
Melanoma Brain Metastases: A Systematic Review of Opportunities for Earlier Detection, Diagnosis, and Treatment

 , ,
, , 
Abstract
:1. Introduction
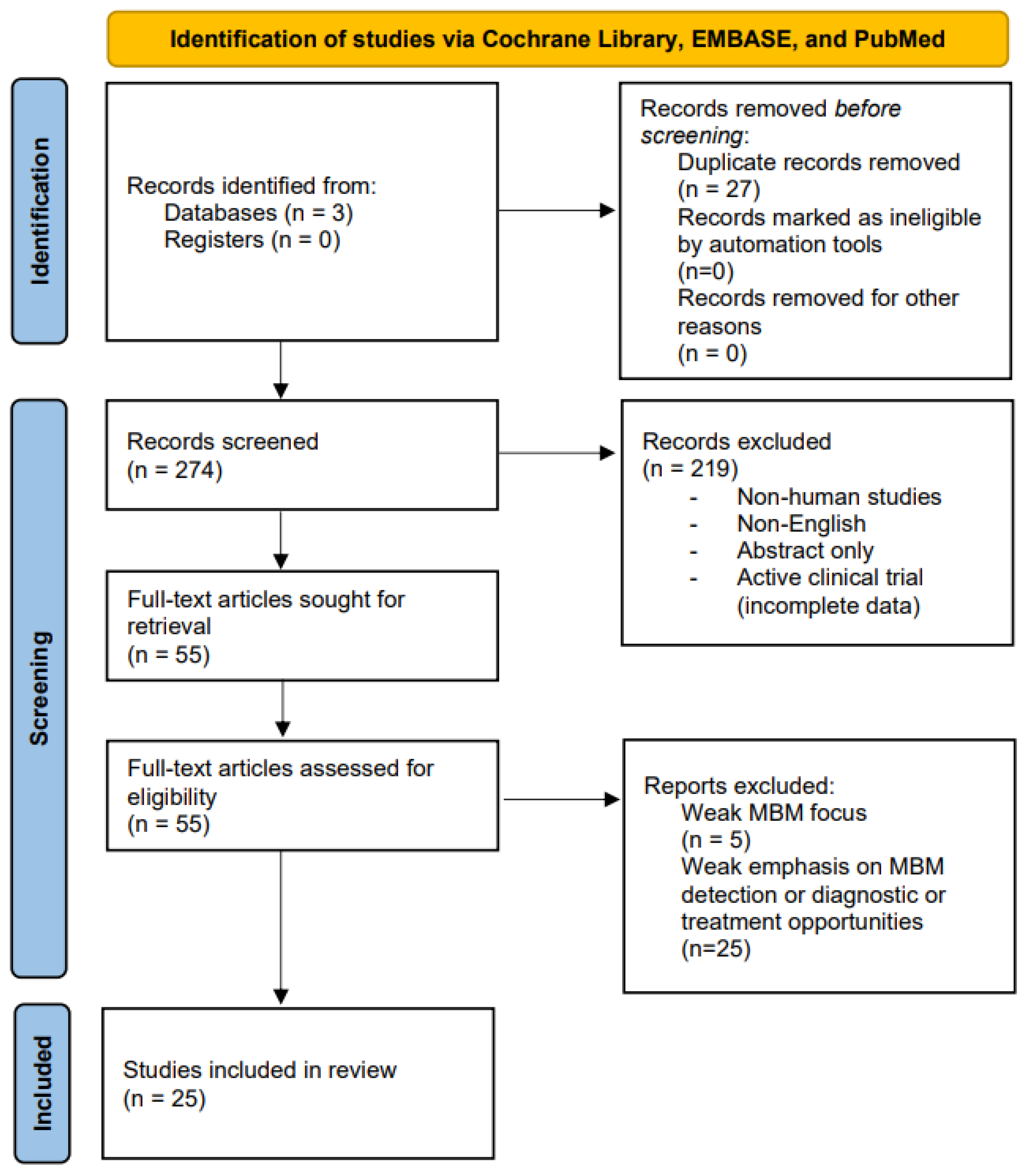
2. Methods
3. Results
3.1. Detection and Diagnosis of Melanoma Brain Metastases
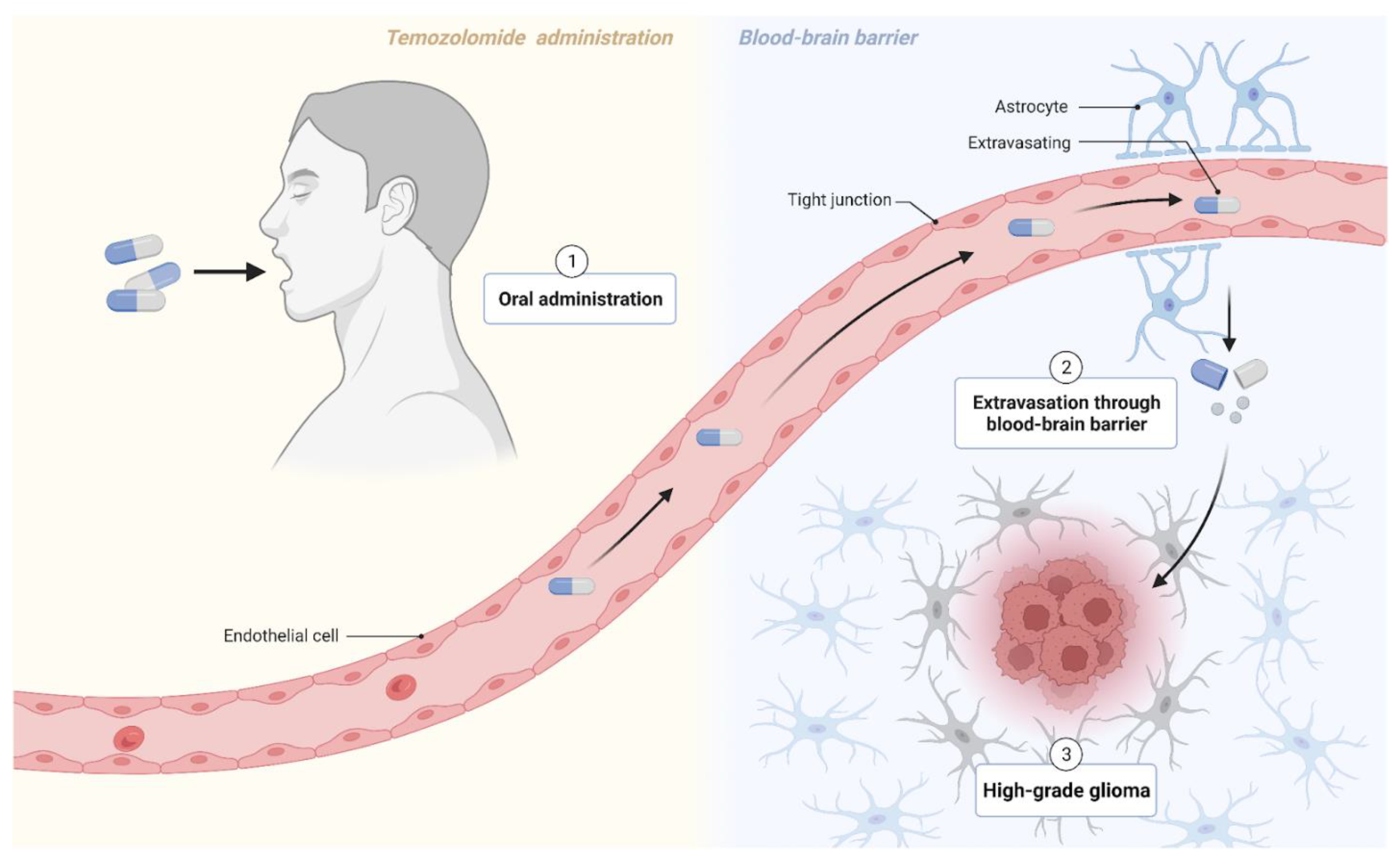
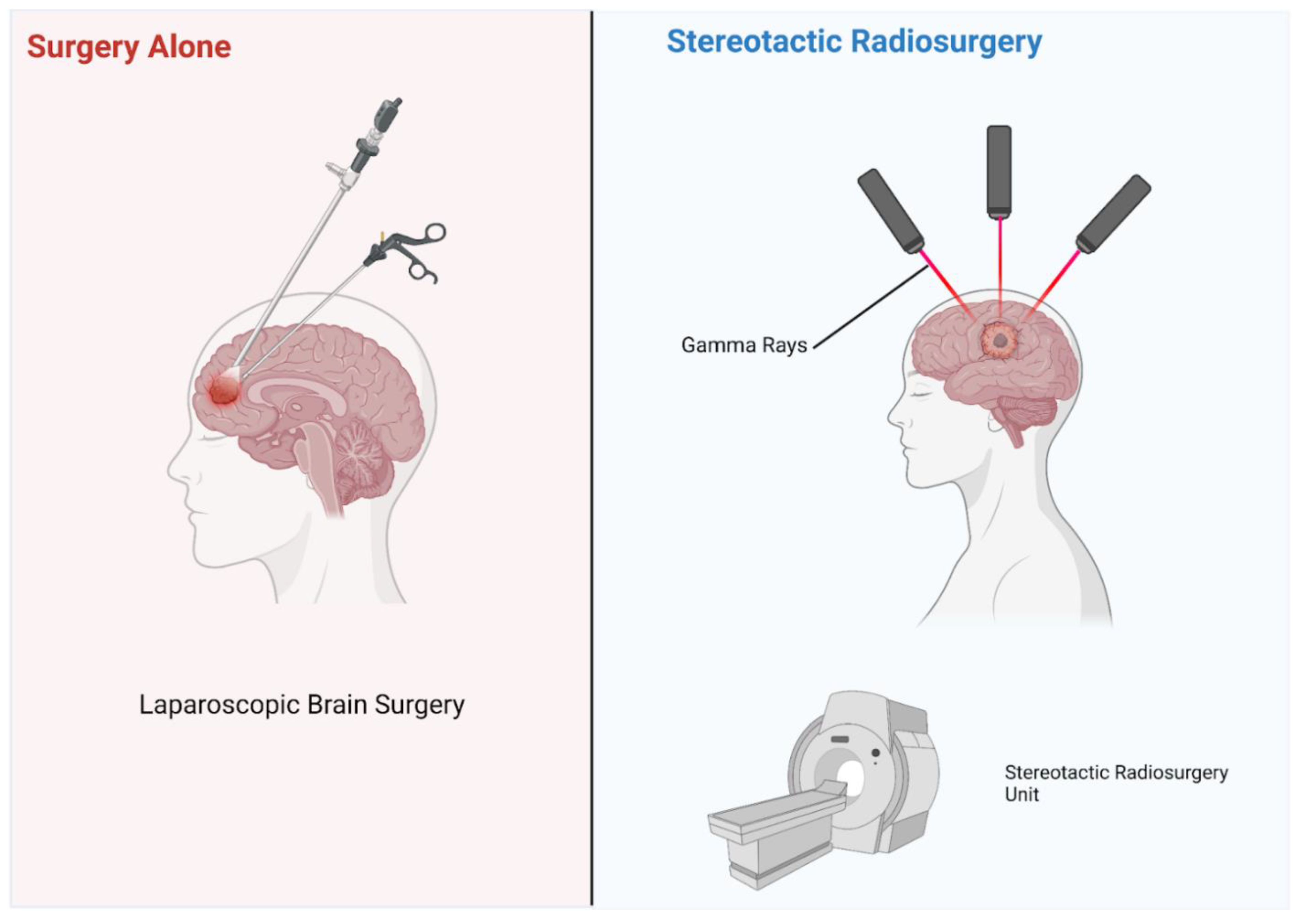
3.2. Treatment of Melanoma Brain Metastases
3.3. Emerging Clinical Evidence and Focus Areas
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Saginala, K.; Barsouk, A.; Aluru, J.S.; Rawla, P.; Barsouk, A. Epidemiology of Melanoma. Med. Sci. 2021, 9, 63. [Google Scholar] [CrossRef] [PubMed]
- Erdei, E.; Torres, S.M. A new understanding in the epidemiology of melanoma. Expert Rev. Anticancer Ther. 2010, 10, 1811–1823. [Google Scholar] [CrossRef] [Green Version]
- Bellenghi, M.; Puglisi, R.; Pontecorvi, G.; De Feo, A.; Carè, A.; Mattia, G. Sex and Gender Disparities in Melanoma. Cancers 2020, 12, 1819. [Google Scholar] [CrossRef]
- Eddy, K.; Shah, R.; Chen, S. Decoding Melanoma Development and Progression: Identification of Therapeutic Vulnerabilities. Front. Oncol. 2021, 10, 626129. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef]
- Damsky, J.W.E.; Rosenbaum, L.E.; Bosenberg, M. Decoding Melanoma Metastasis. Cancers 2010, 3, 126–163. [Google Scholar] [CrossRef] [PubMed]
- Ajithkumar, T.; Parkinson, C.; Fife, K.; Corrie, P.; Jefferies, S. Evolving treatment options for melanoma brain metastases. Lancet Oncol. 2015, 16, e486–e497. [Google Scholar] [CrossRef] [PubMed]
- Oliva, I.G.; Tawbi, H.; Davies, M.A. Melanoma Brain Metastases: Current Areas of Investigation and Future Directions. Cancer J. 2017, 23, 68–74. [Google Scholar] [CrossRef] [Green Version]
- Davies, M.A.; Liu, P.; McIntyre, S.; Kim, K.B.; Papadopoulos, N.; Hwu, W.-J.; Hwu, P.; Bedikian, A. Prognostic factors for survival in melanoma patients with brain metastases. Cancer 2011, 117, 1687–1696. [Google Scholar] [CrossRef]
- Vosoughi, E.; Lee, J.M.; Miller, J.R.; Nosrati, M.; Minor, D.R.; Abendroth, R.; Lee, J.W.; Andrews, B.T.; Leng, L.Z.; Wu, M.; et al. Survival and clinical outcomes of patients with melanoma brain metastasis in the era of checkpoint inhibitors and targeted therapies. BMC Cancer 2018, 18, 490. [Google Scholar] [CrossRef] [PubMed]
- Middleton, M.; Grob, J.-J.; Aaronson, N.; Fierlbeck, G.; Tilgen, W.; Seiter, S.; Gore, M.; Aamdal, S.; Cebon, J.; Coates, A.; et al. Randomized phase III study of temozolomide versus dacarbazine in the treatment of patients with advanced metastatic malignant melanoma. J. Clin. Oncol. 2000, 18, 158–166. [Google Scholar] [CrossRef] [PubMed]
