report. Clin. Orthop. Relat. Res. 1974, 103, 40–45. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [Green Version]
- Insall, J.; Salvati, E. Patella position in the normal knee joint. Radiology 1971, 101, 101–104. [Google Scholar] [CrossRef]
- Slattery, C.; Kweon, C.Y. Classifications in Brief: Outerbridge Classification of Chondral Lesions. Clin. Orthop. Relat. Res. 2018, 476, 2101–2104. [Google Scholar] [CrossRef]
- Kazley, J.M.; Banerjee, S. Classifications in Brief: The Dejour Classification of Trochlear Dysplasia. Clin. Orthop. Relat. Res. 2019, 477, 2380–2386. [Google Scholar] [CrossRef]
- Panni, A.S.; Cerciello, S.; Maffulli, N.; Di Cesare, M.; Servien, E.; Neyret, P. Patellar shape can be a predisposing factor in patellar instability. Knee Surg. Sports Traumatol. Arthrosc. 2011, 19, 663–670. [Google Scholar] [CrossRef]
- Ward, B.D.; Lubowitz, J.H. Basic knee arthroscopy part 2: Surface anatomy and portal placement. Arthrosc. Tech. 2013, 2, e501–e502. [Google Scholar] [CrossRef]
- Kujala, U.M.; Jaakkola, L.H.; Koskinen, S.K.; Taimela, S.; Hurme, M.; Nelimarkka, O. Scoring of patellofemoral disorders. Arthroscopy 1993, 9, 159–163. [Google Scholar] [CrossRef]
- Lysholm, J.; Gillquist, J. Evaluation of knee ligament surgery results with special emphasis on use of a scoring scale. Am. J. Sports Med. 1982, 10, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Briggs, K.K.; Lysholm, J.; Tegner, Y.; Rodkey, W.G.; Kocher, M.S.; Steadman, J.R. The reliability, validity, and responsiveness of the Lysholm score and Tegner activity scale for anterior cruciate ligament injuries of the knee: 25 years later. Am. J. Sports Med. 2009, 37, 890–897. [Google Scholar] [CrossRef] [PubMed]
- Nikku, R.; Nietosvaara, Y.; Aalto, K.; Kallio, P.E. Operative treatment of primary patellar dislocation does not improve medium-term outcome: A 7-year follow-up report and risk analysis of 127 randomized patients. Acta Orthop. 2005, 76, 699–704. [Google Scholar] [CrossRef]
- Clifton, R.; Ng, C.Y.; Nutton, R.W. What is the role of lateral retinacular release? J. Bone Jt. Surg. Br. 2010, 92, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Aglietti, P.; Pisaneschi, A.; Buzzi, R.; Gaudenzi, A.; Allegra, M. Arthroscopic lateral release for patellar pain or instability. Arthroscopy 1989, 5, 176–183. [Google Scholar] [CrossRef]
- Larson, R.L.; Cabaud, H.E.; Slocum, D.B.; James, S.L.; Keenan, T.; Hutchinson, T. The patellar compression syndrome: Surgical treatment by lateral retinacular release. Clin. Orthop. Relat. Res. 1978, 134, 158–167. [Google Scholar] [CrossRef]
- Krompinger, W.J.; Fulkerson, J.P. Lateral retinacular release for intractable lateral retinacular pain. Clin. Orthop. Relat. Res. 1983, 179, 191–193. [Google Scholar] [CrossRef]
- Gecha, S.R.; Torg, J.S. Clinical prognosticators for the efficacy of retinacular release surgery to treat patellofemoral pain. Clin. Orthop. Relat. Res. 1990, 253, 203–208. [Google Scholar] [CrossRef]
- Hinckel, B.; Arendt, E. Lateral Retinaculum Lengthening or Release. Oper. Tech. Sports Med. 2015, 23, 100–106. [Google Scholar] [CrossRef]
- Metcalf, R.W. An arthroscopic method for lateral release of subluxating or dislocating patella. Clin. Orthop. Relat. Res. 1982, 167, 9–18. [Google Scholar] [CrossRef]
- Lattermann, C.; Toth, J.; Bach, B.R., Jr. The role of lateral retinacular release in the treatment of patellar instability. Sports Med. Arthrosc. Rev. 2007, 15, 57–60. [Google Scholar] [CrossRef] [Green Version]
- Fithian, D.C.; Paxton, E.W.; Post, W.R.; Panni, A.S.; International Patellofemoral Study Group. Lateral retinacular release: A survey of the International Patellofemoral Study Group. Arthroscopy 2004, 20, 463–468. [Google Scholar] [CrossRef]
- Felli, L.; Formica, M.; Lovisolo, S.; Capello, A.G.; Alessio-Mazzola, M. Clinical Outcome of Arthroscopic Lateral Retinacular Release for Symptomatic Bipartite Patella in Athletes. Arthroscopy 2018, 34, 1550–1558. [Google Scholar] [CrossRef]
- Fulkerson, J.P.; Shea, K.P. Disorders of patellofemoral alignment. J. Bone Jt. Surg. Am. 1990, 72, 1424–1429. [Google Scholar] [CrossRef]
- Ficat, P. The syndrome of lateral hyperpressure of the patella. Acta Orthop. Belg. 1978, 44, 65–76. [Google Scholar]
- Mori, Y.; Fujimoto, A.; Okumo, H.; Kuroki, Y. Lateral retinaculum release in adolescent patellofemoral disorders: Its relationship to peripheral nerve injury in the lateral retinaculum. Bull. Hosp. Jt. Dis. Orthop. Inst. 1991, 51, 218–229. [Google Scholar]
- Woods, G.W.; Elkousy, H.A.; O’Connor, D.P. Arthroscopic release of the vastus lateralis tendon for recurrent patellar dislocation. Am. J. Sports Med. 2006, 34, 824–831. [Google Scholar] [CrossRef]
