

Effects of Dehydroepiandrosterone (DHEA) Supplementation on Ovarian Cumulus Cells following In Vitro Fertilization (IVF)/Intra-Cytoplasmic Sperm Injection (ICSI) Treatment—A Systematic Review
 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Selection of Studies
2.5. Data Extraction and Management
2.6. Assessment of Risk of Bias
2.7. Protocol Registration
3. Results
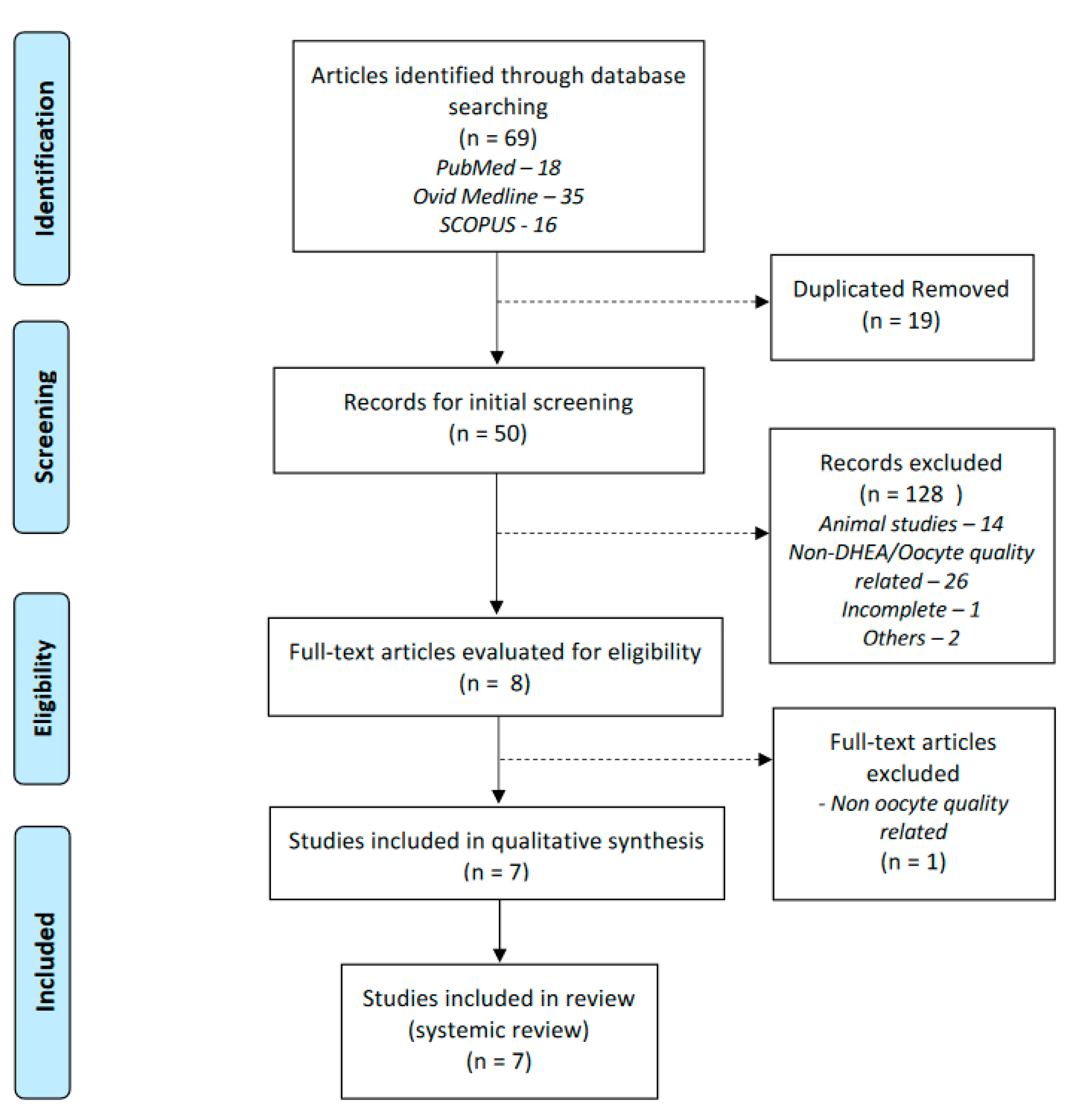
3.1. Result of Search
3.2. Characteristics of Included Studies
3.3. CC-Related Outcomes

{kind=link}
| Study | Narkwichean et al., 2017 [14] | |
|---|---|---|
| Q1 | Was true randomization used for assignment of participants to treatment groups? | Yes |
| Q2 | Was allocation to treatment groups concealed? | Yes |
| Q3 | Were treatment groups similar at the baseline? | Yes |
| Q4 | Were participants blind to treatment assignment? | Yes |
| Q5 | Were those delivering treatment blind to treatment assignment? | Yes |
| Q6 | Were outcomes assessors blind to treatment assignment? | Yes |
| Q7 | Were treatment groups treated identically other than the intervention of interest? | Yes |
| Q8 | Was follow up complete and if not, were difference between groups in terms of their follow up adequately described and analyzed? | Yes |
| Q9 | Were participants analyzed in the groups to which they were randomized? | Yes |
| Q10 | Were outcomes measures in the same way for treatment groups? | Yes |
| Q11 | Were outcomes measured in a reliable way? | Yes |
| Q12 | Was appropriate statistical analysis used? | Yes |
| Q13 | Was the trial design appropriate, and any deviations from the standard RCT design accounted for in the conduct and analysis of the trial? | Yes |
| Total Score | 100% |
| Study | Tsui et al., 2014 [13] | Lin et al., 2017 [15] | |
|---|---|---|---|
| Q1 | Were the two groups similar and recruited from the same population? | Yes | Yes |
| Q2 | Were the exposures measured similarly to assign people to both exposed and unexposed groups? | Yes | Yes |
| Q3 | Was the exposure measured in a valid and reliable way? | Yes | Yes |
| Q4 | Were confounding factors identified? | No | Yes |
| Q5 | Were strategies to deal with confounding factors stated? | No | Yes |
| Q6 | Were the groups/participants free of the outcome at the start of the study? | Not applicable | Not applicable |
| Q7 | Were the outcomes measured in a valid and reliable way? | Yes | Yes |
| Q8 | Was the follow up time reported and sufficient to be long enough for outcomes to occur? | Yes | Yes |
| Q9 | Was follow up complete, and if not, were the reasons to loss to follow up described and explored? | Yes | Yes |
| Q10 | Were strategies to address incomplete follow up utilized? | Not applicable | Not applicable |
