
Efficacy and Safety of Da-Chai-Hu-Tang in Lipid Profiles in High-Risk, Statin-Treated Patients with Residual HyperTG: A 12-Week, Randomized, Active-Control, Open Clinical Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
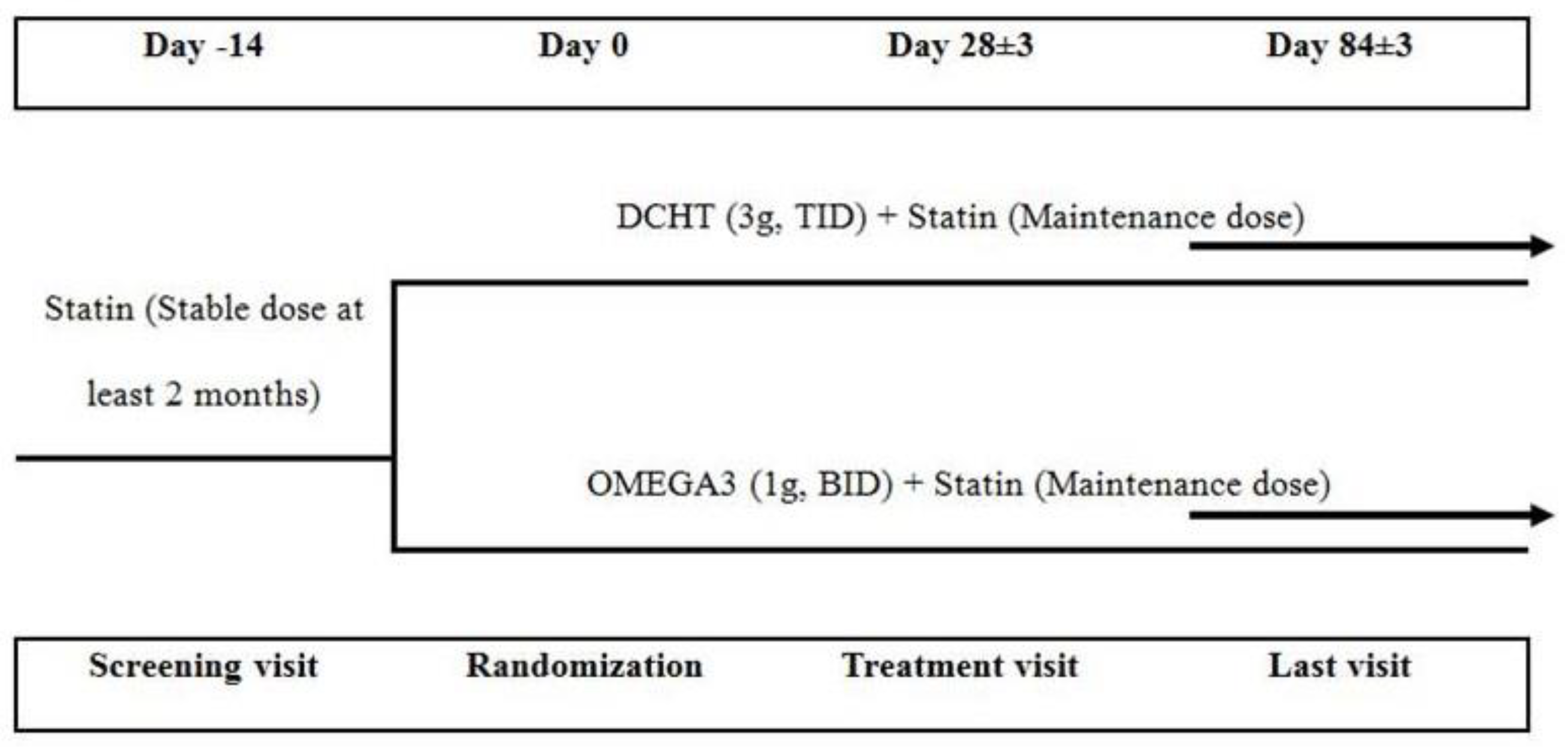
2.2. Study Design
2.3. Study Medication
2.4. Efficacy and Safety Assessment
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
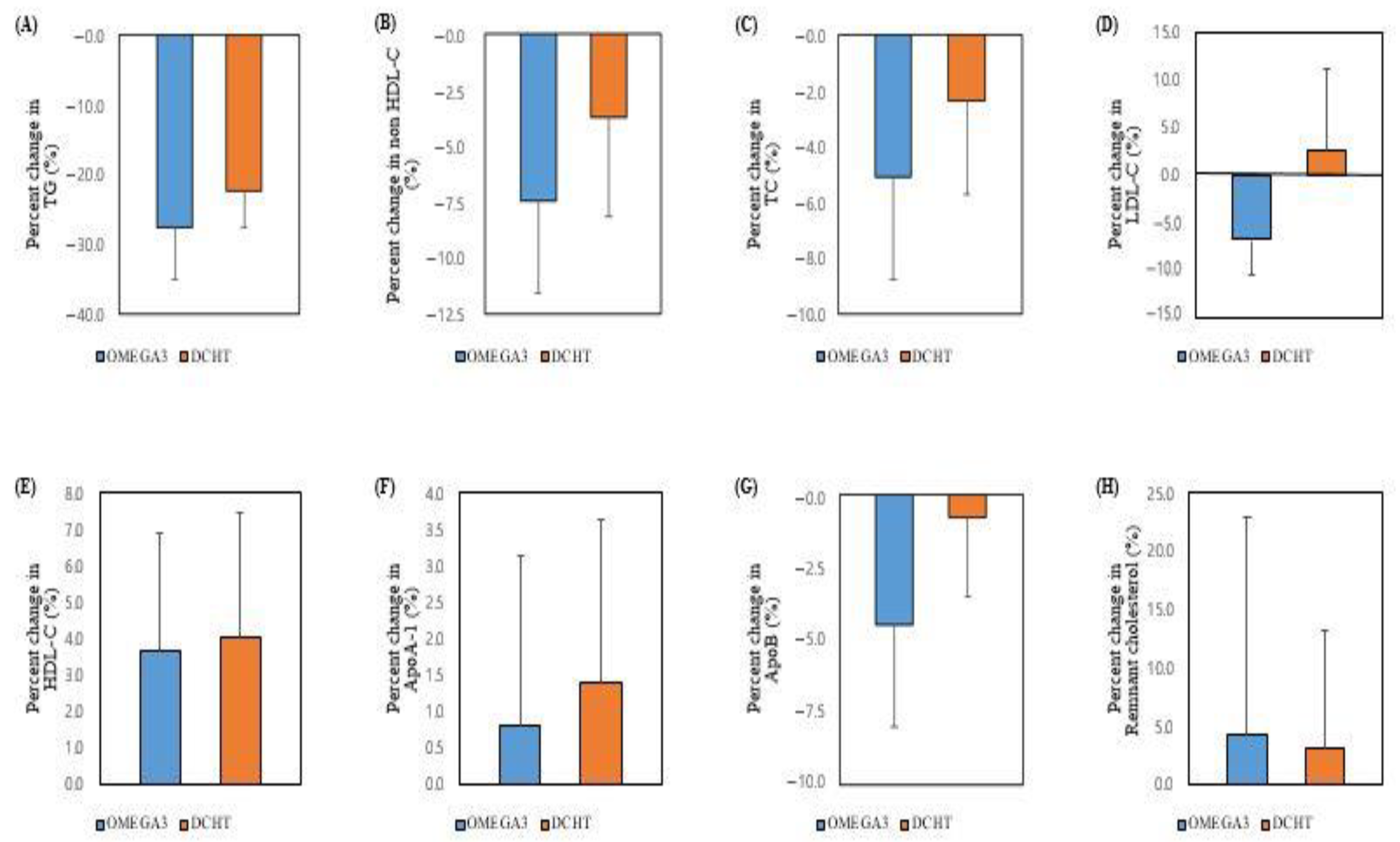
3.2. Efficacy Analyses
3.3. Safety Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lee, Y.S.; Lee, J.M.; Chung, H.M.; Woo, J.S.; Lee, B.C.; Kim, W. Efficacy and Safety of Da-Chai-Hu-Tang in Lipid Profile in High-Risk, Statin-Treated Patients with Residual HyperTG: An 12-Week, Randomized, Active-Control, Open Clinical Study 2021. Available online: https://www.researchsquare.com/article/rs-842205/v1 (accessed on 13 September 2021).
