


Parkinson’s Disease and the Cardiac Cycle: A Rapid Literature Review and Case Series

Abstract
:1. Introduction
2. Materials and Methods
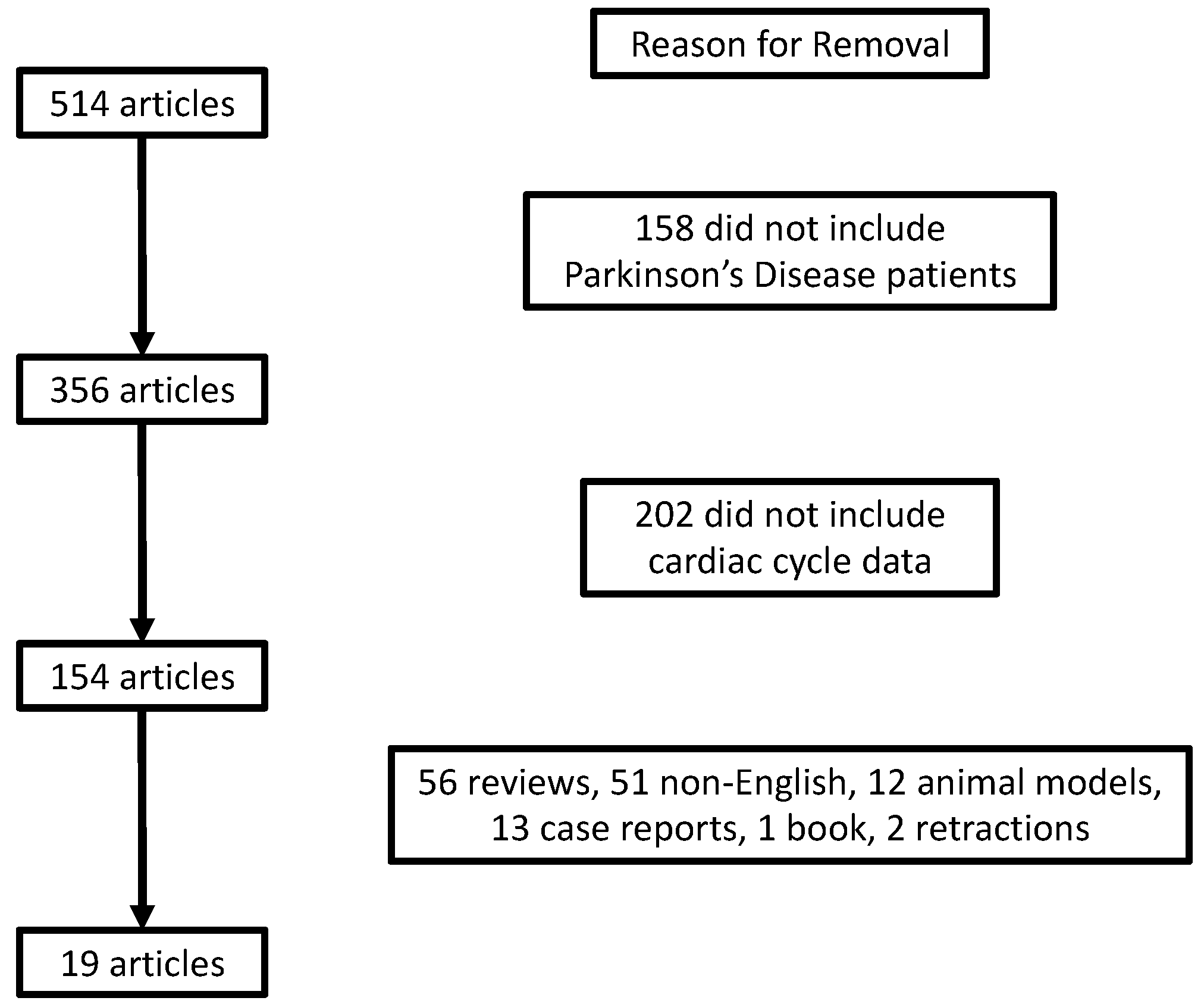
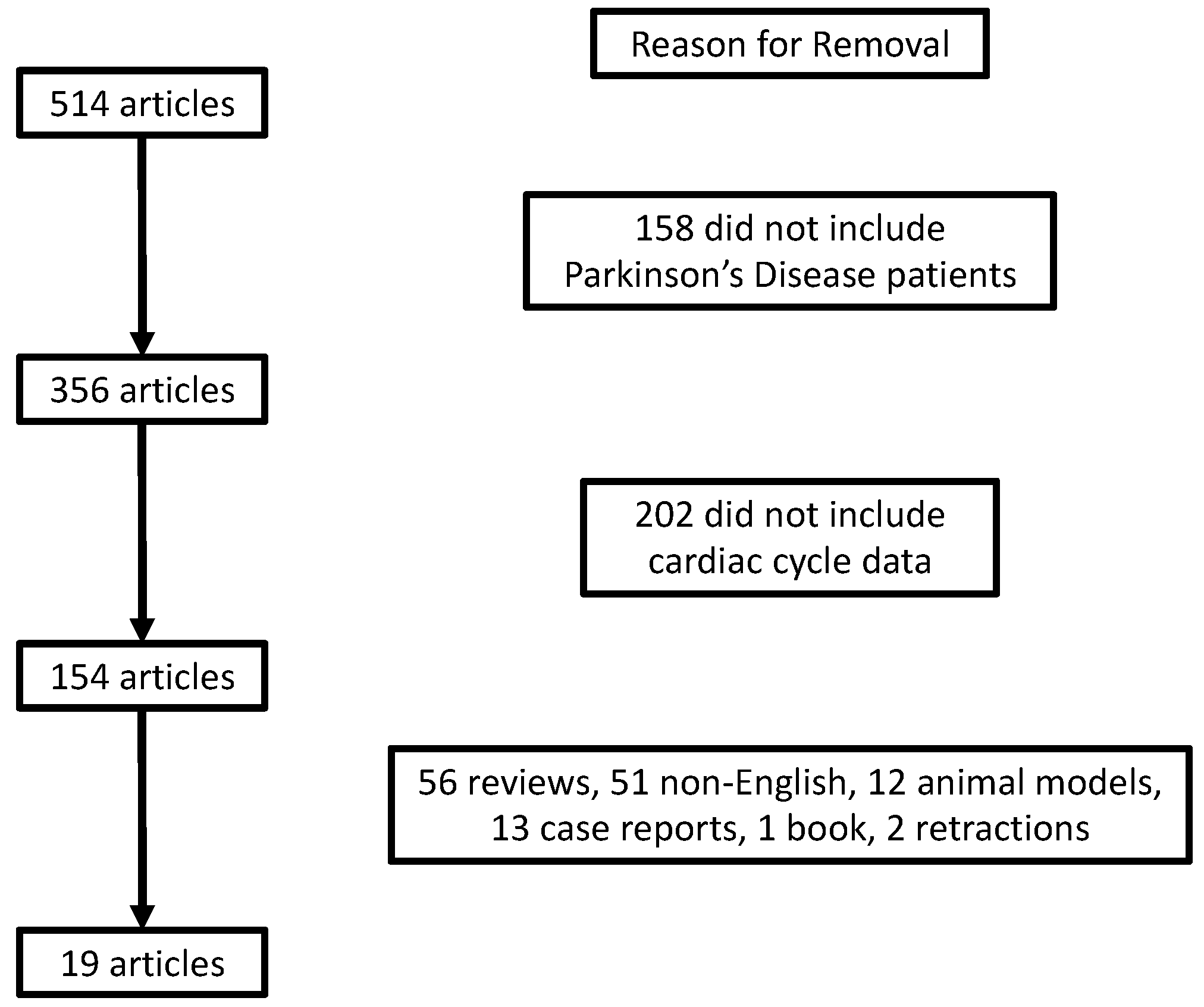
2.1. Literature Review
2.2. Case Series Methods
- -
- Diastolic performance index: DPI = IVRT/Ejection time
- -
- Systolic performance index: SPI = IVCT/Ejection time
- -
- Heart (or myocardial index) performance index: HPI (or MPI) = (IVCT + IVRT)/Ejection time
3. Results
3.1. Review Results
3.1.1. Baseline Observational Studies
3.1.2. Autonomic Dysfunction
3.1.3. Impact of Medication

{kind=link}
| Author | Population | Primary Method of Assessment | Primary Cardiac Findings |
|---|---|---|---|
| (Erken Pamukcu et al., 2018) [19] | 40 Parkinson’s Disease (H&Y = 2.5) and 40 healthy controls | Conventional and strain echocardiography | Reduced global longitudinal strain, left ventricular end-diastolic dimension, left ventricular end-systolic dimension and ejection fraction |
| (Strano et al., 2016) [20] | 18 Parkinson’s Disease (H&Y = 1 or 2) and 18 healthy controls | Transthoracic echocardiography | No differences between groups |
| (Zhao et al., 2017) [21] | 22 Parkinson’s Disease in coordination and manipulation therapy and 14 Parkinson’s Disease control PD (H&Y = 2–4) | Not stated | Baseline LVEF was lower in the coordination and manipulation therapy group, and increased over time |
| (Gunaydin et al., 2016) [22] | 55 Parkinson’s Disease patients with L-dopa therapy and 30 healthy controls (H&Y = 1–4) | Transthoracic and strain echocardiography | Reduced E/A in PD, however, Levodopa therapy has no impact on left ventricular systolic function |
| (Ozer et al., 2014) [23] | 34 Parkinson’s Disease cabergoline and 42 Parkinson’s Disease no cabergoline | Conventional echocardiography and tissue doppler imaging | Only diastolic differences (E parameters) associated with cumulative cabergoline dose |
| (Rasmussen et al., 2008a) [24] | 71 Parkinson’s Disease with EDDA for at least 6 months and 39 non-EDDA | Conventional and speckle tracking echocardiography and tissue doppler imaging | No differences in myocardial systolic and diastolic function between groups |
