
First-Trimester Maternal Folic Acid Supplementation Modifies the Effects of Risk Factors Exposures on Congenital Heart Disease in Offspring

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Data Collection
2.3. Classification of CHD Phenotypes
2.4. CHD Risk Factors
2.5. First-Trimester Maternal FAS
2.6. Covariates
2.7. Statistical Analysis
3. Results
4. Discussion
4.1. Interaction Effects of FAS/Non-FAS, Viral Infection, and Fever on CHDs
4.2. Synergistic Effects of Non-FAS and Maternal Risk Factors on CHD Categories
4.3. Synergistic Effects of Non-FAS and Living in a Newly Renovated Home on CHDs
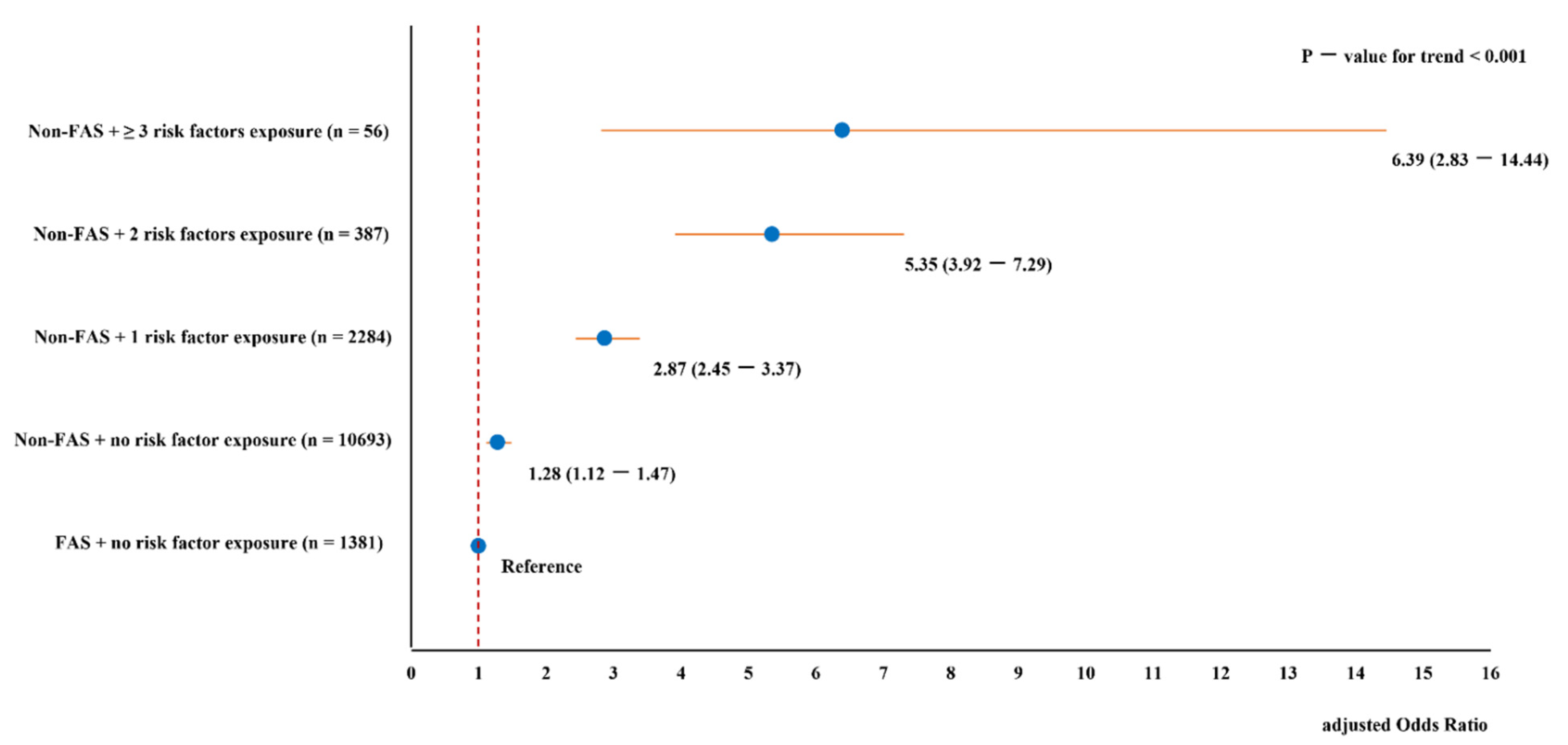
4.4. Dose Response and Joint Effects of Non-FAS and Risk Factors Exposures on CHDs
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Van der Linde, D.; Konings, E.E.M.; Slager, M.A.; Witsenburg, M.; Helbing, W.A.; Takkenberg, J.J.M.; Roos-Hesselink, J.W. Birth prevalence of congenital heart disease worldwide: A systematic review and meta-analysis. J. Am. Coll. Cardiol. 2011, 58, 2241–2247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dolk, H.; Loane, M.; Garne, E. Congenital heart defects in Europe: Prevalence and perinatal mortality, 2000 to 2005. Circulation 2011, 123, 841–849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Razzaghi, H.; Oster, M.; Reefhuis, J. Long-term outcomes in children with congenital heart disease: National Health Interview Survey. J. Pediatr. 2015, 166, 119–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collaborators, G. 2017 C.H.D. Global, regional, and national burden of congenital heart disease, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Child. Adolesc. Health 2020, 4, 185–200. [Google Scholar] [CrossRef] [Green Version]
- Nora, J.J. Multifactorial inheritance hypothesis for the etiology of congenital heart diseases. The genetic-environmental interaction. Circulation 1968, 38, 604–617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pierpont, M.E.; Basson, C.T.; Benson, D.W.J.; Gelb, B.D.; Giglia, T.M.; Goldmuntz, E.; McGee, G.; Sable, C.A.; Srivastava, D.; Webb, C.L. Genetic basis for congenital heart defects: Current knowledge: A scientific statement from the American Heart Association Congenital Cardiac Defects Committee, Council on Cardiovascular Disease in the Young: Endorsed by the American Academy of Pediatrics. Circulation 2007, 115, 3015–3038. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pierpont, M.E.; Brueckner, M.; Chung, W.K.; Garg, V.; Lacro, R.V.; McGuire, A.L.; Mital, S.; Priest, J.R.; Pu, W.T.; Roberts, A.; et al. Genetic Basis for Congenital Heart Disease: Revisited: A Scientific Statement from the American Heart Association. Circulation 2018, 138, e653–e711. [Google Scholar] [CrossRef]