- Grundy, S.M.; Stone, N.J.; Bailey, A.L.; Beam, C.; Birtcher, K.K.; Blumenthal, R.S.; Braun, L.T.; de Ferranti, S.; Faiella-Tommasino, J.; Forman, D.E.; et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2019, 73, e285–e350. [Google Scholar] [CrossRef] [PubMed]
- Kei, A.; Tellis, C.; Liberopoulos, E.; Tselepis, A.; Elisaf, M. Effect of Switch to the Highest Dose of Rosuvastatin Versus Add-on-Statin Fenofibrate Versus Add-on-Statin Nicotinic Acid/Laropiprant on Oxidative Stress Markers in Patients with Mixed Dyslipidemia. Cardiovasc. Ther. 2014, 32, 139–146. [Google Scholar] [CrossRef] [Green Version]
- Fulcher, J.; O’Connell, R.; Voysey, M.; Emberson, J.; Blackwell, L.; Mihaylova, B.; Simes, J.; Collins, R.; Kirby, A.; Colhoun, H.; et al. Efficacy and safety of LDL-lowering therapy among men and women: Meta-analysis of individual data from 174,000 participants in 27 randomised trials. Lancet 2015, 385, 1397–1405. [Google Scholar] [PubMed]
- Grundy, S.M.; Becker, D.; Clark, L.T.; Cooper, R.S.; Denke, M.A.; Howerd, W.J.; Hunninghake, D.B.; Illingworth, D.R.; Leupker, R.V.; McBride, P.; et al. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002, 106, 3143–3421. [Google Scholar]
- Libby, P. The forgotten majority: Unfinished business in cardiovascular risk reduction. J. Am. Coll. Cardiol. 2005, 46, 1225–1228. [Google Scholar] [CrossRef]
- Ganda, O.P.; Bhatt, D.L.; Mason, R.P.; Miller, M.; Boden, W.E. Unmet Need for Adjunctive Dyslipidemia Therapy in Hypertriglyceridemia Management. J. Am. Coll. Cardiol. 2018, 72, 330–343. [Google Scholar] [CrossRef]
- Sarwar, N.; Danesh, J.; Eiriksdottir, G.; Sigurdsson, G.; Wareham, N.; Bingham, S.; Boekholdt, S.M.; Khaw, K.-T.; Gudnason, V. Triglycerides and the risk of coronary heart disease: 10,158 incident cases among 262,525 participants in 29 Western prospective studies. Circulation 2007, 115, 450–458. [Google Scholar] [CrossRef]
- Triglyceride Coronary Disease Genetics Consortium and Emerging Risk Factors Collaboration; Sarwar, N.; Sandhu, M.S.; Ricketts, S.L.; Butterworth, A.S.; Di Angelantonio, E.; Boekholdt, S.M.; Ouwehand, W.; Watkins, H.; Samani, N.J.; et al. Triglyceride-mediated pathways and coronary disease: Collaborative analysis of 101 studies. Lancet 2010, 375, 1634–1639. [Google Scholar]
- Nordestgaard, B.G.; Benn, M.; Schnohr, P.; Tybjærg-Hansen, A. Nonfasting triglycerides and risk of myocardial infarction, ischemic heart disease, and death in men and women. JAMA 2007, 298, 299–308. [Google Scholar] [CrossRef] [Green Version]
- Nordestgaard, B.G.; Varbo, A. Triglycerides and cardiovascular disease. Lancet 2014, 384, 626–635. [Google Scholar] [CrossRef]
- Miller, M.; Cannon, C.P.; Murphy, S.A.; Qin, J.; Ray, K.K.; Braunwald, E. Impact of triglyceride levels beyond low-density lipoprotein cholesterol after acute coronary syndrome in the PROVE IT-TIMI 22 trial. J. Am. Coll. Cardiol. 2008, 51, 724–730. [Google Scholar] [CrossRef] [Green Version]