| (Rasmussen et al., 2008b) [25] | 85 Parkinson’s Disease (H&Y = 2.3) with EDAA and 53 non-EDAA (H&Y = 1.9) | Continuous wave Doppler | No differences in LVEF |
| (Kenangil et al., 2007) [26] | 46 Parkinson’s Disease on pergolide or cabergoline or both for a minimum of 1 year and 49 healthy controls | Conventional echocardiography | No differences in LVEF |
| (Imrich et al., 2009) [27] | 13 Parkinson’s Disease (H&Y = 1–5) or pure autonomic failure, 15 patients with multiple system atrophy and 5 healthy controls | Impedance cardiogram | Tyramine infusion had little response on cardiac intervals in PD |
| (Meijer et al., 2008) [28] | 18 healthy young controls, 25 elderly healthy controls, 18 Parkinson’s Disease (H&Y = 1–3) | Impedance cardiogram | Reduced relative contribution of PEP to RR intervals and reduced exertion during exercise in PD |
| (Imrich et al., 2008) [29] | 9 Parkinson’s Disease and 3 with pure autonomic failure | Impedance cardiogram | No reduction in PEP following tyramine infusion |
| (Whitsett & Goldberg, 1972) [30] | 6 Parkinson’s Disease assessed after 2 weeks of levodopa therapy and after 3 months of continuous therapy | Carotid pulse contour and phonocardiogram | PEP responses of acute and chronic levodopa to dopamine and epinephrine intake are not different |
3.2. Case Series Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wong, S.L.; Gilmour, H.; Ramage-Morin, P.L. Parkinson’s disease: Prevalence, diagnosis and impact. Health Rep. 2014, 25, 10–14. [Google Scholar] [PubMed]
- Zhang, Y.; Ren, R.; Sanford, L.D.; Yang, L.; Zhou, J.; Tan, L.; Li, T.; Zhang, J.; Wing, Y.K.; Shi, J.; et al. Sleep in Parkinson’s disease: A systematic review and meta-analysis of polysomnographic findings. Sleep Med. Rev. 2020, 51, 101281. [Google Scholar] [CrossRef] [PubMed]
- Kataoka, H.; Saeki, K.; Kurumatani, N.; Sugie, K.; Obayashi, K. Objective sleep measures between patients with Parkinson’s disease and community-based older adults. Sleep Med. 2020, 68, 110–114. [Google Scholar] [CrossRef] [PubMed]
- El Mokadem, M.O.; Hassan, A.; Hussein, M.; Mohamed, Y.M. The potential role of 2D-speckle tracking echocardiography for detecting left ventricular systolic dysfunction in patients with Parkinson’s disease: A case control study. Acta Cardiol. 2021, 76, 979–986. [Google Scholar] [CrossRef] [PubMed]
