
Efficacy of Different Types of Therapy for COVID-19: A Comprehensive Review


 , , ,
, , , 
Abstract
:1. Introduction
2. Results and Discussion
2.1. Antiviral Therapies
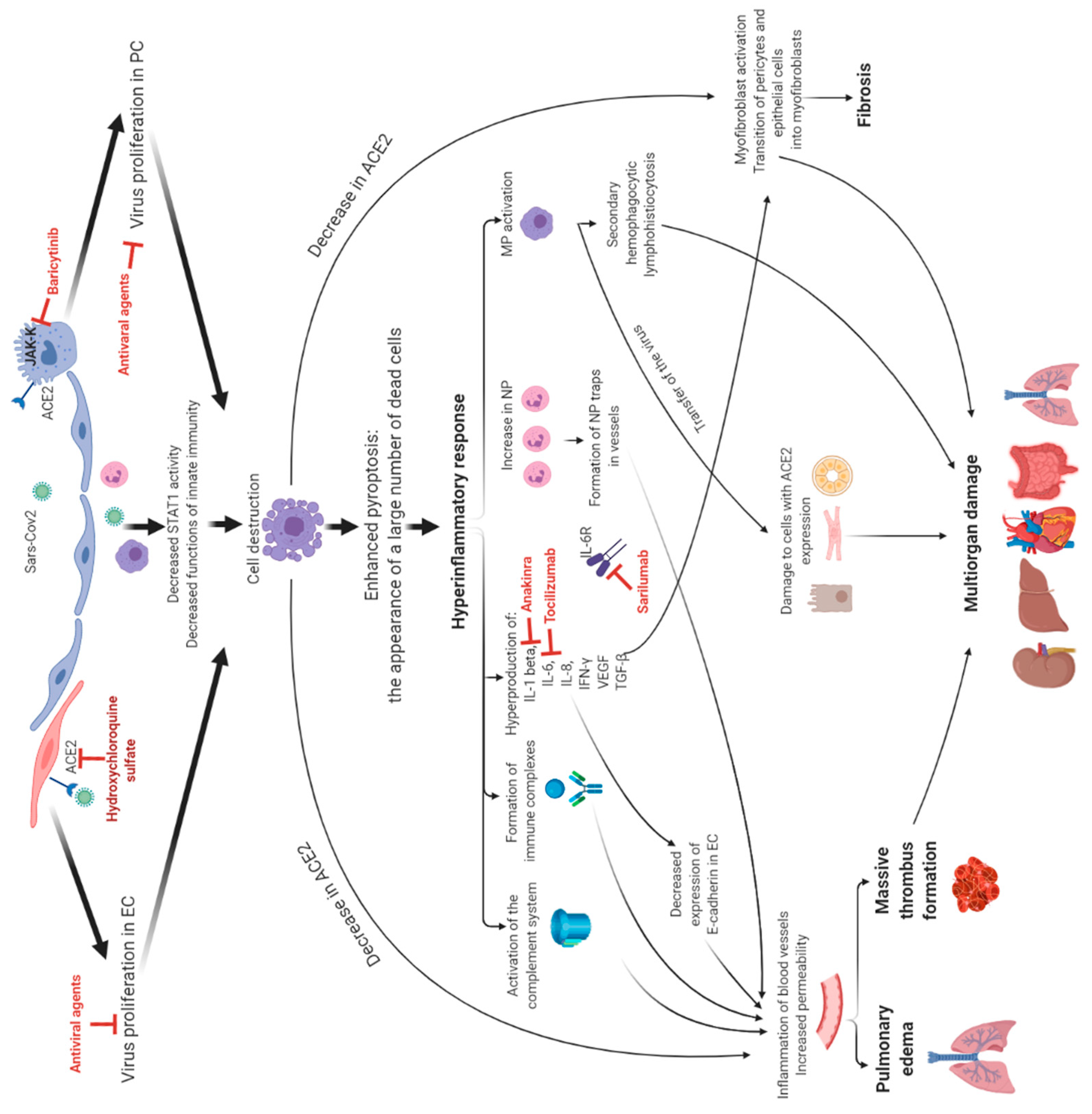
2.2. Immune Therapy
- Kinase inhibitors;
- Polyclonal antibodies by plasma therapy;
- Intravenous immunoglobulin IgG (IVIG);
- Polypeptide hormone for maturation of T cells.
2.2.1. Monoclonal Antibodies against Cytokines and Their Receptors
2.2.2. The Kinase Inhibitors
2.2.3. Intravenous Immunoglobulin IgG (IVIG)
2.2.4. Convalescent Plasma Transfusion
2.2.5. Polypeptide Hormone for Maturation of T Cells
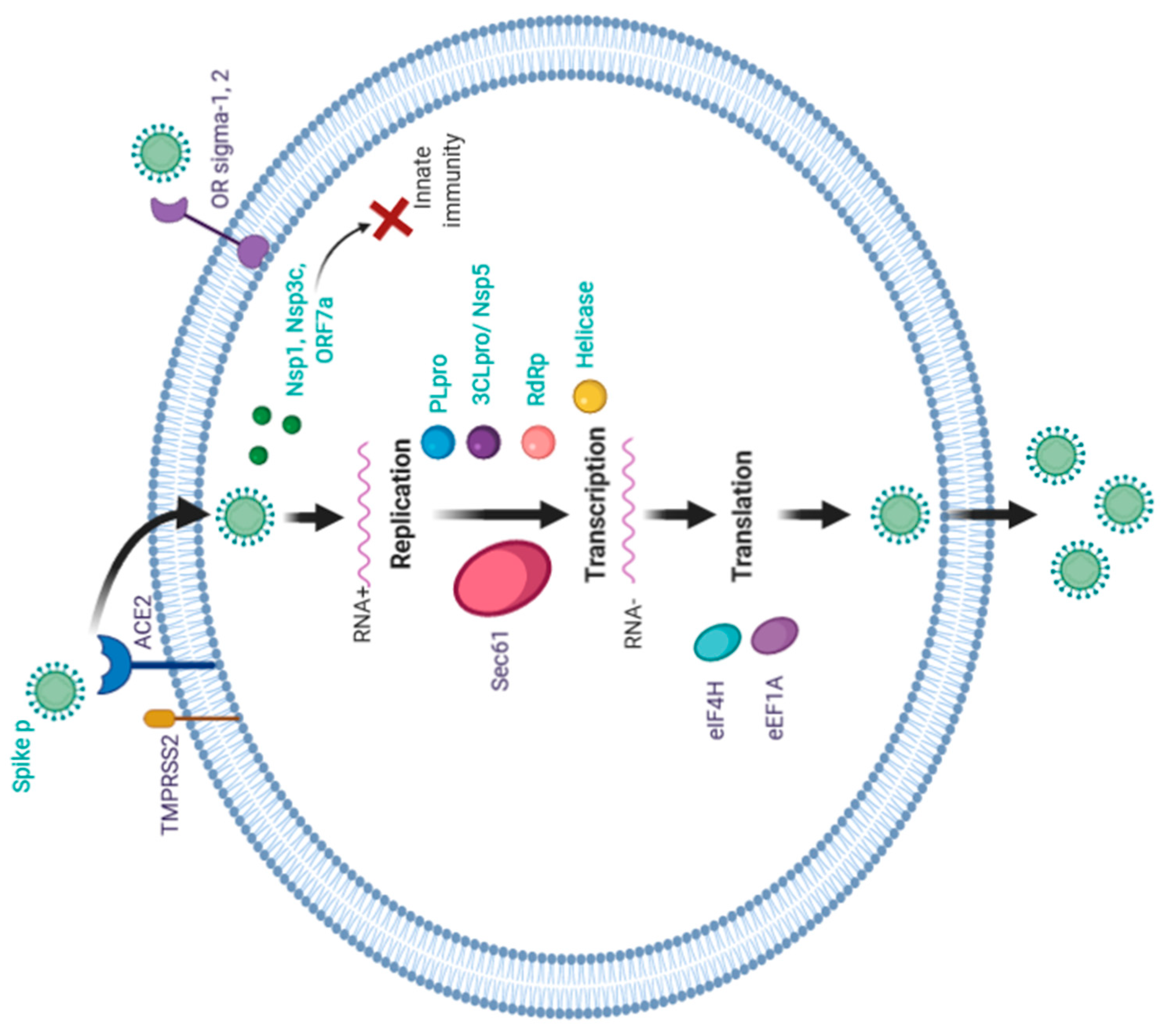
3. Possible Therapy Targets for COVID Treatment
- Enzymes or functional proteins for RNA synthesis and replication, for example: Nsp3 (Nsp3b, e Papain-like proteinase (PLpro)), Nsp7*Nsp8 complex, Nsp9eNsp10, Nsp14eNsp16, Nsp5 (3CLpro), Nsp12 (RdRp), Nsp13 (Helicase);
- Structural proteins for binding to human cell receptors, for example: Spike protein, E-channel, C-terminal RNA binding domain (CRBD), N-terminal RNA binding domain (NRBD);
- Virulence factors damaging the host’s innate immunity, for example: Nsp1, Nsp3c, ORF7a;
- The host’s specific receptors or enzymes, for example: TMPRSSS2, ACE2.
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Emergency Use ICD Codes for COVID-19 Disease Outbreak; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- WHO. Coronavirus Disease (COVID-19) Pandemic; WHO: Geneva, Switzerland, 2020; Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 5 May 2021).
- Tagarro, A.; Epalza, C.; Santos, M.; Sanz-Santaeufemia, F.J.; Otheo, E.; Moraleda, C.; Calvo, C. Screening and Severity of Coronavirus Disease 2019 (COVID-19) in Children in Madrid, Spain. JAMA Pediatr. 2021, 175, 316–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.; Liang, X.; Bi, Z.; Ren, J.; Wang, B.; Li, L. Consideration on the strategies during epidemic stage changing from emergency response to continuous prevention and control. Chin. J. Endem. 2020, 41, 297–300. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Wölfel, R.; Corman, V.M.; Guggemos, W.; Seilmaier, M.; Zange, S.; Müller, M.A.; Niemeyer, D.; Jones, T.C.; Vollmar, P.; Rothe, C.; et al. Virological assessment of hospitalized patients with COVID-2019. Nature 2020, 581, 465–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rothe, C.; Schunk, M.; Sothmann, P.; Bretzel, G.; Froeschl, G.; Wallrauch, C.; Zimmer, T.; Thiel, V.; Janke, C.; Guggemos, W.; et al. Transmission of 2019-nCoV Infection from an Asymptomatic Contact in Germany. N. Engl. J. Med. 2020, 382, 970–971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, L.; Lu, L.; Cao, W.; Li, T. Hypothesis for potential pathogenesis of SARS-CoV-2 infection–a review of immune changes in patients with viral pneumonia. Emerg. Microbes Infect. 2020, 9, 727–732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sims, A.C.; Baric, R.S.; Yount, B.; Burkett, S.E.; Collins, P.L.; Pickles, R.J. Severe Acute Respiratory Syndrome Coronavirus Infection of Human Ciliated Airway Epithelia: Role of Ciliated Cells in Viral Spread in the Conducting Airways of the Lungs. J. Virol. 2005, 79, 15511–15524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guan, W.; Ni, Z.; Hu, Y.; Liang, W.; Ou, C.; He, J.; Liu, L.; Shan, H.; Lei, C.; Hui, D.S.C.; et al. Clinical characteristics of 2019 novel coronavirus infection in China. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- Babcock, G.J.; Esshaki, D.J.; Thomas, W.D.; Ambrosino, D.M. Amino Acids 270 to 510 of the Severe Acute Respiratory Syndrome Coronavirus Spike Protein Are Required for Interaction with Receptor. J. Virol. 2004, 78, 4552–4560. [Google Scholar] [CrossRef] [Green Version]