- Kim, C.H.; Han, K.A.; Yu, J.; Lee, S.H.; Jeon, H.K.; Kim, S.H.; Kim, S.Y.; Han, K.H.; Won, K.; Kim, D.-B.; et al. Efficacy and safety of adding omega-3 fatty acids in statin-treated patients with residual hypertriglyceridemia: ROMANTIC (Rosuvastatin-OMAcor iN residual hyperTrIglyCeridemia), a randomized, double-blind, and placebo-controlled trial. Clin. Ther. 2018, 40, 83–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhatt, D.L.; Steg, P.G.; Miller, M.; Brinton, E.A.; Jacobson, T.A.; Ketchum, S.B.; Doyle, R.T., Jr.; Juliano, R.A.; Jiao, L.; Granowitz, C.; et al. Cardiovascular Risk Reduction with Icosapent Ethyl for Hypertriglyceridemia. N. Engl. J. Med. 2019, 380, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Boden, W.E.; Probstfield, J.L.; Anderson, T.; Chaitman, B.R.; Desvignes-Nickens, P.; Koprowicz, K.; McBride, R.; Teo, K.; Weintraub, W. Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy. N. Engl. J. Med. 2011, 365, 2255–2267. [Google Scholar]
- Group, A.S. Effects of combination lipid therapy in type 2 diabetes mellitus. N. Engl. J. Med. 2010, 362, 1563–1574. [Google Scholar]
- Hallén, J.; Sreeharan, N. Development of triglyceride-lowering drugs to address residual cardiovascular risk: Strategic and clinical considerations. European Heart Journal–Cardiovascular Pharmacotherapy 2018, 4, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, K.; Ogawa, Y.; Yanagita, T.; Morito, F.; Fukushima, N.; Ozaki, I.; Mizuta, T.; Setoguchi, Y.; Sakai, T. Pharmacological effects of dai-saiko-to on lipid biosynthesis in cultured human hepatocyte HepG2 cells. J. Ethnopharmacol. 1995, 46, 49–54. [Google Scholar] [CrossRef]
- Umeda, M.; Amagaya, S.; Ogihara, Y. Effect of shosaikoto, daisaikoto and sannoshashinto (traditional Japanese and Chinese medicines) on experimental hyperlipidemia in rats. J. Ethnopharmacol. 1989, 26, 255–269. [Google Scholar] [CrossRef]
- Iizuka, A.; Iijima, O.T.; Yoshie, F.; Makino, B.; Amagaya, S.; Komatsu, Y.; Kondo, K.; Matsumoto, A.; Itakura, H. Inhibitory effects of Dai-saiko-to (Da-Chai-Hu-Tang) on the progression of atherosclerotic lesions in Kurosawa and Kusanagi-hypercholesterolemic rabbits. J. Ethnopharmacol. 1998, 63, 209–218. [Google Scholar] [CrossRef]
- Yoshie, F.; Iizuka, A.; Kondo, K.; Matsumoto, A.; Itakura, H.; Komatsu, Y. Antiatherosclerotic effect of Dai-saiko-to in the Kurosawa and Kusanagi hypercholesterolemic rabbit. Res. Commun. Pharmacol. Toxicol. 2000, 5, 77–90. [Google Scholar]
- Iizuka, A.; Yoshie, F.; Amagaya, S.; Yasuda, T.; Iizuka, M.; Yamaguchi, H.; Yamaguchi, H.; Nagumo, S.; Kondo, K. Effect of dai-saiko-to (Da-Chai-Hu-Tang) on ldl-receptor gene expression in human hepatoma cell line (hepg2). Am. J. Plant Sci. 2013, 4, 28475. [Google Scholar] [CrossRef] [Green Version]
- Yamano, S. Effects of Dai-saiko-to on lipid metabolism and common carotid hemodynamics in patients with hyperlipidemia. J. Tradit. Med. 1994, 11, 38–43. [Google Scholar]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; de Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk: The Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS). Eur. Heart J. 2019, 41, 111–188. [Google Scholar] [CrossRef] [PubMed]
- Mian, M.; Brunelleschi, S.; Tarli, S.; Rubino, A.; Benetti, D.; Fantozzi, R.; Zilletti, L. Rhein: An anthraquinone that modulates superoxide anion production from human neutrophils. J. Pharm. Pharmacol. 1987, 39, 845–847. [Google Scholar] [CrossRef] [PubMed]
