
Can The ‘Speed Bump Sign’ Be a Diagnostic Tool for Acute Appendicitis? Evidence-Based Appraisal by Meta-Analysis and GRADE


Abstract
:1. Introduction
2. Materials and Methods
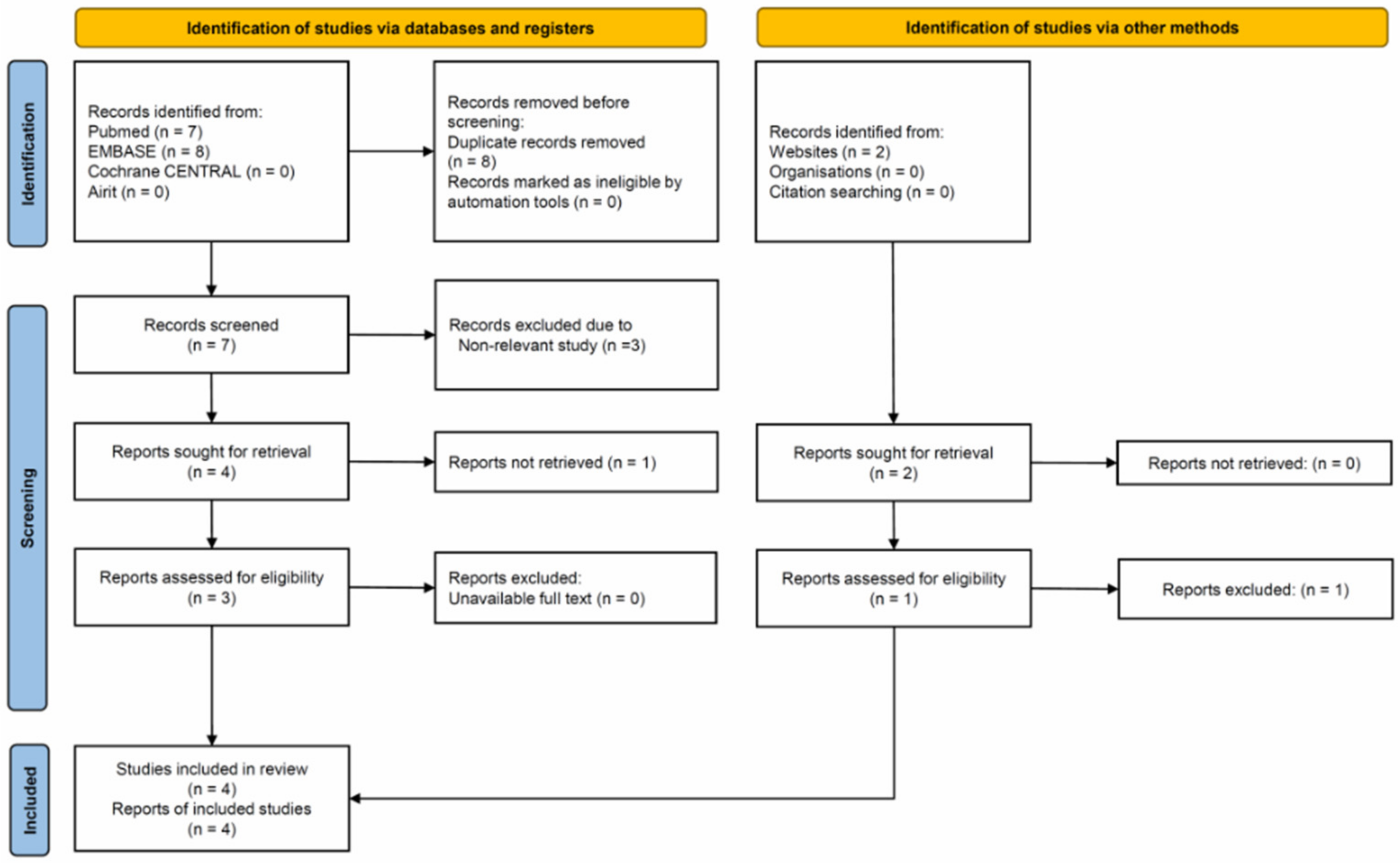
2.1. Search Strategy and Study Eligibility
2.2. Methodologic Quality Assessment
2.3. Data Extraction and Statistical Analysis
2.4. Grading of the Certainty of Evidence
3. Results
3.1. Characteristics of the Enrolled Studies
3.2. Quality of the Enrolled Studies
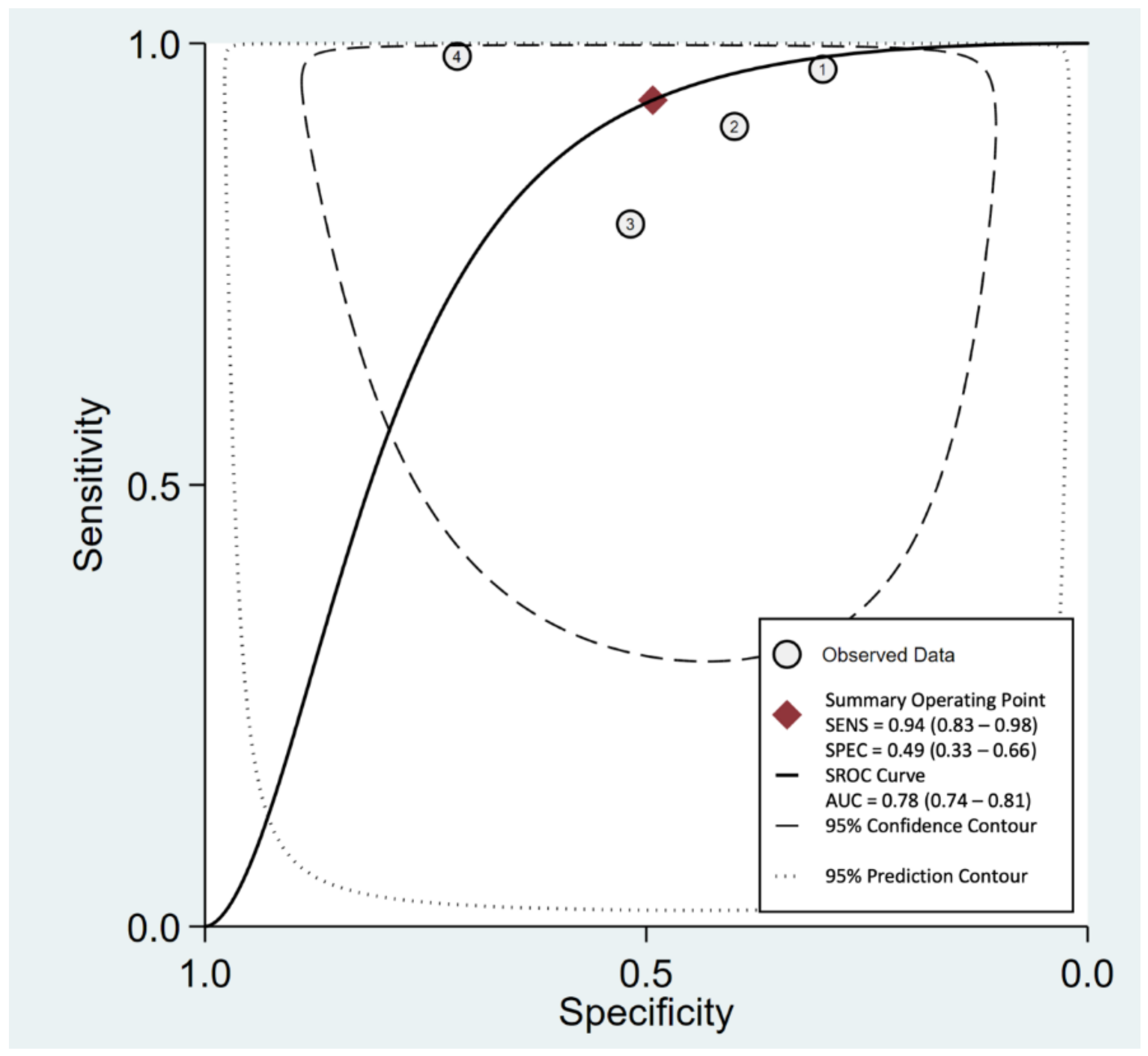
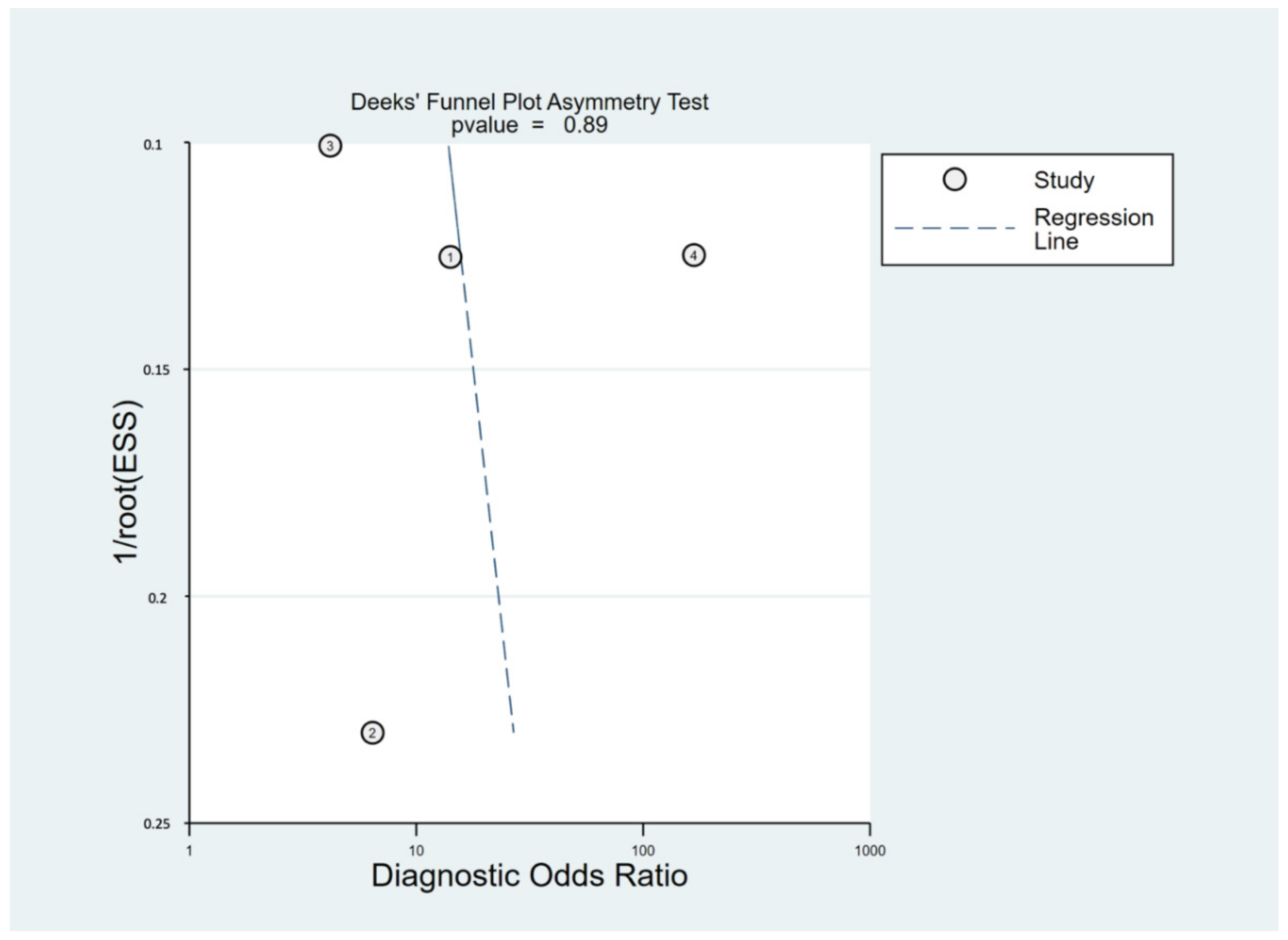
3.3. Pooled Estimates of Sensitivity/Specificity, sROC and DOR
3.4. CoE by GRADE Methodology
3.5. Fagan’s Nomogram Plot Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Humes, D.J.; Simpson, J. Acute appendicitis. BMJ 2006, 333, 530–534. [Google Scholar] [CrossRef] [Green Version]
- Ashdown, H.F.; D’Souza, N.; Karim, D.; Stevens, R.J.; Huang, A.; Harnden, A. Pain over speed bumps in diagnosis of acute appendicitis: Diagnostic accuracy study. BMJ 2012, 345, e8012. [Google Scholar] [CrossRef] [Green Version]
- Wagner, M.; Tubre, D.J.; Asensio, J.A. Evolution and Current Trends in the Management of Acute Appendicitis. Surg. Clin. N. Am. 2018, 98, 1005–1023. [Google Scholar] [CrossRef] [PubMed]
- Di Saverio, S.; Podda, M.; De Simone, B.; Ceresoli, M.; Augustin, G.; Gori, A.; Boermeester, M.; Sartelli, M.; Coccolini, F.; Tarasconi, A.; et al. Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines. World J. Emerg. Surg. 2020, 15, 27. [Google Scholar] [CrossRef]
- Apisarnthanarak, P.; Suvannarerg, V.; Pattaranutaporn, P.; Charoensak, A.; Raman, S.S.; Apisarnthanarak, A. Alvarado score: Can it reduce unnecessary CT scans for evaluation of acute appendicitis? Am. J. Emerg. Med. 2015, 33, 266–270. [Google Scholar] [CrossRef]
