
Links between Endothelial Glycocalyx Changes and Microcirculatory Parameters in Septic Patients


Abstract
:1. Introduction
2. Materials and Methods
2.1. Evaluation of the Microcirculation
2.2. Evaluation of the Glycocalyx
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Jedlicka, J.; Becker, B.F.; Chappell, D. Endothelial Glycocalyx. Crit. Care Clin. 2020, 36, 217–232. [Google Scholar] [CrossRef]
- Alphonsus, C.S.; Rodseth, R.N. The Endothelial Glycocalyx: A Review of the Vascular Barrier. Anaesthesia 2014, 69, 777–784. [Google Scholar] [CrossRef] [PubMed]
- Butler, M.J.; Down, C.J.; Foster, R.R.; Satchell, S.C. The Pathological Relevance of Increased Endothelial Glycocalyx Permeability. Am. J. Pathol. 2020, 190, 742–751. [Google Scholar] [CrossRef]
- Iba, T.; Levy, J.H. Derangement of the Endothelial Glycocalyx in Sepsis. J. Thromb. Haemost. 2019, 17, 283–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pranskūnas, A.; Pilvinis, V.; Dambrauskas, Ž; Rasimavičiūtė, R.; Milieškaitė, E.; Bubulis, A.; Veikutis, V.; Vaitkaitis, D.; Boerma, E.C. Microvascular Distribution in the Ocular Conjunctiva and Digestive Tract in an Experimental Setting. Medicina 2012, 48, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Rovas, A.; Seidel, L.M.; Vink, H.; Pohlkötter, T.; Pavenstädt, H.; Ertmer, C.; Hessler, M.; Kümpers, P. Association of Sublingual Microcirculation Parameters and Endothelial Glycocalyx Dimensions in Resuscitated Sepsis. Crit. Care 2019, 23, 260–262. [Google Scholar] [CrossRef] [Green Version]
- Rovas, A.; Sackarnd, J.; Rossaint, J.; Kampmeier, S.; Pavenstädt, H.; Vink, H.; Kümpers, P. Identification of Novel Sublingual Parameters to Analyze and Diagnose Microvascular Dysfunction in Sepsis: The NOSTRADAMUS Study. Crit. Care 2021, 25, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Beurskens, D.M.; Bol, M.E.; Delhaas, T.; van de Poll, M.C.; Reutelingsperger, C.P.; Nicolaes, G.A.; Sels, J.E. Decreased Endothelial Glycocalyx Thickness is an Early Predictor of Mortality in Sepsis. Anaesth. Intensive Care 2020, 48, 221–228. [Google Scholar] [CrossRef]
