
Determinants of Processing Speed Trajectories among Middle Aged or Older Adults, and Their Association with Chronic Illnesses: The English Longitudinal Study of Aging

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Setting
2.2. Measurements
2.2.1. Processing Speed Assessment
2.2.2. Baseline and Follow-Up Assessments
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Study Participants
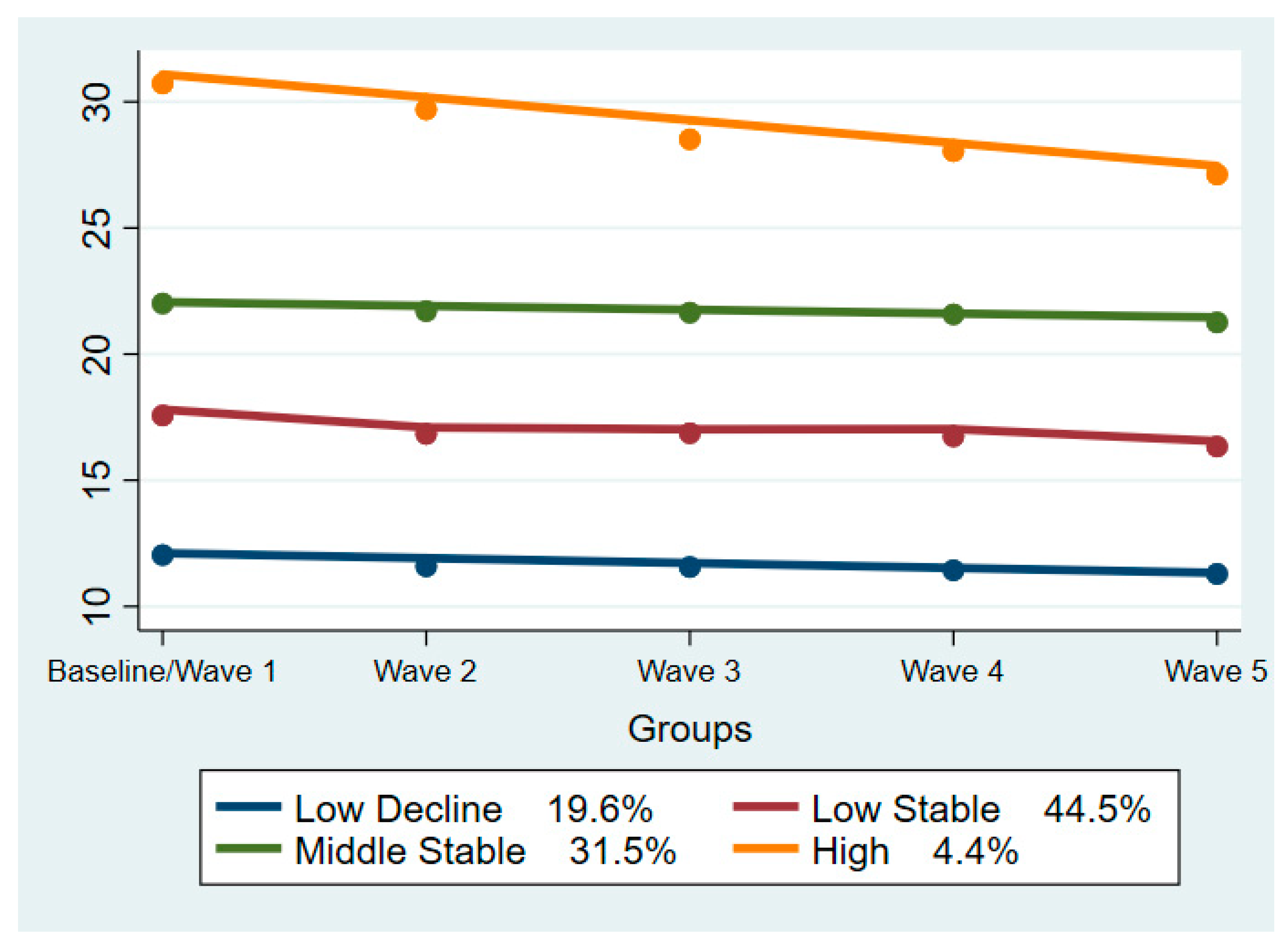
3.2. Trajectories of Processing Speed
3.3. Processing Speed Trajectories in Relation to Chronic Illnesses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A
Choice of Model

{kind=link}
| Groups | Polynomial Orders | BIC Value |
|---|---|---|
| 4 | 1311 | −117683 |
| 4 | 1312 | −117686 |
| 4 | 1111 | −117686 |
| 4 | 1411 | −117688 |
| 4 | 1112 | −117688 |
| 4 | 2311 | −117688 |
| .. | .. | .. |
| .. | .. | .. |
| 3 | 111 | −118358 |
| Group | APP |
|---|---|
| 1 | 0.82 |
| 2 | 0.77 |
| 3 | 0.82 |
| 4 | 0.89 |
| Wave | Number of Participants |
|---|---|
| 1 | 12,099 |
| 2 | 9432 |
| 3 | 9741 |
| 4 | 11,050 |
| 5 | 10,317 |
| Characteristic | Trajectory | |||
|---|---|---|---|---|
| Marital Status | Low Decline | Middle Decline | Middle Stable | High |
| Single | 219 (2%) | 268 (2.43%) | 51 (0.46%) | 21 (0.19%) |
| Married | 1762 (16%) | 4508 (40.91%) | 1100 (9.98%) | 164 (1.49%) |
| Separated, Divorced | 272 (2.47%) | 561 (5.1%) | 176 (1.6%) | 19 (0.17%) |
| Widowed | 516 (4.68%) | 1030 (9.35%) | 309 (2.8%) | 44 (0.4%) |
| Sex, males | 1749 (15.87%) | 2791 (25.33%) | 436 (3.96%) | 54 (0.5%) |
| Education | ||||
| Low | 1635 (16/27%) | 2497 (24.85%) | 486 (4.84%) | 83 (0.83%) |
| Medium | 800 (7.26%) | 2541 (23.06%) | 678 (6.15%) | 107 (0.97%) |
| High | 116 (1.05%) | 762 (6.91%) | 302 (2.74%) | 41 (0.37%) |
| Physical activity level | ||||
| No Physical Activity | ||||
| Mild | 903 (8.19%) | 2676 (24.28%) | 810 (7.35%) | 119 (1.08%) |
| Moderate | 671 (6.09%) | 1210 (10.1%) | 387 (3.51%) | 54 (0.5%) |
| Vigorous | 339 (3.08%) | 222 (2.01%) | 52 (0.47%) | 3 (0.03%) |
| NA values | ||||
| Ever smoked, yes | 1915 (17.38%) | 4103 (37.23%) | 946 (8.58%) | 149 (1.35%) |
| CVD, yes | 562 (5.1%) | 926 (8.4%) | 192 (1.72%) | 25 (0.23%) |
| Diabetes, yes | 265 (2.41%) | 452 (4.1%) | 88 (0.8%) | 13 (0.12%) |
| Depressive Symptoms, yes | 601 (5.54%) | 949 (8.75%) | 227 (2.09%) | 22 (0.2%) |
| Sleeping Disturbances, yes | 1554 (14.3%) | 3728 (34.31%) | 967 (8.9%) | 161 (1.48%) |
References
- Harvey, P.D. Domains of cognition and their assessment. Dialogues Clin. Neurosci. 2019, 21, 227–237. [Google Scholar] [CrossRef]