- Zheng, C.D.; Duan, Y.Q.; Gao, J.M.; Ruan, Z.G. Screening for anti-lipase properties of 37 traditional Chinese medicinal herbs. J. Chin. Med. Assoc. 2010, 73, 319–324. [Google Scholar] [CrossRef] [Green Version]
- Goel, V.; Cheema, S.K.; Agellon, L.B.; Ooraikul, B.; Basu, T.K. Dietary rhubarb (Rheum rhaponticum) stalk fibre stimulates cholesterol 7α-hydroxylase gene expression and bile acid excretion in cholesterol-fed C57BL/6J mice. Br. J. Nutr. 1999, 81, 65–71. [Google Scholar] [CrossRef] [Green Version]
- Matsuo, Y.; Matsumoto, K.; Inaba, N.; Mimaki, Y. Daisaikoto inhibits pancreatic lipase activity and decreases serum triglyceride levels in mice. Biol. Pharm. Bull. 2018, 41, 1485–1488. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.M.; Kang, Y.H.; Kim, K.K.; Kim, T.W.; Choe, M. A study of the lipoprotein lipase inhibitory mechanism of Poncirus trifoliata water extracts. J. Nutr. Health 2015, 48, 9–18. [Google Scholar] [CrossRef]
- Yoshie, F.; Iizuka, A.; Komatsu, Y.; Matsumoto, A.; Itakura, H.; Kondo, K. Effects of Dai-saiko-to (Da-Chai-Hu-Tang) on plasma lipids and atherosclerotic lesions in female heterozygous heritable Kurosawa and Kusanagi-hypercholesterolemic (KHC) rabbits. Pharmacol. Res. 2004, 50, 223–230. [Google Scholar] [CrossRef]
- Stirban, A.; Nandrean, S.; Götting, C.; Tamler, R.; Pop, A.; Negrean, M.; Gawlowski, T.; Stratmann, B.; Tschoepe, D. Effects of n-3 fatty acids on macro- and microvascular function in subjects with type 2 diabetes mellitus. Am. J. Clin. Nutr. 2010, 91, 808–813. [Google Scholar] [CrossRef]
- Dangardt, F.; Osika, W.; Chen, Y.; Nilsson, U.; Gan, L.-M.; Gronowitz, E.; Strandvik, B.; Friberg, P. Omega-3 fatty acid supplementation improves vascular function and reduces inflammation in obese adolescents. Atherosclerosis 2010, 212, 580–585. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.-Y.; Yiu, K.-H.; Li, S.-W.; Lee, S.; Tam, S.; Lau, C.-P.; Tse, H.-F. Fish-oil supplement has neutral effects on vascular and metabolic function but improves renal function in patients with Type 2 diabetes mellitus. Diabet Med. 2010, 27, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Skulas-Ray, A.C.; Kris-Etherton, P.M.; Harris, W.S.; Vanden Heuvel, J.P.; Wagner, P.R.; West, S.G. Dose-response effects of omega-3 fatty acids on triglycerides, inflammation, and endothelial function in healthy persons with moderate hypertriglyceridemia. Am. J. Clin. Nutr. 2011, 93, 243–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zehr, K.R.; Walker, M.K. Omega-3 polyunsaturated fatty acids improve endothelial function in humans at risk for atherosclerosis: A review. Prostaglandins Lipid Mediat. 2018, 134, 131–140. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| OMEGA3 | DCHT | p-Value | |
|---|---|---|---|
| Age | 62.5 ± 8.6 | 64.9 ± 8.2 | 0.36 |
| Gender | 0.43 | ||
| Female | 5 (25.0) | 8 (36.4) | |
| Male | 15 (75.0) | 14 (63.6) | |
| BMI | 26.6 ± 3.5 | 26.9 ± 2.7 | 0.74 |
| Past medical history | |||
| Stable angina | 5 (25.0) | 9 (40.9) | 0.28 |
| ACS | 8 (40.0) | 7 (31.8) | 0.58 |
| PCI | 11 (55.0) | 8 (36.4) | 0.23 |
| Stroke | 2 (10.0) | 2 (9.1) | 1.00 |
| Carotid atherosclerosis | 5 (25.0) | 2 (9.1) | 0.23 |