- Wong, S.K.; Li, W.; Moore, M.J.; Choe, H.; Farzan, M. A 193-Amino Acid Fragment of the SARS Coronavirus S Protein Efficiently Binds Angiotensin-converting Enzyme 2. J. Biol. Chem. 2004, 279, 3197–3201. [Google Scholar] [CrossRef] [Green Version]
- Xiao, X.; Chakraborti, S.; Dimitrov, A.S.; Gramatikoff, K.; Dimitrov, D.S. The SARS-CoV S glycoprotein: Expression and functional characterization. Biochem. Biophys. Res. Commun. 2003, 312, 1159–1164. [Google Scholar] [CrossRef] [PubMed]
- Harmer, D.; Gilbert, M.; Borman, R.; Clark, K.L. Quantitative mRNA expression profiling of ACE 2, a novel homologue of angiotensin converting enzyme. FEBS Lett. 2002, 532, 107–110. [Google Scholar] [CrossRef] [Green Version]
- Letko, M.; Marzi, A.; Munster, V. Functional assessment of cell entry and receptor usage for SARS-CoV-2 and other lineage B betacoronaviruses. Nat. Microbiol. 2020, 5, 562–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamming, I.; Timens, W.; Bulthuis, M.L.C.; Lely, A.T.; Navis, G.J.; van Goor, H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J. Pathol. 2004, 203, 631–637. [Google Scholar] [CrossRef]
- Giani, M.; Seminati, D.; Lucchini, A.; Foti, G.; Pagni, F. Exuberant Plasmocytosis in Bronchoalveolar Lavage Specimen of the First Patient Requiring Extracorporeal Membrane Oxygenation for SARS-CoV-2 in Europe. J. Thorac. Oncol. 2020, 15, e65–e66. [Google Scholar] [CrossRef]
- Ehrenfeld, M.; Tincani, A.; Andreoli, L.; Cattalini, M.; Greenbaum, A.; Kanduc, D.; Alijotas-Reig, J.; Zinserling, V.; Semenova, N.; Amital, H.; et al. Covid-19 and autoimmunity. Autoimmun. Rev. 2020, 19, 102597. [Google Scholar] [CrossRef]
- Blanco-Melo, D.; Nilsson-Payant, B.E.; Liu, W.C.; Uhl, S.; Hoagland, D.; Møller, R.; Jordan, T.X.; Oishi, K.; Panis, M.; Sachs, D.; et al. Imbalanced Host Response to SARS-CoV-2 Drives Development of COVID-19. Cell 2020, 181, 1036–1045. [Google Scholar] [CrossRef]
- Chen, I.Y.; Moriyama, M.; Chang, M.F.; Ichinohe, T. Severe acute respiratory syndrome coronavirus viroporin 3a activates the NLRP3 inflammasome. Front. Microbiol. 2019, 10, 50. [Google Scholar] [CrossRef] [Green Version]
- Loppnow, H.; Libby, P. Proliferating or interleukin 1-activated human vascular smooth muscle cells secrete copious interleukin 6. J. Clin. Investig. 1990, 85, 731–738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavalli, E.; Petralia, M.C.; Basile, M.S.; Bramanti, A.; Bramanti, P.; Nicoletti, F.; Spandidos, D.A.; Shoenfeld, Y.; Fagone, P. Transcriptomic analysis of covid-19 lungs and bronchoalveolar lavage fluid samples reveals predominant b cell activation responses to infection. Int. J. Mol. Med. 2020, 46, 1266–1273. [Google Scholar] [CrossRef] [PubMed]
- Solun, B.; Shoenfeld, Y. Inhibition of metalloproteinases in therapy for severe lung injury due to COVID-19. Med. Drug Discov. 2020, 7, 100052. [Google Scholar] [CrossRef]
- Cao, B.; Wang, Y.; Wen, D.; Liu, W.; Wang, J.; Fan, G.; Ruan, L.; Song, B.; Cai, Y.; Wei, M.; et al. A Trial of Lopinavir–Ritonavir in Adults Hospitalized with Severe Covid-19. N. Engl. J. Med. 2020, 382, 1787–1799. [Google Scholar] [CrossRef]
- Li, Y.; Xie, Z.; Lin, W.; Cai, W.; Wen, C.; Guan, Y.; Mo, X.; Wang, J.; Wang, Y.; Peng, P.; et al. Efficacy and Safety of Lopinavir/Ritonavir or Arbidol in Adult Patients with Mild/Moderate COVID-19: An Exploratory Randomized Controlled Trial. Med 2020, 1, 105–113. [Google Scholar] [CrossRef]
- Gautret, P.; Lagier, J.-C.; Parola, P.; Hoang, V.T.; Meddeb, L.; Mailhe, M.; Doudier, B.; Courjon, J.; Giordanengo, V.; Vieira, V.E.; et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: Results of an open-label non-randomized clinical trial. medRxiv 2020. [Google Scholar] [CrossRef] [PubMed]
