
Effect of Different Physical Therapy Interventions on Brain-Derived Neurotrophic Factor Levels in Chronic Musculoskeletal Pain Patients: A Systematic Review

 ,
,  ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
Types of Studies
- ○
- PopulationAccording to these criteria, subjects with a chronic musculoskeletal pain condition were included and studies whose patients presented acute pain or neuropathic pain were excluded.
- ○
- InterventionThe treatment had to be a physiotherapy intervention (using physical agents), including education and any modality of exercise and manual therapy was included.
- ○
- ComparatorNo restrictions were placed on the comparator to analyze all the existing literature on the subject.
- ○
- Outcome measuresIn each study, the peripheral evaluation of BDNF concentration (serum or plasma) before and after physical therapy treatment was performed along with perceived levels of pain.
2.3. Study Selection
2.4. Data Extraction
2.5. Methodological Quality Assessment
3. Results
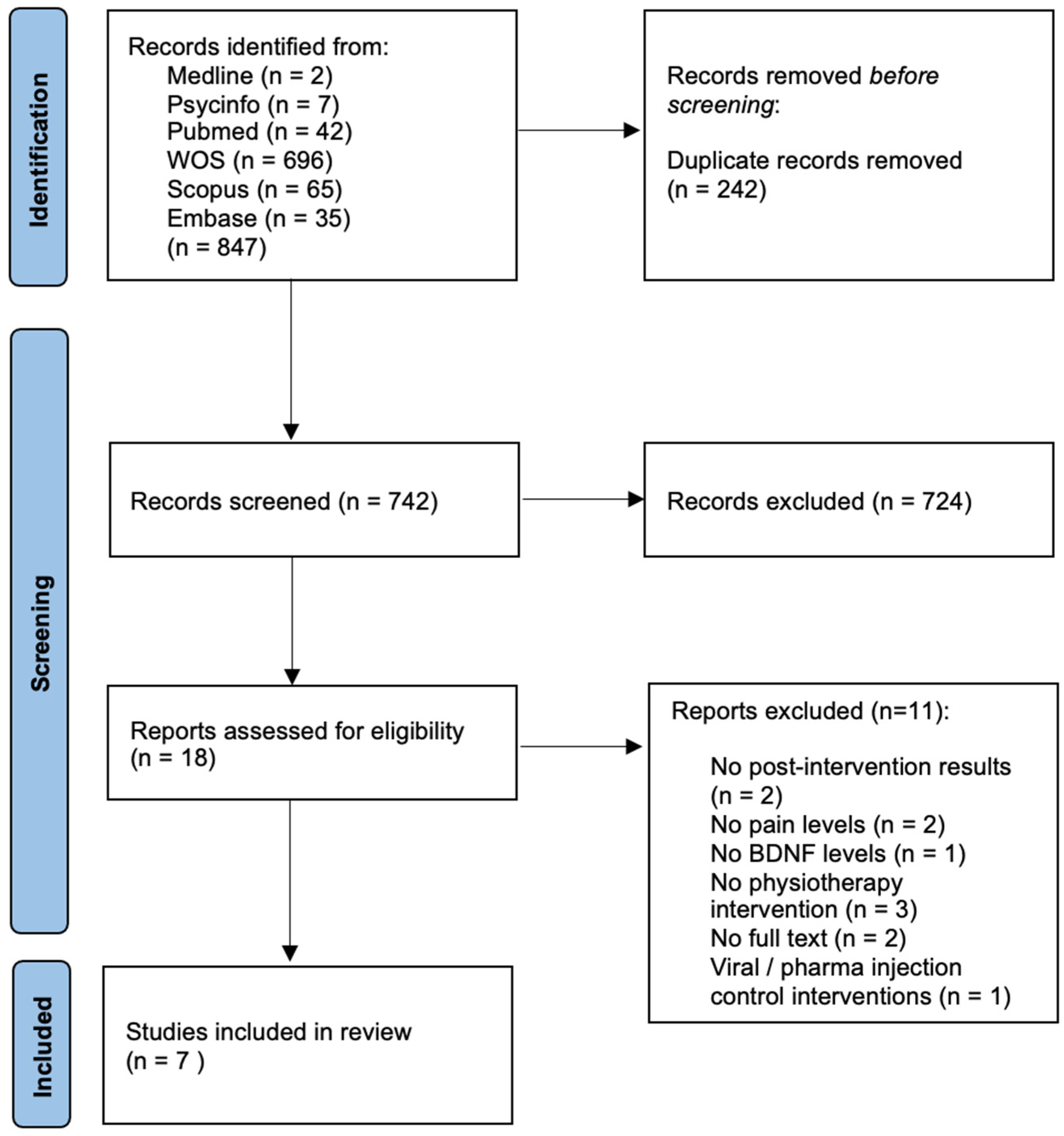
3.1. Literature Search
3.2. Description of Included Studies
3.3. Methodological Quality
3.4. Effects of Physiotherapy on BDNF Levels
3.4.1. Exercise
3.4.2. Electrotherapy
3.5. Effects of Physiotherapy on Pain Levels
3.5.1. Exercise
3.5.2. Electrotherapy
3.6. Relationship between Changes in BDNF Levels and Pain Severity
4. Discussion
4.1. Exercise Therapy
4.2. Non-Invasive Neuromodulation Techniques: rTMS&tDCS
4.2.1. rTMS
4.2.2. tDCS
5. Limitations
6. Implications for Research
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cohen, S.P.; Vase, L.; Hooten, W.M. Chronic pain: An update on burden, best practices, and new advances. Lancet 2021, 397, 2082–2097. [Google Scholar] [CrossRef] [PubMed]
- Sneddon, L.U. Comparative Physiology of Nociception and Pain. Physiology 2018, 33, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Woolf, C.J. Central sensitization: Implications for the diagnosis and treatment of pain. Pain 2011, 152, S2–S15. [Google Scholar] [CrossRef] [PubMed]
- Kuner, R.; Flor, H. Structural plasticity and reorganisation in chronic pain. Nat. Rev. Neurosci. 2016, 18, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Nijs, J.; Meeus, M.; Versijpt, J.; Moens, M.; Bos, I.; Knaepen, K.; Meeusen, R. Brain-derived neurotrophic factor as a driving force behind neuroplasticity in neuropathic and central sensitization pain: A new therapeutic target? Expert Opin. Ther. Targets 2014, 19, 565–576. [Google Scholar] [CrossRef]
- Obata, K.; Noguchi, K. BDNF in sensory neurons and chronic pain. Neurosci. Res. 2006, 55, 1–10. [Google Scholar] [CrossRef]