- Nicqeshen, N.; Dilashini, S.; Kirthana, S. Role of clinical scoring system and imaging in acute appendicitis in adults: A review of literature. Med. J. Malays. 2020, 75, 316–321. [Google Scholar]
- Kim, H.Y.; Park, J.H.; Lee, Y.J.; Lee, S.S.; Jeon, J.J.; Lee, K.H. Systematic Review and Meta-Analysis of CT Features for Differentiating Complicated and Uncomplicated Appendicitis. Radiology 2018, 287, 104–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eng, K.A.; Abadeh, A.; Ligocki, C.; Lee, Y.K.; Moineddin, R.; Adams-Webber, T.; Schuh, S.; Doria, A.S. Acute Appendicitis: A Meta-Analysis of the Diagnostic Accuracy of US, CT, and MRI as Second-Line Imaging Tests after an Initial US. Radiology 2018, 288, 717–727. [Google Scholar] [CrossRef] [Green Version]
- Seetahal, S.A.; Bolorunduro, O.B.; Sookdeo, T.C.; Oyetunji, T.A.; Greene, W.R.; Frederick, W.; Cornwell, E.E., 3rd; Chang, D.C.; Siram, S.M. Negative appendectomy: A 10-year review of a nationally representative sample. Am. J. Surg. 2011, 201, 433–437. [Google Scholar] [CrossRef] [PubMed]
- Eid, M.M.; Al-Kaisy, M. The utility of the speed bump sign for diagnosing acute appendicitis. Am. J. Emerg. Med. 2020, 38, 1551–1553. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (updated February 2021). Available online: www.training.cochrane.org/handbook (accessed on 16 January 2022).
- Boswell, L.; Hulme, P. BET 2: Utility of the speed bump sign in diagnosis of acute appendicitis. Emerg. Med. J. 2018, 35, 397–398. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M.; The QUADAS-2 Group. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Takwoingi, Y.; Riley, R.D.; Deeks, J.J. Meta-analysis of diagnostic accuracy studies in mental health. Evid.-Based Ment. Health 2015, 18, 103–109. [Google Scholar] [CrossRef]