- Gautret, P.; Lagier, J.-C.; Parola, P.; Hoang, V.T.; Meddeb, L.; Mailhe, M.; Doudier, B.; Courjon, J.G.V. Clinical and microbiological effect of a combination of hydroxychloroquine and azithromycin in 80 COVID-19 patients with at least a six-day follow up: A pilot observational study. Travel Med. Infect. Dis. 2020, 34, 101663. [Google Scholar] [CrossRef] [PubMed]
- Geleris, J.; Sun, Y.; Platt, J.; Zucker, J.; Baldwin, M.; Hripcsak, G.; Labella, A.; Manson, D.K.; Kubin, C.; Barr, G.; et al. Observational Study of Hydroxychloroquine in Hospitalized Patients with Covid-19. N. Engl. J. Med. 2020, 382, 2411–2418. [Google Scholar] [CrossRef]
- Grein, J.; Ohmagari, N.; Shin, D.; Diaz, G.; Asperges, E.; Castagna, A.; Feldt, T.; Green, G.; Green, M.L.; Lescure, F.-X.; et al. Compassionate Use of Remdesivir for Patients with Severe COVID-19. N. Engl. J. Med. 2020, 382, 2327–2336. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhang, D.; Du, G.; Du, R.; Zhao, J.; Jin, Y.; Fu, S.; Gao, L.; Cheng, Z.; Lu, Q.; et al. Remdesivir in adults with severe COVID-19: A randomised, double-blind, placebo-controlled, multicentre trial. Lancet 2020, 395, 1569–1578. [Google Scholar] [CrossRef]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of COVID-19—Final Report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef] [PubMed]
- Goldman, J.D.; Lye, C.B.D.; Hui, S.D.; Marks, M.K.; Bruno, R.; Montejano, R.; Spinner, D.C.; Galli, M.; Ahn, M.-Y.; Nahass, G.R.; et al. Remdesivir for 5 or 10 Days in Patients with Severe COVID-19. N. Engl. J. Med. 2020, 383, 1827–1837. [Google Scholar] [CrossRef] [PubMed]
- Boulware, D.R.; Pullen, M.F.; Bangdiwala, A.S.; Pastick, K.A.; Lofgren, S.M.; Okafor, E.C.; Skipper, C.P.; Nascene, A.A.; Nicol, M.R.; Abassi, M.; et al. A Randomized Trial of Hydroxychloroquine as Postexposure Prophylaxis for COVID-19. N. Engl. J. Med. 2020, 383, 517–525. [Google Scholar] [CrossRef] [PubMed]
- Freedberg, D.E.; Conigliaro, J.; Wang, T.C.; Tracey, K.J.; Callahan, M.V.; Abrams, J.A. Famotidine Research Group. Famotidine Use Is Associated With Improved Clinical Outcomes in Hospitalized COVID-19 Patients: A Propensity Score Matched Retrospective Cohort Study. Gastroenterology 2020, 159, 1129–1131. [Google Scholar] [CrossRef] [PubMed]
- Horby, P.W.; Mafham, M.; Linsell, L.; Bell, J.L.; Staplin, N.; Emberson, J.R.; Wiselka, M.; Ustianowski, A.; Elmahi, E.; Prudon, B.; et al. Effect of hydroxychloroquine in hospitalized patients with COVID-19: Preliminary results from a multi-centre, randomized, controlled trial. medRxiv 2020. [Google Scholar] [CrossRef]
- Mather, J.F.; Seip, R.L.; McKay, R.G. Impact of Famotidine Use on Clinical Outcomes of Hospitalized Patients With COVID-19. Am. J. Gastroenterol. 2020, 115, 1617–1623. [Google Scholar] [CrossRef] [PubMed]
- Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; Elmahi, E.; et al. Dexamethasone in Hospitalized Patients with Covid-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- AminJafari, A.; Ghasemi, S. The possible of immunotherapy for COVID-19: A systematic review. Int. Immunopharmacol. 2020, 83. [Google Scholar] [CrossRef]
- Cavalli, G.; De Luca, G.; Campochiaro, C.; Della-Torre, E.; Ripa, M.; Canetti, D.; Oltolini, C.; Castiglioni, B.; Din, C.T.; Boffini, N.; et al. Interleukin-1 blockade with high-dose anakinra in patients with COVID-19, acute respiratory distress syndrome, and hyperinflammation: A retrospective cohort study. Lancet Rheumatol. 2020, 2, e325–e331. [Google Scholar] [CrossRef]
- Pontali, E.; Volpi, S.; Signori, A.; Antonucci, G.; Castellaneta, M.; Buzzi, D.; Montale, A.; Bustaffa, M.; Angelelli, A.; Caorsi, R.; et al. Efficacy of early anti-inflammatory treatment with high doses of intravenous anakinra with or without glucocorticoids in patients with severe COVID-19 pneumonia. J. Allergy Clin. Immunol. 2021, 147, 1217–1225. [Google Scholar] [CrossRef]
