


Embolization of Ruptured Infratentorial Pial AVM in Pregnancy
 ,
,
Abstract
:1. Introduction
2. Management of Radiation Dose Reduction
2.1. Basic Principles and Radiation Limits
Radiation Limit and Fetal Doses
2.2. Radiation Dose Reduction and Protocol Optimization
New Technologies
3. Embolization Techniques
3.1. Transarterial Embolization
3.1.1. Plug Technique and Prolonged Intranidal Injection
3.1.2. Pressure Cooker Technique
3.1.3. Occlusion Balloon Technique
3.1.4. Multiple Catheter Technique
3.2. Transvenous and Combined Techniques
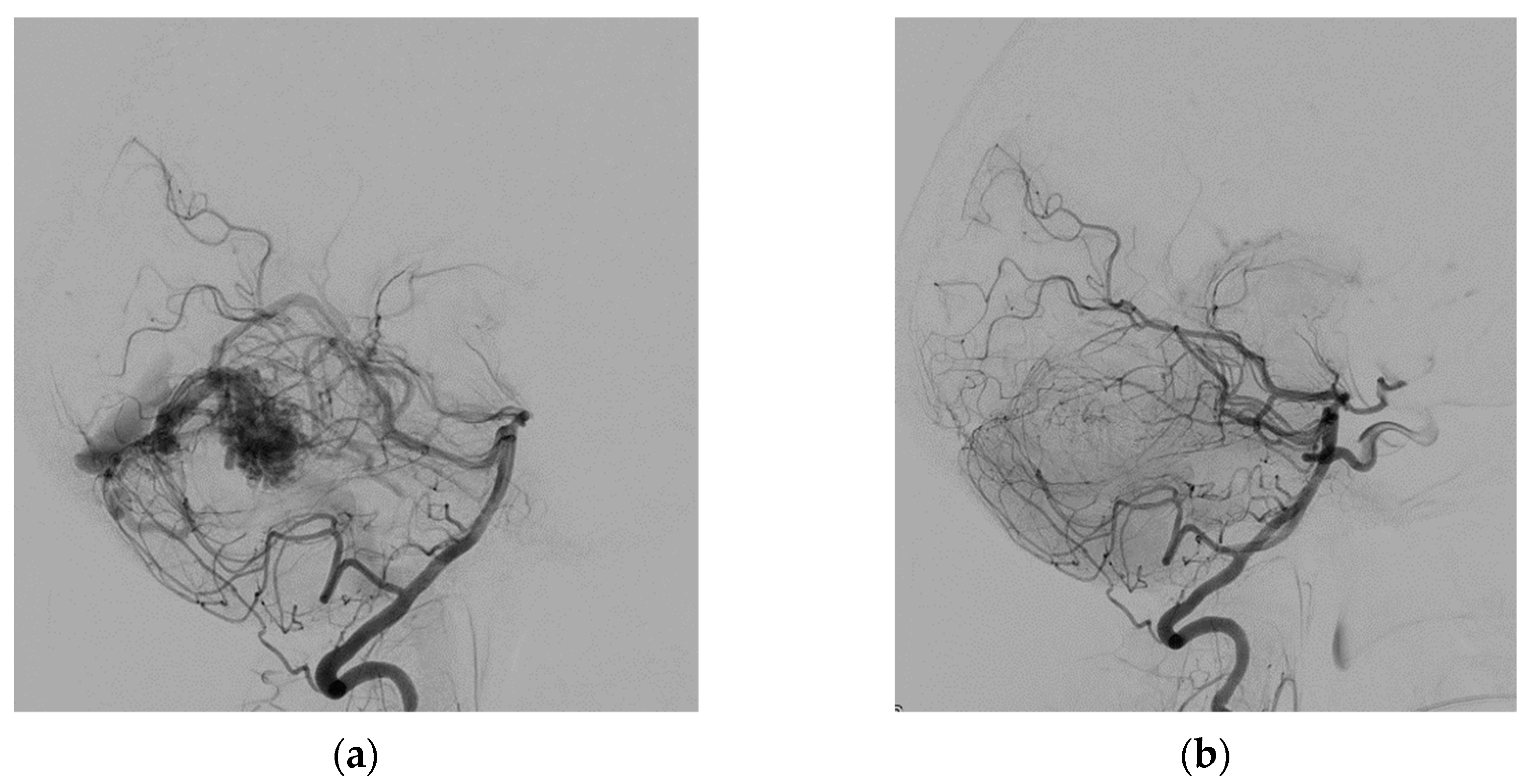
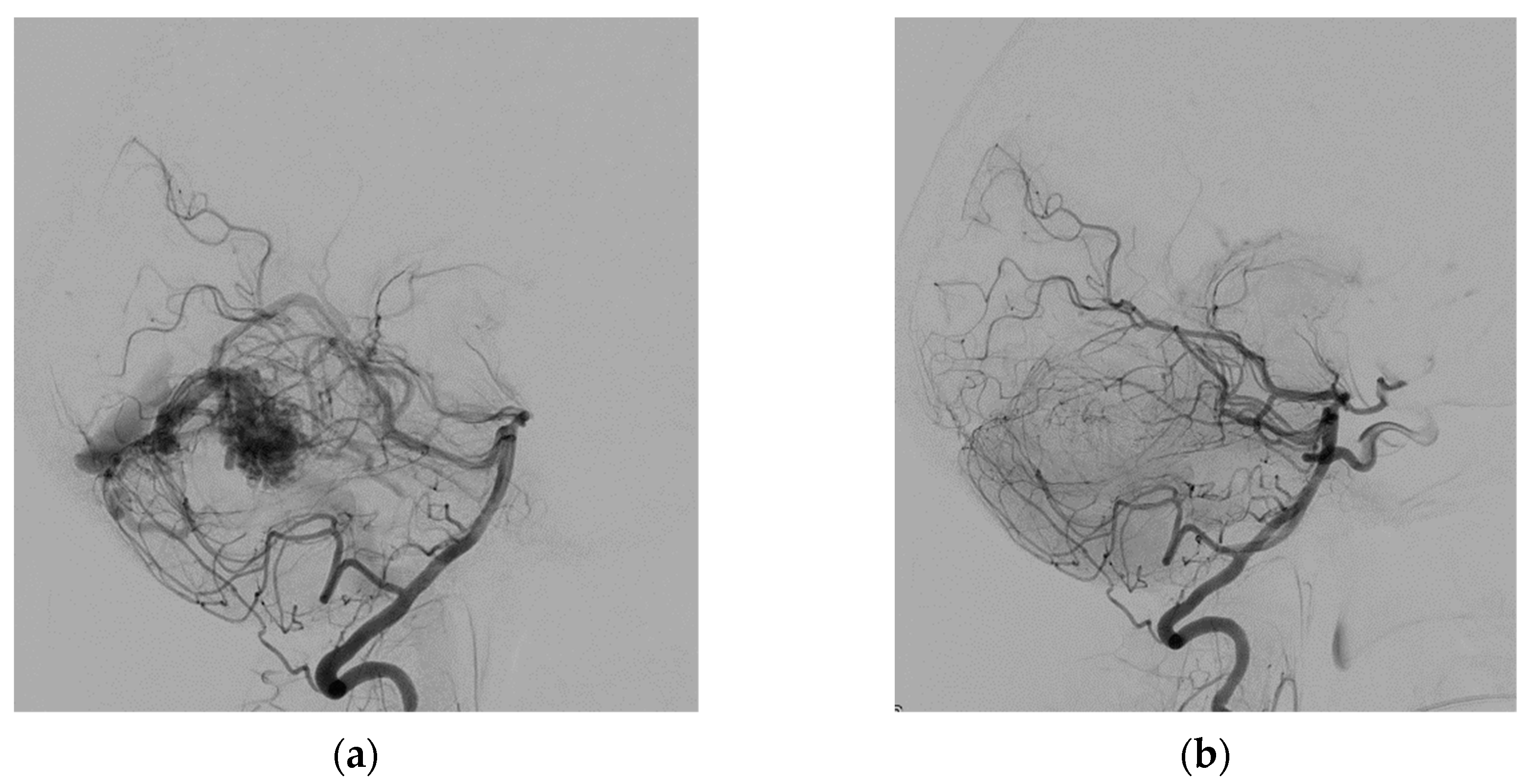
4. Case
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Al-Shahi, R.; Warlow, C. A systematic review of the frequency and prognosis of arteriovenous malformations of the brain in adults. Brain 2001, 124, 1900–1926. [Google Scholar] [CrossRef]
- Derdeyn, C.P.; Zipfel, G.J.; Albuquerque, F.C.; Cooke, D.L.; Feldmann, E.; Sheehan, J.P.; Torner, J.C.; American Heart Association Stroke Council. Management of Brain Arteriovenous Malformations: A Scientific Statement for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2017, 48, e200–e224. [Google Scholar] [CrossRef]
- Gaillard, F.; Weerakkody, Y. Brain Arteriovenous Malformation. Reference Article. Available online: Radiopaedia.org (accessed on 6 February 2022). [CrossRef]
- Dogan, S.N.; Bagcilar, O.; Mammadov, T.; Kizilkilic, O.; Islak, C.; Kocer, N. De Novo Development of a Cerebral Arteriovenous Malformation: Case Report and Review of the Literature. World Neurosurg. 2019, 126, 257–260. [Google Scholar] [CrossRef] [PubMed]
- Lv, X.; Li, Y. The clinical characteristics and treatment of cerebral AVM in pregnancy. Neuroradiol. J. 2015, 28, 385–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohr, J.P.; Parides, M.K.; Stapf, C.; Moquete, E.; Moy, C.S.; Overbey, J.R.; Salman, R.A.-S.; Vicaut, E.; Young, W.L.; Houdart, E.; et al. Medical management with or without interventional therapy for unruptured brain arteriovenous malformations (ARUBA): A multicentre, non-blinded, randomised trial. Lancet 2014, 383, 614–621. [Google Scholar] [CrossRef] [Green Version]
- Can, A.; Gross, B.A.; Du, R. The natural history of cerebral arteriovenous malformations. Handb. Clin. Neurol. 2017, 143, 15–24. [Google Scholar] [CrossRef]
- Ogilvy, C.S.; Stieg, P.E.; Awad, I.; Brown, R.D., Jr.; Kondziolka, D.; Rosenwasser, R.; Young, W.L.; Hademenos, G.; Special Writing Group of the Stroke Council, American Stroke Association. AHA Scientific Statement: Recommendations for the management of intracranial arteriovenous malformations: A statement for healthcare professionals from a special writing group of the Stroke Council, American Stroke Association. Stroke 2001, 32, 1458–1471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Castro-Afonso, L.H.; Vanzim, J.R.; Trivelato, F.P.; Rezende, M.T.; Ulhôa, A.C.; Chodraui-Filho, S.F.; Mattos, L.G.D.A.; Mounayer, C.; Nakiri, G.S.; Colli, B.O.; et al. Association between draining vein diameters and intracranial arteriovenous malformation hemorrhage: A multicentric retrospective study. Neuroradiology 2020, 62, 1497–1505. [Google Scholar] [CrossRef]
- Lee, S.; Kim, Y.; Navi, B.B.; Abdelkhaleq, R.; Salazar-Marioni, S.; Blackburn, S.L.; Bambhroliya, A.B.; Lopez-Rivera, V.; Vahidy, F.; I Savitz, S.; et al. Risk of intracranial hemorrhage associated with pregnancy in women with cerebral arteriovenous malformations. J. NeuroInterv. Surg. 2021, 13, 707–710. [Google Scholar] [CrossRef]