- Russell, M.W.; Chung, W.K.; Kaltman, J.R.; Miller, T.A. Advances in the Understanding of the Genetic Determinants of Congenital Heart Disease and Their Impact on Clinical Outcomes. J. Am. Heart Assoc. 2018, 7. [Google Scholar] [CrossRef] [Green Version]
- Jenkins, K.J.; Correa, A.; Feinstein, J.A.; Botto, L.; Britt, A.E.; Daniels, S.R.; Elixson, M.; Warnes, C.A.; Webb, C.L. Noninherited risk factors and congenital cardiovascular defects: Current knowledge: A scientific statement from the American Heart Association Council on Cardiovascular Disease in the Young: Endorsed by the American Academy of Pediatrics. Circulation 2007, 115, 2995–3014. [Google Scholar] [CrossRef] [Green Version]
- Liang, Q.; Gong, W.; Zheng, D.; Zhong, R.; Wen, Y.; Wang, X. The influence of maternal exposure history to virus and medicine during pregnancy on congenital heart defects of fetus. Environ. Sci. Pollut. Res. Int. 2017, 24, 5628–5632. [Google Scholar] [CrossRef]
- Shi, Q.Y.; Zhang, J.B.; Mi, Y.Q.; Song, Y.; Ma, J.; Zhang, Y.L. Congenital heart defects and maternal fever: Systematic review and meta-analysis. J. Perinatol. 2014, 34, 677–682. [Google Scholar] [CrossRef]
- Ramakrishnan, A.; Lee, L.J.; Mitchell, L.E.; Agopian, A.J. Maternal Hypertension during Pregnancy and the Risk of Congenital Heart Defects in Offspring: A Systematic Review and Meta-analysis. Pediatr. Cardiol. 2015, 36, 1442–1451. [Google Scholar] [CrossRef]
- Ou, Y.; Mai, J.; Zhuang, J.; Liu, X.; Wu, Y.; Gao, X.; Nie, Z.; Qu, Y.; Chen, J.; Kielb, C.; et al. Risk factors of different congenital heart defects in Guangdong, China. Pediatr. Res. 2016, 79, 549–558. [Google Scholar] [CrossRef] [Green Version]
- Blue, G.M.; Kirk, E.P.; Sholler, G.F.; Harvey, R.P.; Winlaw, D.S. Congenital heart disease: Current knowledge about causes and inheritance. Med. J. Aust. 2012, 197, 155–159. [Google Scholar] [CrossRef]
- Feng, Y.; Wang, S.; Zhao, L.; Yu, D.; Hu, L.; Mo, X. Maternal reproductive history and the risk of congenital heart defects in offspring: A systematic review and meta-analysis. Pediatr. Cardiol. 2015, 36, 253–263. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Wang, L.; Yang, T.; Chen, L.; Zhao, L.; Wang, T.; Chen, L.; Ye, Z.; Zheng, Z.; Qin, J. Parental alcohol consumption and the risk of congenital heart diseases in offspring: An updated systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2020, 27, 410–421. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Chen, L.; Yang, T.; Wang, L.; Wang, T.; Zhang, S.; Chen, L.; Ye, Z.; Zheng, Z.; Qin, J. Parental smoking and the risk of congenital heart defects in offspring: An updated meta-analysis of observational studies. Eur. J. Prev. Cardiol. 2020, 27, 1284–1293. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Li, X.; Li, N.; Li, S.; Deng, K.; Lin, Y.; Chen, X.; You, F.; Li, J.; Mu, D.; et al. Association between maternal exposure to housing renovation and offspring with congenital heart disease: A multi-hospital case-control study. Environ. Health 2013, 12, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, A.; Cao, X.; Lu, Y.; Li, H.; Zhu, Q.; Chen, X.; Jiang, H.; Li, X. A Meta-Analysis of the Relationship Between Maternal Folic Acid Supplementation and the Risk of Congenital Heart Defects. Int. Heart J. 2016, 57, 725–728. [Google Scholar] [CrossRef] [Green Version]