| Q11 | Was appropriate statistical analysis used? | Yes | Yes |
| Total Score | 64% | 82% |
| Study | Lin et al., 2017 [18] | Lin et al., 2017 [16] | Li et al., 2021 [19] | Hou et al., 2022 [17] | |
|---|---|---|---|---|---|
| Q1 | Were the groups comparable other than the presence of disease in cases or the absence of disease in controls? | Yes | Yes | Yes | Yes |
| Q2 | Were cases and controls matched appropriately? | Yes | Yes | Yes | Yes |
| Q3 | Were the same criteria used for identification of cases and controls? | Yes | Yes | Yes | Yes |
| Q4 | Was exposure measured in a standard, valid and reliable way? | Yes | Yes | Yes | Yes |
| Q5 | Was exposure measured in the same way for cases and controls? | Yes | Yes | Yes | Yes |
| Q6 | Were confounding factors identified? | Unsure | Unsure | Unsure | Unsure |
| Q7 | Were strategies to deal with confounding factors stated? | Unsure | Unsure | Unsure | Unsure |
| Q8 | Were outcomes assessed in a standard, valid and reliable way for cases and controls? | Yes | Yes | Yes | Yes |
| Q9 | Was the exposure period of interest long enough to be meaningful? | Yes | Yes | Yes | Yes |
| Q10 | Was appropriate statistical analysis used? | Yes | Yes | Yes | Yes |
| Total Score | 80% | 80% | 80% | 80% |
| No | Author, Year | Study Design | Participants | Inclusion Criteria | Exclusion Criteria | Intervention | Duration of Intervention |
|---|---|---|---|---|---|---|---|
| 1 | Narkwichean et al., 2017 [14] | Randomized Controlled Trial | Total: 52 (27 DHEA, 25 placebo) |
|
| DHEA 75 mg/day | Minimum 12 weeks |
| 2 | Tsui et al., 2014 [13] | Prospective Cohort | Total: 10 | PORs, met Bologna Criteria [12] |
| DHEA(exact dose not mentioned) | NA |
| 3 | Lin et al., 2017 [15] | Prospective Cohort | Total: 6 | PORs, met Bologna Criteria [12] and had failed IVF cycle |
| DHEA 90 mg/day | Minimum 2 months |
| 4 | Lin et al., 2017 [18] | Prospective Case-Control | Total: 88≤37 yrs: 30≥37 yrs: 58 (28 with DHEA, 30 without) | Infertile women underwent IVF within study period |
| DHEA 90 mg/day | Minimum 2 months |
| 5 | Lin et al., 2017 [16] | Prospective Case-Control | Total:131NORs: 59PORs: 72 (34 with DHEA, 38 No DHEA) |
| Not mentioned | DHEA 90 mg/day | 8–16 weeks |
| 6 | Li et al., 2021 [19] | Prospective Case-Control | Total: 77≤ 38 yrs: 32>38 yrs: 45(20 with DHEA, 25 without) |
|
| DHEA 25 mg/3 times daily | Minimum 8 weeks |
| 7 | Hou et al., 2022 [17] | Prospective Case-Control | Total:60NORs: 22PORs: 38 (18 with DHEA, 20 No DHEA) |
|
| DHEA 25 mg/3 times daily | Minimum 2 months |
| No | Author | Gene Tested | Outcomes | Pathway Involved | ||
|---|---|---|---|---|---|---|
| Upregulated | Downregulated | No Difference | ||||