- Dilken, O.; Ergin, B.; Ince, C. Assessment of Sublingual Microcirculation in Critically Ill Patients: Consensus and Debate. Ann. Transl. Med. 2020, 8, 793. [Google Scholar] [CrossRef]
- De Backer, D.; Donadello, K.; Sakr, Y.; Ospina-Tascon, G.; Salgado, D.; Scolletta, S.; Vincent, J.L. Microcirculatory Alterations in Patients with Severe Sepsis: Impact of Time of Assessment and Relationship with Outcome. Crit. Care Med. 2013, 41, 791–799. [Google Scholar] [CrossRef] [Green Version]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Gruartmoner, G.; Mesquida, J.; Ince, C. Microcirculatory Monitoring in Septic Patients: Where do we Stand? Med. Intensiva 2017, 41, 44–52. [Google Scholar] [CrossRef]
- Goedhart, P.T.; Khalilzada, M.; Bezemer, R.; Merza, J.; Ince, C. Sidestream Dark Field (SDF) Imaging: A Novel Stroboscopic LED Ring-Based Imaging Modality for Clinical Assessment of the Microcirculation. Opt. Express 2007, 15, 15101–15114. [Google Scholar] [CrossRef] [PubMed]
- Aykut, G.; Veenstra, G.; Scorcella, C.; Ince, C.; Boerma, C. Cytocam-IDF (Incident Dark Field Illumination) Imaging for Bedside Monitoring of the Microcirculation. Intensive Care. Med. Exp. 2015, 3, 40–47. [Google Scholar] [CrossRef] [Green Version]
- Ince, C.; Boerma, E.C.; Cecconi, M.; De Backer, D.; Shapiro, N.I.; Duranteau, J.; Pinsky, M.R.; Artigas, A.; Teboul, J.L.; Reiss, I.K.M.; et al. Second Consensus on the Assessment of Sublingual Microcirculation in Critically Ill Patients: Results from a Task Force of the European Society of Intensive Care Medicine. Intensive Care Med. 2018, 44, 281–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boerma, E.C.; Mathura, K.R.; van der Voort, P.H.; Spronk, P.E.; Ince, C. Quantifying Bedside-Derived Imaging of Microcirculatory Abnormalities in Septic Patients: A Prospective Validation Study. Crit. Care 2005, 9, 