- Rieth, J.; Swami, U.; Mott, S.; Zanaty, M.; Henry, M.; Bossler, A.; Greenlee, J.; Zakharia, Y.; Vanneste, M.; Jennings, B.; et al. Melanoma Brain Metastases in the Era of Targeted Therapy and Checkpoint Inhibitor Therapy. Cancers 2021, 13, 1489. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ (Clin. Res. Ed.) 2021, 372, n71. [Google Scholar] [CrossRef]
- Hauswald, H.; Habl, G.; Krug, D.; Kehle, D.; Combs, S.; Bermejo, J.L.; Debus, J.; Sterzing, F. Whole brain helical Tomotherapy with integrated boost for brain metastases in patients with malignant melanoma–a randomized trial. Radiat. Oncol. 2013, 8, 234. [Google Scholar] [CrossRef] [Green Version]
- Samlowski, W.E.; Moon, J.; Witter, M.; Atkins, M.B.; Kirkwood, J.M.; Othus, M.; Ribas, A.; Sondak, V.K.; Flaherty, L.E. High frequency of brain metastases after adjuvant therapy for high-risk melanoma. Cancer Med. 2017, 6, 2576–2585. [Google Scholar] [CrossRef] [PubMed]
- Fuentes, R.; Osorio, D.; Hernandez, J.E.; Simancas-Racines, D.; Martinez-Zapata, M.J.; Cosp, X.B. Surgery versus stereotactic radiotherapy for people with single or solitary brain metastasis. Cochrane Database Syst. Rev. 2018, 2018, CD012086. [Google Scholar] [CrossRef]
- Syeda, M.M.; Wiggins, J.M.; Corless, B.C.; Long, G.V.; Flaherty, K.T.; Schadendorf, D.; Nathan, P.D.; Robert, C.; Ribas, A.; Davies, M.A.; et al. Circulating tumour DNA in patients with advanced melanoma treated with dabrafenib or dabrafenib plus trametinib: A clinical validation study. Lancet Oncol. 2021, 22, 370–380. [Google Scholar] [CrossRef]
- Long, G.V.; Grob, J.-J.; Nathan, P.; Ribas, A.; Robert, C.; Schadendorf, D.; Lane, S.R.; Mak, C.; Legenne, P.; Flaherty, K.T.; et al. Factors predictive of response, disease progression, and overall survival after dabrafenib and trametinib combination treatment: A pooled analysis of individual patient data from randomised trials. Lancet Oncol. 2016, 17, 1743–1754. [Google Scholar] [CrossRef]
- Azam, F.; Latif, M.F.; Farooq, A.; Tirmazy, S.H.; AlShahrani, S.; Bashir, S.; Bukhari, N. Performance Status Assessment by Using ECOG (Eastern Cooperative Oncology Group) Score for Cancer Patients by Oncology Healthcare Professionals. Case Rep. Oncol. 2019, 12, 728–736. [Google Scholar] [CrossRef]
- Hess, L.M.; Brnabic, A.; Mason, O.; Lee, P.; Barker, S. Relationship between Progression-free Survival and Overall Survival in Randomized Clinical Trials of Targeted and Biologic Agents in Oncology. J. Cancer 2019, 10, 3717–3727. [Google Scholar] [CrossRef] [Green Version]