- Gopalakrishna, G.; Mustafa, R.A.; Davenport, C.; Scholten, R.J.; Hyde, C.; Brozek, J.; Schunemann, H.J.; Bossuyt, P.M.; Leeflang, M.M.; Langendam, M.W. Applying Grading of Recommendations Assessment, Development and Evaluation (GRADE) to diagnostic tests was challenging but doable. J. Clin. Epidemiol. 2014, 67, 760–768. [Google Scholar] [CrossRef] [Green Version]
- Golledge, J.; Toms, A.P.; Franklin, I.J.; Scriven, M.W.; Galland, R.B. Assessment of peritonism in appendicitis. Ann. R. Coll. Surg. Engl. 1996, 78, 11–14. [Google Scholar]
- Haider, A.M.; Ramahi, A.L. Speed Bump Can Help To Diagnose Acute Appendicitis. Eur. J. Biol. Med. Sci. Res. 2015, 3, 40–44. [Google Scholar]
- Muslim, A.; Albahadili, M. New Sign for Diagnosis of Acute Appendicitis. J. Res. Lepid. 2019, 50, 171–176. [Google Scholar] [CrossRef]
- Jones, C.M.; Athanasiou, T. Summary receiver operating characteristic curve analysis techniques in the evaluation of diagnostic tests. Ann. Thorac. Surg. 2005, 79, 16–20. [Google Scholar] [CrossRef]
- Glas, A.S.; Lijmer, J.G.; Prins, M.H.; Bonsel, G.J.; Bossuyt, P.M. The diagnostic odds ratio: A single indicator of test performance. J. Clin. Epidemiol. 2003, 56, 1129–1135. [Google Scholar] [CrossRef]
- Frountzas, M.; Stergios, K.; Kopsini, D.; Schizas, D.; Kontzoglou, K.; Toutouzas, K. Alvarado or RIPASA score for diagnosis of acute appendicitis? A meta-analysis of randomized trials. Int. J. Surg. 2018, 56, 307–314. [Google Scholar] [CrossRef]
- Eun, S.; Ho, I.G.; Bae, G.E.; Kim, H.; Koo, C.M.; Kim, M.K.; Yoon, S.H. Neutrophil-to-lymphocyte ratio for the diagnosis of pediatric acute appendicitis: A systematic review and meta-analysis. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 7097–7107. [Google Scholar] [CrossRef] [PubMed]
- Cui, W.; Liu, H.; Ni, H.; Qin, X.; Zhu, L. Diagnostic accuracy of procalcitonin for overall and complicated acute appendicitis in children: A meta-analysis. Ital. J. Pediatr. 2019, 45, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fu, J.; Zhou, X.; Chen, L.; Lu, S. Abdominal Ultrasound and Its Diagnostic Accuracy in Diagnosing Acute Appendicitis: A Meta-Analysis. Front. Surg. 2021, 8, 707160. [Google Scholar] [CrossRef] [PubMed]
