
Complications in Patients with Chronic Type B Aortic Dissection (cTBAD)—A Long-Term Analysis


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Criteria
2.2. CT Protocol
2.3. Follow-Ups
2.4. Data Collection and Statistical Analysis
3. Results
3.1. Patient Demographics and Therapeutic Approach
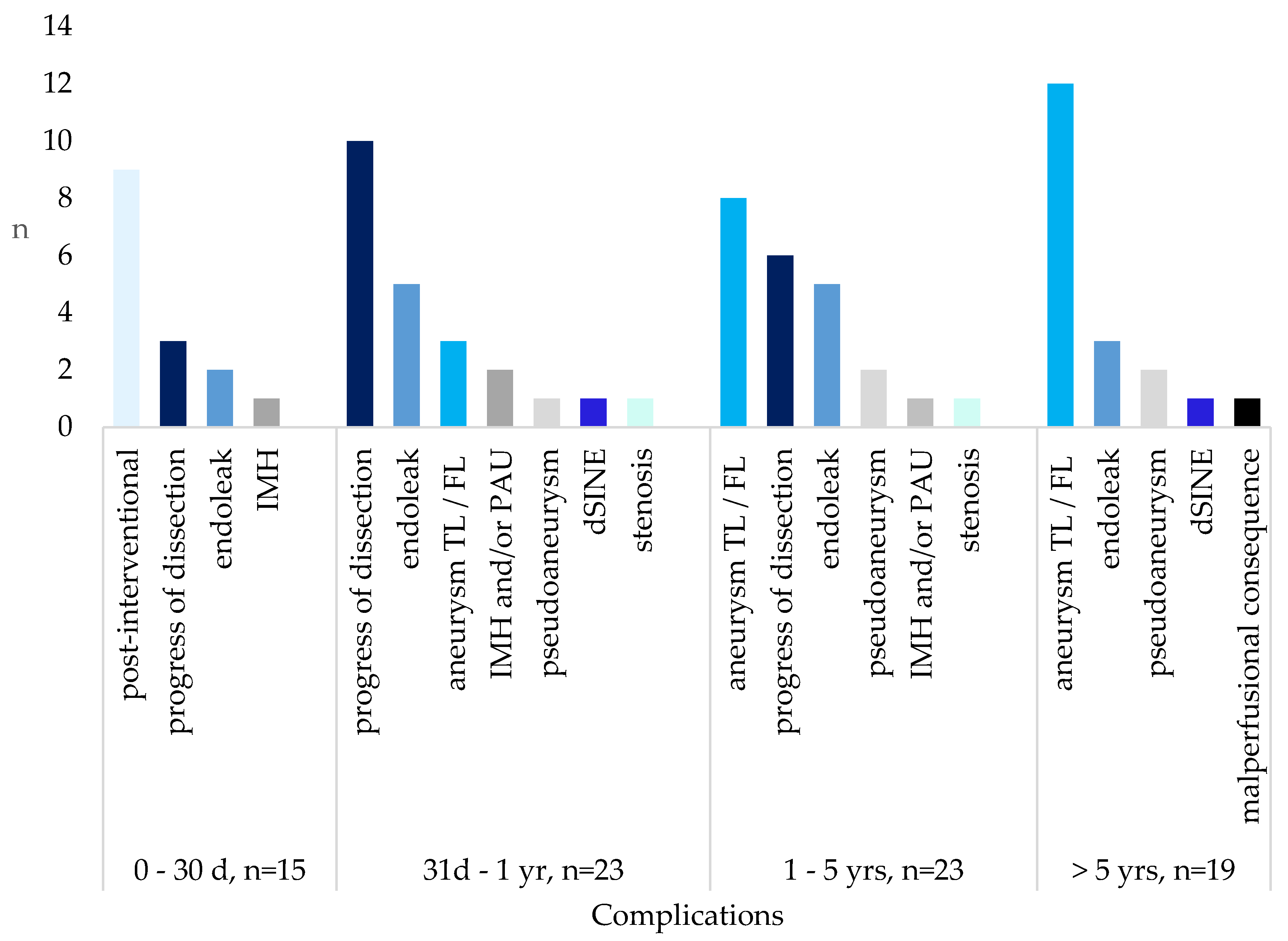
3.2. Complications
3.3. Mortality
3.4. Aortic Remodeling
3.5. Reinterventions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nienaber, C.A.; Clough, R.E.; Sakalihasan, N.; Suzuki, T.; Gibbs, R.; Mussa, F.; Jenkins, M.P.; Thompson, M.M.; Evangelista, A.; Yeh, J.S.M.; et al. Aortic dissection. Nat. Rev. Dis. Prim. 2016, 2, 16053. [Google Scholar] [CrossRef] [PubMed]
- Parve, S.; Ziganshin, B.A.; Elefteriades, J.A. Overview of the current knowledge on etiology, natural history and treatment of aortic dissection. J. Cardiovasc. Surg. 2017, 58, 238–251. [Google Scholar] [CrossRef] [PubMed]
- Jánosi, R.A.; Rassaf, T. Improving risk prediction in patients undergoing TEVAR for Type B Aortic dissection. Int. J. Cardiol. 2020, 303, 74–75. [Google Scholar] [CrossRef]
- Kaji, S. Update on the Therapeutic Strategy of Type B Aortic Dissection. J. Atheroscler. Thromb. 2018, 25, 203–212. [Google Scholar] [CrossRef] [Green Version]
- Alfson, D.B.; Ham, S.W. Type B Aortic Dissections: Current Guidelines for Treatment. Cardiol. Clin. 2017, 35, 387–410. [Google Scholar] [CrossRef]
- Fujioka, S.; Irisawa, Y.; Horai, T.; Hosaka, S. Endovascular Therapy for Chronic Type B Aortic Dissection. Ann. Vasc. Dis. 2019, 12, 449–455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poleri, I.; Dias-Neto, M.; Rocha-Neves, J.; Sampaio, S. Type B Aortic Dissection—A Single Center Series. Rev. Port. Cir. Cardio-Torac. Vasc. Orgao Of. Soc. Port. Cir. Cardio-Torac. Vasc. 2019, 26, 131–137. [Google Scholar]
- Hellgren, T.; Kuzniar, M.; Wanhainen, A.; Steuer, J.; Mani, K. Clinical and Morphologic Outcomes of Endovascular Repair for Subacute and Chronic Type B Aortic Dissection. Ann. Vasc. Surg. 2021, 72, 390–399. [Google Scholar] [CrossRef]
- Li, D.-L.; He, Y.-J.; Wang, X.-H.; He, Y.Y.; Wu, Z.H.; Zhu, Q.Q.; Shang, T.; Zhang, H.K. Long-term Results of Thoracic Endovascular Aortic Repair for Type B Aortic Dissection and Risk Factors for Survival. J. Endovasc. Ther. 2020, 27, 358–367. [Google Scholar] [CrossRef]
- Erbel, R.; Aboyans, V.; Boileau, C.; Bossone, E.; Di Bartolomeo, R.; Eggebrecht, H.; Vrints, C.J. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur. Heart J. 2014, 35, 2873–2926. [Google Scholar] [CrossRef] [Green Version]