- Sikandar, S.; Minett, M.S.; Millet, Q.; Santana-Varela, S.; Lau, J.; Wood, J.N.; Zhao, J. Brain-Derived neurotrophic factor derived from sensory neurons plays a critical role in chronic pain. Brain 2018, 141, 1028–1039. [Google Scholar] [CrossRef]
- Siniscalco, D.; Giordano, C.; Rossi, F.; Maione, S.; De Novellis, V. Role of Neurotrophins in Neuropathic Pain. Curr. Neuropharmacol. 2011, 9, 523–529. [Google Scholar] [CrossRef]
- Kowiański, P.; Lietzau, G.; Czuba, E.; Waśkow, M.; Steliga, A.; Moryś, J. BDNF: A Key Factor with Multipotent Impact on Brain Signaling and Synaptic Plasticity. Cell. Mol. Neurobiol. 2018, 38, 579–593. [Google Scholar] [CrossRef]
- Cappoli, N.; Tabolacci, E.; Aceto, P.; Russo, C.D. The emerging role of the BDNF-TrkB signaling pathway in the modulation of pain perception. J. Neuroimmunol. 2020, 349, 577406. [Google Scholar] [CrossRef]
- Wang, Y.; Zhou, H.; Luo, Q.; Cui, S. The effect of physical exercise on circulating brain-derived neurotrophic factor in healthy subjects: A meta-analysis of randomized controlled trials. Brain Behav. 2022, 12, e2544. [Google Scholar] [CrossRef]
- da Graca-Tarragó, M.; Deitos, A.; Patrícia Brietzke, A.; Torres, I.L.; Cadore Stefani, L.; Fregni, F.; Caumo, W. Electrical Intramuscular Stimulation in Osteoarthritis Enhances the Inhibitory Systems in Pain Processing at Cortical and Cortical Spinal System. Pain Med. 2015, 17, 877–891. [Google Scholar] [CrossRef][Green Version]
- Zortea, M.; Ramalho, L.; Alves, R.L.; Alves, C.F.D.S.; Braulio, G.; Torres, I.L.; Fregni, F.; Caumo, W. Transcranial Direct Current Stimulation to Improve the Dysfunction of Descending Pain Modulatory System Related to Opioids in Chronic Non-cancer Pain: An Integrative Review of Neurobiology and Meta-Analysis. Front. Neurosci. 2019, 13, 1218. [Google Scholar] [CrossRef]
- Higgins, J.W.V.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M. Cochrane Handbook for Systematic Reviews of Interventions; Version 6.2.; John Wiley & Sons: New York, NY, USA, 2021. [Google Scholar]
- Page, M.J.; E McKenzie, J.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Moher, D. Updating guidance for reporting systematic reviews: Development of the PRISMA 2020 statement. J. Clin. Epidemiol. 2021, 134, 103–112. [Google Scholar] [CrossRef]
- Stone, P.W. Popping the (PICO) question in research and evidence-based practice. Appl. Nurs. Res. 2002, 15, 197–198. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro Scale for Rating Quality of Randomized Controlled Trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef]
- Moseley, A.M.; Herbert, R.; Sherrington, C.; Maher, C.G. Evidence for physiotherapy practice: A survey of the Physiotherapy Evidence Database (PEDro). Aust. J. Physiother. 2002, 48, 43–49. [Google Scholar] [CrossRef]