- Ucciferri, C.; Auricchio, A.; Di Nicola, M.; Potere, N.; Abbate, A.; Cipollone, F.; Vechhiet, J.; Falasca, K. Canakinumab in a subgroup of patients with COVID-19. Lancet Rheumatol. 2020, 2, e457–e458. [Google Scholar] [CrossRef]
- Xu, X.; Han, M.; Li, T.; Sun, W.; Wang, D.; Fu, B.; Zhou, Y.; Zheng, X.; Yang, Y.; Li, X.; et al. Effective treatment of severe COVID-19 patients with tocilizumab. Proc. Natl. Acad. Sci. USA 2020, 117, 10970–10975. [Google Scholar] [CrossRef] [PubMed]
- Malekzadeh, R.; Abedini, A.; Mohsenpour, B.; Sharifipour, E.; Ghasemian, R.; Javad-Mousavi, S.A.; Khodashahi, R.; Darban, M.; Kalantari, S.; Abdollahi, N.; et al. Subcutaneous tocilizumab in adults with severe and critical COVID-19: A prospective open-label uncontrolled multicenter trial. Int. Immunopharmacol. 2020, 89, 107102. [Google Scholar] [CrossRef]
- Stone, J.H.; Frigault, M.J.; Serling-Boyd, N.J.; Fernandes, A.D.; Harvey, L.; Foulkes, A.S.; Horick, N.K.; Healy, B.C.; Shah, R.; Bensaci, A.M.; et al. Efficacy of Tocilizumab in Patients Hospitalized with COVID-19. N. Engl. J. Med. 2020, 383, 2333–2344. [Google Scholar] [CrossRef] [PubMed]
- Alattar, R.; Ibrahim, T.B.N.; Shaar, S.H.; Abdalla, S.A.; Shukri, K.; Daghfal, J.N.; Khatib, M.Y.; Abukhattab, M.; Hussam, A.; Alsoub, H.A.; et al. Tocilizumab for the treatment of severe coronavirus disease 2019. J. Med. Virol. 2020, 92, 2042–2049. [Google Scholar] [CrossRef]
- Tsai, A.; Diawara, O.; Nahass, R.G.; Brunetti, L. Impact of tocilizumab administration on mortality in severe COVID-19. medRxiv 2020. [Google Scholar] [CrossRef] [PubMed]
- Klopfenstein, T.; Zayet, S.; Lohse, A.; Balblanc, J.C.; Badie, J.; Royer, P.Y.; Toko, L.; Mezher, C.; Kadiane-Oussou, N.J.; Bossert, M.; et al. Tocilizumab therapy reduced intensive care unit admissions and/or mortality in COVID-19 patients. Med. Mal. Infect. 2020, 50, 397–400. [Google Scholar] [CrossRef] [PubMed]
- Toniati, P.; Piva, S.; Cattalini, M.; Garrafa, E.; Regola, F.; Castelli, F.; Franceschini, F.; Airò, P.; Bazzani, C.; Beindorf, E.-A.; et al. Tocilizumab for the treatment of severe COVID-19 pneumonia with hyperinflammatory syndrome and acute respiratory failure: A single center study of 100 patients in Brescia, Italy. Autoimmun. Rev. 2020, 19, 102568. [Google Scholar] [CrossRef] [PubMed]
- Guaraldi, G.; Meschiari, M.; Cozzi-Lepri, A.; Milic, J.; Tonelli, R.; Menozzi, M.; Franceschini, E.; Cuomo, G.; Orlando, G.; Borghi, V.; et al. Tocilizumab in patients with severe COVID-19: A retrospective cohort study. Lancet Rheumatol. 2020, 2, e474–e484. [Google Scholar] [CrossRef]
- Potere, N.; Di Nisio, M.; Cibelli, D.; Scurti, R.; Frattari, A.; Porreca, E.; Abbate, A.; Parruti, G. Interleukin-6 receptor blockade with subcutaneous tocilizumab in severe COVID-19 pneumonia and hyperinflammation: A case-control study. Ann. Rheum. Dis. 2021, 80, 271–272. [Google Scholar] [CrossRef] [PubMed]
- Rojas-Marte, G.; Khalid, M.; Mukhtar, O.; Hashmi, A.T.; Waheed, M.A.; Ehrlich, S.; Aslam, A.; Siddiqui, S.; Agarwal, C.; Malyshev, Y.; et al. Outcomes in patients with severe COVID-19 disease treated with tocilizumab: A case-controlled study. QJM Int. J. Med. 2020, 113, 546–550. [Google Scholar] [CrossRef]
- Colaneri, M.; Bogliolo, L.; Valsecchi, P.; Sacchi, P.; Zuccaro, V.; Brandolino, F.; Montecucco, C.; Mojoli, F.; Giusti, E.M.; Bruno, R.; et al. Tocilizumab for treatment of severe COVID-19 patients: Preliminary results from smatteo COVID19 registry (smacore). Microorganisms 2020, 8, 695. [Google Scholar] [CrossRef]
- Tarrytown, N.Y. Regeneron and Sanofi Provide Update on U.S. Phase 2/3 Adaptive-Designed Trial of Kevzara® (Sarilumab) in Hospitalized COVID-19 Patients. Regen. Pharm. Inc. 2020. Available online: https://investor.regeneron.com/news-releases/news-release-details/regeneron-and-sanofi-provide-update-us-phase-23-adaptive/ (accessed on 5 July 2021).
