Abstract
The diagnostics of prostate cancer are currently based on three pillars: prostate biomarker panel, imaging techniques, and histological verification. This paper presents a diagnostic algorithm that can serve as a “road map”: from initial patient stratification to the final decision regarding treatment. The algorithm is based on a review of the current literature combined with our own experience. Diagnostic algorithms are a feature of an advanced healthcare system in which all steps are consciously coordinated and optimized to ensure the proper individualization of the treatment process. The prostate cancer diagnostic algorithm was created using the prostate specific antigen and in particular the Prostate Health Index in the first line of patient stratification. It then continued on the diagnostic pathway via imaging techniques, biopsy, or active surveillance, and then on to the treatment decision itself. In conclusion, the prostate cancer diagnostic algorithm presented here is a functional tool for initial patient stratification, comprehensive staging, and aggressiveness assessment. Above all, emphasis is placed on the use of the Prostate Health Index (PHI) in the first stratification of the patients as a predictor of aggressiveness and clinical stage of prostrate cancer (PCa). The inclusion of PHI in the algorithm significantly increases the accuracy and speed of the diagnostic procedure and allows to choose the optimal pathway just from the beginning. The use of advanced diagnostic techniques allows us to move towards to a more advanced level of cancer care. This diagnostics algorithm has become a standard of care in our hospital. The algorithm is continuously validated and modified based on our results.
1. Introduction
Prostate cancer (PCa) is the most frequent malignant disease to occur in men. According to The International Agency for Research on Cancer (IARC), 1,414,259 new cases of PCa were reported and 375,304 men died of PCa worldwide in 2020 [1]. PCa’s incidence and mortality are connected to the human development index (HDI). The disease is most prevalent in developed countries, while its mortality rate is highest in low-HDI countries [2]. The risk of PCa increases with age. The majority of PCa cases are diagnosed in men older than 65 [3]. PCa is a highly heterogeneous disease, ranging from a clinically insignificant manifestation that requires only active surveillance, to a highly aggressive castration-resistant type of tumor that requires a quick and radical course of action. Differences in the incidence rate of PCa worldwide primarily reflect differences in the use of diagnostic testing. Accurate diagnostics and PCa staging are imperative for the selection of the most appropriate therapeutic strategy [4].
The diagnostics of PCa are currently based on three pillars: prostate biomarker panel, imaging techniques, and histological verification. This paper presents a diagnostic algorithm that can serve as a “road map” delineating the course of treatment: from initial patient stratification to the final decision regarding treatment. The algorithm is based on a review of the current literature combined with our own experience.
2. Diagnostic Algorithm
2.1. PCa Diagnostic Algorithm–A Tool for Patient Stratification, Staging and Aggressiveness Assessment
The first algorithm was created a few years ago. Since then, the algorithm has been supplemented every year with new knowledge and new diagnostic procedures introduced into clinical practice. This was done to ensure that the algorithm continues to reflect the most current procedures that are applied in our university hospital.
Diagnostic algorithms are a feature of an advanced healthcare system in which all steps are consciously coordinated and optimized to ensure the proper individualization of the treatment process. The PCa diagnostic algorithm was created using the prostate specific antigen (PSA) and in particular the Prostate Health Index (PHI) in the first line of patient stratification. It then continued on the diagnostic pathway via imaging techniques, biopsy, or active surveillance, and then on to the treatment decision itself (Figure 1).
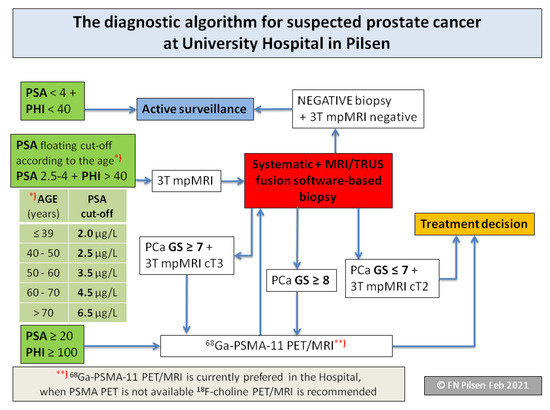
Figure 1.
Prostate cancer diagnostic algorithm.