- Heimrich, K.G.; Lehmann, T.; Schlattmann, P.; Prell, T. Heart Rate Variability Analyses in Parkinson’s Disease: A Systematic Review and Meta-Analysis. Brain Sci. 2021, 11, 959. [Google Scholar] [CrossRef]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [Green Version]
- Haensel, A.; Mills, P.J.; Nelesen, R.A.; Ziegler, M.G.; Dimsdale, J.E. The relationship between heart rate variability and inflammatory markers in cardiovascular diseases. Psychoneuroendocrinology 2008, 33, 1305–1312. [Google Scholar] [CrossRef] [Green Version]
- Singh, J.; Bhagaloo, L.; Sy, E.; Lavoie, A.J.; Dehghani, P.; Bardutz, H.A.; Mang, C.S.; Buttigieg, J.; Neary, J.P. Cardiac impairments in postacute COVID-19 with sustained symptoms: A review of the literature and proof of concept. Physiol. Rep. 2022, 10, e15430. [Google Scholar] [CrossRef]
- Singh, J.; Bhagaloo, L.; Sy, E.; Lavoie, A.J.; Dehghani, P.; Neary, P. Novel effects of acute COVID-19 on cardiac mechanical function: Two case studies. Physiol. Rep. 2021, 9, e14998. [Google Scholar] [CrossRef]
- Singh, J.; Ellingson, C.J.; Ellingson, C.A.; Scott, P.; Neary, J.P. Cardiac cycle timing and contractility following acute sport-related concussion. Res. Sport. Med. 2022, 20, 1–8. [Google Scholar] [CrossRef]
- Singh, J.; Ellingson, C.J.; Ellingson, C.A.; Scott, P.; Patrick Neary, J. Cardiac cycle timing intervals in university varsity athletes. Eur. J. Sport Sci. 2023, 23, 1–15. [Google Scholar] [CrossRef]
- Biering-Sorensen, T.; Mogelvang, R.; Jensen, J.S. Prognostic value of cardiac time intervals measured by tissue Doppler imaging M-mode in the general population. Heart 2015, 101, 954–960. [Google Scholar] [CrossRef] [Green Version]
- Piqueras-Flores, J.; Lopez-Garcia, A.; Moreno-Reig, A.; Gonzalez-Martinez, A.; Hernandez-Gonzalez, A.; Vaamonde-Gamo, J.; Jurado-Roman, A. Structural and functional alterations of the heart in Parkinson’s disease. Neurol. Res. 2018, 40, 53–61. [Google Scholar] [CrossRef]