- Gale, C.R.; Allerhand, M.; Sayer, A.A.; Cooper, C.; Deary, I.J. The dynamic relationship between cognitive function and walking speed: The English Longitudinal Study of Ageing. Age 2014, 36, 9682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, D.C.; Reuter-Lorenz, P. The adaptive brain: Aging and neurocognitive scaffolding. Annu. Rev. Psychol. 2009, 60, 173–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh-Manoux, A.; Kivimaki, M.; Glymour, M.M.; Elbaz, A.; Berr, C.; Ebmeier, K.P.; Ferrie, J.E.; Dugravot, A. Timing of onset of cognitive decline: Results from Whitehall II prospective cohort study. BMJ 2012, 344, d7622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ridderinkhof, K.R.; van der Molen, M.W. Mental resources, processing speed, and inhibitory control: A developmental perspective. Biol. Psychol. 1997, 21, 241–261. [Google Scholar] [CrossRef]
- Salthouse, T.A. The processing-speed theory of adult age differences in cognition. Psychol. Rev. 1996, 103, 403–428. [Google Scholar] [CrossRef] [Green Version]
- Bott, N.T.; Bettcher, B.M.; Yokoyama, J.S.; Frazier, D.T.; Wynn, M.; Karydas, A.; Yaffe, K.; Kramer, J.H. Youthful Processing Speed in Older Adults: Genetic, Biological, and Behavioral Predictors of Cognitive Processing Speed Trajectories in Aging. Front. Aging Neurosci. 2017, 9, 55. [Google Scholar] [CrossRef] [Green Version]
- Steptoe, A.; Breeze, E.; Banks, J.; Nazroo, J. Cohort Profile: The English Longitudinal Study of Ageing. Int. J. Epidemiol. 2013, 42, 1640–1648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchez-Niubo, A.; Egea-Cortés, L.; Olaya, B.; Caballero, F.F.; Ayuso-Mateos, J.L.; Prina, M.; Bobak, M.; Arndt, H.; Tobiasz-Adamczyk, B.; Pająk, A.; et al. The Ageing Trajectories of Health-Longitudinal Opportunities and Synergies (ATHLOS) project. Int. J. Epidemiol. 2019, 48, 1052–1053. [Google Scholar] [CrossRef]
- de la Fuente, J.; Hjelmborg, J.; Wod, M.; de la Torre-Luque, A.; Caballero, F.F.; Christensen, K.; Ayuso-Mateos, J.L. Longitudinal Associations of Sensory and Cognitive Functioning: A Structural Equation Modeling Approach. J. Gerontol. B Psychol. Sci. Soc. Sci. 2019, 74, 1308–1316. [Google Scholar] [CrossRef] [PubMed]
- Nagin, D. Group-Based Modeling of Development; Harvard University Press: Cambridge, MA, USA, 2005. [Google Scholar]
- Nagin, D.S.; Odgers, C.L. Group-Based Trajectory Modeling in Clinical Research. Annu. Rev. Clin. Psychol. 2010, 6, 109–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, B.L.; Nagin, D.S. A Note on a Stata plugin for estimating group-based trajectory models. Sociol. Methods Res. 2013, 42, 608–613. [Google Scholar] [CrossRef]