The first step is to have patients stratified into three groups according to PSA and PHI levels. If the PSA and PHI levels are low, patients are rated as benign: they will still be monitored and will be tested again, usually after six months.
If the level of PSA is above the reference ranges for the patient’s age group, and/or the PHI level is over 40, the second step is to perform imaging techniques. We use multi-parametric magnetic resonance imaging (mpMRI) to localize the lesion, but also to evaluate a more detailed anatomy before surgery. We performed 68Ga-PSMA-11 PET/MRI as part of the comprehensive staging in a selected group of patients before radical prostatectomy, as well as in primary diagnostics before histological verification. This is done in cases where there is a strong suspicion that the patient has a high-risk of developing PCa, or has locally advanced PCa and the extensive staging leads to a change in treatment management. In the middle of the algorithm, the current status of the PCa is proved using biopsy, in order to achieve that each patient with suspected PCa undergoes an mpMRI.
The biopsy holds a key position located in the middle of the algorithm. In order to achieve the best results in histological verification of significant PCa, we perform an MRI/transrectal ultrasound-guided (TRUS) fusion software-based targeted biopsy of the prostate. If the man is biopsy naïve, an additional systematic biopsy will be performed to determine the extent of the tumor and to help in planning the surgery–nerve sparing or not.
Finally, at the end of the algorithm, a treatment decision is made. Based on the results of histology, evaluated using the Gleason score and the imaging examinations, the appropriate method of treatment is selected according to the stage of the disease. As a relatively new approach, active surveillance is also incorporated into the algorithm.
2.2. The Algorithm Is Based on Our Experience, Results and Knowledge
It has been our experience that the value of PHI level can be used for validation in patients after radical prostatectomy. A total of 787 patients were examined and subsequently operated from 1/2013 to 12/2019. A definitive Gleason score was determined. PHI values were compared with definitive staging and grading. The study confirmed a very good ability of PHI to distinguish GS < 7 (low aggressiveness) and GS ≥ 7 (higher aggressiveness) prostate tumors and thus, PHI was added to the first line of biochemical assessment of the tumor aggressiveness [5].
We have performed 3T mpMRI to detect PCa lesions as a standard method from 2012. This step also decreases the over diagnosis of PCa. From 1/2018 to 2/2020, 150 patients underwent 68Ga-PSMA-11 PET/MRI as part of comprehensive staging; this examination is the only one under the clinical trial in our country.
Magnetic resonance imaging and targeted biopsy (MRI/TBx) were performed from 1/2017 to 12/2019 in the examination of 450 patients.
2.3. PHI as a Tool for the First (Initial) Stratification of the Patient
PCa diagnostics using biomarkers started in the 1980s with the total PSA (tPSA) measurement. Total PSA has a limited sensitivity and specificity for PCa detection [6]. Seeking better sensitivity and specificity, free PSA (fPSA) was introduced and then (2])proPSA. These developments enabled physicians not only to start using biomarkers, but also to calculate parameters; namely, the percentage of fPSA (%freePSA = (fPSA/tPSA) * 100) and Prostate Health Index, PHI (PHI = (([-2])proPSA/fPSA) × √tPSA). These parameters, PHI especially, contributed to PCa aggressiveness assessment using biochemical methods [7]. One of the largest recent studies carried out by PROMETHEUS, a Multicentric European Study, confirmed PHI as one of the strongest predictors of PCa, correlating with the Gleason Score (GS). In our own studies, firstly monocentric [5,8] and later on multicentric (with our partners) [9,10], we proved the PHI’s ability to distinguish between PCa GS < 7 (low aggressiveness) and GS ≥ 7 (higher aggressiveness).
2.4. The Key Role of Imaging Techniques in Staging and Surgical Navigation
A pathway with mpMRI combining T2-weighted, dynamic contrast-enhanced (DCE) and diffusion weighted imaging (DWI) has been shown to be accurate in significant PCa. Prostate anatomy is best assessed by T1 and T2 weighted images, with the DCE and DWI contributing functional information. There is also evidence that mpMRI tends to detect higher risk disease, which makes it attractive as a potential triage test [11]. mpMRI in the diagnostics of PCa is very often used for its high sensitivity and specificity. Sensitivity increases especially with tumor size and aggressiveness. The results are excellent, especially for significant tumors: tumor volume ≥ 0.5 mL or GS ≥ 7 [12]. Imaging with mpMRI plays two roles in PCa diagnostics. Firstly, it functions as a secondary screening test, exempting men with nonsuspicious tests from biopsy. MRI reduced the need for biopsy by 68% in men with PSA 3.0 µg/L. The second function of MRI is to provide an image of the lesion(s), so that sampling can be more precise [11].