- Canga, Y.; Emre, A.; Yuksel, G.A.; Karatas, M.B.; Yelgec, N.S.; Gurkan, U.; Calik, A.N.; Tireli, H.; Terzi, S. Assessment of Atrial Conduction Times in Patients with Newly Diagnosed Parkinson’s Disease. Park. Dis. 2018, 2018, 2916905. [Google Scholar] [CrossRef]
- Di Stefano, C.; Sobrero, G.; Milazzo, V.; Vallelonga, F.; Romagnolo, A.; Zibetti, M.; Milan, A.; Veglio, F.; Maule, S. Cardiac organ damage in patients with Parkinson’s disease and reverse dipping. J. Hypertens 2020, 38, 289–294. [Google Scholar] [CrossRef]
- Zawadka-Kunikowska, M.; Słomko, J.; Tafil-Klawe, M.; Klawe, J.J.; Cudnoch-Jędrzejewska, A.; Newton, J.L.; Zalewski, P. Role of peripheral vascular resistance as an indicator of cardiovascular abnormalities in patients with Parkinson’s disease. Clin. Exp. Pharmacol. Physiol. 2017, 44, 1089–1098. [Google Scholar] [CrossRef]
- Pérez, T.; Tijero, B.; Gabilondo, I.; Luna, A.; Llorens, V.; Berganzo, K.; Acera, M.; Gonzalez, A.; Sanchez-Ferro, A.; Lezcano, E.; et al. Cardiocirculatory manifestations in Parkinson’s disease patients without orthostatic hypotension. J. Hum. Hypertens 2015, 29, 604–609. [Google Scholar] [CrossRef]
- Kinbara, T.; Hayano, T.; Otani, N.; Furutani, Y.; Tanaka, S. Iodine-123 metaiodobenzylguanidine imaging can predict future cardiac events in Japanese patients with Parkinson’s disease. Ann. Nucl. Med. 2013, 27, 123–131. [Google Scholar] [CrossRef]
- Erken Pamukcu, H.; Gerede Uludag, D.M.; Tekin Tak, B.; Sorgun, M.H.; Efe, T.H.; Acibuca, A.; Akbostanci, C.; Turhan, S. Evaluation of the effect of non-ergot dopamine agonists on left ventricular systolic function with speckle tracking echocardiography. Anatol. J. Cardiol. 2018, 20, 213–219. [Google Scholar] [CrossRef] [Green Version]
- Strano, S.; Fanciulli, A.; Rizzo, M.; Marinelli, P.; Palange, P.; Tiple, D.; De Vincentis, G.; Calcagnini, G.; Censi, F.; Meco, G.; et al. Cardiovascular dysfunction in untreated Parkinson’s disease: A multi-modality assessment. J. Neurol. Sci. 2016, 370, 251–255. [Google Scholar] [CrossRef]
- Zhao, M.; Hu, C.; Wu, Z.; Chen, Y.; Li, Z.; Zhang, M. Effects of coordination and manipulation therapy for patients with Parkinson disease. Int. J. Neurosci. 2017, 127, 762–769. [Google Scholar] [CrossRef] [PubMed]