- Olaya, B.; Bobak, M.; Haro, J.M.; Demakakos, P. Trajectories of Verbal Episodic Memory in Middle-Aged and Older Adults: Evidence from the English Longitudinal Study of Ageing. J. Am. Geriatr. Soc. 2017, 65, 1274–1281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zahodne, L.B.; Wall, M.M.; Schupf, N.; Mayeux, R.; Manly, J.J.; Stern, Y.; Brickman, A.M. Late-life memory trajectories in relation to incident dementia and regional brain atrophy. J. Neurol. 2015, 262, 2484–2490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terrera, G.M.; Brayne, C.; Matthews, F.; the CC75C Study Collaboration Group. One size fits all? Why we need more sophisticated analytical methods in the explanation of trajectories of cognition in older age and their potential risk factors. Int. Psychogeriatr. 2010, 22, 291–299. [Google Scholar] [CrossRef]
- Ferraro, O.E.; Guaita, A.; Villani, S. Cognitive, physical and disability trajectories in community-dwelling elderly people [published online ahead of print, 2021 Feb 16]. Aging Clin. Exp. Res. 2021. [Google Scholar] [CrossRef]
- McDowell, I.; Xi, G.; Lindsay, J.; Tierney, M. Mapping the connections between education and dementia. J. Clin. Exp. Neuropsychol. 2007, 29, 127–141. [Google Scholar] [CrossRef]
- Schmand, B.; Smit, J.; Lindeboom, J.; Smits, C.; Hooijer, C.; Jonker, C.; Deelman, B. Low education is a genuine risk factor for accelerated memory decline and dementia. J. Clin. Epidemiol. 1997, 50, 1025–1033. [Google Scholar] [CrossRef]
- Biddle, K.D.; Jacobs, H.I.L.; d’Oleire Uquillas, F.; Zide, B.S.; Kirn, D.R.; Properzi, M.R.; Rentz, D.M.; Johnson, K.A.; Sperling, R.A.; Donovan, N.J. Associations of Widowhood and β-Amyloid With Cognitive Decline in Cognitively Unimpaired Older Adults. JAMA Netw. Open 2020, 3, e200121. [Google Scholar] [CrossRef] [Green Version]
- Håkansson, K.; Rovio, S.; Helkala, E.-L.; Vilska, A.-R.; Winblad, B.; Soininen, H.; Nissinen, A.; Mohammed, A.H.; Kivipelto, M. Association between mid-life marital status and cognitive function in later life: Population based cohort study. BMJ 2009, 339, b2462. [Google Scholar] [CrossRef] [Green Version]