| 1 | Narkwichean et al. [14] |
| - | - | PTGS2, HAS2, PTX3, GREM1, AREG, EREG, BTC |
|
| 2 | Tsui et al. [13] |
| HAS2, VCAN, THBS1 | RUNX2, CBX3, TRIM28, BCL2, BAX, ANKRD57 | - |
|
| 3 | Lin et al. [15] |
| BCL2,Mitochondrial dehydrogenase activity | BAX, Cytochrome c, Caspase 3, Caspase 9 | - |
|
| 4 | Lin et al. [16] |
| BCL2TFAM | BAX, BAD, Cytochrome c, Caspase 3, Caspase 9 | - |
|
| 5 | Hou et al. [17] | PGAM5 | PGAM5 | - |
| |
| Study Author | Narkwichean et al. [14] | Tsui et al. [13] | Lin et al. [15] | Lin et al. [18] | Lin et al. [16] | Li et al. [19] | Hou et al. [17] |
|---|---|---|---|---|---|---|---|
| Comparison | DHEA vs. Non-DHEA | Post-DHEA | Post vs. Pre-DHEA | Older group DHEA vs. No DHEA | PORs group DHEA vs. No DHEA | Older group DHEA vs. No DHEA | PORs group DHEA vs. No DHEA |
| Stimulation Outcomes | |||||||
| Stimulation Duration (Days) | 12.5 (10–17) vs. 13 (10–14); p = 0.81 | NA | 10.3 ± 2.2 vs. 9.8 ± 2.5; p = 0.64 | 10.9 ± 1.9 vs. 10.3 ± 2.2 | NA | NA | 10.5 ± 1.5 vs. 12.1 ± 2.2 |
| Gonadotrophin doses (IU) | 3801.6 ± 1007.9 vs. 3802.2 ± 678.9; p = 0.99 | NA | 3150.0 ± 264.02 vs. 2950.0 ± 745.0; p = 0.49 | 3139.3 ± 595.7 vs. 2910.0 ± 813.3 | NA | NA | 2795.4 ± 684.1 vs. 2775.1 ± 806.9 |
| Cycle Outcomes | |||||||
| N. of oocytes retrieved | med (IQR): 4, 0–18 vs. 4, 0–15; p = 0.54 | p < 0.01 | 3.17 ± 1.60 vs. 2.00 ± 1.10; p = 0.17 | 3.5 ± 2.1 vs. 2.4 ± 1.3 | 3.5 ± 2 vs. 2.3 ± 1.2 | 5.2 ± 1.4 vs. 3.2 ± 2.1; p < 0.05 | 3.8 ± 2.1 vs. 3.2 ± 2.2; p < 0.05 |
| N. of MII oocytes retrieved | NA | NA | 1.67 ± 0.82 vs. 0.50 ± 0.55; p < 0.05 | 2.3 ± 1.7 vs. 1.2 ± 1.0 | 2.2 ± 1.6 vs. 1.1 ± 0.9 | 2.3 ± 1.5 vs. 1.8 ± 1.7 | 2.7 ± 1.2 vs. 1.4 ± 2.5 |
| Fertilization rate (%) | 64.5 ± 24.9 vs. 48.0 ± 30.4; p = 0.052 | NA | 75.6 ± 28.5 vs. 22.2 ± 27.2; p < 0.01 | 76.8 vs. 55.4; p < 0.05 | 75.9 vs. 58.8; p < 0.05 | 71.7 ± 22.0 vs. 67.8 ± 21.2 | 76.5 ± 21.2 vs. 66.2 ± 11.2 |
| N. of day 3 embryos | NA | p < 0.0001 | 2.17 ± 0.98 vs. 0.67 ± 0.82; p < 0.05 | NA | NA | 3.4 ± 1.6 vs. 1.7 ± 2.1; p < 0.05 | 3.5 ± 1.5 vs. 1.5 ± 2.2; p < 0.05 |
| N. of top-quality D3 embryos | NA | NA | NA | 1.2 ± 1.1 vs. 0.3 ± 0.6 | 1.2 ± 1.1 vs. 0.3 ± 0.6; p < 0.05 | 2.4 ± 1.7 vs. 0.7 ± 1.2; p < 0.05 | 1.9 ± 1.7 vs. 0.7 ± 1.5; p < 0.05 |
| Pregnancy Outcomes | |||||||
| Clinical pregnancy rate (%) | 8 ± 30 vs. 9 ± 36; p = 0.63 | NA | NA | 17.7 vs. 4.8 | 18.7 vs. 5.2 | 26.3 vs. 16 | 27.7 vs. 15.0 |
| Ongoing pregnancy rate (%) | NA | NA | NA | NA | 15.6 vs. 2.6 | 26.3 vs. 16 | 22.2 vs. 15.0 |
| Live birth rate (%) | 7 ± 26 vs. 8 ± 32; p = 0.63 | NA | NA | NA | 12.9 vs. 2.6 | 16.7 vs. 12 | 22.2 vs. 10.0 |
3.4. Clinical Outcomes
4. Discussion
5. Strength and Limitation
6. Gaps and Future Recommendation