| DM | 12 (60.0) | 11 (50.0) | 0.26 |
| HTN | 14 (70.0) | 18 (81.8) | 0.48 |
| Current smoker | 3 (15.0) | 2 (9.1) | 0.34 |
| OMEGA3 | DCHT | ||||||
|---|---|---|---|---|---|---|---|
| Baseline | 12 Weeks | Percent Change (%) | Baseline | 12 Weeks | Percent Change (%) | p-Value | |
| TG | 294.5 ± 72.0 | 210.0 ± 107.8 | −27.6 ± 33.6 | 288.7 ± 59.1 | 227.5 ± 98.1 | −22.5 ± 24.1 | 0.58 |
| Total cholesterol | 151.2 ± 30.8 | 142.6 ± 26.8 | −4.6 ± 14.8 | 152.2 ± 27.1 | 146.6 ± 20.0 | −2.1 ± 14.2 | 0.59 |
| LDL-C | 88.6 ± 21.8 | 80.8 ± 17.5 | −6.8 ± 16.2 | 86.2 ± 21.5 | 82.9 ± 15.4 | 2.7 ± 40.4 | 0.49 |
| HDL-C | 42.7 ± 8.5 | 44.2 ± 10.8 | 3.7 ± 14.5 | 45.4 ± 8.1 | 46.7 ± 8.1 | 4.1 ± 16.0 | 0.93 |
| Apo A-1 | 126.9 ± 71.8 | 128.1 ± 24.9 | 0.8 ± 10.4 | 132.8 ± 15.0 | 133.9 ± 14.9 | 1.4 ± 10.5 | 0.86 |
| Apo B | 79.5 ± 17.5 | 74.9 ± 16.5 | −4.5 ± 15.8 | 75.8 ± 12.4 | 74.6 ± 11.9 | −0.8 ± 12.8 | 0.41 |
| Non-HDL | 108.5 ± 30.3 | 98.0 ± 26.1 | −7.5 ± 18.1 | 106.8 ± 25.5 | 99.9 ± 20.9 | −3.8 ± 20.7 | 0.54 |
| LDL-C/HDL-C | 2.1 ± 0.7 | 1.9 ± 0.6 | −9.0 ± 16.7 | 1.9 ± 0.5 | 1.8 ± 0.5 | 1.4 ± 46.9 | 0.62 |
| TC/HDL-C | 3.6 ± 1.0 | 3.4 ± 1.0 | −6.7 ± 16.6 | 3.4 ± 0.7 | 3.2 ± 0.7 | −4.1 ± 19.1 | 0.65 |
| Non-HDL-C/HDL-C | 2.6 ± 1.0 | 2.4 ± 1.0 | −9.1 ± 21.9 | 2.4 ± 0.7 | 2.2 ± 0.7 | −4.8 ± 28.2 | 0.59 |
| Apo B/Apo A-I | 0.6 ± 0.2 | 0.6 ± 0.2 | −4.9 ± 15.0 | 0.6 ± 0.1 | 0.6 ± 0.7 | −1.3 ± 16.1 | 0.46 |
| Remnant cholesterol | 19.9 ± 10.8 | 17.2 ± 11.2 | 4.3 ± 83.4 | 20.64 ± 9.2 | 17.00 ± 8.3 | 3.2 ± 82.1 | 0.72 |
| OMEGA3 | DCHT | |||||
|---|---|---|---|---|---|---|
| Baseline | 12 Weeks | p-Value | Baseline | 12 Weeks | p-Value | |
| AST (U/L) | 33.1 ± 13.7 | 34.2 ± 17.6 | 0.81 | 32.1 ± 11.3 | 34.5 ± 17.3 | 0.48 |
| ALT (U/L) | 33.1 ± 12.5 | 34.5 ± 18.4 | 0.96 | 35.2 ± 14.8 | 35.3 ± 17.6 | 0.72 |
| Creatinine (mg/dL) | 0.9 ± 0.2 | 0.9 ± 0.2 | 0.60 | 0.8 ± 0.2 | 0.8 ± 0.2 | 0.73 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, Y.-S.; Lee, J.-M.; Chung, H.; Woo, J.-S.; Lee, B.-C.; Kim, W. Efficacy and Safety of Da-Chai-Hu-Tang in Lipid Profiles in High-Risk, Statin-Treated Patients with Residual HyperTG: A 12-Week, Randomized, Active-Control, Open Clinical Study. Life 2022, 12, 408. https://doi.org/10.3390/life12030408
Lee Y-S, Lee J-M, Chung H, Woo J-S, Lee B-C, Kim W. Efficacy and Safety of Da-Chai-Hu-Tang in Lipid Profiles in High-Risk, Statin-Treated Patients with Residual HyperTG: A 12-Week, Randomized, Active-Control, Open Clinical Study. Life. 2022; 12(3):408. https://doi.org/10.3390/life12030408
Chicago/Turabian StyleLee, Young-Shin, Jung-Myung Lee, Hyemoon Chung, Jong-Shin Woo, Byung-Cheol Lee, and Weon Kim. 2022. "Efficacy and Safety of Da-Chai-Hu-Tang in Lipid Profiles in High-Risk, Statin-Treated Patients with Residual HyperTG: A 12-Week, Randomized, Active-Control, Open Clinical Study" Life 12, no. 3: 408. https://doi.org/10.3390/life12030408
APA StyleLee, Y.-S., Lee, J.-M., Chung, H., Woo, J.-S., Lee, B.-C., & Kim, W. (2022). Efficacy and Safety of Da-Chai-Hu-Tang in Lipid Profiles in High-Risk, Statin-Treated Patients with Residual HyperTG: A 12-Week, Randomized, Active-Control, Open Clinical Study. Life, 12(3), 408. https://doi.org/10.3390/life12030408