601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pranskunas, A.; Arstikyte, J.; Pranskuniene, Z.; Bernatoniene, J.; Kiudulaite, I.; Vaitkaitiene, E.; Vaitkaitis, D.; Brazaitis, M. Time Evolution of Sublingual Microcirculatory Changes in Recreational Marathon Runners. Biomed. Res. Int. 2017, 2017, 7120785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Backer, D.; Hollenberg, S.; Boerma, C.; Goedhart, P.; Buchele, G.; Ospina-Tascon, G.; Dobbe, I.; Ince, C. How to Evaluate the Microcirculation: Report of a Round Table Conference. Crit. Care 2007, 11, R101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, D.H.; Dane, M.J.; van den Berg, B.M.; Boels, M.G.; van Teeffelen, J.W.; de Mutsert, R.; den Heijer, M.; Rosendaal, F.R.; van der Vlag, J.; van Zonneveld, A.J.; et al. Deeper Penetration of Erythrocytes into the Endothelial Glycocalyx is Associated with Impaired Microvascular Perfusion. PLoS ONE 2014, 9, e96477. [Google Scholar] [CrossRef] [Green Version]
- Vink, H.; Duling, B.R. Identification of Distinct Luminal Domains for Macromolecules, Erythrocytes, and Leukocytes within Mammalian Capillaries. Circ. Res. 1996, 79, 581–589. [Google Scholar] [CrossRef]
- Martens, R.J.; Vink, H.; van Oostenbrugge, R.J.; Staals, J. Sublingual Microvascular Glycocalyx Dimensions in Lacunar Stroke Patients. Cerebrovasc. Dis. 2013, 35, 451–454. [Google Scholar] [CrossRef]
- Rovas, A.; Lukasz, A.H.; Vink, H.; Urban, M.; Sackarnd, J.; Pavenstädt, H.; Kümpers, P. Bedside Analysis of the Sublingual Microvascular Glycocalyx in the Emergency Room and Intensive Care Unit-The Glyco Nurse Study. Scand. J. Trauma. Resusc. Emerg. Med. 2018, 26, 16. [Google Scholar] [CrossRef] [Green Version]
- Cabrales, P.; Vázquez, B.Y.; Tsai, A.G.; Intaglietta, M. Microvascular and Capillary Perfusion Following Glycocalyx Degradation. J. Appl. Physiol. 2007, 102, 2251–2259. [Google Scholar] [CrossRef] [Green Version]