- Zhong, Z.; Ni, H.; Zhu, J.; Jiang, H.; Hu, J.; Lin, D.; Bian, L. Management of Acute Hemorrhage Caused by Cerebral Arteriovenous Malformation During Pregnancy–Case Series and Literature Review. World Neurosurg. 2021, 152, e688–e699. [Google Scholar] [CrossRef]
- Health Risks. Available online: https://www.epa.ie/environment-and-you/radiation/radiation-exposure-and-your-health/health-risks/ (accessed on 12 February 2022).
- UNSCEAR 2000 REPORT Vol. I. SOURCES AND EFFECTS OF IONIZING RADIATION. Available online: http://www.unscear.org/unscear/en/publications/2000_1.html (accessed on 12 February 2022).
- Walsh, C. Interpretation of risk for low dose radiation exposures: Inconsistencies, philosophical problems and fallacies. J. Radiol. Prot. 2020, 40, 646–653. [Google Scholar] [CrossRef] [PubMed]
- Shuryak, I.; Cornforth, M.N. Accounting for overdispersion of lethal lesions in the linear quadratic model improves performance at both high and low radiation doses. Int. J. Radiat. Biol. 2021, 97, 50–59. [Google Scholar] [CrossRef] [PubMed]
- European Council Directive. 2013/59/Euratom on basic safety standards for protection against the dangers arising from ex-posure to ionising radiation and repealing directives 89/618/Euratom, 90/641/ Euratom, 96/29/Euratom, 97/43/Euratom and 2003/122/Euratom. Off. J. Eur. Union 2014, L13, 1–73. [Google Scholar]
- European Society of Radiology (ESR). Summary of the European Directive 2013/59/Euratom: Essentials for health professionals in radiology. Insights Imaging 2015, 6, 411–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wrixon, A.D. New ICRP recommendations. J. Radiol. Prot. 2008, 28, 161–168. [Google Scholar] [CrossRef]
- ICRP. Publication 84: Pregnancy and medical radiation. Ann. ICRP 2000, 30, 1–43. Available online: https://journals.sagepub.com/doi/pdf/10.1177/ANIB_30_1 (accessed on 20 February 2022).
- Allisy-Roberts, P.J.; Williams, J. Farr’s Physics for Medical Imaging, 2nd ed.; Elsevier Health Sciences: Amsterdam, The Netherlands, 2008. [Google Scholar] [CrossRef]
- Ploussi, A.; Efstathopoulos, E.P.; Brountzos, E. The Importance of Radiation Protection Education and Training for Medical Professionals of All Specialties. Cardiovasc. Interv. Radiol. 2021, 44, 829–834. [Google Scholar] [CrossRef]
- Paulo, G.; Bartal, G.; Vano, E. Radiation Dose of Patients in Fluoroscopically Guided Interventions: An Update. Cardiovasc. Interv. Radiol. 2021, 44, 842–848. [Google Scholar] [CrossRef]
- Rehani, M.M.; Miller, D.L.; Baliyan, V. High-Dose Fluoroscopically Guided Procedures in Patients: Radiation Management Recommendations for Interventionalists. Cardiovasc. Interv. Radiol. 2021, 44, 849–856. [Google Scholar] [CrossRef]
- Ploussi, A.; Brountzos, E.; Rammos, S.; Apostolopoulou, S.; Efstathopoulos, E.P. Radiation Exposure in Pediatric Interventional Procedures. Cardiovasc. Interv. Radiol. 2021, 44, 857–865. [Google Scholar] [CrossRef]
- Torresin, A.; Evans, S.; Lizio, D.; Pierotti, L.; Stasi, M.; Salerno, S. Practical recommendations for the application of DE 59/2013. Radiol. Med. 2019, 124, 721–727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cornacchia, S.; Errico, R.; La Tegola, L.; Maldera, A.; Simeone, G.; Fusco, V.; Niccoli-Asabella, A.; Rubini, G.; Guglielmi, G. The new lens dose limit: Implication for occupational radiation protection. Radiol. Med. 2019, 124, 728–735. [Google Scholar] [CrossRef] [PubMed]