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gnoth, C.; Godehardt, E.; Frank-Herrmann, P.; Friol, K.; Tigges, J.; Freundl, G. Definition and prevalence of subfertility and infertility. Hum. Reprod. 2005, 20, 1144–1147. [Google Scholar] [CrossRef]
- Weil, S.J.; Vendola, K.; Zhou, J.; Adesanya, O.O.; Wang, J.; Okafor, J.; Bondy, C.A. Androgen receptor gene expression in the primate ovary: Cellular localization, regulation, and functional correlations. J. Clin. Endocrinol. Metab. 1998, 83, 2479–2485. [Google Scholar] [CrossRef]
- Bachmann, G.; Bancroft, J.; Braunstein, G.; Burger, H.; Davis, S.; Dennerstein, L.; Goldstein, I.; Guay, A.; Leiblum, S.; Lobo, R.; et al. Female androgen insufficiency: The Princeton consensus statement on definition, classification, and assessment. Fertil. Steril. 2002, 77, 660–665. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, B.W.; Kirchengast, S.; Albrecht, A.; Laml, T.; Soregi, G.; Huber, J.C. Androgen serum levels in women with premature ovarian failure compared to fertile and menopausal controls. Gynecol. Obstet. Investig. 1997, 44, 127–131. [Google Scholar] [CrossRef] [PubMed]
- Burger, H.G. Androgen production in women. Fertil. Steril. 2002, 77 (Suppl. 4), S3–S5. [Google Scholar] [CrossRef] [PubMed]
- Nagels, H.E.; Rishworth, J.R.; Siristatidis, C.S.; Kroon, B. Androgens (dehydroepiandrosterone or testosterone) for women undergoing assisted reproduction. Cochrane Database Syst. Rev. 2015, 11, CD009749. [Google Scholar] [CrossRef]
- Casson, P.R.; Santoro, N.; Elkind-Hirsch, K.; Carson, S.A.; Hornsby, P.J.; Abraham, G.; Buster, J.E. Postmenopausal dehydroepiandrosterone administration increases free insulin-like growth factor-I and decreases high-density lipoprotein: A six-month trial. Fertil. Steril. 1998, 70, 107–110. [Google Scholar] [CrossRef] [PubMed]
- Cillo, F.; Brevini, T.A.; Antonini, S.; Paffoni, A.; Ragni, G.; Gandolfi, F. Association between human oocyte developmental competence and expression levels of some cumulus genes. Reproduction 2007, 134, 645–650. [Google Scholar] [CrossRef]
- Wathlet, S.; Adriaenssens, T.; Segers, I.; Verheyen, G.; Van de Velde, H.; Coucke, W.; Ron El, R.; Devroey, P.; Smitz, J. Cumulus cell gene expression predicts better cleavage-stage embryo or blastocyst development and pregnancy for ICSI patients. Hum. Reprod. 2011, 26, 1035–1051. [Google Scholar] [CrossRef]
- Lin, L.T.; Tsui, K.H.; Wang, P.H. Clinical application of dehydroepiandrosterone in reproduction: A review of the evidence. J. Chin. Med. Assoc. 2015, 78, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Qureshi, R.; Mattis, P.; Lisy, K.; et al. Chapter 7: Systematic reviews of etiology and risk. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020. [Google Scholar]