- Kappa, C.; Becker, G. Creating Comparability Among Reliability Coefficients: The Case O F Cronbach. Psychol. Reporfr O Psychol. Rep. 2000, 87, 1171–1182. [Google Scholar]
- Jablochkova, A.; Bäckryd, E.; Kosek, E.; Mannerkorpi, K.; Ernberg, M.; Gerdle, B.; Ghafouri, B. Unaltered low nerve growth factor and high brain-derived neurotrophic factor levels in plasma from patients with fibromyalgia after a 15-week progressive resistance exercise. J. Rehabil. Med. 2019, 51, 779–787. [Google Scholar] [CrossRef]
- McGrath, P.J.; Finley, G.A. Measurement of pain. Ann. Nestle 1999, 57, 13–20. [Google Scholar]
- Liu, J.; Chen, L.; Chen, X.; Hu, K.; Tu, Y.; Lin, M.; Huang, J.; Liu, W.; Wu, J.; Qiu, Z.; et al. Modulatory effects of different exercise modalities on the functional connectivity of the periaqueductal grey and ventral tegmental area in patients with knee osteoarthritis: A randomised multimodal magnetic resonance imaging study. Br. J. Anaesth. 2019, 123, 506–518. [Google Scholar] [CrossRef] [PubMed]
- Dall’Agnol, L.; Medeiros, L.F.; Torres, I.L.; Deitos, A.; Brietzke, A.; Laste, G.; de Souza, A.; Vieira, J.L.; Fregni, F.; Caumo, W. Repetitive Transcranial Magnetic Stimulation Increases the Corticospinal Inhibition and the Brain-Derived Neurotrophic Factor in Chronic Myofascial Pain Syndrome: An Explanatory Double-Blinded, Randomized, Sham-Controlled Trial. J. Pain 2014, 15, 845–855. [Google Scholar] [CrossRef] [PubMed]
- Botelho, L.; Angoleri, L.; Zortea, M.; Deitos, A.; Brietzke, A.; Torres, I.L.; Fregni, F.; Caumo, W. Insights About the Neuroplasticity State on the Effect of Intramuscular Electrical Stimulation in Pain and Disability Associated with Chronic Myofascial Pain Syndrome (MPS): A Double-Blind, Randomized, Sham-Controlled Trial. Front. Hum. Neurosci. 2018, 12, 388. [Google Scholar] [CrossRef] [PubMed]
- Santos, V.S.D.S.D.; Zortea, M.; Alves, R.L.; Naziazeno, C.C.D.S.; Saldanha, J.S.; Carvalho, S.D.C.R.D.; Leite, A.J.D.C.; Torres, I.L.D.S.; de Souza, A.; Calvetti, P.; et al. Cognitive effects of transcranial direct current stimulation combined with working memory training in fibromyalgia: A randomized clinical trial. Sci. Rep. 2018, 8, 12477. [Google Scholar] [CrossRef]
- Da Graca-Tarragó, M.; Lech, M.; Angoleri, L.D.M.; Santos, D.S.; Deitos, A.; Brietzke, A.P.; Caumo, W. Intramuscular electrical stimulus potentiates motor cortex modulation effects on pain and descending inhibitory systems in knee osteoarthritis: A randomized, factorial, sham-controlled study. J. Pain Res. 2019, 12, 209–221. [Google Scholar] [CrossRef]
- Medeiros, L.F.; Caumo, W.; Dussán-Sarria, J.; Deitos, A.; Brietzke, A.; Laste, G.; Campos-Carraro, C.; de Souza, A.; Scarabelot, V.L.; Cioato, S.G.; et al. Effect of Deep Intramuscular Stimulation and Transcranial Magnetic Stimulation on Neurophysiological Biomarkers in Chronic Myofascial Pain Syndrome. Pain Med. 2015, 17, 122–135. [Google Scholar] [CrossRef][Green Version]