- Gunaydin, Z.Y.; Bektas, O.; Karagoz, A.; Ozer, F.F. Effects of levodopa therapy on global left ventricular systolic function in patients with Parkinson disease. Wien. Klin. Wochenschr. 2016, 128, 528–533. [Google Scholar] [CrossRef] [PubMed]
- Ozer, N.; Yorgun, H.; Canpolat, U.; Elibol, B. Evaluation of the valvular and biventricular functions in Parkinson patients using ergotamine-derived dopamine agonist: An observational study. Anadolu. Kardiyol. Derg. 2014, 14, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, V.G.; Poulsen, S.H.; Dupont, E.; Ostergaard, K.; Safikhany, G.; Egeblad, H. Ergotamine-derived dopamine agonists and left ventricular function in Parkinson patients: Systolic and diastolic function studied by conventional echocardiography, tissue Doppler imaging, and two-dimensional speckle tracking. Eur. J. Echocardiogr. 2008, 9, 803–808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasmussen, V.G.; Poulsen, S.H.; Dupont, E.; Ostergaard, K.; Safikhany, G.; Egeblad, H. Heart valve disease associated with treatment with ergot-derived dopamine agonists: A clinical and echocardiographic study of patients with Parkinson’s disease. J. Intern. Med. 2008, 263, 90–98. [Google Scholar] [CrossRef]
- Kenangil, G.; Ozekmekçi, S.; Koldas, L.; Sahin, T.; Erginöz, E. Assessment of valvulopathy in Parkinson’s disease patients on pergolide and/or cabergoline. Clin. Neurol. Neurosurg. 2007, 109, 350–353. [Google Scholar] [CrossRef]
- Imrich, R.; Eldadah, B.A.; Bentho, O.; Pechnik, S.; Sharabi, Y.; Holmes, C.; Grossman, E.; Goldstein, D.S. Functional effects of cardiac sympathetic denervation in neurogenic orthostatic hypotension. Park. Relat. Disord. 2009, 15, 122–127. [Google Scholar] [CrossRef] [Green Version]
- Meijer, J.H.; Boesveldt, S.; Elbertse, E.; Berendse, H.W. Method to measure autonomic control of cardiac function using time interval parameters from impedance cardiography. Physiol. Meas. 2008, 29, S383–S391. [Google Scholar] [CrossRef]
- Imrich, R.; Eldadah, B.A.; Bentho, O.; Pechnik, S.; Sharabi, Y.; Holmes, C.; Goldstein, D.S. Attenuated pre-ejection period response to tyramine in patients with cardiac sympathetic denervation. Ann. N. Y. Acad. Sci. 2008, 1148, 486–489. [Google Scholar] [CrossRef] [Green Version]