As part of the unification of the MRI description, the European Society for Uroradiology (ESUR) introduced the PI-RADS (Prostate imagining reporting and data system) classification system. This prostate sector diagram employs forty-one sectors/regions: thirty-eight for the prostate, two for the seminal vesicles and one for the external urethral sphincter [13,14].
PET/CT with radiolabeled choline analogs is widely used in clinical practice for prostate cancer staging. 18F-fluoroethylcholine PET demonstrated higher accuracy than MRI for the detection of primary prostate cancer; specificity was however limited by choline uptake in benign lesions [15]. Since 2012, [18F]- and [68Ga]-labeled inhibitors of prostate-specific membrane antigen (PSMA) entered early clinical development for PET imaging of PCa and showed immediate promise for sensitive and specific identification of local and distant sites of disease [16,17]. Results from [68Ga]-PSMA-11 PET/MRI and PET/CT in Figure 2, Figure 3 and Figure 4. To summarize, according to the available systematic reviews and clinical trials, the sensitivity and specificity in primary staging of PCa using PSMA ligands is usually above 40% and over 85%, respectively. The impact on therapy planning was also investigated, performing PET/CT or, less frequently, PET/MRI using PSMA ligands, the therapeutic procedure changes in approximately 21% of patients in the primary staging [18,19].
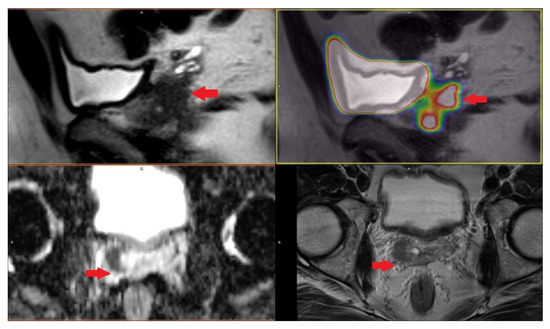
Figure 2.
Patient with prostate cancer GS 7 (4 + 3) in right lobe with right seminal vesicle invasion cT3b iPSA 4.17 PHI 64.93 in [68Ga]-PSMA-11 PET/MRI.
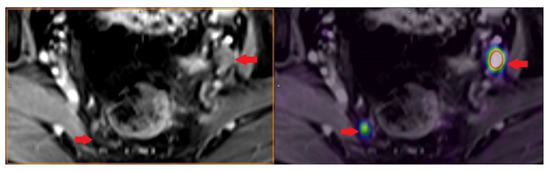
Figure 3.
Patient with lymph nodes metastases in prostate cancer GS 9 (4 + 5) iPSA 22.85 PHI 130.63 in [68Ga]-PSMA-11 PET/MRI.
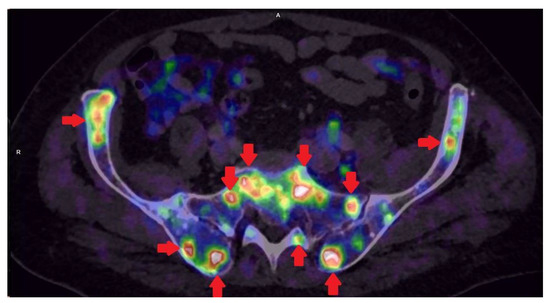
Figure 4.
Patient with multiple bones metastases in prostate cancer GS 8 (4 + 4) iPSA 45.33 PHI 176.8 in [68Ga]-PSMA-11 PET/CT.