- Dutriaux, C.; Robert, C.; Grob, J.-J.; Mortier, L.; Dereure, O.; Lebbe, C.; Mansard, S.; Grange, F.; Neidhardt, E.-M.; Lesimple, T.; et al. An open label, non-randomised, phase IIIb study of trametinib in combination with dabrafenib in patients with unresectable (stage III) or distant metastatic (stage IV) BRAF V600-mutant melanoma: A subgroup analysis of patients with brain metastases. Eur. J. Cancer 2022, 175, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Krepler, C.; Sproesser, K.; Brafford, P.; Beqiri, M.; Garman, B.; Xiao, M.; Shannan, B.; Watters, A.; Perego, M.; Zhang, G.; et al. A Comprehensive Patient-Derived Xenograft Collection Representing the Heterogeneity of Melanoma. Cell Rep. 2017, 21, 1953–1967. [Google Scholar] [CrossRef] [Green Version]
- Petralia, G.; Padhani, A.; Summers, P.; Alessi, S.; Raimondi, S.; Testori, A.; Bellomi, M. Whole-body diffusion-weighted imaging: Is it all we need for detecting metastases in melanoma patients? Eur. Radiol. 2013, 23, 3466–3476. [Google Scholar] [CrossRef] [PubMed]
- Fogarty, G.; Morton, R.L.; Vardy, J.; Nowak, A.K.; Mandel, C.; Forder, P.M.; Hong, A.; Hruby, G.; Burmeister, B.; Shivalingam, B.; et al. Whole brain radiotherapy after local treatment of brain metastases in melanoma patients—A randomised phase III trial. BMC Cancer 2011, 11, 142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pasquali, S.; Hadjinicolaou, A.V.; Sileni, V.C.; Rossi, C.R.; Mocellin, S. Systemic treatments for metastatic cutaneous melanoma. Cochrane Database Syst. Rev. 2018, 2, CD011123. [Google Scholar] [CrossRef] [PubMed]
- Richtig, E.; Hofmann-Wellenhof, R.; Pehamberger, H.; Forstinger, C.; Wolff, K.; Mischer, P.; Raml, J.; Fritsch, P.; Zelger, B.; Ratzinger, G.; et al. Temozolomide and interferon alpha2b in metastatic melanoma stage IV. Br. J. Dermatol. 2004, 151, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Amaravadi, R.K.; Schuchter, L.M.; McDermott, D.F.; Kramer, A.; Giles, L.; Gramlich, K.; Carberry, M.; Troxel, A.B.; Letrero, R.; Nathanson, K.L.; et al. Phase II Trial of Temozolomide and Sorafenib in Advanced Melanoma Patients with or without Brain Metastases. Clin. Cancer Res. 2009, 15, 7711–7718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiarion-Sileni, V.; Guida, M.; Ridolfi, L.; Romanini, A.; Del Bianco, P.; Pigozzo, J.; Brugnara, S.; Colucci, G.; Ridolfi, R.; De Salvo, G.L. Central nervous system failure in melanoma patients: Results of a randomised, multicentre phase 3 study of temozolomide- and dacarbazine- based regimens. Br. J. Cancer 2011, 104, 1816–1821. [Google Scholar] [CrossRef] [Green Version]