- Evans, I.E.; Martyr, A.; Collins, R.; Brayne, C.; Clare, L. Social Isolation and Cognitive Function in Later Life: A Systematic Review and Meta-Analysis. J. Alzheimer’s Dis. 2019, 70, S119–S144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Northey, J.M.; Cherbuin, N.; Pumpa, K.L.; Smee, D.J.; Rattray, B. Exercise interventions for cognitive function in adults older than 50: A systematic review with meta-analysis. Br. J. Sports Med. 2018, 52, 154–160. [Google Scholar] [CrossRef]
- Chang, H.; Kim, K.; Jung, Y.-J.; Kato, M. Effects of acute high-intensity resistance exercise on cognitive function and oxygenation in prefrontal cortex. J. Exerc. Nutr. Biochem. 2017, 21, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Gale, S.D.; Erickson, L.D.; Brown, B.L.; Woody, P.; Hedges, D.W. Cognitive function in older adults according to current socioeconomic status. Neuropsychol. Dev. Cogn. B Aging Neuropsychol. Cogn. 2015, 22, 534–543. [Google Scholar] [CrossRef] [PubMed]
- Stuckenschneider, T.; Askew, C.D.; Rüdiger, S.; Polidori, M.C.; Abeln, V.; Vogt, T.; Krome, A.; Rikkert, M.O.; Lawlor, B.; Schneider, S.; et al. Cardiorespiratory Fitness and Cognitive Function are Positively Related Among Participants with Mild and Subjective Cognitive Impairment. J. Alzheimer’s Dis. 2018, 62, 1865–1875. [Google Scholar] [CrossRef]
- Fillit, H.; Nash, D.T.; Rundek, T.; Zuckerman, A. Cardiovascular risk factors and dementia. Am. J. Geriatr. Pharmacother. 2008, 6, 100–118. [Google Scholar] [CrossRef]
- Moheet, A.; Mangia, S.; Seaquist, E.R. Impact of diabetes on cognitive function and brain structure. Ann. N. Y. Acad. Sci. 2015, 1353, 60–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marseglia, A.; Aslan, A.K.D.; Fratiglioni, L.; Santoni, G.; Pedersen, N.L.; Xu, W. Cognitive Trajectories of Older Adults With Prediabetes and Diabetes: A Population-Based Cohort Study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2018, 73, 400–406. [Google Scholar] [CrossRef]
- Rock, P.L.; Roiser, J.P.; Riedel, W.J.; Blackwell, A.D. Cognitive impairment in depression: A systematic review and meta-analysis. Psychol. Med. 2014, 44, 2029–2040. [Google Scholar] [CrossRef] [Green Version]

| Characteristic | Overall N = 12099 |
|---|---|
| Marital Status | |
| Single | 575 (4.75%) |
| Married | 8539 (70.58%) |
| Separated, Divorced | 1034 (8.55%) |
| Widowed | 1951 (16.13%) |
| Sex, males | 5335 (44.1%) |
| Education | |
| Low | 5008 (41.39%) |
| Medium | 4653 (38.46%) |
| High | 1388 (11.47%) |
| NA values | 1040 (8.5%) |
| Physical activity level | |
| No Physical Activity | 1835 (16.9%) |
| Mild | 4909 (45.22%) |
| Moderate | 2483 (22.87%) |
| Vigorous | 654 (6.02%) |
| NA values | 975 (9%) |
| Ever smoked, yes | 7623 (63%) |
| History of cardiovascular disease, yes | 1804 (15.9%) |