- Kim, T.K. Practical statistics in pain research. Korean J. Pain 2017, 30, 243–249. [Google Scholar] [CrossRef]
- Lee, M.; Moon, W.; Kim, J. Effect of Yoga on Pain, Brain-Derived Neurotrophic Factor, and Serotonin in Premenopausal Women with Chronic Low Back Pain. Evid.-Based Complement. Altern. Med. 2014, 2014, 203173. [Google Scholar] [CrossRef]
- Nugraha, B.; Karst, M.; Engeli, S.; Gutenbrunner, C. Brain-derived neurotrophic factor and exercise in fibromyalgia syndrome patients: A mini review. Rheumatol. Int. 2011, 32, 2593–2599. [Google Scholar] [CrossRef]
- Xiong, G.L.; Doraiswamy, P.M. Does Meditation Enhance Cognition and Brain Plasticity? Ann. N. Y. Acad. Sci. 2009, 1172, 63–69. [Google Scholar] [CrossRef]
- Begliuomini, S.; Lenzi, E.; Ninni, F.; Casarosa, E.; Merlini, S.; Pluchino, N.; Valentino, V.; Luisi, S.; Luisi, M.; Genazzani, A.R. Plasma brain-derived neurotrophic factor daily variations in men: Correlation with cortisol circadian rhythm. J. Endocrinol. 2008, 197, 429–435. [Google Scholar] [CrossRef]
- Arbat-Plana, A.; Cobianchi, S.; Herrando-Grabulosa, M.; Navarro, X.; Udina, E. Endogenous modulation of TrkB signaling by treadmill exercise after peripheral nerve injury. Neuroscience 2017, 340, 188–200. [Google Scholar] [CrossRef]
- Risa, T.Y.; Ikemoto, H.; Okumo, T.; Sakhri, F.Z.; Horikawa, H.; Nakamura, A.; Sunagawa, M. Analgesic effect of voluntary exercise in a rat model of persistent pain via suppression of microglial activation in the spinal cord. Biomed. Res. 2021, 42, 67–76. [Google Scholar]
- Pedersen, B.K. Physical activity and muscle–brain crosstalk. Nat. Rev. Endocrinol. 2019, 15, 383–392. [Google Scholar] [CrossRef]
- Ziegenhorn, A.A.; Schulte-Herbrüggen, O.; Danker-Hopfe, H.; Malbranc, M.; Hartung, H.-D.; Anders, D.; Lang, U.E.; Steinhagen-Thiessen, E.; Schaub, R.T.; Hellweg, R. Serum neurotrophins—A study on the time course and influencing factors in a large old age sample. Neurobiol. Aging 2007, 28, 1436–1445. [Google Scholar] [CrossRef]
- Scharfman, H.E.; MacLusky, N.J. Estrogen and brain-derived neurotrophic factor (BDNF) in hippocampus: Complexity of steroid hormone-growth factor interactions in the adult CNS. Front. Neuroendocr. 2006, 27, 415–435. [Google Scholar] [CrossRef]
- Shimizu, E.; Hashimoto, K.; Okamura, N.; Koike, K.; Komatsu, N.; Kumakiri, C.; Nakazato, M.; Watanabe, H.; Shinoda, N.; Okada, S.; et al. Alterations of serum levels of brain-derived neurotrophic factor (BDNF) in depressed patients with or without antidepressants. Biol. Psychiatry 2003, 54, 70–75. [Google Scholar] [CrossRef]