- Gritsch, D.M.; Mrugala, M.M.M.; Marks, L.A.M.; Wingerchuk, D.M.M.; O’Carroll, C.B.M. In Patients With Melanoma Brain Metastases, Is Combination Immune Checkpoint Inhibition a Safe and Effective First-Line Treatment? A Critically Appraised Topic. Neurologist 2022, 27, 290–297. [Google Scholar] [CrossRef]
- Guo, T.; Chu, L.; Chu, X.; Yang, X.; Li, Y.; Zhou, Y.; Xu, D.; Zhang, J.; Wang, S.; Hu, J.; et al. Brain metastases, patterns of intracranial progression, and the clinical value of upfront cranial radiotherapy in patients with metastatic non-small cell lung cancer treated with PD-1/PD-L1 inhibitors. Transl. Lung Cancer Res. 2022, 11, 173–187. [Google Scholar] [CrossRef]
- Bedikian, A.Y.; Richards, J.; Kharkevitch, D.; Atkins, M.B.; Whitman, E.; Gonzalez, R. A phase 2 study of high-dose Allovectin-7 in patients with advanced metastatic melanoma. Melanoma Res. 2010, 20, 218–226. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Wu, X.; Chen, P.; Pei, Y.; Zheng, K.; Wang, W.; Qiu, E.; Zhang, X. Interferon-α versus interleukin-2 in Chinese patients with malignant melanoma: A randomized, controlled, trial. Anti-Cancer Drugs 2019, 30, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Hong, A.M.; Fogarty, G.B.; Dolven-Jacobsen, K.; Burmeister, B.H.; Lo, S.N.; Haydu, L.E.; Vardy, J.L.; Nowak, A.; Dhillon, H.M.; Ahmed, T.; et al. Adjuvant Whole-Brain Radiation Therapy Compared With Observation After Local Treatment of Melanoma Brain Metastases: A Multicenter, Randomized Phase III Trial. J. Clin. Oncol. 2019, 37, 3132–3141. [Google Scholar] [CrossRef] [PubMed]
- Tsao, M.N.; Xu, W.; Wong, R.K.; Lloyd, N.; Laperriere, N.; Sahgal, A.; Rakovitch, E.; Chow, E. Whole brain radiotherapy for the treatment of newly diagnosed multiple brain metastases. Cochrane Database Syst. Rev. 2018, 1, CD003869. [Google Scholar] [CrossRef]
- Martinage, G.; Hong, A.M.; Fay, M.; Thachil, T.; Roos, D.; Williams, N.; Lo, S.; Fogarty, G. Quality assurance analysis of hippocampal avoidance in a melanoma whole brain radiotherapy randomized trial shows good compliance. Radiat. Oncol. 2018, 13, 132. [Google Scholar] [CrossRef] [Green Version]
- Fogarty, G.B.; Hong, A.; Dolven-Jacobsen, K.; Reisse, C.H.; Burmeister, B.; Haydu, L.H.; Dhillon, H.; Steel, V.; Shivalingam, B.; Drummond, K.; et al. First interim analysis of a randomised trial of whole brain radiotherapy in melanoma brain metastases confirms high data quality. BMC Res. Notes 2015, 8, 192. [Google Scholar] [CrossRef] [Green Version]
- Janavicius, M.; Lachej, N.; Anglickiene, G.; Vincerzevskiene, I.; Brasiuniene, B. Outcomes of Treatment for Melanoma Brain Metastases. J. Ski. Cancer 2020, 2020, 7520924. [Google Scholar] [CrossRef]