- Ferraretti, A.P.; La Marca, A.; Fauser, B.C.; Tarlatzis, B.; Nargund, G.; Gianaroli, L. ESHRE working group on Poor Ovarian Response Definition. ESHRE consensus on the definition of ‘poor response’ to ovarian stimulation for in vitro fertilization: The Bologna criteria. Hum. Reprod. 2011, 26, 1616–1624. [Google Scholar] [CrossRef] [PubMed]
- Tsui, K.H.; Lin, L.T.; Horng, H.C.; Chang, R.; Huang, B.S.; Cheng, J.T.; Wang, P.H. Gene expression of cumulus cells in women with poor ovarian response after dehydroepiandrosterone supplementation. Taiwan J. Obstet. Gynecol. 2014, 53, 559–565. [Google Scholar] [CrossRef] [PubMed]
- Narkwichean, A.; Maalouf, W.; Baumgarten, M.; Polanski, L.; Raine-Fenning, N.; Campbell, B.; Jayaprakasan, K. Efficacy of Dehydroepiandrosterone (DHEA) to overcome the effect of ovarian ageing (DITTO): A proof of principle double blinded randomized placebo controlled trial. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 218, 39–48. [Google Scholar] [CrossRef]
- Lin, L.T.; Wang, P.H.; Chen, S.N.; Li, C.J.; Wen, Z.H.; Cheng, J.T.; Tsui, K.H. Protection of cumulus cells following dehydroepiandrosterone supplementation. Gynecol. Endocrinol. 2017, 33, 100–104. [Google Scholar] [CrossRef]
- Lin, L.T.; Wang, P.H.; Wen, Z.H.; Li, C.J.; Chen, S.N.; Tsai, E.M.; Cheng, J.-T.; Tsui, K.-H. The Application of Dehydroepiandrosterone on Improving Mitochondrial Function and Reducing Apoptosis of Cumulus Cells in Poor Ovarian Responders. Int. J. Med. Sci. 2017, 14, 585–594. [Google Scholar] [CrossRef] [PubMed]
- Hou, Y.L.; Li, C.J.; Lin, L.T.; Chen, S.N.; Wen, Z.H.; Tsui, K.H. DHEA restores mitochondrial dynamics of cumulus cells by regulating PGAM5 expression in poor ovarian responders. Taiwan. J. Obstet. Gynecol. 2022, 61, 223–229. [Google Scholar] [CrossRef]
- Lin, L.T.; Cheng, J.T.; Wang, P.H.; Li, C.J.; Tsui, K.H. Dehydroepiandrosterone as a potential agent to slow down ovarian aging. J. Obstet. Gynaecol. Res. 2017, 43, 1855–1862. [Google Scholar] [CrossRef]
- Li, C.J.; Lin, L.T.; Tsui, K.H. Dehydroepiandrosterone Shifts Energy Metabolism to Increase Mitochondrial Biogenesis in Female Fertility with Advancing Age. Nutrients 2021, 13, 2449. [Google Scholar] [CrossRef]
- Barad, D.H.; Gleicher, N. Increased oocyte production after treatment with dehydroepiandrosterone. Fertil. Steril. 2005, 84, 756.e1–756.e3. [Google Scholar] [CrossRef]
- Hu, Q.; Hong, L.; Nie, M.; Wang, Q.; Fang, Y.; Dai, Y.; Zhai, Y.; Wang, S.; Yin, C.; Yang, X. The effect of dehydroepiandrosterone supplementation on ovarian response is associated with androgen receptor in diminished ovarian reserve women. J. Ovarian. Res. 2017, 10, 32. [Google Scholar] [CrossRef]