- Lortz, J.; Papathanasiou, M.; Rammos, C.; Steinmetz, M.; Lind, A.; Tsagakis, K.; Schlosser, T.; Jakob, H.; Rassaf, T.; Jánosi, R.A. High intimal flap mobility assessed by intravascular ultrasound is associated with better short-term results after TEVAR in chronic aortic dissection. Sci. Rep. 2019, 9, 7267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oberhuber, A. S2k Leitlinie Typ B Aortendissektion; Deutsche Gesellschaft für Gefäßchirurgie und Gefäßmedizin: Berlin, Germany, 2022. [Google Scholar]
- Lortz, J.; Leinburger, F.; Tsagakis, K.; Rammos, C.; Lind, A.; Schlosser, T.; Jakob, H.; Rassaf, T.; Jánosi, R.A. Distal Stent Graft Induced New Entry: Risk Factors in Acute and Chronic Type B Aortic Dissections. Eur. J. Vasc. Endovasc. Surg. 2019, 58, 822–830. [Google Scholar] [CrossRef]
- Lortz, J.; Tsagakis, K.; Rammos, C.; Horacek, M.; Schlosser, T.; Jakob, H.; Rassaf, T.; Jánosi, R.A. Intravascular ultrasound assisted sizing in thoracic endovascular aortic repair improves aortic remodeling in Type B aortic dissection. PLoS ONE 2018, 13, e0196180. [Google Scholar] [CrossRef] [Green Version]
- Burdess, A.; Mani, K.; Tegler, G.; Wanhainen, A. Stent-graft induced new entry tears after type B aortic dissection: How to treat and how to prevent? J. Cardiovasc. Surg. 2018, 59, 789–796. [Google Scholar] [CrossRef] [PubMed]
- Puech-Leao, P.; Estenssoro, A.E.V.; Wakassa, T.B.; Casella, I.B.; DeLuccia, N. Long-term Results of Endovascular Treatment of Chronic Type B Aortic Dissection by Closure of the Primary Tear. Ann. Vasc. Surg. 2020, 66, 179–182. [Google Scholar] [CrossRef]
- Arnaoutakis, D.J.; Khan, T.A.; Scali, S.T.; Neal, D.; Giles, K.A.; Cooper, M.A.; Beaver, T.M.; Huber, T.S.; Upchurch, G.R.; Arnaoutakis, G.J.; et al. Remodeling, Reintervention, and Survival After Endovascular Repair of Chronic Type B Dissection. Ann. Thorac. Surg. 2021, 111, 1560–1569. [Google Scholar] [CrossRef] [PubMed]
- Giles, K.A.; Beck, A.W.; Lala, S.; Patterson, S.; Back, M.; Fatima, J.; Arnaoutakis, D.J.; Arnaoutakis, G.J.; Beaver, T.M.; Berceli, S.A.; et al. Implications of secondary aortic intervention after thoracic endovascular aortic repair for acute and chronic type B dissection. J. Vasc. Surg. 2019, 69, 1367–1378. [Google Scholar] [CrossRef]
- Alexander, S.A.; Rubin, G.D. Imaging the thoracic aorta: Anatomy, technical considerations, and trauma. Semin. Roentgenol. 2009, 44, 8–15. [Google Scholar] [CrossRef]