- Marechal, X.; Favory, R.; Joulin, O.; Montaigne, D.; Hassoun, S.; Decoster, B.; Zerimech, F.; Neviere, R. Endothelial Glycocalyx Damage during Endotoxemia Coincides with Microcirculatory Dysfunction and Vascular Oxidative Stress. Shock 2008, 29, 572–576. [Google Scholar] [CrossRef]
- Nieuwdorp, M.; Meuwese, M.C.; Mooij, H.L.; van Lieshout, M.H.; Hayden, A.; Levi, M.; Meijers, J.C.; Ince, C.; Kastelein, J.J.; Vink, H.; et al. Tumor Necrosis Factor-Alpha Inhibition Protects Against Endotoxin-Induced Endothelial Glycocalyx Perturbation. Atherosclerosis 2009, 202, 296–303. [Google Scholar] [CrossRef]
- Koning, N.J.; Vonk, A.B.; Vink, H.; Boer, C. Side-by-Side Alterations in Glycocalyx Thickness and Perfused Microvascular Density during Acute Microcirculatory Alterations in Cardiac Surgery. Microcirculation 2016, 23, 69–74. [Google Scholar] [CrossRef]
- Pranskunas, A.; Tamosuitis, T.; Balciuniene, N.; Damanskyte, D.; Sneider, E.; Vitkauskiene, A.; Sirvinskas, E.; Pilvinis, V.; Boerma, E.C. Alterations of Conjunctival Glycocalyx and Microcirculation in Non-Septic Critically Ill Patients. Microvasc. Res. 2018, 118, 44–48. [Google Scholar] [CrossRef]
- Wu, Q.; Gao, W.; Zhou, J.; He, G.; Ye, J.; Fang, F.; Luo, J.; Wang, M.; Xu, H.; Wang, W. Correlation Between Acute Degradation of the Endothelial Glycocalyx and Microcirculation Dysfunction during Cardiopulmonary Bypass in Cardiac Surgery. Microvasc. Res. 2019, 124, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Donati, A.; Damiani, E.; Luchetti, M.; Domizi, R.; Scorcella, C.; Carsetti, A.; Gabbanelli, V.; Carletti, P.; Bencivenga, R.; Vink, H.; et al. Microcirculatory Effects of the Transfusion of Leukodepleted Or Non-Leukodepleted Red Blood Cells in Patients with Sepsis: A Pilot Study. Crit. Care 2014, 18, R33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vincent, J. Annual Update in Intensive Care and Emergency Medicine 2020; Springer: Berlin/Heidelberg, Germany, 2020; pp. 213–220. [Google Scholar]