- Alomari, M.A.; Khabour, O.F.; Alawneh, K.; Alzoubi, K.H.; Maikano, A.B. The importance of physical fitness for the relationship of BDNF with obesity measures in young normal-weight adults. Heliyon 2020, 6, e03490. [Google Scholar] [CrossRef]
- Edelmann, E.; Leßmann, V.; Brigadski, T. Pre- and postsynaptic twists in BDNF secretion and action in synaptic plasticity. Neuropharmacology 2014, 76, 610–627. [Google Scholar] [CrossRef]
- Cefis, M.; Quirié, A.; Pernet, N.; Marie, C.; Garnier, P.; Prigent-Tessier, A. Brain-derived neurotrophic factor is a full endothelium-derived factor in rats. Vasc. Pharmacol. 2020, 128–129, 106674. [Google Scholar] [CrossRef] [PubMed]
- Tamura, S.; Nagasawa, A.; Masuda, Y.; Tsunematsu, T.; Hayasaka, K.; Matsuno, K.; Shimizu, C.; Ozaki, Y.; Moriyama, T. BDNF, produced by a TPO-Stimulated megakaryocytic cell line, regulates autocrine proliferation. Biochem. Biophys. Res. Commun. 2012, 427, 542–546. [Google Scholar] [CrossRef] [PubMed]
- Liang, F.-Q.; Allen, G.; Earnest, D. Role of Brain-Derived Neurotrophic Factor in the Circadian Regulation of the Suprachiasmatic Pacemaker by Light. J. Neurosci. 2000, 20, 2978–2987. [Google Scholar] [CrossRef] [PubMed]
- Cubeddu, A.; Bucci, F.; Giannini, A.; Russo, M.; Daino, D.; Russo, N.; Merlini, S.; Pluchino, N.; Valentino, V.; Casarosa, E.; et al. Brain-derived neurotrophic factor plasma variation during the different phases of the menstrual cycle in women with premenstrual syndrome. Psychoneuroendocrinology 2011, 36, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Nofuji, Y.; Suwa, M.; Sasaki, H.; Ichimiya, A.; Nishichi, R.; Kumagai, S. Different circulating brain-derived neurotrophic factor responses to acute exercise between physically active and sedentary subjects. J. Sports Sci. Med. 2012, 11, 83–88. [Google Scholar]
- Stefani, L.C.; Torres, I.L.D.S.; de Souza, I.C.C.; Rozisky, J.R.; Fregni, F.; Caumo, W. BDNF as an effect modifier for gender effects on pain thresholds in healthy subjects. Neurosci. Lett. 2012, 514, 62–66. [Google Scholar] [CrossRef]
- Misailidou, V.; Malliou, P.; Beneka, A.; Karagiannidis, A.; Godolias, G. Assessment of patients with neck pain: A review of definitions, selection criteria, and measurement tools. J. Chiropr. Med. 2010, 9, 49–59. [Google Scholar] [CrossRef]
- Merighi, A.; Salio, C.; Ghirri, A.; Lossi, L.; Ferrini, F.; Betelli, C.; Bardoni, R. BDNF as a pain modulator. Prog. Neurobiol. 2008, 85, 297–317. [Google Scholar] [CrossRef]
- Van den Dool, J. Non-Invasive Interventions to Alter Maladaptive Neuroplasticity in the Complex Regional Pain Syndrome: A Systematic Review and a Pilot Study. 2012. Available online: studenttheses.uu.nl/handle/20.500.12932/9839 (accessed on 1 January 2023).