- Guglielmi, G.; Pinto, A.; Salerno, S. Editorial from guest editors current Euratom legislation (DE 59/2013): New patient management in radiation protection. Radiol. Med. 2019, 124, 711–713. [Google Scholar] [CrossRef] [Green Version]
- Loose, R.; Wucherer, M. How to Measure/Calculate Radiation Dose in Patients? Cardiovasc. Interv. Radiol. 2021, 44, 835–841. [Google Scholar] [CrossRef]
- Bohrer, E.; Schäfer, S.B.; Krombach, G.A. Die neue Strahlenschutzgesetzgebung—Teil 1: Änderungen für die arbeitstägliche Routine in der Radiologie [The new radiation protection legislation-part 1: Modifications in radiology for the workflow in clinical routine]. Radiologe 2020, 60, 721–728. [Google Scholar] [CrossRef] [PubMed]
- Bartal, G.; Vano, E.; Paulo, G. Get Protected! Recommendations for Staff in IR. Cardiovasc. Interv. Radiol. 2021, 44, 871–876. [Google Scholar] [CrossRef]
- Wojcik, A.; Harms-Ringdahl, M. Radiation protection biology then and now. Int. J. Radiat. Biol. 2019, 95, 841–850. [Google Scholar] [CrossRef] [Green Version]
- Englander, M.J.; Ghatan, C. Radiation and the Pregnant IR: Myth versus Fact. Cardiovasc. Interv. Radiol. 2021, 44, 877–882. [Google Scholar] [CrossRef]
- Sanchez, R.; Vano, E.; Fernández, J.; Moreu, M.; Lopez-Ibor, L. Brain Radiation Doses to Patients in an Interventional Neuroradiology Laboratory. AJNR Am. J. Neuroradiol. 2014, 35, 1276–1280. [Google Scholar] [CrossRef] [Green Version]
- Borota, L.; Jangland, L.; Åslund, P.-E.; Ronne-Engström, E.; Nyberg, C.; Mahmoud, E.; Sakaguchi, T.; Patz, A. Spot fluoroscopy: A novel innovative approach to reduce radiation dose in neurointerventional procedures. Acta Radiol. 2017, 58, 600–608. [Google Scholar] [CrossRef] [Green Version]
- Nagesh, S.V.S.; Vakharia, K.; Waqas, M.; Fennell, V.S.; Atwal, G.S.; Shallwani, H.; Bednarek, D.R.; Davies, J.M.; Snyder, K.V.; Mokin, M.; et al. High-Definition Zoom Mode: A High Resolution X-ray Microscope for Neurointerventional Treatment Procedures. J. Neuroimaging 2019, 29, 565–572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clarençon, F.; Maizeroi-Eugène, F.; Maingreaud, F.; Bresson, D.; Ayoub, D.; Sourour, N.-A.; de Champfleur, N.M.; Chiras, J.; Yardin, C.; Mounayer, C. Interest of convex spherical anamorphosis in better understanding of brain AVMs’ angioarchitecture. J. NeuroInterv. Surg. 2016, 8, 959–964. [Google Scholar] [CrossRef] [PubMed]
- Keil, F.; Bergkemper, A.; Birkhold, A.; Kowarschik, M.; Tritt, S.; Berkefeld, J. 4D Flat Panel Conebeam CTA for Analysis of the Angioarchitecture of Cerebral AVMs with a Novel Software Prototype. AJNR Am. J. Neuroradiol. 2022, 43, 102–109. [Google Scholar] [CrossRef]
- Kocer, N.; Kandemirli, S.G.; Dashti, R.; Kizilkilic, O.; Hanimoglu, H.; Sanus, G.Z.; Tunali, Y.; Tureci, E.; Islak, C.; Kaynar, M.Y. Single-stage planning for total cure of grade III–V brain arteriovenous malformations by embolization alone or in combination with microsurgical resection. Neuroradiology 2019, 61, 195–205. [Google Scholar] [CrossRef] [PubMed]
- Durst, C.R.; Starke, R.M.; Gaughen, J.; Evans, A.J. A method for complete angiographic obliteration of a brain arteriovenous malformation in a single session through a single pedicle. J. Clin. Neurosci. 2015, 22, 391–395. [Google Scholar] [CrossRef]