- McKenzie, L.J.; Pangas, S.A.; Carson, S.A.; Kovanci, E.; Cisneros, P.; Buster, J.E.; Amato, P.; Matzuk, M.M. Human cumulus granulosa cell gene expression: A predictor of fertilization and embryo selection in women undergoing IVF. Hum. Reprod. 2004, 19, 2869–2874. [Google Scholar] [CrossRef] [PubMed]
- Gebhardt, K.M.; Feil, D.K.; Dunning, K.R.; Lane, M.; Russell, D.L. Human cumulus cell gene expression as a biomarker of pregnancy outcome after single embryo transfer. Fertil. Steril. 2011, 96, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Shen, Q.; Chen, M.; Zhao, X.; Liu, Y.; Ren, X.; Zhang, L. Versican expression level in cumulus cells is associated with human oocyte developmental competence. Syst. Biol. Reprod. Med. 2020, 66, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Xiong, S.; Mu, T.; Wang, G.; Jiang, X. Mitochondria-mediated apoptosis in mammals. Protein Cell 2014, 5, 737–749. [Google Scholar] [CrossRef]
- Roy, M.J.; Vom, A.; Czabotar, P.E.; Lessene, G. Cell death and the mitochondria: Therapeutic targeting of the BCL-2 family-driven pathway. Br. J. Pharmacol. 2014, 171, 1973–1987. [Google Scholar] [CrossRef] [PubMed]
- Dimri, G.P.; Lee, X.; Basile, G.; Acosta, M.; Scott, G.; Roskelley, C.; Medrano, E.E.; Linskens, M.; Rubelj, I.; Pereira-Smith, O. A biomarker that identifies senescent human cells in culture and in aging skin in vivo. Proc. Natl. Acad. Sci. USA 1995, 92, 9363–9367. [Google Scholar] [CrossRef]
- Geng, Y.Q.; Guan, J.T.; Xu, X.H.; Fu, Y.C. Senescence-associated beta-galactosidase activity expression in aging hippocampal neurons. Biochem. Biophys. Res. Commun. 2010, 396, 866–869. [Google Scholar] [CrossRef]
- Vlahos, N.; Papalouka, M.; Triantafyllidou, O.; Vlachos, A.; Vakas, P.; Grimbizis, G.; Creatsas, G.; Zikopoulos, K. Dehydroepiandrosterone administration before IVF in poor responders: A prospective cohort study. Reprod. Biomed. Online 2015, 30, 191–196. [Google Scholar] [CrossRef]
- Yeung, T.; Chai, J.; Li, R.; Lee, V.; Ho, P.C.; Ng, E. A double-blind randomised controlled trial on the effect of dehydroepiandrosterone on ovarian reserve markers, ovarian response and number of oocytes in anticipated normal ovarian responders. BJOG Int. J. Obstet. Gynaecol. 2016, 123, 1097–1105. [Google Scholar] [CrossRef]
- Wang, Z.; Yang, A.; Bao, H.; Wang, A.; Deng, X.; Xue, D.; Tan, H.; Zhou, Y.; Wu, C.; Chen, Z.-J.; et al. Effect of dehydroepiandrosterone administration before in vitro fertilization on the live birth rate in poor ovarian responders according to the Bologna criteria: A randomised controlled trial. BJOG Int. J. Obstet. Gynaecol. 2022, 129, 1030–1038. [Google Scholar] [CrossRef]