- Ding, X.; Liang, Y.-J.; Su, L.; Liao, F.-F.; Fang, D.; Tai, J.; Xing, G.-G. BDNF contributes to the neonatal incision-induced facilitation of spinal long-term potentiation and the exacerbation of incisional pain in adult rats. Neuropharmacology 2018, 137, 114–132. [Google Scholar] [CrossRef]
- Chen, W.; Walwyn, W.; Ennes, H.S.; Kim, H.; McRoberts, J.A.; Marvizón, J.C.G. BDNF released during neuropathic pain potentiates NMDA receptors in primary afferent terminals. Eur. J. Neurosci. 2014, 39, 1439–1454. [Google Scholar] [CrossRef]
- Porcher, C.; Hatchett, C.; Longbottom, R.E.; McAinch, K.; Sihra, T.S.; Moss, S.J.; Thomson, A.M.; Jovanovic, J.N. Positive Feedback Regulation between γ-Aminobutyric Acid Type A (GABAA) Receptor Signaling and Brain-derived Neurotrophic Factor (BDNF) Release in Developing Neurons. J. Biol. Chem. 2011, 286, 21667–21677. [Google Scholar] [CrossRef]


{kind=link}
| Author (Year) | Study Design | Diagnosis | Groups Characterization (Intervention: n, Age, % Females) | Intervention | Control | BDNF: Sample/Analysis Kit | BDNF Results | Pain Outcome | Pain Results |
|---|---|---|---|---|---|---|---|---|---|
| Dall’Agnol et al., 2014 [24] | RCT | CMPS | rTMS: n = 11, 45.83 (9.63), 100% Sham: n = 12, 44.83 (14.09), 100% | rTMS. Left motor cortex (M1). Trains: 16 series of 10 sec.pulse/high-frequency of 10 Hz biphasic magnetic stimulator 26 s rest. 1600 pulses per session. 10 sessions. | Sham Identical experience but without the impulses | Serum/ELISA | Not expose intra-group changes rTMS Increased BDNF vs. Sham | VAS | Higher pain score was correlated negatively with serum BDNF level [r-squared = 0.89, Beta= −0.15, SE = 0.008, (CI) 95% −0.17 to −0.13]. |
| Botelho et al., 2018 [25] | RCT | CMPS | EIMS n = 12 48.36 (10.97) 100% Sham n = 12 46.00 (13.55) 100% | EIMS Paraspinal region related to the nerve roots (the splenius capitis and semispinalis capitis). 20-min at at 2 Hz. 10 sessions | Sham The same device but the output jack plug was broken | Serum/ELISA | Intra-group: EIMS increased BDNF EIMS Increased BDNF vs. Sham | VAS | Increase in serum BDNF induced by the EIMS was correlated negatively with pain at the end of follow-up (Beta: 0.67 t = 2.24 p = 0,02 (CI) 95% = 0.07 to 1.26) |
| Dos Santos et al., 2018 [26] | RCT | FM | tDCS n = 20, 49.15 (8.43) 100% Sham n = 20 50.05 (11.19) 100% | tDCS with a cognitive training task. Anode over the left DLPFC, cathode at right supraorbital region. 2 mA for 20 min. The cognitive training: online app of a Dual N-Back task. 8 consecutive days. | Sham The stimulator was turned off after a ramp-up of 30 s of stimulation | Serum/ELISA | Does not expose the results | VAS | Does not expose the results |