- Giantsos-Adams, K.M.; Koo, A.J.; Song, S.; Sakai, J.; Sankaran, J.; Shin, J.H.; Garcia-Cardena, G.; Dewey, C.F., Jr. Heparan Sulfate Regrowth Profiles Under Laminar Shear Flow Following Enzymatic Degradation. Cell. Mol. Bioeng. 2013, 6, 160–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamzaoui, O.; Shi, R. Microcirculation and Mean Arterial Pressure: Friends Or Foes? Ann. Transl. Med. 2020, 8, 803. [Google Scholar] [CrossRef] [PubMed]
- Margraf, A.; Herter, J.M.; Kühne, K.; Stadtmann, A.; Ermert, T.; Wenk, M.; Meersch, M.; Van Aken, H.; Zarbock, A.; Rossaint, J. 6% Hydroxyethyl Starch (HES 130/0.4) Diminishes Glycocalyx Degradation and Decreases Vascular Permeability During Systemic and Pulmonary Inflammation in Mice. Crit. Care 2018, 22, 111–113. [Google Scholar] [CrossRef] [Green Version]
- Jacob, M.; Chappell, D.; Becker, B.F. Regulation of Blood Flow and Volume Exchange Across the Microcirculation. Crit. Care 2016, 20, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Becker, B.F.; Jacob, M.; Leipert, S.; Salmon, A.H.; Chappell, D. Degradation of the Endothelial Glycocalyx in Clinical Settings: Searching for the Sheddases. Br. J. Clin. Pharmacol. 2015, 80, 389–402. [Google Scholar] [CrossRef]
- Ince, C. Hemodynamic Coherence and the Rationale for Monitoring the Microcirculation. Crit. Care 2015, 19, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cosgun, Z.C.; Fels, B.; Kusche-Vihrog, K. Nanomechanics of the Endothelial Glycocalyx: From Structure to Function. Am. J. Pathol. 2020, 190, 732–741. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Variable | Septic Patients |
|---|---|
| Number of participants | 28 |
| Female sex; n (%) | 9 (32) |
| Age (years) | 65 (58–80) |
| Body mass index (BMI; kg/m2) | 25.0 (21.0–27.8) |
| Time to inclusion (hours) | 14 (6–24) |
| SOFA score | 9 (8–11) |
| Mechanical ventilation (n (%)) | 28 (100) |
| Vasopressors (n (%)) | 28 (100) |
| Norepinephrine | |
| Dose (μg/kg/min) | 0.23 (0.12–0.37) |
| Septic shock (n (%)) | 14 (50) |
| In-hospital mortality (n (%)) | 12 (42.9) |
| APACHE II score | 17.50 (14.25–22.00) |