- Yu, D.; Feng, Y.; Yang, L.; Da, M.; Fan, C.; Wang, S.; Mo, X. Maternal socioeconomic status and the risk of congenital heart defects in offspring: A meta-analysis of 33 studies. PLoS ONE 2014, 9, e111056. [Google Scholar] [CrossRef] [Green Version]
- Feng, Y.; Wang, S.; Chen, R.; Tong, X.; Wu, Z.; Mo, X. Maternal folic acid supplementation and the risk of congenital heart defects in offspring: A meta-analysis of epidemiological observational studies. Sci. Rep. 2015, 5, 8506. [Google Scholar] [CrossRef] [Green Version]
- Qu, Y.; Lin, S.; Zhuang, J.; Bloom, M.S.; Smith, M.; Nie, Z.; Mai, J.; Ou, Y.; Wu, Y.; Gao, X.; et al. First trimester maternal folic acid supplementation reduced risks of severe and most congenital heart diseases in offspring: A large case control study. J. Am. Heart Assoc. 2020. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Jin, L.; Meng, Q.; Gao, L.; Zhang, L.; Li, Z.; Ren, A. Changes in folic acid supplementation behaviour among women of reproductive age after the implementation of a massive supplementation programme in China. Public Health Nutr. 2015, 18, 582–588. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Nie, Z.; Chen, J.; Guo, X.; Ou, Y.; Chen, G.; Mai, J.; Gong, W.; Wu, Y.; Gao, X.; et al. Does maternal environmental tobacco smoke interact with social-demographics and environmental factors on congenital heart defects? Environ. Pollut. 2018, 234, 214–222. [Google Scholar] [CrossRef]
- Boyd, P.A.; Haeusler, M.; Barisic, I.; Loane, M.; Garne, E.; Dolk, H. Paper 1: The EUROCAT network--organization and processes. Birth Defects Res. A Clin. Mol. Teratol. 2011, 91 (Suppl. 1), S2–S15. [Google Scholar] [CrossRef] [PubMed]
- Slaughter, J.L.; Cua, C.L.; Notestine, J.L.; Rivera, B.K.; Marzec, L.; Hade, E.M.; Maitre, N.L.; Klebanoff, M.A.; Ilgenfritz, M.; Le, V.T.; et al. Early prediction of spontaneous Patent Ductus Arteriosus (PDA) closure and PDA-associated outcomes: A prospective cohort investigation. BMC Pediatr. 2019, 19, 333. [Google Scholar] [CrossRef] [Green Version]
- Nie, Z.; Yang, B.; Ou, Y.; Bloom, M.S.; Han, F.; Qu, Y.; Nasca, P.; Matale, R.; Mai, J.; Wu, Y.; et al. Maternal residential greenness and congenital heart defects in infants: A large case-control study in Southern China. Environ. Int. 2020, 142, 105859. [Google Scholar] [CrossRef]
