
Ultrasound-Guided PECS II + Serratus Plane Fascial Blocks Are Associated with Reduced Opioid Consumption and Lengths of Stay for Minimally Invasive Cardiac Surgery: An Observational Retrospective Study


 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Population and Data Sources
2.2. Primary and Secondary Outcomes
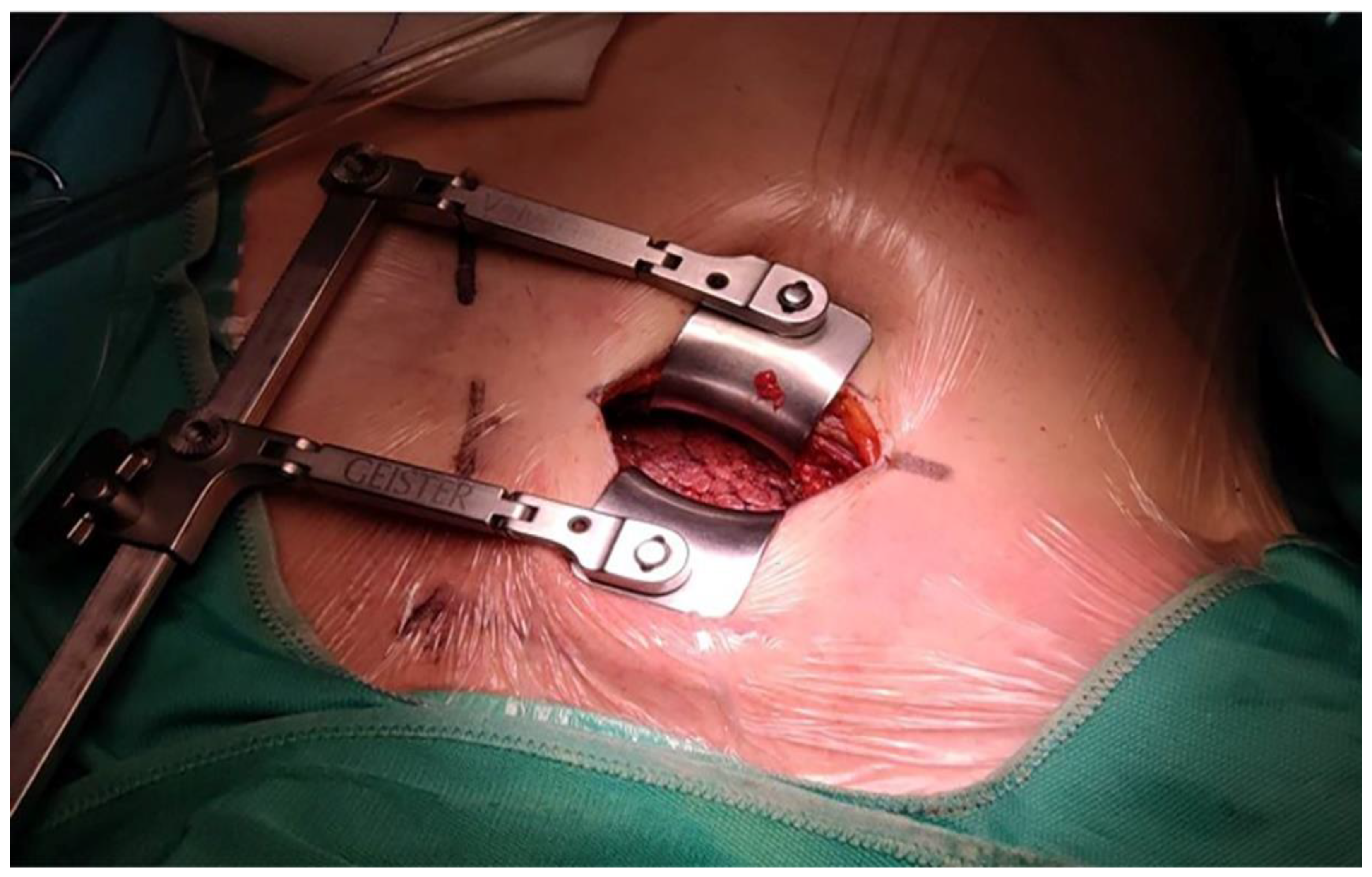
2.3. Pre- and Intra-Operative Management
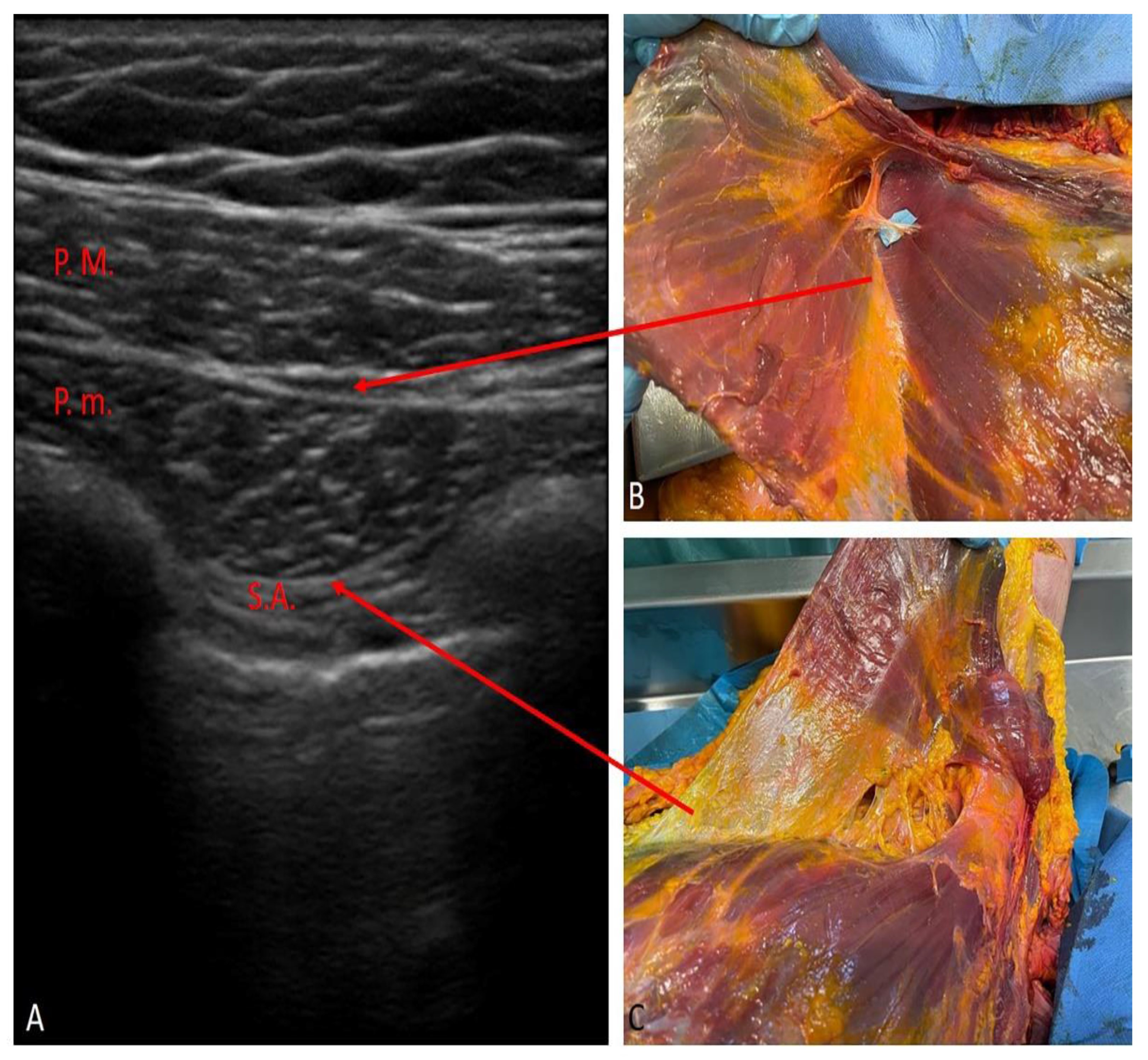
2.3.1. PECS II Block
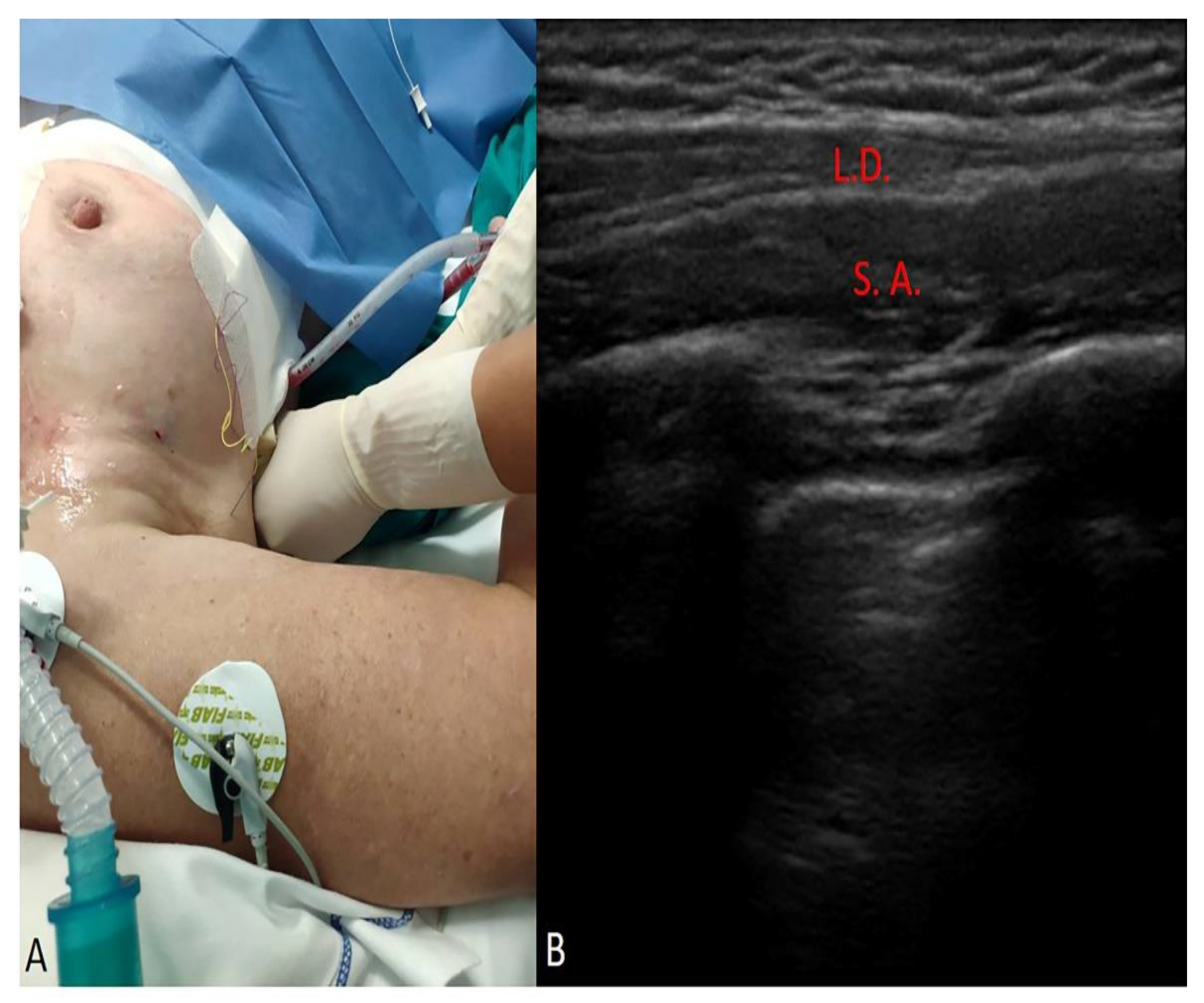
2.3.2. SAP Block
2.4. Statistical Analysis
3. Results
3.1. Primary Outcome
3.2. Secondary Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mariscalco, G.; Musumeci, F. The minithoracotomy approach: A safe and effective alternative for heart valve surgery. Ann. Thorac. Surg. 2014, 97, 356–364. [Google Scholar] [CrossRef]
- Kastengren, M.; Svenarud, P.; Ahlsson, A.; Dalén, M. Minimally invasive mitral valve surgery is associated with a low rate of complications. J. Intern. Med. 2019, 286, 614–626. [Google Scholar] [CrossRef] [Green Version]
- Melloul, E.; Hübner, M.; Scott, M.; Snowden, C.; Prentis, J.; Dejong, C.H.; Garden, O.J.; Farges, O.; Kokudo, N.; Vauthey, J.N.; et al. Guidelines for Perioperative Care for Liver Surgery: Enhanced Recovery after Surgery (ERAS) Society Recommendations. World J. Surg. 2016, 40, 2425–2440. [Google Scholar] [CrossRef] [Green Version]