- Sciascia, S.; Aprà, F.; Baffa, A.; Baldovino, S.; Boaro, D.; Boero, R.; Bonora, S.; Calcagno, A.; Cecchi, I.; Cinnirella, G.; et al. Pilot prospective open, single-arm multicentre study on off-label use of tocilizumab in patients with severe COVID-19. Clin. Exp. Rheumatol. 2020, 38, 529–532. [Google Scholar]
- Salvarani, C.; Dolci, G.; Massari, M.; Merlo, D.F.; Cavuto, S.; Savoldi, L.; Bruzzi, P.; Boni, F.; Braglia, L.; Turrà, C.; et al. Effect of Tocilizumab vs. Standard Care on Clinical Worsening in Patients Hospitalized With COVID-19 Pneumonia: A Randomized Clinical Trial. JAMA Intern. Med. 2021, 181, 24–31. [Google Scholar] [CrossRef]
- Babon, J.J.; Lucet, I.S.; Murphy, J.M.; Nicola, N.A.; Varghese, L.N. The molecular regulation of Janus kinase (JAK) activation. Biochem. J. 2014, 462, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Bousoik, E.; Montazeri Aliabadi, H. “Do We Know Jack” About JAK? A Closer Look at JAK/STAT Signaling Pathway. Front. Oncol. 2018, 8, 287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cantini, F.; Niccoli, L.; Matarrese, D.; Nicastri, E.; Stobbione, P.; Goletti, D. Baricitinib therapy in COVID-19: A pilot study on safety and clinical impact. J. Infect. 2020, 81, 318–356. [Google Scholar] [CrossRef]
- Kalil, A.C.; Patterson, T.F.; Mehta, A.K.; Tomashek, K.M.; Wolfe, C.R.; Ghazaryan, V.; Marconi, V.C.; Ruiz-Palacios, G.M.; Hsieh, L.; Kline, S.; et al. Baricitinib plus Remdesivir for Hospitalized Adults with COVID-19. N. Engl. J. Med. 2021, 384, 795–807. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Wei, J.; Zou, L.; Jiang, T.; Wang, G.; Chen, L.; Meng, F.; Huang, L.; Wang, N.; Zhou, X.; et al. Ruxolitinib in treatment of severe coronavirus disease 2019 (COVID-19): A multicenter, single-blind, randomized controlled trial. J. Allergy Clin. Immunol. 2020, 146, 137–146. [Google Scholar] [CrossRef]
- Roschewski, M.; Lionakis, M.S.; Sharman, J.P.; Roswarski, J.; Goy, A.; Monticelli, M.A.; Roshon, M.; Wrzesinski, S.H.; Desai, J.V.; Zarakas, M.A.; et al. Inhibition of Bruton tyrosine kinase in patients with severe COVID-19. Sci. Immunol. 2020, 5. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Cao, S.; Dong, H.; Li, Q.; Chen, E.; Zhang, W.; Yang, L.; Fu, S.; Wang, R. Effect of regular intravenous immunoglobulin therapy on prognosis of severe pneumonia in patients with COVID-19. J. Infect. 2020, 81, 318. [Google Scholar] [CrossRef]
- Zhou, Z.-G.; Xie, S.-M.; Zhang, J.; Zheng, F.; Jiang, D.-X.; Li, K.-Y.; Liu, L.-H.; Cai, C.-L.; Zhang, L. Short-term moderate-dose corticosteroid plus immunoglobulin effectively reverses COVID-19 patients who have failed low-dose therapy. 2020. Preprints. [Google Scholar]
- Shao, Z.; Feng, Y.; Zhong, L.; Xie, Q.; Lei, M.; Liu, Z.; Wang, C.; Ji, J.; Liu, H.; Gu, Z.; et al. Clinical efficacy of intravenous immunoglobulin therapy in critical ill patients with COVID-19: A multicenter retrospective cohort study. Clin. Transl. Immunol. 2020, 9. [Google Scholar] [CrossRef] [PubMed]
- Marano, G.; Vaglio, S.; Pupella, S.; Facco, G.; Catalano, L.; Liumbruno, G.M.; Grazzini, G. Convalescent plasma: New evidence for an old therapeutic tool? Blood Transfus. 2016, 14, 152–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rojas, M.; Rodriguez, Y.; Monsalve, D.M.; Acrosta-Ampudia, Y.; Camacho, B.; Gallo, J.E.; Tojas-Villarraga, A.; Ramirez-Santana, C.; Diaz-Coronado, J.C.; Maniriqu, R.; et al. Convalescent plasma in COVID-19: Possible mechanisms of action. Autoimmun. Rev. 2020, 19, 102554. [Google Scholar] [CrossRef]
- Pathak, E.B. Convalescent plasma is ineffective for COVID-19. BMJ 2020, 371. [Google Scholar] [CrossRef]
- Simonovich, V.A.; Burgos Pratx, L.D.; Scibona, P.; Beruto, M.V.; Vallone, M.G.; Vázquez, C.; Savoy, C.; Giunta, D.H.; Pérez, L.G.; Gamarnik, A.V.; et al. A Randomized Trial of Convalescent Plasma in COVID-19 Severe Pneumonia. N. Engl. J. Med. 2021, 384, 619–629. [Google Scholar] [CrossRef] [PubMed]
- Libster, R.; Pérez Marc, G.; Wappner, D.; Coviello, S.; Bianchi, A.; Braem, V.; Esteban, I.; Caballero, M.T.; Wood, C.; Berrueta, M.; et al. Early High-Titer Plasma Therapy to Prevent Severe COVID-19 in Older Adults. N. Engl. J. Med. 2021, 384, 610–618. [Google Scholar] [CrossRef] [PubMed]
- Salazar, E.; Christensen, P.A.; Graviss, E.A.; Nguyen, D.T.; Castillo, B.; Chen, J.; Lopez, B.V.; Eagar, T.N.; Yi, X.; Zhao, P.; et al. Treatment of Coronavirus Disease 2019 Patients with Convalescent Plasma Reveals a Signal of Significantly Decreased Mortality. Am. J. Pathol. 2020, 190, 2290–2303. [Google Scholar] [CrossRef] [PubMed]
- Khamis, F.; Al-Zakwani, I.; Al-Hashmi, S.; Al-Dowaiki, S.; Al-Bahrani, M.; Pandak, N.; Al-Khalili, H.M.Z. Therapeutic plasma exchange in adults with severe COVID-19 infection. Int. J. Infect. Dis. 2020, 99, 214–218. [Google Scholar] [CrossRef]
- Li, L.; Zhang, W.; Hu, Y.; Tong, X.; Zheng, S.; Yang, J.; Kong, Y.; Ren, L.; Wei, Q.; Mei, H.; et al. Effect of Convalescent Plasma Therapy on Time to Clinical Improvement in Patients with Severe and Life-threatening COVID-19: A Randomized Clinical Trial. JAMA J. Am. Med. Assoc. 2020, 324, 460–470. [Google Scholar] [CrossRef]
- Gharbharan, A.; Jordans, C.C.E.; Geurtsvankessel, K.G.; den Hollander, G.J.; Femke, K.F.P.N.; Mollema, F.P.N.; Stalenhoef-Schukken, M.J.E.; Dofferhoff, A.; Ludwig, I.; Koster, A.; et al. Convalescent plasma for COVID-19: A randomized clinical trial. medRxiv 2020. [CrossRef]