- Kirkpatrick, J.P.; Wang, Z.; Sampson, J.H.; McSherry, F.; Herndon, J.E.; Allen, K.J.; Duffy, E.; Hoang, J.K.; Chang, Z.; Yoo, D.S.; et al. Defining the optimal planning target volume in image-guided stereotactic radiosurgery of brain metastases: Results of a randomized trial. Int. J. Radiat. Oncol. 2015, 91, 100–108. [Google Scholar] [CrossRef]
- Tétu, P.; Allayous, C.; Oriano, B.; Dalle, S.; Mortier, L.; Leccia, M.; Guillot, B.; Dalac, S.; Dutriaux, C.; Lacour, J.-P.; et al. Impact of radiotherapy administered simultaneously with systemic treatment in patients with melanoma brain metastases within MelBase, a French multicentric prospective cohort. Eur. J. Cancer 2019, 112, 38–46. [Google Scholar] [CrossRef]
- Long, G.V.; Atkinson, V.; Lo, S.; Sandhu, S.; Guminski, A.D.; Brown, M.P.; Wilmott, J.S.; Edwards, J.; Gonzalez, M.; Scolyer, R.A.; et al. Combination nivolumab and ipilimumab or nivolumab alone in melanoma brain metastases: A multicentre randomised phase 2 study. Lancet Oncol. 2018, 19, 672–681. [Google Scholar] [CrossRef]
- Di Giacomo, A.M.; Chiarion-Sileni, V.; Del Vecchio, M.; Ferrucci, P.F.; Guida, M.; Quaglino, P.; Guidoboni, M.; Marchetti, P.; Cutaia, O.; Amato, G.; et al. Primary Analysis and 4-Year Follow-Up of the Phase III NIBIT-M2 Trial in Melanoma Patients with Brain Metastases. J. Clin. Oncol. 2021, 27, 4737–4745. [Google Scholar] [CrossRef] [PubMed]
- Larkin, J.; Weber, J.; Del Vecchio, M.; Gogas, H.; Arance, A.M.; Dalle, S.; Cowey, C.L.; Schenker, M.; Grob, J.-J.; Chiarion-Sileni, V.; et al. Adjuvant nivolumab versus ipilimumab (CheckMate 238 trial): Reassessment of 4-year efficacy outcomes in patients with stage III melanoma per AJCC-8 staging criteria. Eur. J. Cancer 2022, 173, 285–296. [Google Scholar] [CrossRef] [PubMed]
- Tjulandin, S.; Demidov, L.; Moiseyenko, V.; Protsenko, S.; Semiglazova, T.; Odintsova, S.; Zukov, R.; Lazarev, S.; Makarova, Y.; Nechaeva, M.; et al. Novel PD-1 inhibitor prolgolimab: Expanding non-resectable/metastatic melanoma therapy choice. Eur. J. Cancer 2021, 149, 222–232. [Google Scholar] [CrossRef] [PubMed]
- Eggermont, A.M.; Meshcheryakov, A.; Atkinson, V.; Blank, C.U.; Mandala, M.; Long, G.V.; Barrow, C.; Di Giacomo, A.M.; Fisher, R.; Sandhu, S.; et al. Crossover and rechallenge with pembrolizumab in recurrent patients from the EORTC 1325-MG/Keynote-054 phase III trial, pembrolizumab versus placebo after complete resection of high-risk stage III melanoma. Eur. J. Cancer 2021, 158, 156–168. [Google Scholar] [CrossRef] [PubMed]
- Tran, A.D.; Fogarty, G.; Nowak, A.K.; Diaby, V.; Hong, A.; Watts, C.; Morton, R.L. Cost-Effectiveness of Subsequent Whole-Brain Radiotherapy or Hippocampal-Avoidant Whole-Brain Radiotherapy Versus Stereotactic Radiosurgery or Surgery Alone for Treatment of Melanoma Brain Metastases. Appl. Health Econ. Health Policy 2020, 18, 679–687. [Google Scholar] [CrossRef]