- Wainwright, T.W.; Gill, M.; McDonald, D.A.; Middleton, R.G.; Reed, M.; Sahota, O.; Yates, P.; Ljungqvist, O. Consensus statement for perioperative care in total hip replacement and total knee replacement surgery: Enhanced Recovery after Surgery (ERAS®) Society recommendations. Acta Orthop. 2020, 91, 3–19. [Google Scholar] [CrossRef] [Green Version]
- Gustafsson, U.O.; Scott, M.J.; Hubner, M.; Nygren, J.; Demartines, N.; Francis, N.; Rockall, T.A.; Young-Fadok, T.M.; Hill, A.G.; Soop, M.; et al. Guidelines for Perioperative Care in Elective Colorectal Surgery: Enhanced Recovery after Surgery (ERAS®) Society Recommendations: 2018. World J. Surg. 2019, 43, 659–695. [Google Scholar] [CrossRef] [Green Version]
- Batchelor, T.J.P.; Rasburn, N.J.; Abdelnour-Berchtold, E.; Brunelli, A.; Cerfolio, R.J.; Gonzalez, M.; Ljungqvist, O.; Petersen, R.H.; Popescu, W.M.; Slinger, P.D.; et al. Guidelines for enhanced recovery after lung surgery: Recommendations of the Enhanced Recovery after Surgery (ERAS®) Society and the European Society of Thoracic Surgeons (ESTS). Eur. J. Cardiothorac. Surg. 2019, 55, 91–115. [Google Scholar] [CrossRef]
- Engelman, D.T.; Ben Ali, W.; Williams, J.B.; Perrault, L.P.; Reddy, V.S.; Arora, R.C.; Roselli, E.E.; Khoynezhad, A.; Gerdisch, M.; Levy, J.H.; et al. Guidelines for Perioperative Care in Cardiac Surgery: Enhanced Recovery after Surgery Society Recommendations. JAMA Surg. 2019, 154, 755–766. [Google Scholar] [CrossRef]