2.5. The Basic Role of the Biopsy in Tumor Aggressiveness Assessment
A necessary condition for the initiation of PCa therapy is PCa histological verification using biopsy. The transrectal ultrasound (TRUS) navigated biopsy is used as a basic procedure [20]. The second option is the cognitive biopsy in which the result of the imaging technique, most often mpMRI, is known. Currently, the preferred procedure is the fusion biopsy, where images from mpMRI and TRUS are merged by software [20,21]. MRI information can be used to guide prostate biopsy cores, especially MRI/TRUS fusion software-based targeted biopsy of the prostate (MRI-TBx) to suspicious areas in the prostate. MRI-TBx has a higher detection rate for significant PCa and a lower detection rate for insignificant PCa compared with T-Bx [22]. Nonetheless, some lesions might also be missed on MRI-guided biopsies and these are the patients who pose a diagnostic challenge. With the introduction of 68Ga-PSMA, ligands which exhibit almost exclusive expression in the prostate and increased expression in PCa are more often detected [23]. PSMA-PET/MRI in combination with a newly developed fusion biopsy system-PET/TRUS and PET/MRI/TRUS fusion-proved to be a valuable tool for the detection of PCa in patients following a prior negative prostate biopsy and is therefore attracting increasing attention [24].
Based on biopsies, the Gleason score (GS) has been used since the 1960s as the main grading system for PCa cell assessment. The GS ranges from 1 to 10 and was considered a main factor when a treatment plan was determined. This was the case until 2016 when the International Society of Urological Pathology (ISUP) revised the PCa grading system and a new scale, the 5 ISUP Grades, was established [25].
2.6. Active Surveillance–A Suitable Procedure for Tumors with Low Aggressiveness
With more and more advanced diagnostic methods and increasingly accurate assessment of tumor aggressiveness, new approaches such as active surveillance can be applied instead of urgent surgery [26]. Active surveillance is an excellent example of how the medical paradigm has slowly changed during recent years. As aggressiveness is the main predictive factor for subsequent treatment management in the case of PCa, the main current task is to make precise and timely aggressiveness assessments [27]. Considering the side effects of radical prostatectomy (incontinence or sexual dysfunction), which is indicated in the case of highly aggressive PCa (GS ≥ 7), active surveillance seems to be the suitable option for PCa with low aggressiveness (GS < 7).
3. Discussion
The above-described PCa diagnostic algorithm has a few limitations. One major difficulty may arise when using highly specific imaging methods with the latest radiotracers; these, however, are not widely available. Nonetheless, the algorithm was designed precisely with the aim of incorporating these state-of-the-art diagnostic methods and implementing them in clinical practice in order to achieve a clear indication.
Hybrid imaging using PET and MRI has been intentionally incorporated into the algorithm. MRI is perfect for the imaging of both the prostate, especially for targeted prostate biopsy, and for the detection of lymph node metastases. It has an irreplaceable role in preoperative lymph node staging. Having used the [68Ga]-PSMA-11 as the latest radiotracer with very promising results, we believe that thus performed staging is highly specialized and yields the best results. [68Ga]-labelled PSMA ligand could be superior to choline tracers in its ability to obtain high contrast. PSMA tracer can detect lesions characteristic of PCa with improved contrast when compared to the standard [18F]-fluoromethylcholine, especially at low PSA levels. A significant advantage of [68Ga]-PSMA-11 is that lesions characteristic of lymph node metastases are frequently presented in very high contrast when compared to choline. The superior contrast in [68Ga]-PSMA-11 has also been demonstrated in most skeletal metastases [28].
Due to the low availability of PET/MRI scanners, PET/CT can be used instead. When this is the case, however, we lose the possibility of using images for targeted prostate biopsy and we are forced to perform further examinations in the form of at least mpMRI of the prostate, which delays further treatment decisions and initiations. Furthermore, the hybrid imaging method PET/MRI has the advantage of a reduced radiation dose compared to PET/CT.