- Liberman, R.F.; Getz, K.D.; Lin, A.E.; Higgins, C.A.; Sekhavat, S.; Markenson, G.R.; Anderka, M. Delayed diagnosis of critical congenital heart defects: Trends and associated factors. Pediatrics 2014, 134, e373–e381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Botto, L.D.; Lin, A.E.; Riehle-Colarusso, T.; Malik, S.; Correa, A. Seeking causes: Classifying and evaluating congenital heart defects in etiologic studies. Birth Defects Res. A Clin. Mol. Teratol. 2007, 79, 714–727. [Google Scholar] [CrossRef]
- Mouri, M.; Hall, H.; Rupp, T.J. Threatened Abortion; StatPearls: Treasure Island, FL, USA, 2021. [Google Scholar]
- Knol, M.J.; Egger, M.; Scott, P.; Geerlings, M.I.; Vandenbroucke, J.P. When one depends on the other: Reporting of interaction in case-control and cohort studies. Epidemiology 2009, 20, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Knol, M.J.; VanderWeele, T.J.; Groenwold, R.H.H.; Klungel, O.H.; Rovers, M.M.; Grobbee, D.E. Estimating measures of interaction on an additive scale for preventive exposures. Eur. J. Epidemiol. 2011, 26, 433–438. [Google Scholar] [CrossRef] [Green Version]
- Rayburn, W.F. Infectious diseases in pregnancy. Obstet. Gynecol. Clin. N. Am. 2014, 41, ix–x. [Google Scholar] [CrossRef]
- Ye, Z.; Wang, L.; Yang, T.; Chen, L.; Wang, T.; Chen, L.; Zhao, L.; Zhang, S.; Zheng, Z.; Luo, L.; et al. Maternal Viral Infection and Risk of Fetal Congenital Heart Diseases: A Meta-Analysis of Observational Studies. J. Am. Heart Assoc. 2019, 8, e011264. [Google Scholar] [CrossRef] [Green Version]
- Botto, L.D.; Lynberg, M.C.; Erickson, J.D. Congenital heart defects, maternal febrile illness, and multivitamin use: A population-based study. Epidemiology 2001, 12, 485–490. [Google Scholar] [CrossRef] [Green Version]
- Botto, L.D.; Erickson, J.D.; Mulinare, J.; Lynberg, M.C.; Liu, Y. Maternal fever, multivitamin use, and selected birth defects: Evidence of interaction? Epidemiology 2002, 13, 485–488. [Google Scholar] [CrossRef]
- Shaw, G.M.; Nelson, V.; Carmichael, S.L.; Lammer, E.J.; Finnell, R.H.; Rosenquist, T.H. Maternal periconceptional vitamins: Interactions with selected factors and congenital anomalies? Epidemiology 2002, 13, 625–630. [Google Scholar] [CrossRef]
- Lynberg, M.C.; Khoury, M.J.; Lu, X.; Cocian, T. Maternal flu, fever, and the risk of neural tube defects: A population-based case-control study. Am. J. Epidemiol. 1994, 140, 244–255. [Google Scholar] [CrossRef]
- Zhang, J.; Cai, W.W. Association of the common cold in the first trimester of pregnancy with birth defects. Pediatrics 1993, 92, 559–563. [Google Scholar] [PubMed]
- Mirkes, P.E.; Cornel, L.M.; Park, H.W.; Cunningham, M.L. Induction of thermotolerance in early postimplantation rat embryos is associated with increased resistance to hyperthermia-induced apoptosis. Teratology 1997, 56, 210–219. [Google Scholar] [CrossRef]
- Kvansakul, M. Viral Infection and Apoptosis. Viruses 2017, 9, 356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watanabe, M.; Choudhry, A.; Berlan, M.; Singal, A.; Siwik, E.; Mohr, S.; Fisher, S.A. Developmental remodeling and shortening of the cardiac outflow tract involves myocyte programmed cell death. Development 1998, 125, 3809–3820. [Google Scholar] [CrossRef] [PubMed]