- Saatci, I.; Geyik, S.; Yavuz, K.; Cekirge, H.S. Endovascular treatment of brain arteriovenous malformations with prolonged intranidal Onyx injection technique: Long-term results in 350 consecutive patients with completed endovascular treatment course. J. Neurosurg. 2011, 115, 78–88. [Google Scholar] [CrossRef]
- Chapot, R.; Stracke, P.; Velasco, A.; Nordmeyer, H.; Heddier, M.; Stauder, M.; Schooss, P.; Mosimann, P.J. The Pressure Cooker Technique for the treatment of brain AVMs. J. Neuroradiol. 2014, 41, 87–91. [Google Scholar] [CrossRef]
- Nishiyama, T.; Yabuta, M.; Ogawa, R.; Kurihara, Y. n-Butyl Cyanoacrylate Embolization with Coil Protection to Prevent Reflux: A Modified Pressure Cooker Technique Using a Single Microcatheter. J. Vasc. Interv. Radiol. 2022, 33, 721–724. [Google Scholar] [CrossRef]
- Spiotta, A.M.; James, R.F.; Lowe, S.R.; Vargas, J.; Turk, A.S.; Chaudry, M.I.; Bhalla, T.; Janjua, R.M.; Delaney, J.J.; Quintero-Wolfe, S.; et al. Balloon-augmented Onyx embolization of cerebral arteriovenous malformations using a dual-lumen balloon: A multicenter experience. J. NeuroInterv. Surg. 2015, 7, 721–727. [Google Scholar] [CrossRef]
- Vollherbst, D.F.; Chapot, R.; Wallocha, M.; Saatci, I.; Cekirge, S.; Rouchaud, A.; Mounayer, C.; Kocer, N.; Kizilkilic, O.; A Sourour, N.; et al. First clinical multicenter experience with the new Scepter Mini microballoon catheter. J. NeuroInterv. Surg. 2021, 13, 261–266. [Google Scholar] [CrossRef]
- Mendes, G.A.C.; Silveira, E.P.; Saleme, S.; Iosif, C.; Ponomarjova, S.; Caire, F.; Mounayer, C. Balloon-assisted microcatheter navigation for AVM embolization: Technical note. J. Neurosurg. 2015, 123, 1120–1124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abud, D.; Riva, R.; Nakiri, G.; Padovani, F.; Khawaldeh, M.; Mounayer, C. Treatment of Brain Arteriovenous Malformations by Double Arterial Catheterization with Simultaneous Injection of Onyx: Retrospective Series of 17 Patients. AJNR Am. J. Neuroradiol. 2011, 32, 152–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bendszus, M.; Möhlenbruch, M.; Rohde, S. Comment On: Curative Embolization of Brain Arteriovenous Malformations with Onyx: Patient Selection, Embolization Technique, and Results. Clin. Neuroradiol. 2012, 22, 181–182. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-J.; Norat, P.; Ding, D.; Mendes, G.A.C.; Tvrdik, P.; Park, M.S.; Kalani, M.Y. Transvenous embolization of brain arteriovenous malformations: A review of techniques, indications, and outcomes. Neurosurg. Focus 2018, 45, E13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massoud, T.F.; Hademenos, G.J. Transvenous Retrograde Nidus Sclerotherapy under Controlled Hypotension (TRENSH): A Newly Proposed Treatment for Brain Arteriovenous Malformations-Concepts and Rationale. Neurosurgery 1999, 45, 351–363; discussion 363–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhoton, A.L., Jr. The cerebral veins. Neurosurgery 2002, 51, S159–S205. [Google Scholar] [CrossRef]
- Komiyama, M. Functional Venous Anatomy of the Brain for Neurosurgeons. Jpn. J. Neurosurg. 2017, 26, 488–495. [Google Scholar] [CrossRef] [Green Version]
- Hudak, I.; Botz, L.; Ezero, E.; Doczi, T. A Novel Strategy in the Treatment of High-Grade Brain AVMs: Combined Transarterial and Transvenous Embolization by Means of a Polyurethane Based New Liquid Embolizing Agent. In Abstracts—9th Congress of the WFITN (World Federation of Interventional Neuroradiology)—Jiuhua Resort & Convention Center, Beijing, China, 9–13 September 2007. Interv. Neuroradiol. 2007, 13 (Suppl. 2), 128. [Google Scholar] [CrossRef]