- Kumar, K.N.; Kalyane, R.N.; Singh, N.G.; Nagaraja, P.S.; Krishna, M.; Babu, B.; Varadaraju, R.; Sathish, N.; Manjunatha, N. Efficacy of bilateral pectoralis nerve block for ultrafast tracking and postoperative pain management in cardiac surgery. Ann. Card. Anaesth. 2018, 21, 333–338. [Google Scholar]
- Toscano, A.; Capuano, P.; Costamagna, A.; Burzio, C.; Ellena, M.; Scala, V.; Pasero, D.; Rinaldi, M.; Brazzi, L. The Serratus Anterior Plane Study: Continuous Deep Serratus Anterior Plane Block for Mitral Valve Surgery Performed in Right Minithoracotomy. J. Cardiothorac. Vasc. Anesth. 2020, 34, 2975–2982. [Google Scholar] [CrossRef]
- Ritter, M.J.; Christensen, J.M.; Yalamuri, S.M. Regional Anesthesia for Cardiac Surgery: A Review of Fascial Plane Blocks and Their Uses. Adv. Anesth. 2021, 39, 215–240. [Google Scholar] [CrossRef]
- Devarajan, J.; Balasubramanian, S.; Nazarnia, S.; Lin, C.; Subramaniam, K. Regional Analgesia for Cardiac Surgery Part 1. Current status of neuraxial and paravertebral blocks for adult cardiac surgery. Semin. Cardiothorac. Vasc. Anesth. 2021, 25, 252–264. [Google Scholar] [CrossRef] [PubMed]
- Devarajan, J.; Balasubramanian, S.; Shariat, A.N.; Bhatt, H.V. Regional Analgesia for Cardiac Surgery. Part 2: Peripheral Regional Analgesia for Cardiac Surgery. Semin. Cardiothorac. Vasc. Anesth. 2021, 25, 265–279. [Google Scholar] [CrossRef] [PubMed]