- Hughston, J.C.; Deese, M. Medial subluxation of the patella as a complication of lateral retinacular release. Am. J. Sports Med. 1988, 16, 383–388. [Google Scholar] [CrossRef]
- Colvin, A.C.; West, R.V. Patellar instability. J. Bone Jt. Surg. Am. 2008, 90, 2751–2762. [Google Scholar] [CrossRef]
- Johnson, R.P. Lateral facet syndrome of the patella. Lateral restraint analysis and use of lateral resection. Clin. Orthop. Relat. Res. 1989, 238, 148–158. [Google Scholar] [CrossRef]
- Christoforakis, J.; Bull, A.M.; Strachan, R.K.; Shymkiw, R.; Senavongse, W.; Amis, A.A. Effects of lateral retinacular release on the lateral stability of the patella. Knee Surg. Sports Traumatol. Arthrosc. 2006, 14, 273–277. [Google Scholar] [CrossRef] [Green Version]
- Panni, A.S.; Cerciello, S.; Vasso, M. Patellofemoral instability: Surgical treatment of soft tissues. Joints 2013, 1, 34–39. [Google Scholar] [PubMed]
- Senavongse, W.; Amis, A.A. The effects of articular, retinacular, or muscular deficiencies on patellofemoral joint stability: A biomechanical study in vitro. J. Bone Jt. Surg. Br. 2005, 87, 577–582. [Google Scholar] [CrossRef] [Green Version]
- Elkousy, H. Complications in brief: Arthroscopic lateral release. Clin. Orthop. Relat. Res. 2012, 470, 2949–2953. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.H.; Wu, C.C.; Pan, R.Y.; Lu, H.T.; Shen, H.C. Medial retinacular flap advancement and arthroscopic lateral release for symptomatic chronic patellar lateral subluxation with tilting. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 2499–2504. [Google Scholar] [CrossRef]
- Fu, F.H.; Maday, M.G. Arthroscopic lateral release and the lateral patellar compression syndrome. Orthop. Clin. N. Am. 1992, 23, 601–612. [Google Scholar] [CrossRef]
- Unal, B.; Hinckel, B.B.; Sherman, S.L.; Lattermann, C. Comparison of Lateral Retinaculum Release and Lengthening in the Treatment of Patellofemoral Disorders. Am. J. Orthop. 2017, 46, 224–228. [Google Scholar]
- Ceder, L.C.; Larson, R.L. Z-plasty lateral retinacular release for the treatment of patellar compression syndrome. Clin. Orthop. Relat. Res. 1979, 144, 110–113. [Google Scholar] [CrossRef]
- Sanchis-Alfonso, V.; Montesinos-Berry, E. Is lateral retinacular release still a valid surgical option? From release to lengthening. Ann. Transl. Med. 2015, 3, 301. [Google Scholar] [CrossRef] [PubMed]
- Pagenstert, G.; Wolf, N.; Bachmann, M.; Gravius, S.; Barg, A.; Hintermann, B.; Wirtz, D.C.; Valderrabano, V.; Leumann, A.G. Open lateral patellar retinacular lengthening versus open retinacular release in lateral patellar hypercompression syndrome: A prospective double-blinded comparative study on complications and outcome. Arthroscopy 2012, 28, 788–797. [Google Scholar] [CrossRef]
- O’Neill, D.B. Open lateral retinacular lengthening compared with arthroscopic release. A prospective, randomized outcome study. J. Bone Jt. Surg. Am. 1997, 79, 1759–1769. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Eligibility Criteria |
|---|
| Inclusion Criteria |
|
| Exclusion Criteria |
|
| Endpoint | Value |
|---|---|
| Procedures (n) | 31 |
| Age (mean) | 34.2 ± 13.1 |
| Sex (female) | 55% (17 of 31) |
| Side (right) | 58% (18 of 31) |
| Hospitalization length (days) | 3.5 ± 1.4 |
| Length of follow up (months) | 86.0 ± 22.8 |
| Scores | Value |
|---|---|
| Numeric Rating System | 1.2 ± 0.8 |
| Kujala Anterior Knee Pain Scale | 91.3 ± 11.3 |
| Lysholm Knee Scoring Scale | 93.1 ± 15.0 |
| Tegner Activity Scale | 5.0 ± 1.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Migliorini, F.; Lüring, C.; Eschweiler, J.; Baroncini, A.; Driessen, A.; Spiezia, F.; Tingart, M.; Maffulli, N. Isolated Arthroscopic Lateral Retinacular Release for Lateral Patellar Compression Syndrome. Life 2021, 11, 295. https://doi.org/10.3390/life11040295
Migliorini F, Lüring C, Eschweiler J, Baroncini A, Driessen A, Spiezia F, Tingart M, Maffulli N. Isolated Arthroscopic Lateral Retinacular Release for Lateral Patellar Compression Syndrome. Life. 2021; 11(4):295. https://doi.org/10.3390/life11040295
Chicago/Turabian StyleMigliorini, Filippo, Christian Lüring, Jörg Eschweiler, Alice Baroncini, Arne Driessen, Filippo Spiezia, Markus Tingart, and Nicola Maffulli. 2021. "Isolated Arthroscopic Lateral Retinacular Release for Lateral Patellar Compression Syndrome" Life 11, no. 4: 295. https://doi.org/10.3390/life11040295
APA StyleMigliorini, F., Lüring, C., Eschweiler, J., Baroncini, A., Driessen, A., Spiezia, F., Tingart, M., & Maffulli, N. (2021). Isolated Arthroscopic Lateral Retinacular Release for Lateral Patellar Compression Syndrome. Life, 11(4), 295. https://doi.org/10.3390/life11040295