- Mendes, G.A.C.; Kalani, M.Y.S.; Iosif, C.; Lucena, A.F.; Carvalho, R.; Saleme, S.; Mounayer, C. Transvenous Curative Embolization of Cerebral Arteriovenous Malformations: A Prospective Cohort Study. Neurosurgery 2018, 83, 957–964. [Google Scholar] [CrossRef]
- Koyanagi, M.; Mosimann, P.J.; Nordmeyer, H.; Heddier, M.; Krause, J.; Narata, A.-P.; El Serwi, A.; Stracke, C.P.; Chapot, R. The transvenous retrograde pressure cooker technique for the curative embolization of high-grade brain arteriovenous malformations. J. NeuroInterv. Surg. 2021, 13, 637–641. [Google Scholar] [CrossRef]
- Zeleňák, K.; Sýkora, J.; Vorčák, M.; Zeleňáková, J.; Kurča, E.; Deriggo, J.; Hanko, M.; Kolarovszki, B. Transvenous embolization of a ruptured brain arteriovenous malformation. Cesk. Slov. Neurol. N. 2020, 83, 441–443. [Google Scholar] [CrossRef]
- Iosif, C.; Filho, J.A.A.; Gilbert, C.E.; Rafie, A.N.; Saleme, S.; Rouchaud, A.; Mounayer, C. Selective arterial temporary flow arrest with balloons during transvenous embolization for the treatment of brain arteriovenous malformations: A feasibility study with MRI-monitored adverse events. J. NeuroInterv. Surg. 2022, 14, 1234–1238. [Google Scholar] [CrossRef] [PubMed]
- Iosif, C.; de Lucena, A.F.; Abreu-Mattos, L.G.; Ala, V.H.E.; El-Ghanam, A.; Saleme, S.; Caire, F.; Mounayer, C. Curative endovascular treatment for low-grade Spetzler-Martin brain arteriovenous malformations: A single-center prospective study. J. NeuroInterv. Surg. 2019, 11, 699–705. [Google Scholar] [CrossRef] [PubMed]
- Mendes, G.A.; Silveira, E.P.; Caire, F.; Martel, M.-P.B.; Saleme, S.; Iosif, C.; Mounayer, C. Endovascular Management of Deep Arteriovenous Malformations. Neurosurgery 2016, 78, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Fahed, R.; E Darsaut, T.; Mounayer, C.; Chapot, R.; Piotin, M.; Blanc, R.; Pereira, V.M.; Abud, D.G.; Iancu, D.; Weill, A.; et al. Transvenous Approach for the Treatment of cerebral Arteriovenous Malformations (TATAM): Study protocol of a randomised controlled trial. Interv. Neuroradiol. 2019, 25, 305–309. [Google Scholar] [CrossRef]
- Draper, E.S.; Zeitlin, J.; Fenton, A.C.; Weber, T.; Gerrits, J.; Martens, G.; Misselwitz, B.; Breart, G.; MOSAIC Research Group. Investigating the variations in survival rates for very preterm infants in 10 European regions: The MOSAIC birth cohort. Arch. Dis. Child Fetal Neonatal Ed. 2009, 94, F158–F163. [Google Scholar] [CrossRef] [Green Version]
- Dinc, N.; Platz, J.; Tritt, S.; Quick-Weller, J.; Eibach, M.; Wolff, R.; Berkefeld, J.; Seifert, V.; Marquardt, G. Posterior fossa AVMs: Increased risk of bleeding and worse outcome compared to supratentorial AVMs. J. Clin. Neurosci. 2018, 53, 171–176. [Google Scholar] [CrossRef]
- Lai, L.-F.; Chen, J.-X.; Zheng, K.; He, X.-Y.; Li, X.-F.; Zhang, X.; Wang, Q.-J.; Duan, C.-Z.; Chen, M. Posterior fossa brain arteriovenous malformations: Clinical features and outcomes of endovascular embolization, adjuvant microsurgery and radiosurgery. Clin. Neuroradiol. 2018, 28, 17–24. [Google Scholar] [CrossRef]
- Asano, S.; Hayashi, N.; Edakubo, S.; Hosokawa, M.; Suwa, J.; Saito, Y.; Ichi, S.; Taneda, M.; Katoh, K. Successful perinatal management of a ruptured brain arteriovenous malformation in a pregnant patient by endovascular embolization followed by elective cesarean section: A single-case experience. JA Clin. Rep. 2016, 2, 21. [Google Scholar] [CrossRef] [Green Version]