- Jánosi, R.A.; Tsagakis, K.; Bettin, M.; Kahlert, P.; Horacek, M.; Al-Rashid, F.; Schlosser, T.; Jakob, H.; Eggebrecht, H.; Erbel, R. Thoracic aortic aneurysm expansion due to late distal stent graft-induced new entry. Catheter. Cardiovasc. Interv. 2015, 85, E43–E53. [Google Scholar] [CrossRef]
- Nienaber, C.A.; Kische, S.; Rousseau, H.; Eggebrecht, H.; Rehders, T.C.; Kundt, G.; Glass, A.; Scheinert, D.; Czerny, M.; Kleinfeldt, T.; et al. Endovascular repair of type B aortic dissection: Long-term results of the randomized investigation of stent grafts in aortic dissection trial. Circ. Cardiovasc. Interv. 2013, 6, 407–416. [Google Scholar] [CrossRef] [Green Version]
- Loskutov, A.; Cooley, M.; Scheidt, M.; Mansukhani, N.; Hart, J.; Hieb, R.A.; Rossi, P.J.; Patel, P.J. Endovascular Management of Chronic Type B Aortic Dissection. Tech. Vasc. Interv. Radiol. 2021, 24, 100752. [Google Scholar] [CrossRef] [PubMed]
- Fukuhara, S.; Tchouta, L.; Pampati, R.; Liesman, D.R.; Khaja, M.S. Laser aortic septotomy during thoracic endovascular aortic repair for chronic type B aortic dissection. J. Thorac. Cardiovasc. Surg. 2022, 164, 450–459. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.L.; de Boer, M.; Hwang, B.; Wilson, B.; Brookes, J.; McNamara, N.; Tian, D.H.; Shiraev, T.; Preventza, O. Thoracic endovascular repair of chronic type B aortic dissection: A systematic review. Ann. Cardiothorac. Surg. 2022, 11, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Kong, M.; Ni, M.; Zhu, X.; Qian, J.; Duan, Q.; Song, J.; Feng, Z.; Dong, A. False lumen patency status and outcomes after endovascular repair of uncomplicated chronic type B dissection. Catheter. Cardiovasc. Interv. 2022, 100, 696–704. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Comorbidity | n (%) |
|---|---|
| Aneurysm of the ascending aorta | 45 (33.8) |
| Aneurysm of the descending aorta | 29 (21.8) |
| Intramural hematoma (IMH) | 21 (15.8) |
| Aneurysm of the infrarenal aorta | 11 (8.3) |
| Penetrating aortic ulcer (PAU) | 6 (4.5) |
| Aneurysm of the iliac artery | 3 (2.3) |
| Comorbidity | n (%) |
|---|---|
| Arterial hypertension | 132 (99.2) |
| Dyslipidemia, hypercholesterinemia | 87 (65.4) |
| Nicotine abuse | 60 (45.1) |
| Coronary heart disease | 59 (44.4) |
| Aortic valve defect | 58 (43.6) |
| Chronic kidney disease (CKD) | 52 (39.1) |
| Obesity (BMI > 30 kg/m2) | 41 (30.8) |
| PTCA and coronary stent implantation | 28 (21.1) |
| Coronary bypass | 17 (12.8) |
| Diabetes mellitus type 2 | 16 (12.0) |