- Huang, R.F.; Ho, Y.H.; Lin, H.L.; Wei, J.S.; Liu, T.Z. Folate deficiency induces a cell cycle-specific apoptosis in HepG2 cells. J. Nutr. 1999, 129, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Qu, Y.; Liu, X.; Zhuang, J.; Chen, G.; Mai, J.; Guo, X.; Ou, Y.; Chen, J.; Gong, W.; Gao, X.; et al. Incidence of Congenital Heart Disease: The 9-Year Experience of the Guangdong Registry of Congenital Heart Disease, China. PLoS ONE 2016, 11, e0159257. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Maternal Exposures | Total | CHD Case, n (%) | Control, n (%) | OR (95% CI) * |
|---|---|---|---|---|
| Total | 15297 | 8379 | 6918 | - |
| Maternal FAS † | ||||
| Yes | 1877 (12.3) | 928 (11.1) | 949 (13.7) | 0.69 (0.62-0.76) |
| No | 13,420 (87.7) | 7451 (88.9) | 5969 (86.3) | 1.00 (ref) |
| Maternal disease † | ||||
| Fever | ||||
| Yes | 371 | 306 (3.7) | 65 (0.9) | 2.41 (1.81–3.20) |
| No | 14,926 | 8073 (96.3) | 6853 (99.1) | 1.00 (Ref) |
| Viral infection | ||||
| Yes | 1114 | 885 (10.6) | 229 (3.3) | 3.00 (2.56–3.52) |
| No | 14,183 | 7494 (89.4) | 6689 (96.7) | 1.00 (Ref) |
| Hypertension | ||||
| Yes | 148 | 115 (1.4) | 33 (0.5) | 2.37 (1.52–3.70) |
| No | 15,149 | 8264 (98.6) | 6885 (99.5) | 1.00 (Ref) |
| Threatened abortion | ||||
| Yes | 727 | 546 (6.5) | 181 (2.6) | 1.95 (1.62–2.35) |
| No | 14,567 | 7831 (93.5) | 6736 (97.4) | 1.00 (Ref) |
| Reproductive history | ||||
| Previous pregnancies with birth defects | ||||
| Yes | 106 | 95 (1.1) | 11 (0.2) | 6.55 (3.48–12.35) |
| No | 15,191 | 8284 (98.9) | 6907 (99.8) | 1.00 (Ref) |
| Spontaneous/elective abortion history | ||||
| Yes | 1037 | 644 (7.7) | 393 (5.7) | 1.28 (1.12–1.47) |
| No | 14,260 | 7735 (92.3) | 6525 (94.3) | 1.00 (Ref) |
| Maternal lifestyle and environmental factors | ||||
| Alcohol consumption † | ||||
| Yes | 87 | 65 (0.8) | 22 (0.3) | 1.65 (0.99–2.73) |
| No | 15,210 | 8314 (99.2) | 6896 (99.7) | 1.00 (Ref) |
| Active Smoking † | ||||
| Yes | 141 | 119 (1.4) | 22 (0.3) | 1.38 (0.82–2.32) |
| No | 15,156 | 8260 (98.6) | 6896 (99.7) | 1.00 (Ref) |
| Living in newly renovated home ‡ | ||||
| Yes | 392 | 317 (3.8) | 75 (1.1) | 2.28 (1.74–2.99) |
| No | 14,905 | 8062 (96.2) | 6843 (98.9) | 1.00 (Ref) |
| Residing within 50 m of a high traffic roadway ‡ | ||||
| Yes | 1721 | 1076 (12.8) | 645 (9.3) | 1.16 (1.04–1.30) |
| No | 13,576 | 7303 (87.2) | 6273 (90.7) | 1.00 (Ref) |
| With FAS | Without FAS | ||||
|---|---|---|---|---|---|
| Strata of Maternal Exposures | CHD Cases/ Participants | OR * (95% CI) | CHD Cases/ Participants | OR * (95% CI) | p-Value for Multiplicative Interaction |
| Total | 928/1877 | - | 7451/13,420 | - | - |
| Maternal disease † | |||||
| Fever (>38 °C) | |||||