- Constantin, V.; Carap, A.C.; Zaharia, L.; Bobic, S.; Ciudin, A.; Brătilă, E.; Vlădăreanu, V.; Socea, B. High correlation of lung ultrasound and chest X-ray after tube drainage in patients with primary spontaneous pneumothorax: Can we omit X-rays for tube management? Eur. Surg. 2015, 47, 175–180. [Google Scholar] [CrossRef]
- Blanco, R.; Parras, T.; McDonnell, J.G.; Prats-Galino, A. Serratus plane block: A novel ultrasound-guided thoracic wall nerve block. Anaesthesia 2013, 68, 1107–1113. [Google Scholar] [CrossRef] [PubMed]
- Al Ja’bari, A.; Robertson, M.; El-Boghdadly, K.; Albrecht, E. A randomised controlled trial of the pectoral nerves-2 (PECS-2) block for radical mastectomy. Anaesthesia 2019, 74, 1277–1281. [Google Scholar] [CrossRef] [PubMed]
- Chong, M.; Berbenetz, N.; Kumar, K.; Lin, C. The serratus plane block for postoperative analgesia in breast and thoracic surgery: A systematic review and meta-analysis. Reg. Anesth. Pain Med. 2019, 44, 1066–1074. [Google Scholar] [CrossRef]
- Yang, J.K.; Char, D.S.; Motonaga, K.S.; Navaratnam, M.; Dubin, A.M.; Trela, A.; Hanisch, D.G.; McFadyen, G.; Chubb, H.; Goodyer, W.R.; et al. Pectoral nerve blocks decrease postoperative pain and opioid use after pacemaker or implantable cardioverter-defibrillator placement in children. Heart Rhythm. 2020, 17, 1346–1353. [Google Scholar] [CrossRef]