| Da Graca-Tarragó et al., 2019 [27] | RCT | Knee OA | a-EIMS/A-TDCS n = 15 66 (9.08) 100% A-tDCS/s-EIMS n = 15 64.4 (9.82) 100% S-TDCS/a-EIMS n = 15 64.40 (6.02) 100% s-tDCS/S-EIMS n = 15 63.87 (7.07) 100% | a-tDCS Anodal in the contralateral primary motor cortex (M1), cathode in the contralateral supraorbital region. 2 mA, rumps 30 s, 0.057 mA/cm2, electrodes 35 cm 2.5 s, 30 min. a-EIMS Needles (40 mm × 0.25 mm + constant current 2 Hz, intensity adjusted to tolerability, location 12 L1-S2, vast medial, rectur femoris, vast lateral, anterior tibialis and pes anserine bursae, 5 s, 30 min. | Sham transcranial direct current stimulation (s-tDCS) The stimulator was turned off after a ramp-up of 30 s of stimulation Sham intramuscular electrical stimulation (s-EIMS) electrodes were placed on the sites where the needles were placed. No electrical stimulation passed to the patient | Serum/ELISA | Not expose intra-group changes No difference between groups neither at baseline nor at the treatment end | VAS, PPT | Serum BDNF levels at baseline were correlated negatively with the PPT at the end of the treatment All groups showed decreased pain scores over time The aTDCS/aEIMS produced higher reduction compared with all three groups |
| Medeiros et al., 2016 [28] | RCT | CMPS | a-rTMS/a-DIMST n = 11 49.18 (11.63) 100% a-rTMS/s-DIMST n = 12 45.83 (9.63) 100% s-rTMS/a-DIMST n = 12 47.25 (11.00) 100% s-rTMS/s-DIMST n = 11 46.73 (13.09) 100% | a-TMS Coil over the left primary motor cortex. 600 pulses at 10 Hz frequency 80% resting motor threshold (rMT) intensity. 10 sessions for 20 min each one. a-DIMST Needles (40 mm × 0.25 mm). Nerve roots C2-C3, C3-C4, and C4-C5. Distance from the spinous process line: 1.5 cm). 10 sessions for 20 min using a frequency of 2 Hz. | Sham repetitive transcranial magnetic stimulation (s-TMS) A sham coil was used Sham deep intramuscular stimulation therapy (s-DIMST) Used an electroacupuncture device where the electrical connection between the stimulator and the patient was broken at the output jack plug of the stimulator | Serum/ELISA | No changes in BDNF levels | VAS | All groups presented lower level of Pain VAS than sham-rTMS sham-DIMST. |
| RCT: randomized controlled trial; rTMS: Repetitive transcranial magnetic stimulation; EIMS: Intramuscular electrical stimulation; DIMST: deep intramuscular stimulation therapy; tDCS: transcranidirect current stimulation; ELISA: enzyme-linked immunosorbent assay; BDNF: Brain derived neurotrophic factor; VAS: Visual Analogic Scale; KOOS: Knee injury and Osteoarthritis Outcome Score; PPT: Pressure pain threshold; FM: Fibromyalgia; CMPS: Chronic Myofascial Pain Syndrome: OA: Osteoarthritis; DLPFC: Dorso lateral prefrontal cortex. | |||||||||
| Autor (year) | Study design | Diagnosis | Groups characterization (Intervention: n, age, % females) | Intervention | Control | BDNF: sample/analysis kit | BDNF Results | Pain outcome | Pain results |
| Liu et al., 2019 [22] | RCT | Knee OA | Exercise: (a) Tai Chi n = 35 58.61 (7.62) (b) Baduanjin n = 35 59.66 (7.36) (c) Stationary cycling n = 35 61.26 (7.53) Control n = 35 56.88 (6.51) | Exercise; Tai Chi, Baduanjin and Stationary cycling. 1 h 5/w for 12 w | Control: Basic health education 1 h, 1/w for 12 w | Serum/ELISA | Not expose intra-group changes No difference between groups | KOOS pain | Taichi, Baduanjin and cycling decreased pain (increased KOOS pain score) vs. control |