Even though the PSMA-PET scan has shown considerable early promise, its availability is limited and incurs considerable cost. Furthermore, since prostate cancer patients commonly undergo mpMRI of the prostate, there is the possibility of a one-stop staging modality in the form of a whole-body MRI (wb-MRI). According to EAU guidelines, wb-MRI is more sensitive than conventional imaging methods and is more sensitive than choline PET/CT in its detection of bone metastases. Nevertheless, choline PET/CT had the highest specificity for diagnostic evaluation [29]. Wb-MRI with DWI is an effective method for overall staging in PCa, as it can detect metastases in normal-sized lymph nodes and early intramedullary bone metastases before the appearance of cortical destruction or reactive processes [30]. The LOCATE trial designed to compare the detection of prostate cancer using conventional imaging methods with wb-MRI will certainly yield promising results [31]. Due to the fact that a whole-body MRI is not a standard imaging method in our hospital, this alternative is not applicable in our case. Currently, mpMRI is the standard method for prostate imaging and it plays an important role in the detection, targeted biopsy, local staging, and risk classification of prostate cancers. Many studies have compared the bi-parametric MRI imaging protocol consisting of T2-weighted imaging and DWI with a standard multi-parametric imaging protocol for the detection of PCa. There is no significant difference regarding the detection of PCa [32,33,34].
Our hospital is committed to performing mpMRI. This is based on knowledge gained from experience: DCE can in some cases help detect prostate cancer in both PZ and TZ. It is sometimes referred to as a “backup” sequence, especially if DWI/ADC is degraded by artifacts [35]. In PI-RADS version 2.1, DCE is used to differentiate scores of 3 and 4 in the peripheral zone. If we have a DWI score of 3 and early saturation is present, the finding is upgraded to a score of 4, which may help achieve a more accurate aggressiveness classification and individualized treatment of prostate cancer [13].
4. Conclusions
The PCa diagnostic algorithm presented here is a functional tool for initial patient stratification, comprehensive staging and aggressiveness assessment.
The use of advanced diagnostic techniques allows us to move towards to a more advanced level of cancer care that is more beneficial for patients. This diagnostics algorithm has become a standard of care in our hospital. The algorithm is continuously validated and modified based on our results.
Author Contributions
Conceptualization, H.S. and O.D.; methodology, R.K.; resources, R.F.; data curation, J.F.; writing—original draft preparation, H.S.; writing—review and editing, O.H. and R.K.; visualization, H.S. and O.D.; supervision, O.T. and M.H. All authors have read and agreed to the published version of the manuscript.
Funding
Supported by Ministry of Health, Czech Republic-conceptual development of research organization (Faculty Hospital in Pilsen-FNPl, 00669806) and BBMRI-CZ: Biobank network-a versatile platform for the research of the etiopathogenesis of diseases CZ.02.1.01/0.0/0.0/16_013/0001674.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Database. Available online: https://Gco.Iarc.Fr/Today/Data/Factsheets/Cancers/27-Prostate-Fact-Sheet.Pdf (accessed on 30 January 2020).