- Whitsett, T.L.; Goldberg, L.I. Effects of levodopa on systolic preejection period, blood pressure, and heart rate during acute and chronic treatment of Parkinson’s disease. Circulation 1972, 45, 97–106. [Google Scholar] [CrossRef] [Green Version]
- Biering-Sorensen, T.; Mogelvang, R.; de Knegt, M.C.; Olsen, F.J.; Galatius, S.; Jensen, J.S. Cardiac Time Intervals by Tissue Doppler Imaging M-Mode: Normal Values and Association with Established Echocardiographic and Invasive Measures of Systolic and Diastolic Function. PLoS ONE 2016, 11, e0153636. [Google Scholar] [CrossRef] [Green Version]
- Biering-Sorensen, T.; Mogelvang, R.; Pedersen, S.; Schnohr, P.; Sogaard, P.; Jensen, J.S. Usefulness of the myocardial performance index determined by tissue Doppler imaging m-mode for predicting mortality in the general population. Am. J. Cardiol. 2011, 107, 478–483. [Google Scholar] [CrossRef]
- Amara, A.W.; Memon, A.A. Effects of Exercise on Non-motor Symptoms in Parkinson’s Disease. Clin. Ther. 2018, 40, 8–15. [Google Scholar] [CrossRef] [Green Version]
- Amara, A.W.; Wood, K.H.; Joop, A.; Memon, R.A.; Pilkington, J.; Tuggle, S.C.; Reams, J.; Barrett, M.J.; Edwards, D.A.; Weltman, A.L.; et al. Randomized, Controlled Trial of Exercise on Objective and Subjective Sleep in Parkinson’s Disease. Mov. Disord. 2020, 35, 947–958. [Google Scholar] [CrossRef]
| Participant Demographics | |
|---|---|
| Age (years) ± SD | 70 ± 7 |
| Weight (kg) ± SD | 77 ± 12 |
| Height (cm) ± SD | 169 ± 7 |
| BMI (kg/m2) ± SD | 27 ± 5 |
| Female (%) | 33 |
| % Hypertension | 72 |
| % Diabetes | 28 |
| % Other cardiac disease | 72 |
| % Prescribed Levodopa | 100 |
| % Exercisers * | 46 |
| Montreal Cognitive Assessment (mean ± SD) | 26 ± 2 |
| W1 | W1 EX | W2 | W2 EX | W3 | W3 EX | W4 | W4 EX | W5 | W5 EX | W6 | W6 EX | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IVRT (ms) | 91 ± 7 | 97 ± 7 | 93 ± 8 | 98 ± 8 | 90 ± 5 | 97 ± 10 | 91 ± 4 | 98 ± 9 | 93 ± 8 | 98 ± 7 | 93 ± 3 | 100 ± 10 |
| % Δ IVRT EX | 4.4 | 6.2 | 5.2 | 3.8 | 3.9 | 4.8 | ||||||
| IVCT (ms) | 34 ± 1 | 34 ± 2 | 33 ± 1 | 37 ± 3 | 33 ± 1 | 37 ± 3 | 33 ± 3 | 36 ± 2 | 35 ± 2 | 37 ± 2 | 35 ± 2 | 37 ± 1 |