| Jablochkoba et al., 2019 [21] | RCT | FM | Resistance exercisen = 41 100% Relaxation therapy n = 34 100% | Resistance exercise Supervised: 10-min warm-up + 50 min. started with 40% MVC, developed up to 70–80%. 2/w for 15 w | Relaxation therapy: 25-min supervised mental exercises. 2/week. | Plasma/(ECLIA) | Intra-group: No changes in BDNF levels in FM (either in the exercise or in the relaxion group) No differences between groups (exercise vs. relaxion group) | VAS | No significant multivariate relationships were found between the changes in BDNF and pain in FM |
| RCT: randomized controlled trial; ECLIA: electrochemiluminescence assay panel; BDNF: Brain derived neurotrophic factor; VAS: Visual Analogic Scale; KOOS: Knee injury and Osteoarthritis Outcome Score; FM: Fibromyalgia; OA: Osteoarthritis. | |||||||||
| Evaluation Criteria | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Dall’Agnol et al., 2014 [24] | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 9 |
| Botelho et al., 2018 [25] | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 10 |
| Dos Santos et al., 2018 [26] | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 9 |
| Da Graca-Tarragó et al., 2019 [27] | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 10 |
| Medeiros et al., 2016 [28] | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 9 |
| Liu et al., 2019 [22] | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 5 |
| Jablochkoba et al., 2019 [21] | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 5 |
| Intervention | BDNF | Pain Intensity | |||||||
|---|---|---|---|---|---|---|---|---|---|
| SERUM | Plasma | VAS | |||||||
| Increase | Decrease | No Change | Increase | Decrease | No Change | Increase | Decrease | No Change | |
| Exercise | |||||||||
| Electro-therapy | |||||||||
| rTMS | |||||||||
| EIMS | |||||||||
| tDCS | |||||||||
| DIMST | |||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di-Bonaventura, S.; Fernández-Carnero, J.; Matesanz-García, L.; Arribas-Romano, A.; Polli, A.; Ferrer-Peña, R. Effect of Different Physical Therapy Interventions on Brain-Derived Neurotrophic Factor Levels in Chronic Musculoskeletal Pain Patients: A Systematic Review. Life 2023, 13, 163. https://doi.org/10.3390/life13010163
Di-Bonaventura S, Fernández-Carnero J, Matesanz-García L, Arribas-Romano A, Polli A, Ferrer-Peña R. Effect of Different Physical Therapy Interventions on Brain-Derived Neurotrophic Factor Levels in Chronic Musculoskeletal Pain Patients: A Systematic Review. Life. 2023; 13(1):163. https://doi.org/10.3390/life13010163
Chicago/Turabian StyleDi-Bonaventura, Silvia, Josué Fernández-Carnero, Luis Matesanz-García, Alberto Arribas-Romano, Andrea Polli, and Raúl Ferrer-Peña. 2023. "Effect of Different Physical Therapy Interventions on Brain-Derived Neurotrophic Factor Levels in Chronic Musculoskeletal Pain Patients: A Systematic Review" Life 13, no. 1: 163. https://doi.org/10.3390/life13010163
APA StyleDi-Bonaventura, S., Fernández-Carnero, J., Matesanz-García, L., Arribas-Romano, A., Polli, A., & Ferrer-Peña, R. (2023). Effect of Different Physical Therapy Interventions on Brain-Derived Neurotrophic Factor Levels in Chronic Musculoskeletal Pain Patients: A Systematic Review. Life, 13(1), 163. https://doi.org/10.3390/life13010163