| History of Diabetes, yes | 866 (7.16%) |
| History of Depressive Symptoms, yes | 1923 (15.9%) |
| History of Sleeping Disturbances, yes | 6942 (57.38%) |
| Group | Parameter | OR | Lower 95%CL | Upper 95%CL | P-value |
|---|---|---|---|---|---|
| Low/Stable vs Low/Decline | Male vs Female | 0.425 | 0.357 | 0.505 | <0.001 |
| Education Level | |||||
| High vs Low | 2.672 | 1.846 | 3.868 | <0.001 | |
| Medium vs Low | 1.879 | 1.577 | 2.239 | <0.001 | |
| Marrital Status | |||||
| Widowed vs Never Married | 0.816 | 0.588 | 1.134 | 0.226 | |
| Separated or Divorced vs Never Married | 2.113 | 1.430 | 3.124 | <0.001 | |
| Married vs Never Married | 1.848 | 1.364 | 2.504 | <0.001 | |
| Level of Physical Activity (PA) | |||||
| Vigorous vs No PA | 0.333 | 0.247 | 0.449 | <0.001 | |
| Moderate vs No PA | 0.805 | 0.651 | 0.995 | 0.045 | |
| Mild vs No PA | 1.569 | 1.287 | 1.913 | <0.001 | |
| High Wealth | 1.716 | 1.463 | 2.013 | <0.001 | |
| Ever Smoked | 1.038 | 0.881 | 1.224 | 0.655 | |
| Middle/Stable vs Low/Decline | Male vs Female | 0.171 | 0.143 | 0.204 | <0.001 |
| Education Level | |||||
| High vs Low | 8.869 | 6.283 | 12.519 | <0.001 | |
| Medium vs Low | 3.485 | 2.923 | 4.155 | <0.001 | |
| Marrital Status | |||||
| Widowed vs Never Married | 0.771 | 0.528 | 1.127 | 0.180 | |
| Separated or Divorced vs Never Married | 3.747 | 2.456 | 5.717 | <0.001 | |
| Married vs Never Married | 3.097 | 2.189 | 4.382 | <0.001 | |
| Level of Physical Activity (PA) | |||||
| Vigorous vs No PA | 0.158 | 0.106 | 0.236 | <0.001 | |
| Moderate vs No PA | 0.733 | 0.595 | 0.902 | <0.003 | |
| Mild vs No PA | 1.527 | 1.260 | 1.850 | <0.001 | |
| High Wealth | 2.381 | 2.018 | 2.808 | <0.001 | |
| Ever Smoked | 0.938 | 0.798 | 1.104 | 0.442 | |
| High vs Low/Decline | Male vs Female | 0.100 | 0.075 | 0.134 | <0.001 |
| Education Level | |||||
| High vs Low | 12.389 | 7.923 | 19.373 | <0.001 | |
| Medium vs Low | 4.049 | 3.064 | 5.351 | <0.001 | |
| Marrital Status | |||||
| Widowed vs Never Married | 0.430 | 0.248 | 0.744 | 0.003 | |
| Separated or Divorced vs Never Married | 1.802 | 0.988 | 3.286 | 0.055 | |
| Married vs Never Married | 1.540 | 0.958 | 2.477 | 0.075 | |
| Level of Physical Activity (PA) | |||||
| Vigorous vs No PA | 0.119 | 0.046 | 0.308 | <0.001 | |
| Moderate vs No PA | 0.783 | 0.554 | 1.107 | 0.167 | |
| Mild vs No PA | 1.710 | 1.277 | 2.290 | <0.001 | |
| High Wealth | 1.963 | 1.496 | 2.577 | <0.001 | |
| Ever Smoked | 1.062 | 0.826 | 1.366 | 0.639 |