- Caulfield, J.I.; Kluger, H.M. Emerging Studies of Melanoma Brain Metastasis. Curr. Oncol. Rep. 2022, 24, 585–594. [Google Scholar] [CrossRef]
- Larkin, J.R.; Dickens, A.M.; Claridge, T.D.W.; Bristow, C.; Andreou, K.; Anthony, D.C.; Sibson, N.R. Early Diagnosis of Brain Metastases Using a Biofluids-Metabolomics Approach in Mice. Theranostics 2016, 6, 2161–2169. [Google Scholar] [CrossRef] [Green Version]
- Babiker, H.M.; Byron, S.A.; Hendricks, W.P.D.; Elmquist, W.F.; Gampa, G.; Vondrak, J.; Aldrich, J.; Cuyugan, L.; Adkins, J.; De Luca, V.; et al. E6201, an intravenous MEK1 inhibitor, achieves an exceptional response in BRAF V600E-mutated metastatic malignant melanoma with brain metastases. Investig. New Drugs 2019, 37, 636–645. [Google Scholar] [CrossRef] [PubMed]
- Richtig, G.; Aigelsreiter, A.; Kashofer, K.; Talakic, E.; Kupsa, R.; Schaider, H.; Richtig, E. Two case reports of rare BRAF mutations in exon 11 and exon 15 with discussion of potential treatment options. Case Rep. Oncol. 2016, 9, 543–546. [Google Scholar] [CrossRef]
- Franklin, C.; Mohr, P.; Bluhm, L.; Grimmelmann, I.; Gutzmer, R.; Meier, F.; Garzarolli, M.; Weichenthal, M.; Pfoehler, C.; Herbst, R.; et al. Impact of radiotherapy and sequencing of systemic therapy on survival outcomes in melanoma patients with previously untreated brain metastasis: A multicenter DeCOG study on 450 patients from the prospective skin cancer registry ADOREG. J. Immunother. Cancer 2022, 10, e004509. [Google Scholar] [CrossRef]
- In, G.K.; Poorman, K.; Saul, M.; O’Day, S.; Farma, J.M.; Olszanski, A.J.; Gordon, M.S.; Thomas, J.S.; Eisenberg, B.; Flaherty, L.; et al. Molecular profiling of melanoma brain metastases compared to primary cutaneous melanoma and to extracranial metastases. Oncotarget 2020, 11, 3118–3128. [Google Scholar] [CrossRef] [PubMed]
- Derks, S.; de Joode, K.; Mulder, E.; Ho, L.; Joosse, A.; de Jonge, M.; Verhoef, C.; Grünhagen, D.; Smits, M.; Bent, M.V.D.; et al. The meaning of screening: Detection of brain metastasis in the adjuvant setting for stage III melanoma. ESMO Open 2022, 7, 100600. [Google Scholar] [CrossRef]
- Tan, X.-L.; Le, A.; Tang, H.; Brown, M.; Scherrer, E.; Han, J.; Jiang, R.; Diede, S.J.; Shui, I.M. Burden and Risk Factors of Brain Metastases in Melanoma: A Systematic Literature Review. Cancers 2022, 14, 6108. [Google Scholar] [CrossRef]