- Agarwal, A.; Mukherjee, A.; Kumar, G.; Chatterjee, P.; Bhatnagar, T.; Malhotra, P. Convalescent plasma in the management of moderate COVID-19 in India: An open-label parallel-arm phase II multicentre randomized controlled trial (PLACID Trial). BMJ 2020. [Google Scholar] [CrossRef] [PubMed]
- Joyner, M.J.; Senefeld, J.W.; Klassen, S.A.; Mills, J.R.; Johnson, P.W.; Theel, E.S.; Wiggins, C.C.; Bruno, K.A.; Klompas, A.M.; Lesser, E.R.; et al. Effect of Convalescent Plasma on Mortality among Hospitalized Patients with COVID-19: Initial Three-Month Experience. medRxiv 2020. [Google Scholar] [CrossRef]
- Liu, S.T.H.; Lin, H.M.; Baine, I.; Wajnberg, A.; Gumprecht, J.P.; Rahman, F.; Rodriguez, D.; Tandon, P.; Bassily-Marcus, A.; Bander, J.; et al. Convalescent plasma treatment of severe COVID-19: A propensity score–matched control study. Nat. Med. 2020, 26, 1708–1713. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Wang, Y.; Qi, C.; Shen, L.; Li, J. Clinical trial analysis of 2019-nCoV therapy registered in China. J. Med. Virol. 2020, 92, 540–545. [Google Scholar] [CrossRef] [PubMed]
- Alunno, A.; Najm, A.; Machado, P.M.; Bertheussen, H.; Burmester, G.R.; Carubbi, F.; Marco, G.D.; Giacomelli, R.; Hermine, O.; Isaacs, J.D.; et al. EULAR points to consider on pathophysiology and use of immunomodulatory therapies in COVID-19. Ann. Rheum. Dis. 2021, 80, 698–706. [Google Scholar] [CrossRef]
- Sarkar, K.; Sil, P.C.; Nabavi, S.F.; Berindan-Neagoe, I.; Cismaru, C.A.; Nabavi, S.M.; Habtemariam, S. Possible Targets and Therapies of SARS-CoV-2 Infection. Mini Rev. Med. Chem. 2020, 20, 1900–1907. [Google Scholar] [CrossRef]
- Wu, C.; Liu, Y.; Yang, Y.; Zhang, P.; Zhong, W.; Wang, Y.; Wang, Q.; Xu, Y.; Li, M.; Li, X.; et al. Analysis of therapeutic targets for SARS-CoV-2 and discovery of potential drugs by computational methods. Acta Pharm. Sin. B 2020, 10, 766–788. [Google Scholar] [CrossRef]
- Gordon, D.E.; Jang, G.M.; Bouhaddou, M.; Xu, J.; Obernier, K.; White, K.M.; O’Meara, M.J.; Rezelj, V.V.; Guo, J.Z.; Swaney, D.L.; et al. A SARS-CoV-2 protein interaction map reveals targets for drug repurposing. Nature 2020, 583, 459–468. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| N | Authors and Year of Publication | The Agent Studied | Mode of Drug Administration | Number of Patients/Control Group | Observation Time, Days (Median) | Comparison of Efficiency with Control Group (%) | Conclusions |
|---|---|---|---|---|---|---|---|
| 1 | Cao B. et al., 2020 [24] | lopinavir/ritonavir | 400/100 mg twice a day 14 days | 99/control (n = 100) | 28 | Mortality 19.2 vs. 25.0 | No difference |
| 2 | Li Y et al., 2020 [25] | lopinavir/ritonavir umifenovir and hydrochloride monohidrate | 200/50 mg 2 times/day 7–14 days and 200 mg 3 t/day 7–14 days | 34 versus 35 and control (n = 17) | 21 | Efficacy: 85.3 vs. 91.4 vs 76.5 | |
| 3 | Gautret Ph. et al., 2020 [26] | Hydroxychlo-roquine sulfate | 600 mg/day 10 days | 20/control (n = 16) | 14 | Efficacy: 57.1 vs. 12.5 | |
| 4 | Gautret P, et al., 2020 [27] | hydroxychloroquine sulfate + azithromycin | 600 mg/day 10 days + 500 mg on 1-st day, further 250 mg 2nd–5th day | 80/no | ≥6 | Efficacy: 93.0 | |
| 5 | Geleris J. et al., 2020 [28] | hydroxychloroquine sulfate | 600 mg on 1-st day, further 400 mg/day | 811/control (n = 565) | 22.5 | Efficacy: 45.8 (no data) | |
| 6 | Grein J. et al., 2020 [29] | remdesivir | 200 mg on 1-st day, further 100 mg 2nd–10th day | 53/no | 19 | Efficacy: 47.0 (no data) | |
| 7 | WangY. et al., 2020 [30] | 200 mg on 1-st day, further 100 mg 2nd–10th day | 158/Placebo control (n = 79) | 28 | Efficacy: 65.0 vs. 58.0 | ||
| 8 | Beige JH. et al., 2020 [31] | 200 mg/day for 10 days | 538/placebo control 521 | 15 | Efficacy: 62.9 vs. 52.7 | ||
| 9 | Goldman JD.et al, 2020 [32] | 200 mg/day for 5 and 10 days | 200 (5 days)/197 (10 days) | 14 | Efficacy: 64.0 vs. 54.0 Mortality 8.0 vs 11.0 | ||
| 10 | Boulware D.R. et al., 2020 [33] | hydroxychloroquine sulfate (prophylactically) | 800 мг in a single dose, further 600 mg after 6 and 8 h, further 600 mg for 4 days | 414 patients with asympto-matic course/407 (placebo) | 14 | Got sick 11.8 vs. 14.3 | |
| 11 | Freedberg ED et al., 2020 [34] | famotidine | 20 mg, 40 mg, 10 mg | 84/control 1536 | 5 | Mortality 10.0 vs. 22.0 | |
| 12 | Horby P. at al, 2020 [35] | hydroxychloroquine sulfate | 800 мг in a single dose, further 400 mg after 12 h and 6 days | 1561/3155 (control) | n | Mortality 27.0 vs. 25.0 | |
| 13 | Mather J et al., 2020 [36] | famotidine + hydroxychloroquine sulfate (n = 36) famotidine + azithromycin (n = 36) famotidine + corticosteroids (n = 48) | 20 mg, 40 mg 7 days | 83/689 (control group) | 36 | Mortality 21.6 vs. 39.7 |
| № | Authors, Year | The Type of the Study | The Drug | The Treatment Characteristics of Patients | Conclusions | |
|---|---|---|---|---|---|---|
| Studied Group | Comparison Group | |||||
| 1 | Cavalli G et al. [39] | Retrospective cohort study | Anakinra (block IL-1 beta R) | Patients (aged ≥18 years) with COVID-19, moderate-to-severe ARDS, and hyperinflammation (n = 29) Standard treatment + Anankinra dose 5 mg/kg twice a day 100 mg subcutaneously 21 days | COVID-19, ARDS, and hyperinflammation Standard treatment | Decreased mortality |
| 2 | Pontali E. et al. [40] | Uncontrolled cohort study | 5 patients with severe/moderate COVID-19 100 mg IV every 8 h n = 5 | - | Faster de-escalation of the intensity of care | |