| Mean arterial pressure (MAP; mmHg) | 75 (63–83) |
| Heart rate (beats/min) | 106 (95–115) |
| Cardiac index (CI; L/min/m2) | 3.2 (2.0–4.4) |
| Laboratory data | |
| C-reactive protein (CRP; mg/L) | 252 (133–415) |
| Interleukin (IL)-6 (pg/mL) | 875 (450–2087) |
| pH | 7.301 (7.261–7.398) |
| Partial pressure of oxygen (pO2, mmHg) | 110 (80–144) |
| Serum lactate (mmol/L) | 2.3 (1.4–3.8) |
| Central venous oxygen saturation (ScvO2,%) | 76.5 (70.8–78.8) |
| Microcirculation data | |
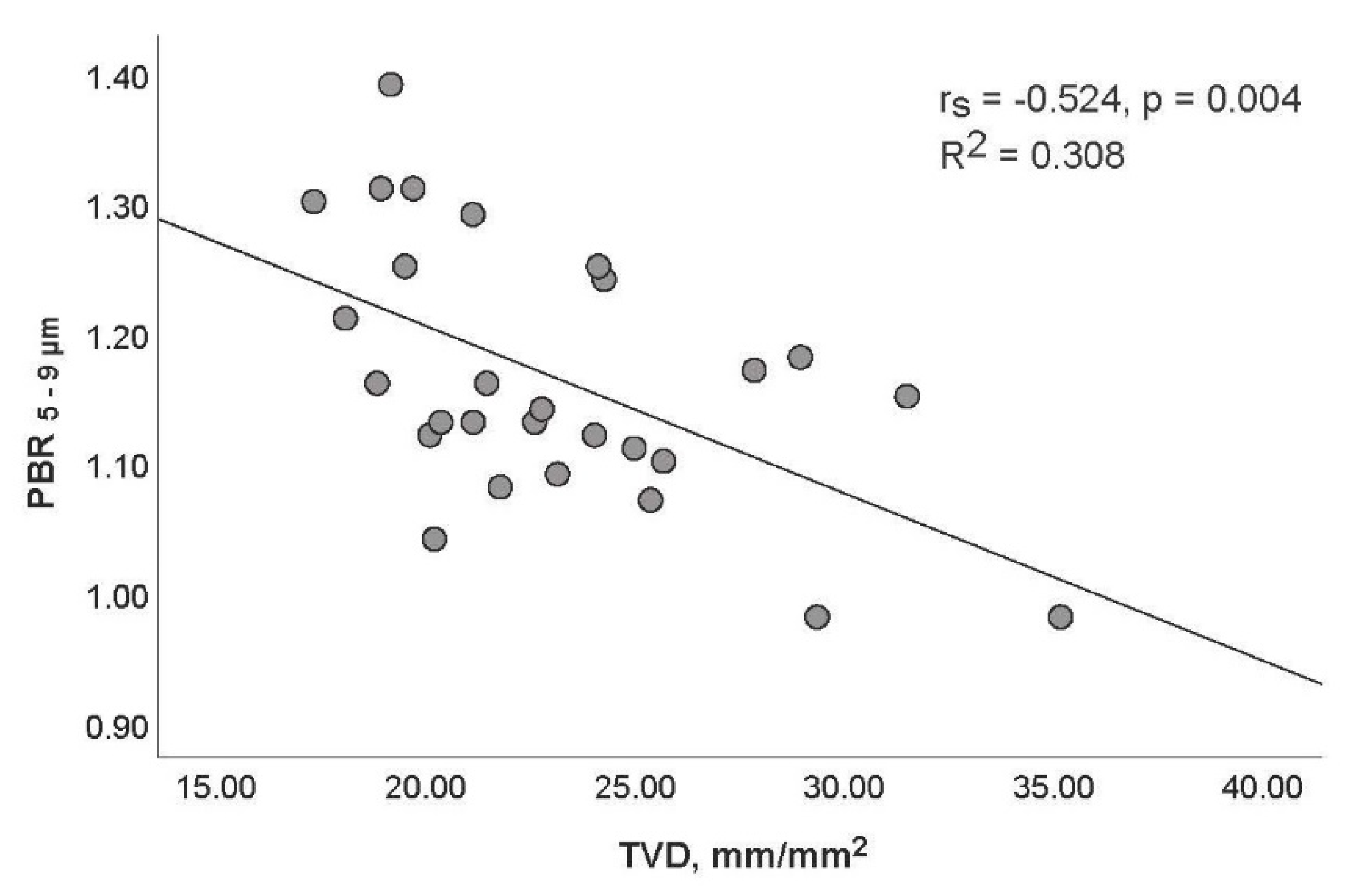
| Total vessel density (TVD, mm/mm2) | 22.2 (19.8–25.3) |
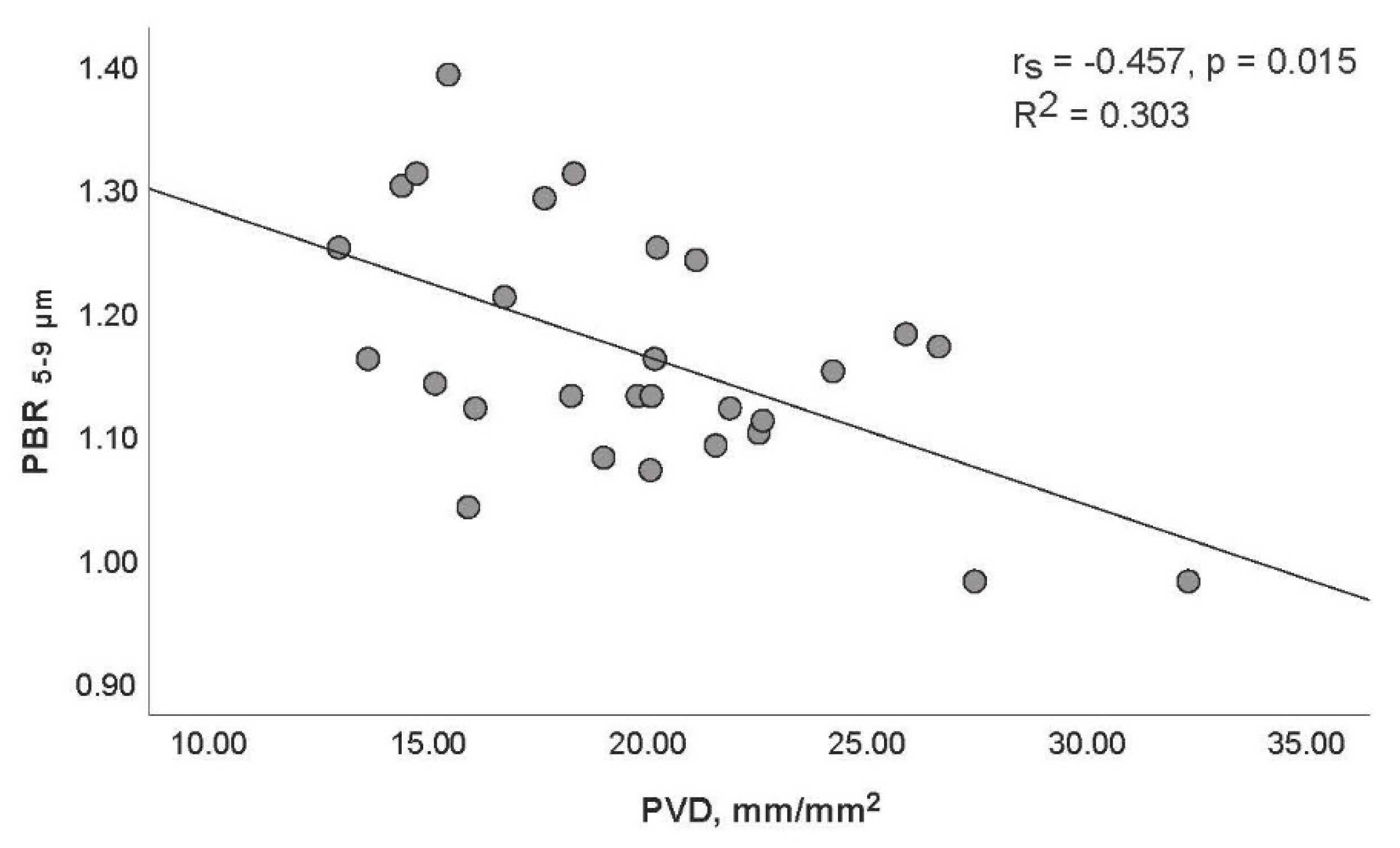
| Perfused vessel density (PVD, mm/mm2) | 19.9 (15.9–22.3) |
| Proportion of perfused vessels (PPV, %) | 87.8 (79,0–91.7) |
| Microvascular flow index (MFI) | 1.96 (1.52–2.17) |
| De Backer score | 14.2 (12.2–16.5) |
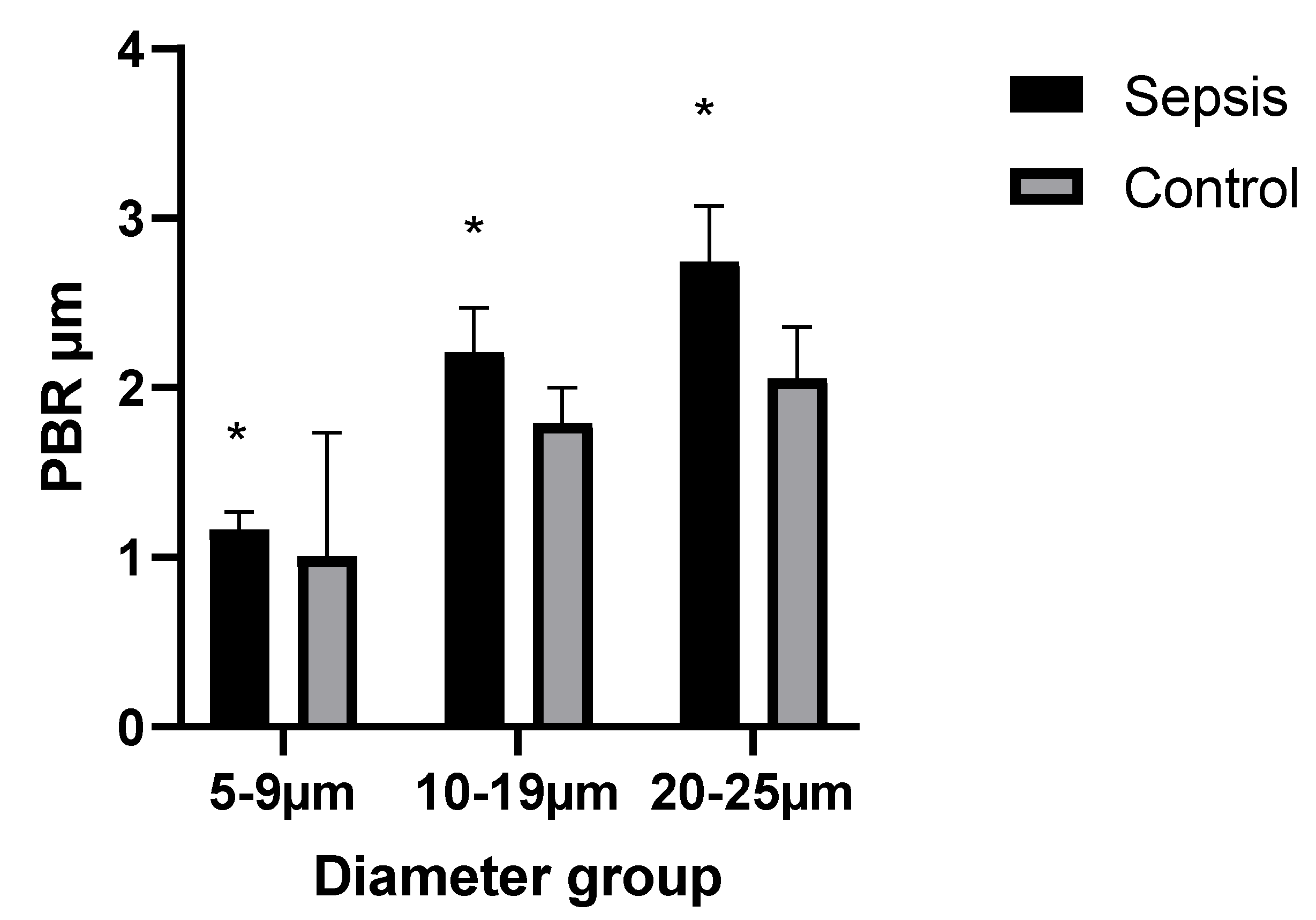
| Endothelial Glycocalyx (EG) | Healthy Subjects | Septic Patients | p-Value |
|---|---|---|---|
| PBR; 5–25 (μm) | 1.70 (1.53–1.84) | 2.10 (2.00–2.30) | <0.001 |
| PBR; 5–9 (μm) | 1.00 (0.97–1.06) | 1.14 (1.10–1.25) | <0.001 |
| PBR; 10–19 (μm) | 1.79 (1.70–2.00) | 2.24 (2.06–2.40) | <0.001 |
| PBR; 20–25 (μm) | 2.06 (1.76–2.29) | 2.75 (2.52–2.94) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Belousoviene, E.; Kiudulaite, I.; Pilvinis, V.; Pranskunas, A. Links between Endothelial Glycocalyx Changes and Microcirculatory Parameters in Septic Patients. Life 2021, 11, 790. https://doi.org/10.3390/life11080790
Belousoviene E, Kiudulaite I, Pilvinis V, Pranskunas A. Links between Endothelial Glycocalyx Changes and Microcirculatory Parameters in Septic Patients. Life. 2021; 11(8):790. https://doi.org/10.3390/life11080790
Chicago/Turabian StyleBelousoviene, Egle, Inga Kiudulaite, Vidas Pilvinis, and Andrius Pranskunas. 2021. "Links between Endothelial Glycocalyx Changes and Microcirculatory Parameters in Septic Patients" Life 11, no. 8: 790. https://doi.org/10.3390/life11080790