- Nagayama, K.; Kurita, H.; Tonari, A.; Takayama, M.; Shiokawa, Y. Radiosurgery for cerebral arteriovenous malformation during pregnancy: A case report focusing on fetal exposure to radiation. Asian J. Neurosurg. 2010, 5, 73–77. [Google Scholar]
- Yu, C.; Jozsef, G.; Apuzzo, M.L.; MacPherson, D.M.; Petrovich, Z. Fetal Radiation Doses for Model C Gamma Knife Radiosurgery. Neurosurgery 2003, 52, 687–693; discussion 693. [Google Scholar] [CrossRef] [PubMed]
- Lv, X.; Liu, P.; Li, Y. Pre-existing, incidental and hemorrhagic AVMs in pregnancy and postpartum: Gestational age, morbidity and mortality, management and risk to the fetus. Interv. Neuroradiol. 2016, 22, 206–211. [Google Scholar] [CrossRef] [Green Version]
- Jermakowicz, W.J.; Tomycz, L.D.; Ghiassi, M.; Singer, R.J. Use of endovascular embolization to treat a ruptured arteriovenous malformation in a pregnant woman: A case report. J. Med. Case Rep. 2012, 6, 113. [Google Scholar] [CrossRef] [Green Version]
- Vollherbst, D.F.; Chapot, R.; Bendszus, M.; Möhlenbruch, M.A. Glue, Onyx, Squid or PHIL? Liquid Embolic Agents for the Embolization of Cerebral Arteriovenous Malformations and Dural Arteriovenous Fistulas. Clin. Neuroradiol. 2022, 32, 25–38. [Google Scholar] [CrossRef] [PubMed]
- Trivedi, R.; Kirkpatrick, P. Arteriovenous malformations of the cerebral circulation that rupture in pregnancy. J. Obstet. Gynaecol. 2003, 23, 484–489. [Google Scholar] [CrossRef] [PubMed]
- Granata, F.; Alafaci, C.; Giacobbe, A.; De Vivo, A.; Mancuso, A.; Conti, A.; Pontoriero, A.; Pitrone, A.; Longo, M. Endovascular Treatment of Cerebral Arteriovenous Malformation Bleeding during Pregnancy—A Case Report. Neuroradiol. J. 2010, 23, 473–478. [Google Scholar] [CrossRef]
- Salvati, A.; Ferrari, C.; Chiumarulo, L.; Medicamento, N.; Dicuonzo, F.; De Blasi, R. Endovascular treatment of brain arteriovenous malformations ruptured during pregnancy—A report of two cases. J. Neurol. Sci. 2011, 308, 158–161. [Google Scholar] [CrossRef]
- Dashti, S.R.; Spalding, A.C.; Yao, T.L. Multimodality treatment of a ruptured grade IV posterior fossa arteriovenous malformation in a patient pregnant with twins: Case report. J. NeuroInterv. Surg. 2012, 4, e21. [Google Scholar] [CrossRef]
- Porras, J.L.; Yang, W.; Philadelphia, E.; Law, J.; Garzon-Muvdi, T.; Caplan, J.M.; Colby, G.P.; Coon, A.L.; Tamargo, R.J.; Huang, J. Hemorrhage Risk of Brain Arteriovenous Malformations During Pregnancy and Puerperium in a North American Cohort. Stroke 2017, 48, 1507–1513. [Google Scholar] [CrossRef]
- Sohail, R.; Bashir, Q.; Kanwal, S.; Ali, M.I. Cerebral arteriovenous malformations during pregnancy: A management dilemma. BMJ Case Rep. 2019, 12, e228759. [Google Scholar] [CrossRef]
- Teik, C.K.; Basri, N.I.; Karim, A.K.A.; Abu, M.A.; Ahmad, M.F.; Ghani, N.A.A.; Hing, E.Y.; Zakaria, R.; Thanabalan, J.A.; Abu Bakar, A.; et al. Management Options and Outcome of Cerebral Arteriovenous Malformation in Pregnancy: Case Series. Arch. Iran. Med. 2019, 22, 340–343. [Google Scholar] [PubMed]
- Yan, K.L.; Ko, N.U.; Hetts, S.W.; Weinsheimer, S.; Abla, A.A.; Lawton, M.T.; Kim, H. Maternal and Fetal Outcomes in Women with Brain Arteriovenous Malformation Rupture during Pregnancy. Cerebrovasc. Dis. 2021, 50, 296–302. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Brain AVM | Value |