- Sackett, D.L.; Straus, S. On some clinically useful measures of the accuracy of diagnostic tests. ACP J. Club 1998, 129, A17–A19. [Google Scholar]
- Alvarado, A. A practical score for the early diagnosis of acute appendicitis. Ann. Emerg. Med. 1986, 15, 557–564. [Google Scholar] [CrossRef]
- Chong, C.F.; Adi, M.I.; Thien, A.; Suyoi, A.; Mackie, A.J.; Tin, A.S.; Tripathi, S.; Jaman, N.H.; Tan, K.K.; Kok, K.Y.; et al. Development of the RIPASA score: A new appendicitis scoring system for the diagnosis of acute appendicitis. Singap. Med. J. 2010, 51, 220–225. [Google Scholar]
- Bom, W.J.; Bolmers, M.D.; Gans, S.L.; van Rossem, C.C.; van Geloven, A.A.W.; Bossuyt, P.M.M.; Stoker, J.; Boermeester, M.A. Discriminating complicated from uncomplicated appendicitis by ultrasound imaging, computed tomography or magnetic resonance imaging: Systematic review and meta-analysis of diagnostic accuracy. BJS Open 2021, 5, zraa030. [Google Scholar] [CrossRef]
- Wickramasinghe, D.P.; Xavier, C.; Samarasekera, D.N. The Worldwide Epidemiology of Acute Appendicitis: An Analysis of the Global Health Data Exchange Dataset. World J. Surg. 2021, 45, 1999–2008. [Google Scholar] [CrossRef]
- Baeyens, J.P.; Serrien, B.; Goossens, M.; Clijsen, R. Questioning the “SPIN and SNOUT” rule in clinical testing. Arch. Physiother. 2019, 9, 4. [Google Scholar] [CrossRef] [Green Version]
- Andersson, R.E. Meta-analysis of the clinical and laboratory diagnosis of appendicitis. Br. J. Surg. 2004, 91, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Schunemann, H.J.; Mustafa, R.A.; Brozek, J.; Steingart, K.R.; Leeflang, M.; Murad, M.H.; Bossuyt, P.; Glasziou, P.; Jaeschke, R.; Lange, S.; et al. GRADE guidelines: 21 part 2. Test accuracy: Inconsistency, imprecision, publication bias, and other domains for rating the certainty of evidence and presenting it in evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2020, 122, 142–152. [Google Scholar] [CrossRef]