| Yes (n = 371) | 44/60 | 1.19 (0.59–2.42) | 262/311 | 2.72 (1.97–3.76) | 0.01 |
| No (n = 14,926) | 884/1817 | 1.00 (ref) | 7189/13,109 | 1.00 (ref) | |
| Viral infection ‡ | |||||
| Yes (n = 1114) | 157/218 | 2.45 (1.73–3.47) | 728/896 | 3.21 (2.68–3.85) | 0.01 |
| No (n = 14,183) | 771/1659 | 1.00 (ref) | 6723/12,524 | 1.00 (ref) | |
| Hypertension | |||||
| Yes (n = 148) | 12/18 | 3.17 (0.94–10.69) | 103/130 | 2.34 (1.44–3.82) | 0.90 |
| No (n = 15,149) | 916/1859 | 1.00 (ref) | 7348/13,290 | 1.00 (ref) | |
| Threatened abortion | |||||
| Yes (n = 727) | 96/152 | 1.60 (1.08–2.39) | 450/575 | 2.07 (1.67–2.56) | 0.05 |
| No (n = 14,570) | 832/1725 | 1.00 (ref) | 7001/12,845 | 1.00 (ref) | |
| Reproduction history | |||||
| Previous pregnancies with birth defects | |||||
| Yes (n = 106) | 13/15 | 4.85 (1.01–23.24) | 82/91 | 6.60 (3.28–13.28) | 0.61 |
| No (n = 15,191) | 915/1862 | 1.00 (ref) | 7369/13,329 | 1.00 (ref) | |
| Spontaneous/elective abortion history | |||||
| Yes (n = 1037) | 123/226 | 1.10 (0.78–1.54) | 521/811 | 1.23 (1.05–1.45) | 0.44 |
| No (n = 14,260) | 805/1651 | 1.00 (ref) | 6930/12,609 | 1.00 (ref) | |
| Maternal lifestyle and environmental factors | |||||
| Alcohol consumption † | |||||
| Yes (n = 87) | 9/10 | 5.45 (0.67–44.74) | 56/77 | 1.46 (0.86–2.47) | 0.11 |
| No (n = 15,210) | 919/1867 | 1.00 (ref) | 7395/13,343 | 1.00 (ref) | |
| Active smoking † | |||||
| Yes (n = 141) | 2/9 | 1.43 (0.26–7.75) | 20/132 | 1.34 (0.77–2.32) | 0.82 |
| No (n = 15,156) | 947/1868 | 1.00 (ref) | 5949/13,288 | 1.00 (ref) | |
| Living in newly renovated home ‡ | |||||
| Yes (n = 392) | 20/30 | 1.02 (0.42–2.51) | 297/360 | 2.54 (1.91–3.38) | 0.93 |
| No (n = 14,905) | 908/1847 | 1.00 (ref) | 7154/13,058 | 1.00 (ref) | |
| Residing within 50 m of a high traffic roadway ‡ | |||||
| Yes (n = 1721) | 94/158 | 1.29 (0.89–1.89) | 982/1563 | 1.13 (1.00–1.27) | 0.93 |
| No (n = 13,576) | 834/1719 | 1.00 (ref) | 6469/11,857 | 1.00 (ref) | |
| Maternal Exposures | OR00 (ref) (FAS, No Exposure) | OR10 (95% CI) (Non-FAS, No Exposure) | OR01 (95% CI) (FAS, Exposure) | OR11 (95% CI) (Non-FAS, Exposure) | RERI (95% CI) | AP (95% CI) | S (95% CI) |
|---|---|---|---|---|---|---|---|
| Maternal disease † | |||||||
| Fever | 1.00 | 1.53 (1.37–1.72) | 1.08 (0.58–2.00) | 4.30 (3.08–6.01) | 2.69 (1.18–4.21) | 0.63 (0.43–0.82) | 5.43 (1.65–17.83) |
| Viral infection | 1.00 | 1.50 (1.34–1.69) | 1.97 (1.42–2.73) | 4.73 (3.85–5.80) | 2.26 (1.22–3.29) | 0.48 (0.32–0.64) | 2.53 (1.56–4.10) |
| Gestational hypertension | 1.00 | 1.56 (1.39–1.75) | 1.82 (0.65–5.15) | 3.05 (1.92–4.85) | 0.67 (−1.67–3.00) | 0.22 (−0.49–0.93) | 1.48 (0.32–6.79) |
| Threatened abortion | 1.00 | 1.52 (1.36–1.71) | 1.33 (0.92–1.91) | 3.08 (2.43–3.90) | 1.23 (0.43–2.03) | 0.40 (0.20–0.60) | 2.45 (1.27–4.73) |
| Reproductive history | |||||||