|---|---|
| Incidence | Approximately 1 per 100,000 per year [1,2,3] |
| Prevalence Rate | Approximately 0.01–0.5% [5] |
| Location | 85% vs. 15% for supratentorial (two-thirds superficial and one-third deep) vs. infratentorial [3] |
| The annual risk of bleeding from unruptured bAVM | Approximately 1–4% [6,7] |
| Rebleeding Rate | Is higher, especially in the first year after rupture, ranging from 6% to 15.8% [7] |
| The potential risk of intracranial hemorrhage compared to a nonpregnant period in women with AVM | Increases 3.27 times during pregnancy and puerperium [10] |
| Mortality Rate | Maternal mortality rate from rebleeding (up to 28%) and 14% fetal death rate [5] |
| Dose | Example |
|---|---|
| 0.1 micro-Sievert (μSv) | The banana equivalent dose (BED)—is the dose one is exposed to by eating one average-sized banana because it contains radioactive isotopes of potassium 1 |
| 1 μSv | The average annual dose to a ‘heavy’ consumer of Irish Sea seafood 1 |
| 8 μSv | The dose received on a return flight from Dublin to London 1 |
| 20 μSv | Dose from a single chest X-ray 1 1 in 1,000,000 lifetime risk of fatal cancer 1 |
| 0.4 mSv = 400 μSv | The worldwide average annual effective dose for the population from diagnostic medical X-ray examinations 2 |
| 2.4 mSv = 2400 μSv | The worldwide annual average effective dose from natural sources (6.57 μSv daily) 2 |
| Dose | Example |
|---|---|
| 1 milli-Sievert (mSv) | As soon as a pregnant worker informs the employer of the pregnancy, the employment conditions must ensure that the equivalent dose to the unborn child is as low as reasonably achievable and unlikely to exceed 1 mSv during at least the remainder of the pregnancy. 1 |
| 6 mSv | Apprentices and students (aged 16–18 years) have more restrictive dose limits: an effective dose of 6 mSv per year and equivalent doses of 15 mSv per year in the lens of the eye, as well as 150 mSv per year in the skin and extremities. 1 |
| 20 mSv | The limit on the effective dose shall be 20 mSv in any single year (in special circumstances 50 mSv if the average annual dose over any 5 consecutive years does not exceed 20 mSv). 1 |
| 20 mSv | The limit on the equivalent dose for the eye lens shall be 20 mSv in a single year or 100 mSv in any 5 consecutive years subject to a maximum dose of 50 mSv in a single year. 1 |
| 500 mSv | The limit on the equivalent dose for the skin and extremities shall be 500 mSv in a year. 1 |
| Fetal Dose | Examination |
|---|---|
| <0.01 mGy | Chest PA 1 |
| 0.1 mGy | CT chest 1 |
| 1 mGy | Abdomen or pelvis AP 1 |
| 1.5 mGy | Lumbar spine (AP and lateral) 1 |
| 25 mGy | CT pelvis 1 |
| 100 mGy | Maximum dose of radiation to the uterus during pregnancy recommended by ICRP 2,3 |
| Principles | Examples | Clinical Practice |
|---|---|---|
| Time | Limit fluoroscopy and exposure time | Select the most experienced operator |
| Limit abdominal or pelvic fluoroscopy | The fetal limit can be approached if the fluoroscopy time exceeds 7 min | |
| Reduce the number of frames per second | Select the appropriate fluoroscopy mode | |
| Ultrasound use | Access artery puncture Guidewire navigation in the pelvic region | |
| Distance | Keep the source-to-image distance (SID) low | Keep the detector as close to the patient as possible |
| Distance between source and fetus | Limited application | |
| Important for operators mainly | Inverse square law | |