- Kucera, R.; Pecen, L.; Topolcan, O.; Dahal, A.R.; Costigliola, V.; Giordano, F.A.; Golubnitschaja, O. Prostate Cancer Management: Long-Term Beliefs, Epidemic Developments in the Early Twenty-First Century and 3PM Dimensional Solutions. EPMA J. 2020, 11, 399–418. [Google Scholar] [CrossRef]
- Catalona, W.J. Prostate Cancer Screening. Med. Clin. N. Am. 2018, 102, 199–214. [Google Scholar] [CrossRef] [PubMed]
- Nevo, A.; Navaratnam, A.; Andrews, P. Prostate Cancer and the Role of Biomarkers. Abdom. Radiol. 2020, 45, 2120–2132. [Google Scholar] [CrossRef]
- Dolejsova, O.; Kucera, R.; Fuchsova, R.; Topolcan, O.; Svobodova, H.; Hes, O.; Eret, V.; Pecen, L.; Hora, M. The Ability of Prostate Health Index (PHI) to Predict Gleason Score in Patients with Prostate Cancer and Discriminate Patients Between Gleason Score 6 and Gleason Score Higher Than 6—A Study on 320 Patients After Radical Prostatectomy. Technol. Cancer Res. Treat. 2018, 17, 153303381878737. [Google Scholar] [CrossRef]
- Wilt, T.J.; Jones, K.M.; Barry, M.J.; Andriole, G.L.; Culkin, D.; Wheeler, T.; Aronson, W.J.; Brawer, M.K. Follow-up of Prostatectomy versus Observation for Early Prostate Cancer. N. Engl. J. Med. 2017, 377, 132–142. [Google Scholar] [CrossRef] [PubMed]
- Maxeiner, A.; Kilic, E.; Matalon, J.; Friedersdorff, F.; Miller, K.; Jung, K.; Stephan, C.; Busch, J. The Prostate Health Index PHI Predicts Oncological Outcome and Biochemical Recurrence after Radical Prostatectomy—Analysis in 437 Patients. Oncotarget 2017, 8, 79279–79288. [Google Scholar] [CrossRef] [PubMed]
- Ferda, J.; Ferdová, E.; Baxa, J.; Fínek, J.; Topolčan, O. 18F-Fluorocholine PET/MRI in Restaging of Prostatic Carcinoma in Relation to PSA Level and Detection of Active Disease. Anticancer Res. 2018, 38, 4139. [Google Scholar] [CrossRef]
- Stejskal, J.; Adamcová, V.; Záleský, M.; Novák, V.; Čapoun, O.; Fiala, V.; Dolejšová, O.; Sedláčková, H.; Veselý, Š.; Zachoval, R. The Predictive Value of the Prostate Health Index vs. Multiparametric Magnetic Resonance Imaging for Prostate Cancer Diagnosis in Prostate Biopsy. World J. Urol. 2020, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Novak, V.; Vesely, S.; Luksanová, H.; Prusa, R.; Capoun, O.; Fiala, V.; Dolejsová, O.; Sedlacková, H.; Kucera, R.; Stejskal, J.; et al. Preoperative Prostate Health Index Predicts Adverse Pathology and Gleason Score Upgrading after Radical Prostatectomy for Prostate Cancer. BMC Urol. 2020, 20, 144. [Google Scholar] [CrossRef]
- Bergdahl, A.G.; Wilderäng, U.; Aus, G.; Carlsson, S.; Damber, J.-E.; Frånlund, M.; Geterud, K.; Khatami, A.; Socratous, A.; Stranne, J.; et al. Role of Magnetic Resonance Imaging in Prostate Cancer Screening: A Pilot Study within the Göteborg Randomised Screening Trial. Eur. Urol. 2016, 70, 566–573. [Google Scholar] [CrossRef] [PubMed]
- Bratan, F.; Niaf, E.; Melodelima, C.; Chesnais, A.L.; Souchon, R.; Mège-Lechevallier, F.; Colombel, M.; Rouvière, O. Influence of Imaging and Histological Factors on Prostate Cancer Detection and Localisation on Multiparametric MRI: A Prospective Study. Eur. Radiol. 2013, 23, 2019–2029. [Google Scholar] [CrossRef]
- Turkbey, B.; Rosenkrantz, A.B.; Haider, M.A.; Padhani, A.R.; Villeirs, G.; Macura, K.J.; Tempany, C.M.; Choyke, P.L.; Cornud, F.; Margolis, D.J.; et al. Prostate Imaging Reporting and Data System Version 2.1: 2019 Update of Prostate Imaging Reporting and Data System Version 2. Eur. Urol. 2019, 76, 340–351. [Google Scholar] [CrossRef]