- Sonmezer, M.; Ozmen, B.; Cil, A.P.; Ozkavukcu, S.; Tasci, T.; Olmus, H.; Atabekoğlu, C.S. Dehydroepiandrosterone supplementation improves ovarian response and cycle outcome in poor responders. Reprod. Biomed. Online 2009, 19, 508–513. [Google Scholar] [CrossRef] [PubMed]
- Zangmo, R.; Singh, N.; Kumar, S.; Vanamail, P.; Tiwari, A. Role of dehydroepiandrosterone in improving oocyte and embryo quality in IVF cycles. Reprod. Biomed. Online 2014, 28, 743–747. [Google Scholar] [CrossRef] [PubMed]
- Artini, P.G.; Simi, G.; Ruggiero, M.; Pinelli, S.; Di Berardino, O.M.; Papini, F.; Papini, S.; Monteleone, P.; Cela, V. DHEA supplementation improves follicular microenviroment in poor responder patients. Gynecol. Endocrinol. 2012, 28, 669–673. [Google Scholar] [CrossRef] [PubMed]
- Wiser, A.; Gonen, O.; Ghetler, Y.; Shavit, T.; Berkovitz, A.; Shulman, A. Addition of dehydroepiandrosterone (DHEA) for poor-responder patients before and during IVF treatment improves the pregnancy rate: A randomized prospective study. Hum. Reprod. 2010, 25, 2496–2500. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Yuan, H.; Chen, Y.; Wu, H.; Wu, H.; Li, L. A meta-analysis of dehydroepiandrosterone supplementation among women with diminished ovarian reserve undergoing in vitro fertilization or intracytoplasmic sperm injection. Int. J. Gynaecol. Obstet. 2015, 131, 240–245. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yuan, W.S.; Abu, M.A.; Ahmad, M.F.; Elias, M.H.; Abdul Karim, A.K. Effects of Dehydroepiandrosterone (DHEA) Supplementation on Ovarian Cumulus Cells following In Vitro Fertilization (IVF)/Intra-Cytoplasmic Sperm Injection (ICSI) Treatment—A Systematic Review. Life 2023, 13, 1237. https://doi.org/10.3390/life13061237
Yuan WS, Abu MA, Ahmad MF, Elias MH, Abdul Karim AK. Effects of Dehydroepiandrosterone (DHEA) Supplementation on Ovarian Cumulus Cells following In Vitro Fertilization (IVF)/Intra-Cytoplasmic Sperm Injection (ICSI) Treatment—A Systematic Review. Life. 2023; 13(6):1237. https://doi.org/10.3390/life13061237
Chicago/Turabian StyleYuan, Woon Shu, Muhammad Azrai Abu, Mohd Faizal Ahmad, Marjanu Hikmah Elias, and Abdul Kadir Abdul Karim. 2023. "Effects of Dehydroepiandrosterone (DHEA) Supplementation on Ovarian Cumulus Cells following In Vitro Fertilization (IVF)/Intra-Cytoplasmic Sperm Injection (ICSI) Treatment—A Systematic Review" Life 13, no. 6: 1237. https://doi.org/10.3390/life13061237
APA StyleYuan, W. S., Abu, M. A., Ahmad, M. F., Elias, M. H., & Abdul Karim, A. K. (2023). Effects of Dehydroepiandrosterone (DHEA) Supplementation on Ovarian Cumulus Cells following In Vitro Fertilization (IVF)/Intra-Cytoplasmic Sperm Injection (ICSI) Treatment—A Systematic Review. Life, 13(6), 1237. https://doi.org/10.3390/life13061237