- Martinez, T.; Belveyre, T.; Lopez, A.; Dunyach, C.; Bouzit, Z.; Dubreuil, G.; Zetlaoui, P.; Duranteau, J. Serratus Plane Block Is Effective for Pain Control in Patients with Blunt Chest Trauma: A Case Series. Pain Pract. 2020, 20, 197–203. [Google Scholar] [CrossRef]
- Kaushal, B.; Chauhan, S.; Saini, K.; Bhoi, D.; Bisoi, A.K.; Sangdup, T.; Khan, M.A. Comparison of the Efficacy of Ultrasound-Guided Serratus Anterior Plane Block, Pectoral Nerves II Block, and Intercostal Nerve Block for the Management of Postoperative Thoracotomy Pain after Pediatric Cardiac Surgery. J. Cardiothorac. Vasc. Anesth. 2019, 33, 418–425. [Google Scholar] [CrossRef]
- Black, N.D.; Stecco, C.; Chan, V.W.S. Fascial Plane Blocks: More Questions Than Answers? Anesth. Analg. 2021, 132, 899–905. [Google Scholar] [CrossRef]
- Gawęda, B.; Borys, M.; Belina, B.; Bąk, J.; Czuczwar, M.; Wołoszczuk-Gębicka, B.; Kolowca, M.; Widenka, K. Postoperative pain treatment with erector spinae plane block and pectoralis nerve blocks in patients undergoing mitral/tricuspid valve repair—A randomized controlled trial. BMC Anesthesiol. 2020, 20, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balan, C.; Bubenek-Turconi, S.I.; Tomescu, D.R.; Valeanu, L. Ultrasound-Guided Regional Anesthesia-Current Strategies for Enhanced Recovery after Cardiac Surgery. Medicina 2021, 57, 312. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group 1 | Weight | Height | BMI | Age | FE at the Start | Group 2 | Weight | Height | BMI | Age | FE at the Start |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Number of patients | 41 | 41 | 41 | 41 | 41 | Number of patients | 37 | 37 | 37 | 37 | 37 |
| Minimum | 42 | 152 | 16.8 | 52 | 42 | Minimum | 48 | 150 | 19.2 | 37 | 30 |
| 25% Percentile | 64 | 160 | 23.15 | 62 | 53.5 | 25% Percentile | 59.5 | 161.5 | 22.1 | 59.5 | 55 |
| Median | 74 | 173 | 25.1 | 71 | 60 | Median | 70 | 169 | 24 | 71 | 60 |
| 75% Percentile | 83 | 180 | 26.15 | 77 | 63 | 75% Percentile | 76 | 173 | 25.6 | 78.5 | 62.5 |
| Maximum | 119 | 188 | 51.5 | 85 | 71 | Maximum | 95 | 182 | 33.7 | 85 | 80 |
| Mean | 73.83 | 170.6 | 25.35 | 70.2 | 58.12 | Mean | 68.51 | 168.1 | 24.18 | 67.95 | 59.05 |
| Std. Deviation | 15.24 | 9.96 | 5.28 | 9.06 | 6.84 | Std. Deviation | 11.7 | 8.083 | 3.3 | 12.82 | 8.89 |
| Std. Error of Mean | 2.38 | 1.556 | 0.824 | 1.414 | 1.07 | Std. Error of Mean | 1.924 | 1.329 | 0.54 | 2.11 | 1.46 |
| Lower 95% CI of mean | 69.02 | 167.5 | 23.68 | 67.34 | 55.96 | Lower 95% CI of mean | 64.61 | 165.4 | 23.08 | 63.67 | 56.09 |
| Upper 95% CI of mean | 78.64 | 173.8 | 27.01 | 73.05 | 60.28 | Upper 95% CI of mean | 72.41 | 170.7 | 25.28 | 72.22 | 62.02 |
| Coefficient of variation | 20.64% | 5.838% | 20.83% | 12.9% | 11.78% | Coefficient of variation | 17.08% | 4.81% | 13.65% | 18.87% | 15.06% |
| Variables | Group 1 (n = 41) | Group 2 (n = 37) |