| 3 | Ucciferri C et al. [41] | Retrospective cohort study | Canakinumab (block IL-1β) | 300 mg subcutaneously n = 10 | - | Faster de-escalation of the intensity of care |
| 4 | Xu X et al. [42] | Retrospective cohort study | Tocilizumab (block IL-6) | Severe or critical COVID-19 n = 21 4–8 mg/kg, recommended dose–400–800 mg singly 21 days | - | Faster de-escalation of the intensity of care |
| 5 | Malekzadeha R et al. [43] | Multicenter, prospective, open-label, uncontrolled | Adult patients with severe and critical COVID-19 n = 126 324 mg (<100 kg bodyweight) or 486 mg (≥100 kg bodyweight). 40 days | - | Faster de-escalation of the intensity of care | |
| 6 | Stone JH et al. [44] | A randomized, double-blind, placebo-controlled trial | Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection, hyperinflammatory states n = 161 4–8 mg/kg, recommended dose–400–800 mg singly 14 and 28 days | Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection, hyperinflammatory states n = 81 Standard treatment | No difference | |
| 7 | Alattar R et al. [45] | Retrospective cohort study | severe COVID-19 n = 25 4–8 mg/kg, recommended dose–400–800 mg singly 14 and 28 days | n | No difference | |
| 8 | Tsai A et al. [46] | A single-center propensity-score matched cohort study | Severe COVID-19 n = 66 8 mg/kg, recommended dose–400–800 mg singly | Severe COVID-19 n = 66 Standard treatment | No difference | |
| 9 | Klopfenstein T et al. [47] | a retrospective case-control study | Severe COVID-19 n = 20 tocilizumab (1 or 2 doses) | Severe COVID-19 n = 25 Standard treatment | Decreased mortality | |
| 10 | Toniati P et al. [48] | severe COVID-19 n = 100 8 mg/kg by two consecutive intravenous infusions 12 h apart | - | Faster de-escalation of the intensity of care | ||
| 11 | Guaraldi G et al. [49] | Retrospective, observational cohort study | n = 179 intravenously at 8 mg/kg bodyweight (up to a maximum of 800 mg) in two infusions, 12 h apart, or subcutaneously at 162 mg administered in two simultaneous doses, one in each thigh (ie, 324 mg in total) | Adults (≥18 years) with severe COVID-19 n = 365 Standard treatment | Decreased mortality | |
| 12 | Potere N. et al. [50] | Retrospective case–control study | severe COVID-19 n = 40 324 mg, given as two concomitant subcutaneous injections | Severe COVID-19 n = 40 Standard treatment (SOC) | Faster de-escalation of the intensity of care | |
| 13 | Rojas-Marte G. et al. [51] | a Retrospective, case–control, Single-center study | severe to critical COVID-19 n = 96 4–8 mg/kg, recommended dose–400–800 mg singly 15 and 17 days | severe to critical COVID-19 n = 97 Standard treatment | Decreased mortality | |
| 14 | Colaneri M et al. [52] | Prospective study | 8 mg/kg, recommended dose–400–800 mg singly 7 days n = 21 | n = 91 Standard treatment | No difference | |
| 15 | Tarrytown NY. et al. [53] | Randomized Phase 2 | Sarilumab (block IL-6 R) | Critical, severe COVID-19 n = 281 136 (200 mg)/145 (400 mg) | Critical, severe COVID-19 n = 77 placebo | No difference |
| № | Authors, Year | The Type of the Study | The Drug | The Treatment Characteristics of Patients | Conclusions | |
|---|---|---|---|---|---|---|
| Studied Group | Comparison Group | |||||
| 1 | Cantini F et al. [58] | Pilot study with open-label design, with no randomization and a low number of treated patients’ | Baricytinib (block JAK-k) | Moderate COVID-19 4 mg/day 14 days n = 24 | Moderate COVID-19 n = 24 | Faster de-escalation of the intensity of care |
| 2 | Kalil AC et al. [59] | Multicenter. A randomized, double-blind ACTT-2 trial | Moderate to severe COVID-19 4 mg daily (for up to 14 days or until hospital discharge), n = 515 | Moderate to severe COVID-19 n = 518 placebo | Dereased mortality | |
| 3 | Cao Y et al. [60] | Small, single-blind, randomized, controlled Phase 2 trial | Ruxolitinib (block JAK-k) | Severe COVID-19 n = 20 5 mg orally twice daily | Severe COVID-19 n = 21 Placebo (vitamin C 100 mg) | No statistical difference was observed. |
| 4 | Roschewski M et al. [61] | Retrospective case series | Acalabrutinib (Bruton’s Tyrosine Kinase Inhibitors) | Severe COVID-19 n = 19 | - | Faster de-escalation of the intensity of care |
| № | Authors, Year | The Type of the Study | Treatment Patient Characteristics | Conclusions | |
|---|---|---|---|---|---|
| Studied Group | Comparison Group | ||||
| 1 | Shao Z et al. [64] | Multicenter retrospective cohort study | Critical COVID-19 n = 174 human Immunoglobulin (pH4) for intravenous injection 28 and 60 days | Critical COVID-19 n = 151 | No difference |
| 2 | Zhou Z-G et al. [63] | n = 10 Short-term moderate-dose corticosteroid (160 mg/d) plus immunoglobulin (20 g/d) | - | Faster de-escalation of the intensity of care | |
| 3 | Xie Y et al. [62] | Retrospective study | Severe or critical illness due to COVID-19 n = 58 | - | Faster de-escalation of the intensity of care |
| № | Authors, Year | The Type of Research | Treatment Patients Characteristic, n | Conclusions | |
|---|---|---|---|---|---|
| Studied Group | Comparison Group | ||||
| 1 | Simonovich VA et al. [68] | Double-blind, placebo-controlled, multicenter tria | Severe COVID-19 n = 228 Early administration of convalescent plasma (median titer of 1:3200 of total SARS-CoV-2 antibodies) | Severe COVID-19 n = 105 placebo | No difference |