| % Δ IVCT EX | −0.4 | 9.5 | 9.3 | 11.8 | 3.9 | 5.4 | ||||||
| SPI | 0.10 ± 0.01 | 0.10 ± 0.02 | 0.10 ± 0.02 | 0.11 ± 0.02 | 0.11 ± 0.03 | 0.11 ± 0.02 | 0.10 ± 0.02 | 0.11 ± 0.02 | 0.11 ± 0.03 | 0.11 ± 0.01 | 0.11 ± 0.02 | 0.11 ± 0.02 |
| % Δ SPI EX | −0.4 | 11 | −4 | 6.4 | −2.9 | 2.6 | ||||||
| DPI | 0.27 ± 0.02 | 0.28 ± 0.04 | 0.27 ± 0.03 | 0.29 ± 0.05 | 0.30 ± 0.09 | 0.28 ± 0.04 | 0.28 ± 0.03 | 0.29 ± 0.04 | 0.28 ± 0.03 | 0.28 ± 0.04 | 0.28 ± 0.04 | 0.29 ± 0.06 |
| % Δ DPI EX | 5.7 | 8.7 | −7.9 | 2.1 | −1.5 | 3.1 | ||||||
| HPI | 0.37 ± 0.03 | 0.38 ± 0.06 | 0.36 ± 0.05 | 0.40 ± 0.06 | 0.42 ± 0.12 | 0.39 ± 0.05 | 0.38 ± 0.05 | 0.40 ± 0.05 | 0.39 ± 0.06 | 0.38 ± 0.05 | 0.39 ± 0.06 | 0.40 ± 0.07 |
| % Δ HPI EX | 4 | 9.5 | −6.8 | 4.2 | −2.4 | 2.9 | ||||||
| Systole (ms) | 348 ± 43 | 347 ± 56 | 348 ± 53 | 342 ± 65 | 321 ± 56 | 342 ± 53 | 334 ± 33 | 343 ± 58 | 334 ± 50 | 353 ± 58 | 337 ± 43 | 347 ± 60 |
| % Δ Systole EX | −0.2 | −1.7 | 6.6 | 2.8 | 5.7 | 3.1 | ||||||
| TF (mG) | 17 ± 6 | 13 ± 4 | 14 ± 2 | 12 ± 4 | 14 ± 2 | 11 ± 4 | 14 ± 4 | 11 ± 4 | 13 ± 3 | 12 ± 4 | 14 ± 3 | 12 ± 5 |
| % Δ TF EX | −23.2 | −18.3 | −21.9 | −23.2 | −7.6 | −12.6 | ||||||
| SE (%) | 81 ± 11 | 83 ± 9 | 81 ± 9 | 84 ± 8 | 79 ± 13 | 81 ± 9 | 81 ± 12 | 82 ± 8 | 81 ± 12 | 84 ± 7 | 77 ± 15 | 82 ± 9 |
| % Δ SE EX | 2.3 | 2.6 | 3.0 | 0.8 | 3.7 | 6.0 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bardutz, H.; Singh, J.; Rehman, Z.; Bernat, P. Parkinson’s Disease and the Cardiac Cycle: A Rapid Literature Review and Case Series. Life 2023, 13, 1003. https://doi.org/10.3390/life13041003
Bardutz H, Singh J, Rehman Z, Bernat P. Parkinson’s Disease and the Cardiac Cycle: A Rapid Literature Review and Case Series. Life. 2023; 13(4):1003. https://doi.org/10.3390/life13041003
Chicago/Turabian StyleBardutz, Holly, Jyotpal Singh, Ziaur Rehman, and Patrick Bernat. 2023. "Parkinson’s Disease and the Cardiac Cycle: A Rapid Literature Review and Case Series" Life 13, no. 4: 1003. https://doi.org/10.3390/life13041003
APA StyleBardutz, H., Singh, J., Rehman, Z., & Bernat, P. (2023). Parkinson’s Disease and the Cardiac Cycle: A Rapid Literature Review and Case Series. Life, 13(4), 1003. https://doi.org/10.3390/life13041003