| COPD (chronic obstructive lung disease) | 16 (12.0) |
| Myocardial infarction | 14 (10.5) |
| Valve replacement | 12 (9.0) |
| Peripheral artery disease (PAD) | 11 (8.3) |
| Apoplexy | 10 (7.5) |
| Pacemaker | 7 (5.3) |
| Connective tissue disease Marfan’s syndrome, Ehlers-Danlos syndrome, Loeys-Dietz syndrome | 4 (3.0) |
| Bicuspid aortic valve | 3 (2.3) |
| Time Frame | Complications | n (%) |
|---|---|---|
| 0–30 days (n = 15) | Post-interventional | 9 (60) |
| Progress of dissection | 3 (20) | |
| Endoleak | 2 (13.3) | |
| Intramural hematoma (IMH) | 1 (6.7) | |
| 31 days–1 year (n = 23) | Progress of dissection | 10 (43.6) |
| Endoelak | 5 (21.7) | |
| Aneurysm of true (TL) or false lumen (FL) | 3 (13.1) | |
| IMH and/or penetrating aortic ulcer (PAU) | 2 (8.7) | |
| Pseudoaneurysm | 1 (4.3) | |
| Distal stent graft-induced new entry (dSINE) | 1 (4.3) | |
| Stenosis | 1 (4.3) | |
| 1–5 years (n = 23) | Aneurysm of true (TL) or false lumen (FL) | 8 (34.8) |
| Progress of dissection | 6 (26.2) | |
| Endoleak | 5 (21.7) | |
| Pseudoaneurysm | 2 (8.7) | |
| IMH and/or PAU | 1 (4.3) | |
| Stenosis | 1 (4.3) | |
| >5 years (n = 19) | Aneurysm of true (TL) or false lumen (FL) | 12 (63.2) |
| Endoleak | 3 (15.8) | |
| Pseudoaneurysm | 2 (10.4) | |
| dSINE | 1 (5.3) | |
| Long-term malperfusion (renal shrinkage) | 1 (5.3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohajeri, D.; Rammos, C.; Tsagakis, K.; Schlosser, T.; Ruhparwar, A.; Rassaf, T.; Jánosi, R.A.; Lortz, J. Complications in Patients with Chronic Type B Aortic Dissection (cTBAD)—A Long-Term Analysis. Life 2023, 13, 851. https://doi.org/10.3390/life13030851
Mohajeri D, Rammos C, Tsagakis K, Schlosser T, Ruhparwar A, Rassaf T, Jánosi RA, Lortz J. Complications in Patients with Chronic Type B Aortic Dissection (cTBAD)—A Long-Term Analysis. Life. 2023; 13(3):851. https://doi.org/10.3390/life13030851
Chicago/Turabian StyleMohajeri, Darya, Christos Rammos, Konstantinos Tsagakis, Thomas Schlosser, Arjang Ruhparwar, Tienush Rassaf, Rolf Alexander Jánosi, and Julia Lortz. 2023. "Complications in Patients with Chronic Type B Aortic Dissection (cTBAD)—A Long-Term Analysis" Life 13, no. 3: 851. https://doi.org/10.3390/life13030851
APA StyleMohajeri, D., Rammos, C., Tsagakis, K., Schlosser, T., Ruhparwar, A., Rassaf, T., Jánosi, R. A., & Lortz, J. (2023). Complications in Patients with Chronic Type B Aortic Dissection (cTBAD)—A Long-Term Analysis. Life, 13(3), 851. https://doi.org/10.3390/life13030851