| Group | Outcome | Beta Estimate | Standard Error | p-value |
|---|---|---|---|---|
| Low/Decline | Cardiovascular disease | −0.354 | 0.211 | 0.094 |
| Depressive Symptoms | −0.967 | 0.161 | <0.001 | |
| Sleeping Disturbances | −0.461 | 0.132 | <0.001 | |
| Diabetes Mellitus | −0.433 | 0.205 | 0.035 | |
| Low /Stable | Cardiovascular disease | −0.871 | 0.154 | <0.001 |
| Depressive Symptoms | −0.542 | 0.112 | <0.001 | |
| Sleeping Disturbances | −0.121 | 0.082 | 0.139 | |
| Diabetes Mellitus | −0.636 | 0.142 | <0.001 | |
| Middle/Stable | Cardiovascular disease | −0.819 | 0.175 | <0.001 |
| Depressive Symptoms | −0.150 | 0.137 | 0.276 | |
| Sleeping Disturbances | −0.070 | 0.090 | 0.435 | |
| Diabetes Mellitus | −0.672 | 0.174 | <0.001 | |
| High | Cardiovascular disease | −5.214 | 0.998 | <0.001 |
| Depressive Symptoms | 0.507 | 0.404 | 0.209 | |
| Sleeping Disturbances | 0.577 | 0.272 | 0.034 | |
| Diabetes Mellitus | −0.939 | 0.504 | 0.062 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gkotzamanis, V.; Koliopanos, G.; Sanchez-Niubo, A.; Olaya, B.; Caballero, F.F.; Ayuso-Mateos, J.L.; Chatterji, S.; Haro, J.M.; Panagiotakos, D. Determinants of Processing Speed Trajectories among Middle Aged or Older Adults, and Their Association with Chronic Illnesses: The English Longitudinal Study of Aging. Life 2021, 11, 357. https://doi.org/10.3390/life11040357
Gkotzamanis V, Koliopanos G, Sanchez-Niubo A, Olaya B, Caballero FF, Ayuso-Mateos JL, Chatterji S, Haro JM, Panagiotakos D. Determinants of Processing Speed Trajectories among Middle Aged or Older Adults, and Their Association with Chronic Illnesses: The English Longitudinal Study of Aging. Life. 2021; 11(4):357. https://doi.org/10.3390/life11040357
Chicago/Turabian StyleGkotzamanis, Viktor, Giorgos Koliopanos, Albert Sanchez-Niubo, Beatriz Olaya, Francisco Félix Caballero, José Luis Ayuso-Mateos, Somnath Chatterji, Josep Maria Haro, and Demosthenes Panagiotakos. 2021. "Determinants of Processing Speed Trajectories among Middle Aged or Older Adults, and Their Association with Chronic Illnesses: The English Longitudinal Study of Aging" Life 11, no. 4: 357. https://doi.org/10.3390/life11040357
APA StyleGkotzamanis, V., Koliopanos, G., Sanchez-Niubo, A., Olaya, B., Caballero, F. F., Ayuso-Mateos, J. L., Chatterji, S., Haro, J. M., & Panagiotakos, D. (2021). Determinants of Processing Speed Trajectories among Middle Aged or Older Adults, and Their Association with Chronic Illnesses: The English Longitudinal Study of Aging. Life, 11(4), 357. https://doi.org/10.3390/life11040357