- Rowe, S.P.; Pienta, K.J.; Pomper, M.G.; Gorin, M.A. PSMA-RADS Version 1.0: A Step towards Standardizing the Interpretation and Reporting of PSMA–Targeted PET Imaging Studies. Eur. Urol. 2018, 73, 485–487. [Google Scholar] [CrossRef] [PubMed]
- Giovacchini, G.; Giovannini, E.; Leoncini, R.; Riondato, M.; Ciarmiello, A. PET and PET/CT with Radiolabeled Choline in Prostate Cancer: A Critical Reappraisal of 20 Years of Clinical Studies. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1751–1776. [Google Scholar] [CrossRef]
- Rauscher, I.; Maurer, T.; Fendler, W.P.; Sommer, W.H.; Schwaiger, M.; Eiber, M. 68Ga-PSMA Ligand PET/CT in Patients with Prostate Cancer: How We Review and Report. Cancer Imaging 2016, 16, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Fendler, W.P.; Schmidt, D.F.; Wenter, V.; Thierfelder, K.M.; Zach, C.; Stief, C.; Bartenstein, P.; Kirchner, T.; Gildehaus, F.J.; Gratzke, C.; et al. 68Ga-PSMA-HBED-CC PET/CT Detects Location and Extent of Primary Prostate Cancer. J. Nucl. Med. 2016, 57, 1720–1725. [Google Scholar] [CrossRef] [PubMed]
- Von Eyben, F.E.; Picchio, M.; von Eyben, R.; Rhee, H.; Bauman, G. 68Ga-Labeled Prostate-Specific Membrane Antigen Ligand Positron Emission Tomography/Computed Tomography for Prostate Cancer: A Systematic Review and Meta-Analysis. Eur. Urol. Focus 2018, 4, 686–693. [Google Scholar] [CrossRef]
- Roach, P.J.; Francis, R.; Emmett, L.; Hsiao, E.; Kneebone, A.; Hruby, G.; Eade, T.; Nguyen, Q.A.; Thompson, B.D.; Cusick, T.; et al. The Impact of 68Ga-PSMA PET/CT on Management Intent in Prostate Cancer: Results of an Australian Prospective Multicenter Study. J. Nucl. Med. 2018, 59, 82–88. [Google Scholar] [CrossRef]
- Ahmed, H.U.; El-Shater Bosaily, A.; Brown, L.C.; Gabe, R.; Kaplan, R.; Parmar, M.K.; Collaco-Moraes, Y.; Ward, K.; Hindley, R.G.; Freeman, A.; et al. Diagnostic Accuracy of Multi-Parametric MRI and TRUS Biopsy in Prostate Cancer (PROMIS): A Paired Validating Confirmatory Study. Lancet 2017, 389, 815–822. [Google Scholar] [CrossRef]
- Kasivisvanathan, V.; Stabile, A.; Neves, J.B.; Giganti, F.; Valerio, M.; Shanmugabavan, Y.; Clement, K.D.; Sarkar, D.; Philippou, Y.; Thurtle, D.; et al. Magnetic Resonance Imaging-Targeted Biopsy Versus Systematic Biopsy in the Detection of Prostate Cancer: A Systematic Review and Meta-Analysis. Eur. Urol. 2019, 76, 284–303. [Google Scholar] [CrossRef]
- Zettinig, O.; Shah, A.; Hennersperger, C.; Eiber, M.; Kroll, C.; Kübler, H.; Maurer, T.; Milletarì, F.; Rackerseder, J.; Zu Berge, C.S.; et al. Multimodal Image-Guided Prostate Fusion Biopsy Based on Automatic Deformable Registration. Int. J. Comput. Assist. Radiol. Surg. 2015, 10, 1997–2007. [Google Scholar] [CrossRef]
- Eiber, M.; Nekolla, S.G.; Maurer, T.; Weirich, G.; Wester, H.-J.; Schwaiger, M. 68Ga-PSMA PET/MR with Multimodality Image Analysis for Primary Prostate Cancer. Abdom. Imaging 2015, 40, 1769–1771. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Liu, T.; Zhang, Z.; Zhang, N.; Du, P.; Yang, Y.; Liu, Y.; Yu, W.; Li, N.; Gorin, M.A.; et al. 68Ga-PSMA PET/CT Combined with PET/Ultrasound-Guided Prostate Biopsy Can Diagnose Clinically Significant Prostate Cancer in Men with Previous Negative Biopsy Results. J. Nucl. Med. 2020, 61, 1314. [Google Scholar] [CrossRef] [PubMed]
- Epstein, J.; Egevad, L.; Amin, M.; Delahunt, B.; Srigley, J.; Humphrey, P.; Al Hussain, T.; Algaba, F.; Aron, M.; Berman, D.; et al. The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma: Definition of Grading Patterns and Proposal for a New Grading System. Am. J. Surg. Pathol. 2016, 40, 244–252. [Google Scholar] [CrossRef]