| 2 | Libster R et al. [69] | A randomized, double-blind, placebo-controlled trial | Mildly ill infected older adults n = 80 Early administration of high-titer convalescent plasma 250 mL (IgG titer greater than 1:1000 against SARS-CoV-2 spike) | Mildly ill infected older adults n = 80 placebo | No statistical difference reduced the progression of COVID-19 |
| 3 | Salazar E et al. [70] | Prospective, ongoing study | Severe and/or life-threatening COVID-19 n = 136 600 mL plasma was collected from each donor 7 and 14 days | Severe and/or life-threatening COVID-19 n = 251 | Decreaesd mortality |
| 4 | Khamis F et al. [71] | Single-center, case series study | n = 11 Early therapeutic plasma exchange (TPE), 14, 28 days | Critical COVID-19 n = 20 | Decreased mortality |
| 5 | Li L et al. [72] | Open-label, multicenter, randomized clinical trial | Severe or life-threatening COVID-19 n = 52 specific IgG titer ≥ 1:640; 200 mL of plasma 28 days | Severe or life-threatening COVID-19 n = 51 | No difference |
| 6 | Gharbharan A et al. [73] | A randomized trial | n = 43 ≥1:80; 300 mL 15 days | n = 43 | No statistical difference Mortality 14.0 vs. 26.0 |
| 7 | Agarwal A at al [74] | Open label, parallel arm, phase II, multicentre, randomised controlled trial. | Moderate COIVD-19 n = 235 2 doses of 200 mL CP | n = 229 | No statistical difference Mortality: 14.5 vs. 13.5 |
| 8 | Joyner MJ et al. [75] | Open-label, Expanded Access Program (EAP) for the treatment of COVID-19 patients with human convalescent plasma. | Severe critical COVID-19 n = 35 150–200 mL 30 days | n = 322 | Decreased mortality |
| 9 | Liu STH et al. [76] | Retrospective, propensity score-matched case-control study | Severe or life-threatening COVID-19 2 units of CP; 1:320 14 days n = 39 | Severe or life-threatening COVID-19 n = 156 | No diference |
| The Group of Therapeutic Target | The Target | The Inhibiting Molecule |
|---|---|---|
| Blocking replication | Papain-like proteinase (PLpro) | anti-virus drugs (ribavirin, valganciclovir, thymidine) anti-bacterial drugs (chloramphenicol, cefamandole, tigecycline) muscle relaxant drug (chlorphenesin carbamate) anti-tussive drug (levodropropizine) |
| 3C-like main protease (3CLpro/Nsp5) | anti-bacterial drugs (lymecycline, demeclocycline, doxycycline, oxytetracycline) anti-hypertensive drugs (nicardipine, telmisartan, conivaptan) | |
| RNA-dependent RNA polymerase (RdRp) | antifungal drug itraconazole anti-bacterial drug novobiocin gallstone dissolving drug chenodeoxycholic acid anti-allergic drug cortisone anti-tumor drug idarubicin hepatoprotective drug silybin muscle relaxant drug pancuronium bromide anticoagulant drug dabigatran | |
| Helicase | anti-bacterial drug (lymecycline, cefsulodine, rolitetracycline) anti-fungal drug itraconazole anti-HIV1 drug saquinavir anti-coagulant drug dabigatran diuretic drug canrenoic acid | |
| Restoring host’s innate immunity | Nsp1, Nsp3c, ORF7a | anti-bacterial drugs (piperacillin, cefpiramide, streptomycin, lymecycline, tetracycline) |
| Blocking viral structural proteins | Spike protein | antihypertensive drugs (rescinnamine, iloprost, prazosin) antifungal drugs (posaconazole, itraconazole) anti-bacterial drug (sulfasalazine, azlocillin, penicillin, cefsulodin) anti-coagulant drug dabigatran etexilate |
| Interface between Spike and ACE2 | Hesperidin | |
| Blocking host‘s proteins | ACE2 protein | antidiabetes drug troglitazone anti-hypertensive drug losartan analgesia drug ergotamine anti-bacterial drug cefmenoxime hepatoprotective drug silybin phyllaemblicin |
| TMPRSS2 | anti-bacterial drugs (pivampicillin, hetacillin, cefoperazone, clindamycin) | |
| Ligands of the sigma-1,2 receptors | Haloperidol, PB28, PD-144418 and hydroxychloroquine | |
| Eukaryotic Translation Initiation Factor 4H (eIF4H) | Zotatifin | |
| Elongation factor-1A (eEF1A) | Ternatin-4 | |
| Sec61 translocon | PS3061 |
| The Plant | Scutellaria Baicalensis | Cassine Xylocarpa | Swertia Genus | Citrus Aurantium | Phyllanthus Emblica |
|---|---|---|---|---|---|
| Molecules inhibiting Sars-Cov-2 | Baicalin Chrysin-7-o-b-glucuronide Wogonoside Cosmosiin | Betulonal Etexilate betulonal | Deacetylcentapicrin Triptexanthoside D 1,7-dihydroxy-3- methoxyxanthone Kouitchenside I, D | Neohesperidin Hesperidin | Phyllaemblinol Phyllaemblicin B, G7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Starshinova, A.; Malkova, A.; Zinchenko, U.; Kudlay, D.; Glushkova, A.; Dovgalyk, I.; Yablonskiy, P.; Shoenfeld, Y. Efficacy of Different Types of Therapy for COVID-19: A Comprehensive Review. Life 2021, 11, 753. https://doi.org/10.3390/life11080753
Starshinova A, Malkova A, Zinchenko U, Kudlay D, Glushkova A, Dovgalyk I, Yablonskiy P, Shoenfeld Y. Efficacy of Different Types of Therapy for COVID-19: A Comprehensive Review. Life. 2021; 11(8):753. https://doi.org/10.3390/life11080753
Chicago/Turabian StyleStarshinova, Anna, Anna Malkova, Ulia Zinchenko, Dmitry Kudlay, Anzhela Glushkova, Irina Dovgalyk, Piotr Yablonskiy, and Yehuda Shoenfeld. 2021. "Efficacy of Different Types of Therapy for COVID-19: A Comprehensive Review" Life 11, no. 8: 753. https://doi.org/10.3390/life11080753
APA StyleStarshinova, A., Malkova, A., Zinchenko, U., Kudlay, D., Glushkova, A., Dovgalyk, I., Yablonskiy, P., & Shoenfeld, Y. (2021). Efficacy of Different Types of Therapy for COVID-19: A Comprehensive Review. Life, 11(8), 753. https://doi.org/10.3390/life11080753