- Jablonska, P.A.; Fong, C.H.; Kruser, T.; Weiss, J.; Liu, Z.A.; Takami, H.; Narita, Y.; de Moraes, F.Y.; Dasgupta, A.; Ong, C.K.; et al. Recommended first-line management of brain metastases from melanoma: A multicenter survey of clinical practice. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2022, 168, 89–94. [Google Scholar] [CrossRef] [PubMed]
- van Opijnen, M.P.; Dirven, L.; Coremans, I.E.; Taphoorn, M.J.; Kapiteijn, E.H. The impact of current treatment modalities on the outcomes of patients with melanoma brain metastases: A systematic review. Int. J. Cancer 2019, 146, 1479–1489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tawbi, H.A.; Boutros, C.; Kok, D.; Robert, C.; McArthur, G. New Era in the Management of Melanoma Brain Metastases. Am. Soc. Clin. Oncol. Educ. Book 2018, 38, 741–750. [Google Scholar] [CrossRef]
- Long, G.V.; Stroyakovskiy, D.; Gogas, H.; Levchenko, E.; de Braud, F.; Larkin, J.; Garbe, C.; Jouary, T.; Hauschild, A.; Grob, J.-J.; et al. Dabrafenib and trametinib versus dabrafenib and placebo for Val600 BRAF-mutant melanoma: A multicentre, double-blind, phase 3 randomised controlled trial. Lancet 2015, 386, 444–451. [Google Scholar] [CrossRef]
- Hodi, F.S.; O’Day, S.J.; McDermott, D.F.; Weber, R.W.; Sosman, J.A.; Haanen, J.B.; Gonzalez, R.; Robert, C.; Schadendorf, D.; Hassel, J.C.; et al. Improved survival with ipilimumab in patients with metastatic melanoma. N. Engl. J. Med. 2010, 363, 711–723. [Google Scholar] [CrossRef]
- Wolchok, J.D.; Kluger, H.; Callahan, M.K.; Postow, M.A.; Rizvi, N.A.; Lesokhin, A.M.; Segal, N.H.; Ariyan, C.E.; Gordon, R.-A.; Reed, K.; et al. Nivolumab plus ipilimumab in advanced melanoma. N. Engl. J. Med. 2013, 369, 122–133. [Google Scholar] [CrossRef] [Green Version]
- Tumeh, P.C.; Harview, C.L.; Yearley, J.H.; Shintaku, I.P.; Taylor, E.J.M.; Robert, L.; Chmielowski, B.; Spasic, M.; Henry, G.; Ciobanu, V.; et al. PD-1 blockade induces responses by inhibiting adaptive immune resistance. Nature 2014, 515, 568–571. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Liu, S.; Yang, Z.; Algazi, A.P.; Lomeli, S.H.; Wang, Y.; Othus, M.; Hong, A.; Wang, X.; Randolph, C.E.; et al. Anti-PD-1/L1 lead-in before MAPK inhibitor combination maximizes antitumor immunity and efficacy. Cancer Cell 2021, 39, 1375–1387.e6. [Google Scholar] [CrossRef]
- Huynh, S.; Mortier, L.; Dutriaux, C.; Maubec, E.; Boileau, M.; Dereure, O.; Leccia, M.-T.; Arnault, J.P.; Brunet-Possenti, F.; Aubin, F.; et al. Combined Therapy with Anti-PD1 and BRAF and/or MEK Inhibitor for Advanced Melanoma: A Multicenter Cohort Study. Cancers 2020, 12, 1666. [Google Scholar] [CrossRef] [PubMed]