- Xu, J.; Bock, C.; Janisse, J.; Schwartz, K.L.; Triest, J.; Cher, M.L.; Goodman, M. Urologists’ Perceptions of Active Surveillance and Their Recommendations for Low-Risk Prostate Cancer Patients. UrologyJanuary 2021, in press. [Google Scholar] [CrossRef]
- Bul, M.; Zhu, X.; Valdagni, R.; Pickles, T.; Kakehi, Y.; Rannikko, A.; Bjartell, A.; van der Schoot, D.K.; Cornel, E.B.; Conti, G.N.; et al. Active Surveillance for Low-Risk Prostate Cancer Worldwide: The PRIAS Study. Eur. Urol. 2013, 63, 597–603. [Google Scholar] [CrossRef] [PubMed]
- Afshar-Oromieh, A.; Zechmann, C.M.; Malcher, A.; Eder, M.; Eisenhut, M.; Linhart, H.G.; Holland-Letz, T.; Hadaschik, B.A.; Giesel, F.L.; Debus, J.; et al. Comparison of PET Imaging with a 68Ga-Labelled PSMA Ligand and 18F-Choline-Based PET/CT for the Diagnosis of Recurrent Prostate Cancer. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Mottet, N.; van den Bergh, R.C.N.; Briers, E.; Cornford, P.; De Santis, M.; Fanti, S.; Gillessen, S.; Grummet, J.; Henry, A.M.; Lam, T.B.; et al. EAU—ESTRO—ESUR—SIOG Guidelines on Prostate Cancer 2020. In European Association of Urology Guidelines. 2020 Edition; European Association of Urology Guidelines Office: Arnhem, The Netherlands, 2020. [Google Scholar]
- Anttinen, M.; Ettala, O.; Malaspina, S.; Jambor, I.; Sandell, M.; Kajander, S.; Rinta-Kiikka, I.; Schildt, J.; Saukko, E.; Rautio, P.; et al. A Prospective Comparison of 18F-Prostate-Specific Membrane Antigen-1007 Positron Emission Tomography Computed Tomography, Whole-Body 1.5 T Magnetic Resonance Imaging with Diffusion-Weighted Imaging, and Single-Photon Emission Computed Tomography/Computed Tomography with Traditional Imaging in Primary Distant Metastasis Staging of Prostate Cancer (PROSTAGE). Eur. Urol. Oncol. 2020, S2588931120300900. [Google Scholar] [CrossRef]
- Adeleke, S.; Latifoltojar, A.; Sidhu, H.; Galazi, M.; Shah, T.T.; Clemente, J.; Davda, R.; Payne, H.A.; Chouhan, M.D.; Lioumi, M.; et al. Localising Occult Prostate Cancer Metastasis with Advanced Imaging Techniques (LOCATE Trial): A Prospective Cohort, Observational Diagnostic Accuracy Trial Investigating Whole–Body Magnetic Resonance Imaging in Radio-Recurrent Prostate Cancer. BMC Med. Imaging 2019, 19, 90. [Google Scholar] [CrossRef] [PubMed]
- Campli, E.; Delli Pizzi, A.; Seccia, B.; Cianci, R.; d’Annibale, M.; Antonella, C.; Cinalli, S.; Castellan, P.; Navarra, R.; Iantorno, R.; et al. Diagnostic Accuracy of Biparametric vs Multiparametric MRI in Clinically Significant Prostate Cancer: Comparison between Readers with Different Experience. Eur. J. Radiol. 2018, 101, 17–23. [Google Scholar] [CrossRef]
- Xu, L.; Zhang, G.; Shi, B.; Liu, Y.; Zou, T.; Yan, W.; Xiao, Y.; Xue, H.; Feng, F.; Lei, J.; et al. Comparison of Biparametric and Multiparametric MRI in the Diagnosis of Prostate Cancer. Cancer Imaging 2019, 19, 90. [Google Scholar] [CrossRef] [PubMed]
- Alabousi, M.; Salameh, J.-P.; Gusenbauer, K.; Samoilov, L.; Jafri, A.; Yu, H.; Alabousi, A. Biparametric vs. Multiparametric Prostate Magnetic Resonance Imaging for the Detection of Prostate Cancer in Treatment-Naïve Patients: A Diagnostic Test Accuracy Systematic Review and Meta-Analysis. BJU Int. 2019, 124, 209–220. [Google Scholar] [CrossRef] [PubMed]
- Pernický, J.; Tupý, R.; Cibulková, J.; Ferda, J. Changes in the prostate assessment using classification PI-RADS 2.1. Ceska Radiol. 2020, 74, 47–54. [Google Scholar]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).