- Schunemann, H.J.; Mustafa, R.A.; Brozek, J.; Santesso, N.; Bossuyt, P.M.; Steingart, K.R.; Leeflang, M.; Lange, S.; Trenti, T.; Langendam, M.; et al. GRADE guidelines: 22. The GRADE approach for tests and strategies-from test accuracy to patient-important outcomes and recommendations. J. Clin. Epidemiol. 2019, 111, 69–82. [Google Scholar] [CrossRef] [PubMed]
- Hultcrantz, M.; Mustafa, R.A.; Leeflang, M.M.G.; Lavergne, V.; Estrada-Orozco, K.; Ansari, M.T.; Izcovich, A.; Singh, J.; Chong, L.Y.; Rutjes, A.; et al. Defining ranges for certainty ratings of diagnostic accuracy: A GRADE concept paper. J. Clin. Epidemiol. 2020, 117, 138–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Golledge et al. | Ashdown et al. | Haider et al. | Eid et al. |
|---|---|---|---|---|
| Year | 1996 | 2012 | 2015 | 2020 |
| Country | United Kingdom | United Kingdom | Iraq | United Arab Emirates |
| Study design | Prospective | Prospective | Prospective | Prospective |
| Sample size (Male/female) | 100 (39/61) | 64 (NA/NA) | 89 (NA/NA) | 90 (65/23) |
| Median age (years) Range (years) | 25 (4–81) | 34 (17–76) | 39 (16–65) | 34 (15–53) |
| Sensitivity | 0.80 | 0.97 | 0.97 | 0.90 |
| Specificity | 0.52 | 0.30 | 0.30 | 0.40 |
| Question: Should ‘Speed Bump Sign’ Used to Diagnose Acute Appendicitis in Emergency Department? | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Sensitivity | 0.94 (95% CI: 0.83 to 0.98) | ||||||||
| Specificity | 0.49 (95% CI: 0.33 to 0.66) | ||||||||
| Prevalence | 0.228% | ||||||||
| Outcome | № of Studies (№ of Patients) | Study Design | Factors That May Decrease Certainty of Evidence | Effect per 100,000 Patients Tested | Test Accuracy CoE | ||||