- Lau, P.K.H.; Feran, B.; Smith, L.; Lasocki, A.; Molania, R.; Smith, K.; Weppler, A.; Angel, C.; Kee, D.; Bhave, P.; et al. Melanoma brain metastases that progress on BRAF-MEK inhibitors demonstrate resistance to ipilimumab-nivolumab that is associated with the Innate PD-1 Resistance Signature (IPRES). J. Immunother. Cancer 2021, 9, e002995. [Google Scholar] [CrossRef] [PubMed]
- Amaral, T.; Kiecker, F.; Schaefer, S.; Stege, H.; Kaehler, K.; Terheyden, P.; Gesierich, A.; Gutzmer, R.; Haferkamp, S.; Uttikal, J.; et al. Combined immunotherapy with nivolumab and ipilimumab with and without local therapy in patients with melanoma brain metastasis: A DeCOG* study in 380 patients. J. Immunother. Cancer 2020, 8, e000333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amaral, T.; Niessner, H.; Sinnberg, T.; Thomas, I.; Meiwes, A.; Garbe, C.; Garzarolli, M.; Rauschenberg, R.; Eigentler, T.; Meier, F. An open-label, single-arm, phase II trial of buparlisib in patients with melanoma brain metastases not eligible for surgery or radiosurgery—The BUMPER study. Neuro-Oncol. Adv. 2020, 2, vdaa140. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Factors Associated with Lower PFS | Factors Associated with Increased PFS |
|---|---|
| ECOG ≳ 1 | ECOG = 0 |
| Elevated Serum LDH | LDH < ULN |
| ≳3 Sites of Metastasis | <3 Sites of Metastasis |
| Non-Naïve Status | No Prior Treatment |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Diaz, M.J.; Mark, I.; Rodriguez, D.; Gelman, B.; Tran, J.T.; Kleinberg, G.; Levin, A.; Beneke, A.; Root, K.T.; Tran, A.X.V.; et al. Melanoma Brain Metastases: A Systematic Review of Opportunities for Earlier Detection, Diagnosis, and Treatment. Life 2023, 13, 828. https://doi.org/10.3390/life13030828
Diaz MJ, Mark I, Rodriguez D, Gelman B, Tran JT, Kleinberg G, Levin A, Beneke A, Root KT, Tran AXV, et al. Melanoma Brain Metastases: A Systematic Review of Opportunities for Earlier Detection, Diagnosis, and Treatment. Life. 2023; 13(3):828. https://doi.org/10.3390/life13030828
Chicago/Turabian StyleDiaz, Michael Joseph, Isabella Mark, Daphnee Rodriguez, Beata Gelman, Jasmine Thuy Tran, Giona Kleinberg, Anna Levin, Alice Beneke, Kevin Thomas Root, Andrew Xuan Vinh Tran, and et al. 2023. "Melanoma Brain Metastases: A Systematic Review of Opportunities for Earlier Detection, Diagnosis, and Treatment" Life 13, no. 3: 828. https://doi.org/10.3390/life13030828
APA StyleDiaz, M. J., Mark, I., Rodriguez, D., Gelman, B., Tran, J. T., Kleinberg, G., Levin, A., Beneke, A., Root, K. T., Tran, A. X. V., & Lucke-Wold, B. (2023). Melanoma Brain Metastases: A Systematic Review of Opportunities for Earlier Detection, Diagnosis, and Treatment. Life, 13(3), 828. https://doi.org/10.3390/life13030828