|---|---|---|
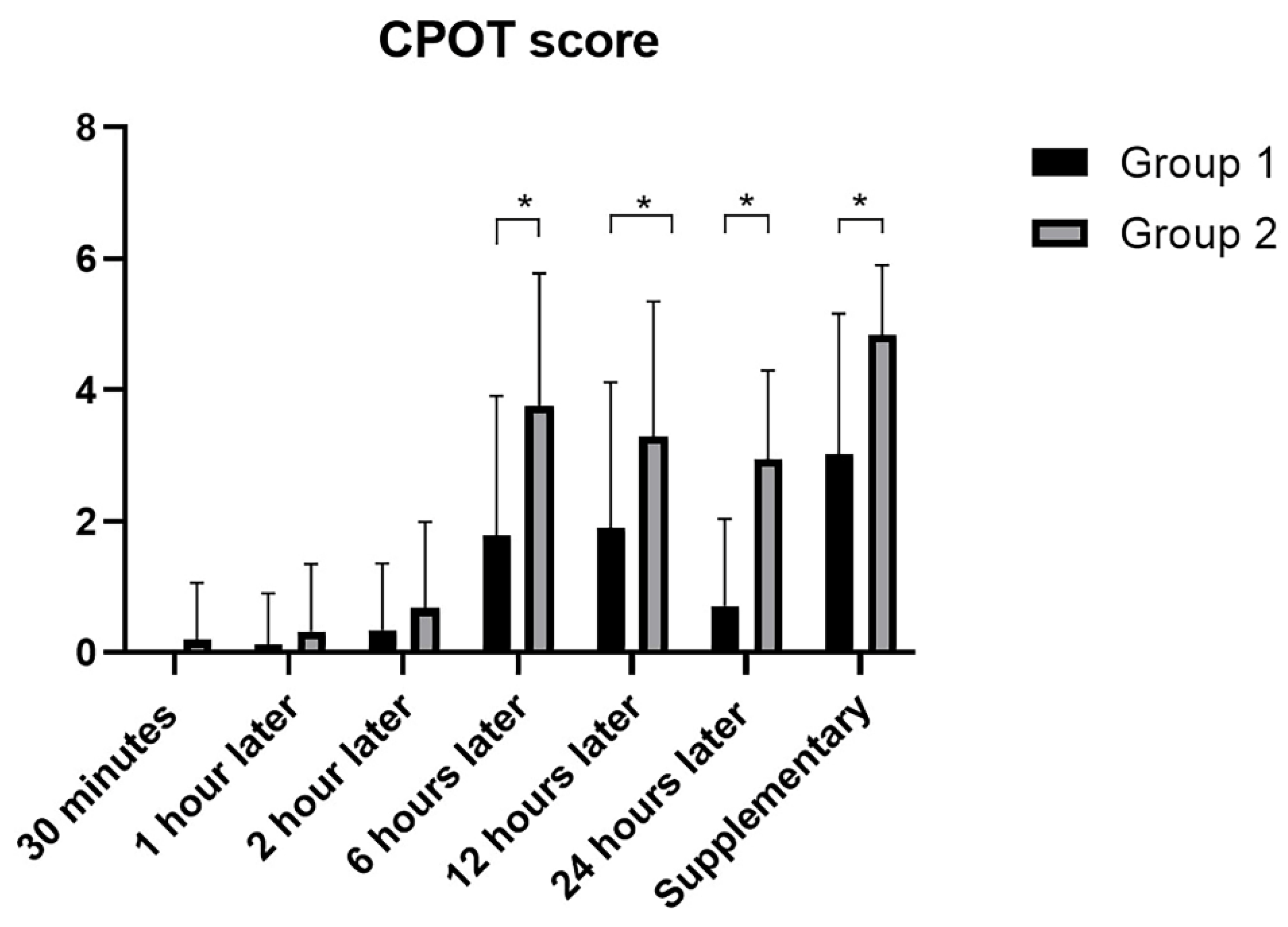
| CPOT score 30 min | 0 ± 0 | 0.18 ± 0.87 |
| CPOT score 1 h | 0.12 ± 0.78 | 0.32 ± 1.02 |
| CPOT score 2 h | 0.34 ± 1.01 | 0.67 ± 1.31 |
| CPOT score 6 h | 1.78 ± 2.12 | 3.75 ± 2.01 |
| CPOT score 12 h | 1.90 ± 2.21 | 3.29 ± 2.05 |
| CPOT score 24 h | 0.70 ± 1.32 | 2.94 ± 1.35 |
| CPOT score supplement analgesia | 3.02 ± 2.13 | 4.83 ± 1.06 |
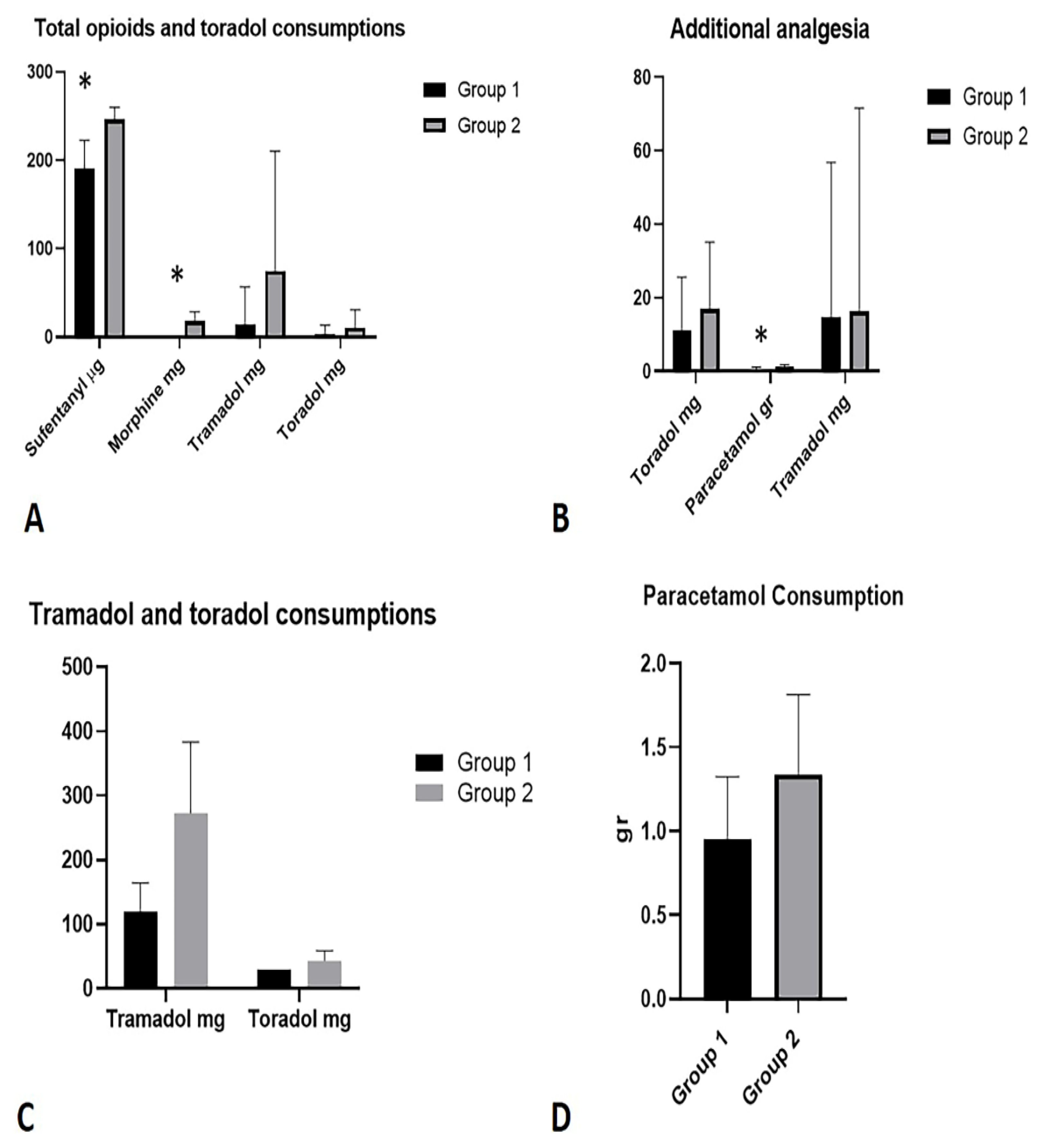
| Sufentanyl (μg) | 191.2 ± 31.4 | 246.2 ± 14.01 |
| Morphine (mg) | 0.12 ± 0.78 | 18.19 ± 10.32 |
| Tramadol (mg) | 14.63 ± 42.2 | 81.08 ± 139.1 |
| Toradol (mg) | 3.65 ± 9.93 | 10.54 ± 20.27 |
| Toradol (mg) Additional analgesia | 10.98 ± 14.63 | 17.03 ± 18.08 |
| Paracetamol (mg) Additional analgesia | 0.53 ± 0.55 | 1.08 ± 0.68 |
| Tramadol (mg) Additional analgesia | 14.63 ± 42.2 | 16.22 ± 55.34 |
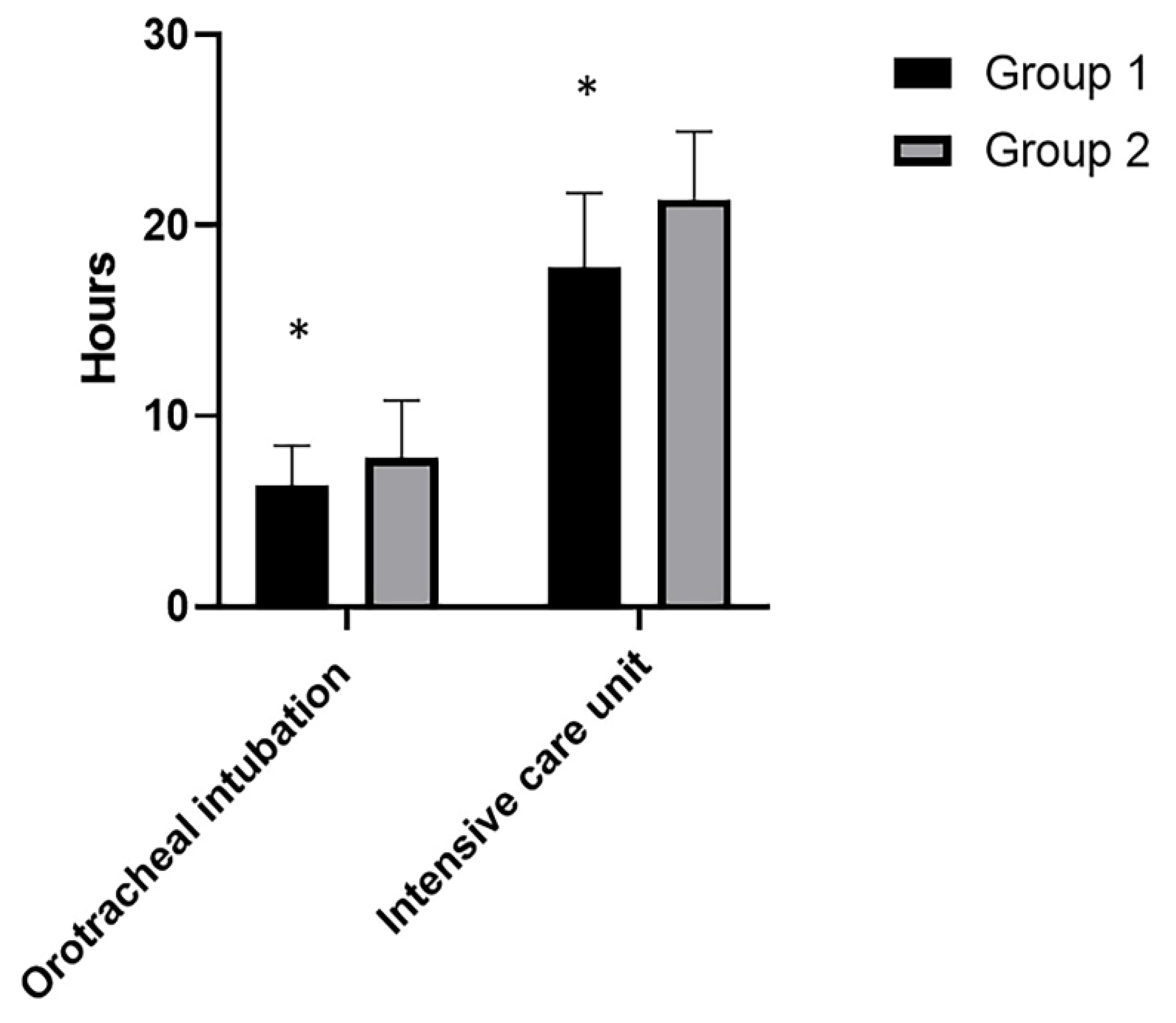
| Orotracheal Intubation (h) | 6.36 ± 2.08 | 7.81 ± 2.98 |
| Intensive care unit (h) | 17.78 ± 3.92 | 21.38 ± 3.55 |
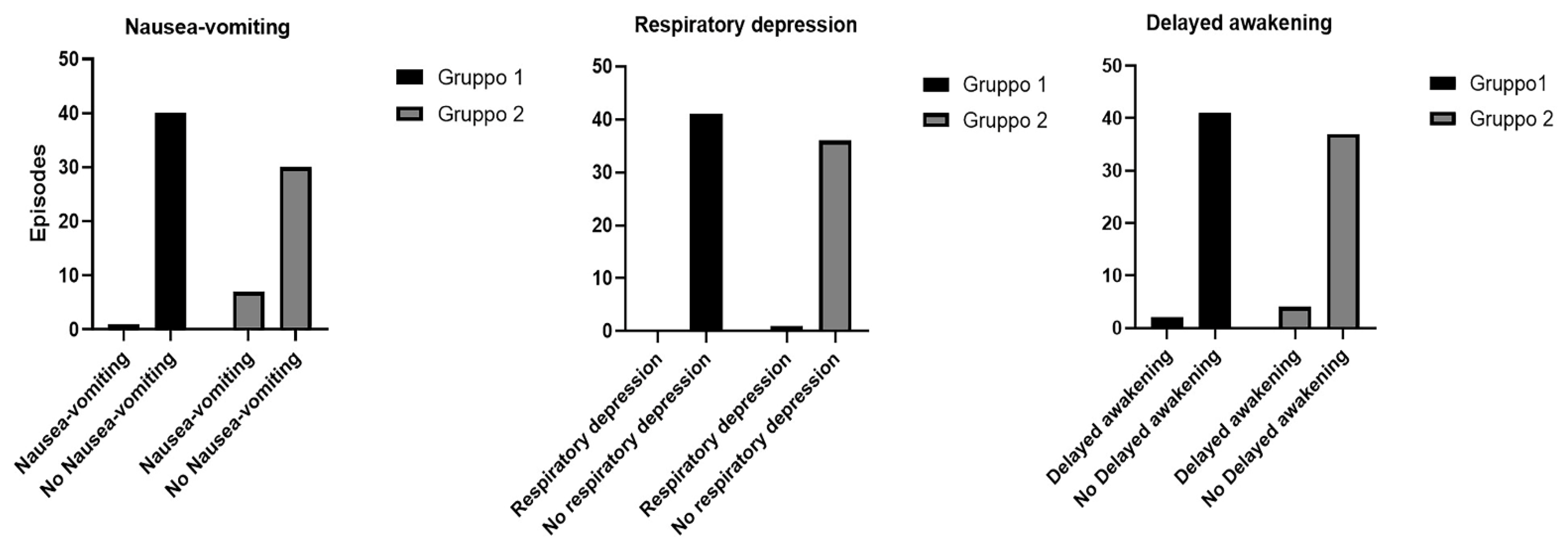
| Nausea-vomiting (episodes) | 1 | 7 |
| No Nausea-vomiting (episodes) | 40 | 30 |
| Respiratory depression (episodes) | 0 | 1 |
| No respiratory-depression (episodes) | 41 | 36 |
| Delayed awakening (episodes) | 2 | 4 |