| Risk of Bias | Indirectness | Inconsistency | Imprecision | Publication Bias | Pre-Test Probability of 0.228% | ||||
| True positives (patients with acute appendicitis) | 4 studies 343 patients | cross-sectional (cohort type accuracy study) | serious a | not serious | serious b | not serious | none | 214 (189 to 223) | ⨁⨁◯◯ Low |
| False negatives (patients incorrectly classified as not having acute appendicitis) | 14 (5 to 39) | ||||||||
| True negatives (patients without acute appendicitis) | 4 studies 343 patients | cross-sectional (cohort type accuracy study) | serious a | not serious | serious b | serious c | none | 48,888 (32925 to 65,850) | ⨁◯◯◯ Very low |
| False positives (patients incorrectly classified as having acute appendicitis) | 50,884 (33,922 to 66,847) | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, L.; Ling, C.-H.; Lai, P.-C.; Huang, Y.-T. Can The ‘Speed Bump Sign’ Be a Diagnostic Tool for Acute Appendicitis? Evidence-Based Appraisal by Meta-Analysis and GRADE. Life 2022, 12, 138. https://doi.org/10.3390/life12020138
Wang L, Ling C-H, Lai P-C, Huang Y-T. Can The ‘Speed Bump Sign’ Be a Diagnostic Tool for Acute Appendicitis? Evidence-Based Appraisal by Meta-Analysis and GRADE. Life. 2022; 12(2):138. https://doi.org/10.3390/life12020138
Chicago/Turabian StyleWang, Ling, Ching-Hsien Ling, Pei-Chun Lai, and Yen-Ta Huang. 2022. "Can The ‘Speed Bump Sign’ Be a Diagnostic Tool for Acute Appendicitis? Evidence-Based Appraisal by Meta-Analysis and GRADE" Life 12, no. 2: 138. https://doi.org/10.3390/life12020138
APA StyleWang, L., Ling, C.-H., Lai, P.-C., & Huang, Y.-T. (2022). Can The ‘Speed Bump Sign’ Be a Diagnostic Tool for Acute Appendicitis? Evidence-Based Appraisal by Meta-Analysis and GRADE. Life, 12(2), 138. https://doi.org/10.3390/life12020138