| Previous pregnancy with birth defect | 1.00 | 1.40 (1.23–1.58) | 4.49 (0.96–21.05) | 9.78 (4.83–19.82) | 4.90 (−4.83–14.63) | 0.00 (−0.29–1.29) | 2.26 (0.32–15.8) |
| Spontaneous/elective abortion history | 1.00 | 1.39 (1.22–1.57) | 1.17 (0.86–1.58) | 1.80 (1.49–2.18) | 0.24 (−0.20–0.69) | 0.14 (−0.10–0.37) | 1.44 (0.69–3.00) |
| Maternal lifestyle and environmental factors | |||||||
| Alcohol consumption † | 1.00 | 1.57 (1.40–1.76) | 8.23 (1.02–66.39) | 2.28 (1.34–3.90) | −6.51 (−23.72–10.7) | −2.85 (−10.63–4.92) | 0.16 (0.02–1.80) |
| Active smoking † | 1.00 | 1.40 (1.24–1.59) | 1.23 (0.23–6.66) | 1.77 (1.01–3.09) | 1.43 (−2.17–5.02) | 0.47 (0.09–0.84) | 3.25 (1.07–9.86) |
| Living in newly renovated home ‡ | 1.00 | 1.54 (1.38–1.73) | 0.87 (0.39–1.93) | 3.92 (2.89–5.32) | 2.51 (1.19–3.84) | 0.64 (0.44–0.84) | 7.14 (1.20–42.34) |
| Residing within 50 m of a high traffic roadway ‡ | 1.00 | 1.56 (1.39–1.75) | 1.07 (0.75–1.54) | 1.70 (1.46–1.99) | 0.07 (−0.36–0.50) | 0.04 (−0.21–0.29) | 1.11 (0.57–2.17) |
| Exposures | n | OR (95% CI) * |
|---|---|---|
| FAS + No risk factor exposure | 1381 | 1.00 (Reference) |
| Non-FAS + Viral infection + Living in newly renovated home | 30 | 4.45 (1.74–11.40) |
| Non-FAS + Viral infection + Threatened abortion | 42 | 4.87 (2.17–10.92) |
| Non-FAS + Fever + Living in newly renovated home | 6 | 5.63 (0.61–52.35) |
| Non-FAS + Threatened abortion + Living in newly renovated home | 94 | 6.19 (2.77–13.86) |
| Non-FAS + Fever + Viral infection | 92 | 6.33 (3.47–11.56) |
| Non-FAS + Fever + Threatened abortion | 17 | 7.19 (1.58–32.62) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qu, Y.; Lin, S.; Bloom, M.S.; Wang, X.; Nie, Z.; Ou, Y.; Mai, J.; Gao, X.; Wu, Y.; Chen, J.; et al. First-Trimester Maternal Folic Acid Supplementation Modifies the Effects of Risk Factors Exposures on Congenital Heart Disease in Offspring. Life 2021, 11, 724. https://doi.org/10.3390/life11080724
Qu Y, Lin S, Bloom MS, Wang X, Nie Z, Ou Y, Mai J, Gao X, Wu Y, Chen J, et al. First-Trimester Maternal Folic Acid Supplementation Modifies the Effects of Risk Factors Exposures on Congenital Heart Disease in Offspring. Life. 2021; 11(8):724. https://doi.org/10.3390/life11080724
Chicago/Turabian StyleQu, Yanji, Shao Lin, Michael S. Bloom, Ximeng Wang, Zhiqiang Nie, Yanqiu Ou, Jinzhuang Mai, Xiangmin Gao, Yong Wu, Jimei Chen, and et al. 2021. "First-Trimester Maternal Folic Acid Supplementation Modifies the Effects of Risk Factors Exposures on Congenital Heart Disease in Offspring" Life 11, no. 8: 724. https://doi.org/10.3390/life11080724
APA StyleQu, Y., Lin, S., Bloom, M. S., Wang, X., Nie, Z., Ou, Y., Mai, J., Gao, X., Wu, Y., Chen, J., Justino, J., Tan, H., Zhuang, J., & Liu, X. (2021). First-Trimester Maternal Folic Acid Supplementation Modifies the Effects of Risk Factors Exposures on Congenital Heart Disease in Offspring. Life, 11(8), 724. https://doi.org/10.3390/life11080724