| No Delayed awakening (episodes) | 41 | 37 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Torre, D.E.; Pirri, C.; Contristano, M.; Behr, A.U.; De Caro, R.; Stecco, C. Ultrasound-Guided PECS II + Serratus Plane Fascial Blocks Are Associated with Reduced Opioid Consumption and Lengths of Stay for Minimally Invasive Cardiac Surgery: An Observational Retrospective Study. Life 2022, 12, 805. https://doi.org/10.3390/life12060805
Torre DE, Pirri C, Contristano M, Behr AU, De Caro R, Stecco C. Ultrasound-Guided PECS II + Serratus Plane Fascial Blocks Are Associated with Reduced Opioid Consumption and Lengths of Stay for Minimally Invasive Cardiac Surgery: An Observational Retrospective Study. Life. 2022; 12(6):805. https://doi.org/10.3390/life12060805
Chicago/Turabian StyleTorre, Debora Emanuela, Carmelo Pirri, Marialuisa Contristano, Astrid Ursula Behr, Raffaele De Caro, and Carla Stecco. 2022. "Ultrasound-Guided PECS II + Serratus Plane Fascial Blocks Are Associated with Reduced Opioid Consumption and Lengths of Stay for Minimally Invasive Cardiac Surgery: An Observational Retrospective Study" Life 12, no. 6: 805. https://doi.org/10.3390/life12060805
APA StyleTorre, D. E., Pirri, C., Contristano, M., Behr, A. U., De Caro, R., & Stecco, C. (2022). Ultrasound-Guided PECS II + Serratus Plane Fascial Blocks Are Associated with Reduced Opioid Consumption and Lengths of Stay for Minimally Invasive Cardiac Surgery: An Observational Retrospective Study. Life, 12(6), 805. https://doi.org/10.3390/life12060805