| Shielding | Protect the abdominal area of the patient/fetus | Lead skirt shielding with a lead equivalent of 0.5 mm |
| Collimate | Whenever possible | |
| Other | Increase field of view (FOV) and collimate | Limit image magnification |
| Prefer the lateral view | ||
| Minimize C-arm angulation | If you cannot reduce it, move it | |
| Experience | ||
| New technologies | Spot fluoroscopy | 50% reduction in the total fluoroscopic dose-area product |
| High-definition detector | High-definition zoom mode |
| Material Characterization | Trademark | Company–Producer |
|---|---|---|
| N-Butyl-2-cyanoacrylate (n-BCA) | TRUFILL n-BCA liquid embolic system | Codman Neuro |
| Synthetic modified co-monomer cyanoacrylate glue | Glubran 2 | GEM |
| n-hexyl-cyanoacrylate | Magic glue | Balt |
| Ethylene-vinyl alcohol (EVOH) copolymer | Onyx/Squid/Menox | Medtronic/Balt/Meril |
| Polylactide-coglycolide and polyhydroxyethylmethacrylate | PHIL (precipitating hydrophobic injectable liquid) | Microvention |
| Author | Year | Number of Cases/Age of Pregnant Women (Year) | Gestational Age at the Time of AVM Rupture (Weeks) | Embolic Material/ Number of Sessions | AVM Size, cm/Grade/ Location | Radiation Dose to the Fetus | Baby Injury | Note |
|---|---|---|---|---|---|---|---|---|
| Trivedi [69] | 2003 | 1/30 | 16 | — | —/4/dominant frontal | — | No | Preoperative embolization |
| Granata [70] | 2010 | 1/39 | 27 | 1 mL of Onyx 18/1 | 0.8/2/left parietal | — | No | Radiosurgery after pregnancy |
| Salvati [71] | 2011 | 1/23 | 19 | NBCA/1 | —/—/right frontal | — | No | Complete AVM occlusion |
| Dashti [72] | 2012 | 1/17 | 20 | Onyx/2 | 5.5/IV/posterior fossa | 1.9 × 10−30 mGy | No | The patient delivered healthy twin girls at 36 weeks of gestation by planned cesarean section |
| Jermakowicz [67] | 2012 | 1/23 | 22 | Onyx 18/1 | —/—/Left P–O | — | No | 50% embolization performed 3 weeks after bleeding, followed by complete resection 3 weeks later |
| Asano [63] | 2016 | 1/34 | 25 | 50% NBCA/1 | 1/2/right occipital | 0.14 mGy | No | Elective cesarean section at 38 weeks of gestation |
| Porras [73] | 2017 | 4/25–41 | 19–38 | — | 2–7/3–4/R–P/O, L–P/O, R–F/P, R–O | — | No | In 3 of 4 embolizations combined with radiosurgery. C-section 29–40 weeks. |
| Sohail [74] | 2019 | 1/20 | 15 | 20% Glubran/1 | —/3/right hemisphere | — | — | Termination of pregnancy by hysterotomy |
| Teik [75] | 2019 | 2/32–33 | 14–33 | —/1–2 | 2–3.2/—/basal ganglia, left parasagital | — | No | A patient with basal ganglia AVM died with an unsuccessful pregnancy |
| Yan [76] | 2021 | 3/16–26 | 16–23 | —/1 | 1.1–7.6/—/Right T/O, left T, right cerebellar | — | No | Embolization and resection in all cases. One patient underwent two resections. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zeleňák, K.; Šalát, D.; Kolarovszki, B.; Kurča, E.; Zeleňáková, J.; Koçer, N. Embolization of Ruptured Infratentorial Pial AVM in Pregnancy. Life 2023, 13, 896. https://doi.org/10.3390/life13040896
Zeleňák K, Šalát D, Kolarovszki B, Kurča E, Zeleňáková J, Koçer N. Embolization of Ruptured Infratentorial Pial AVM in Pregnancy. Life. 2023; 13(4):896. https://doi.org/10.3390/life13040896
Chicago/Turabian StyleZeleňák, Kamil, Dušan Šalát, Branislav Kolarovszki, Egon Kurča, Jana Zeleňáková, and Naci Koçer. 2023. "Embolization of Ruptured Infratentorial Pial AVM in Pregnancy" Life 13, no. 4: 896. https://doi.org/10.3390/life13040896